
Abstract
Individuals with psychosis are at increased risk of suicide, particularly during the initial few years following illness onset [1,2], including the period before detection and treatment [3–6]. Several studies have examined the prevalence of suicide attempts and suicides among people receiving psychiatric treatment following their first episode psychosis (FEP). FEP refers to psychosis that has not previously been treated with neuroleptic medication [6]. In the 12 months since the initial contact with a mental health service, between 21% and 50% of patients seriously consider suicide [3,7], and about 10% make a suicide attempt [3,7–9]. Up to 1.5% of patients die from suicide within 18 months of treatment for FEP [8–11]. Developing strategies to minimize the number of suicide attempts and suicides is therefore an important challenge for psychiatric services treating patients at the early stages of a psychotic illness [12].
Research among people with psychotic disorders, including those undergoing treatment for FEP [8,9,11], has for the most part adopted a risk recognition suicide prevention paradigm. Studies have examined various socio-demographic, clinical, and treatment characteristics of at risk individuals, as well as factors that could become specific targets of preventative interventions. The utility of the findings has been limited, however, due to the low sensitivity and specificity of the risk factors, making it difficult to identify the few patients who will attempt suicide.
An alternative approach is to investigate the characteristics of suicide attempts and suicides, which could lead to recommendations for clinical care and service-level prevention strategies. Moreover, this approach may be more effective in preventing suicide attempts in high risk groups where the identification of people who are at greatest risk often proves difficult. An example of such studies are the national and state-wide audits of clinical records of users of public mental health services who suicided, conducted in Australia and England [13–16]. The Australian audit focused on aspects of clinical care (e.g. quality of staff–patient relationships; adequacy of suicide risk assessment; length of time between outpatient appointments) with a view to determining whether and how some of the suicides could have been prevented by services [13]. The English audit also investigated various elements of clinical care, including treatment setting, the nature of the last contact with a mental health professional, the methods, and the locations of suicides [14–16]. Both audits recommended measures by which services could minimize the risk of suicide attempts and suicides, and had implications for policy development [13–16].
The findings based on audits of suicides in heterogenous groups of psychiatric patients may not generalize to young individuals with FEP who have limited, if any, previous experience of mental health services [17]. However, to date no study has profiled suicide attempts in youth undergoing treatment for FEP. Thus, the aim of the present study was to examine the characteristics of suicide attempts in young people who were receiving treatment at a specialist early psychosis service at the time of the incident. In particular, we were interested in profiling: the methods, locations, treatment settings, level of impulsivity, precipitants, help-seeking patterns, severity, medical assistance and psychiatric admissions associated with suicide attempts. We were also interested in determining the prevalence of multiple suicide attempts during treatment, and in comparing the characteristics of single versus repeat attempts.
Method
Sample and setting
The sample was identified from a database recording information about all individuals accepted into the Early Psychosis Prevention and Intervention Centre (EPPIC) [17,18] between 1 December 2002 and 30 November 2005 (N = 699). EPPIC is a comprehensive, specialist service in a catchment area of Melbourne, Australia, of approximately 960 000 inhabitants, with a mandate to treat 15–24 year olds experiencing FEP. Patients receive treatment for up to 18 months [17]; for those admitted at 15 years of age, treatment extends until their eighteenth birthday [18].
Study design
This cohort study used data collected from retrospective medical record audit. The period of observation was from the date of assessment of psychotic symptoms that led to EPPIC treatment to the date of discharge from the service (mean (M) = 574.5 days, median = 581.5, mode = 546). The project was approved by the Mental Health Research and Ethics Committee and La Trobe University Human Ethics Committee.
Procedure
The study procedure involved three steps. First, from 699 patients accepted for treatment at EPPIC in the period of interest, 50 individuals (7.3%) were excluded because their medical records were unavailable. A further 42 patients (6%) were excluded as their discharge reports indicated that the apparent psychotic symptoms upon presentation to the service were subsequently considered to be part of a personality disorder. Second, one investigator (I.F.) identified potential suicide or suicide attempt incidents by reviewing medical files of the remaining 607 patients. An incident referred to any self-inflicted injury or self-inflicted poisoning that the patient carried out or was about to carry out. All assessment and discharge reports, notes from emergency rooms, and suicide risk assessment forms covering the period of treatment at EPPIC were reviewed, followed by an in-depth inspection of case notes related to the incident. Each incident was then assessed with the Classification Algorithm for Determination of Suicide Attempt and Suicide (CAD-SAS) [19]. Last, incidents deemed to be ‘true’ suicide attempts or suicides were rated on the variables described in the next section.
Measures
The CAD-SAS is a classification system developed for the purpose of this study. It provides an algorithm that enables raters with limited clinical experience to classify narrative information about self-injurious incidents into one of three categories: ‘suicide attempt or suicide’, ‘not suicide attempt or suicide’, or ‘undetermined incident’. The CAD-SAS has excellent test − retest reliability (97.2% concordance), good inter-rater reliability (kappa or κ = 0.70), and good construct validity (κ = 0.46) [Fedyszyn, Harris, Robinson, Paxton: under review].
Structured file audit tools were developed to aid the extraction of demographic, clinical, and treatment information associated with suicide attempts. If a patient made multiple attempts, each attempt was rated independently of others. Key variables included: date of assessment for psychotic symptoms at EPPIC, date of suicide attempt, days to suicide attempt (defined as the period between assessment and attempt), methods used for suicide attempt, including classification into violent and non-violent methods [20], impulsive or planned nature of suicide attempt (a planned attempt was operationalized as an act where there is evidence that a person was preparing for it at least one day in advance; an impulsive attempt had a plan hastily put together or did not have a plan), presence of a suicide note, treatment status at the time of attempt, key precipitants as reported by the patient, help-seeking behaviour immediately before suicide attempt (operationalized as contacting somebody or a service within minutes before the attempt); help-seeking behaviour immediately after suicide attempt (operationalized as contacting somebody or a service within minutes after the attempt), severity of suicide attempt, (defined according to the World Health Organization Life Chart [21] as mild/hardly any injury, moderate/some injury, or severe/almost died or serious lasting injury), mental state within several hours after attempt, presence of medical assistance in response to attempt, psychiatric admission in response to attempt, whether the person attempted suicide once or on multiple occasions, and number of days between consecutive attempts for repeated attempts.
Statistical analysis
Two-group comparisons for categorical data were performed using the χ2 test with Fisher's probability test where appropriate [22], and an independent sample t-test was used for continuous data. All tests were two-tailed, with α < 0.05.
Results
Prevalence of suicide attempts and sample characteristics
Of the 607 patients, 73 (12%) were classified as having made a suicide attempt during treatment. Of these 73 patients, 34 were men (46.6%), and the mean age was 19.21 years (SD = 2.62). The majority (58/73; 79.4%) were diagnosed with non-affective psychosis (i.e. schizophrenia, schizophreniform disorder, brief psychotic disorder, psychosis not otherwise specified, delusional disorder, or substance-induced psychosis). Over two thirds (49/73; 67.1%) had at least one comorbid diagnosis, most commonly depression (24/73; 32.9%), substance abuse/dependence (20/73; 27.4%), anxiety disorders (12/73; 16.4%), and personality disorders (21/73; 28.8%), predominantly borderline personality disorder (17/73; 23.3%). Most patients were never married, nor partnered (63/73; 86.3%), 9.7% (7/73) lived alone, and just under half (34/73; 46.6%) were unemployed, with a further quarter (19/73; 26.8%) not participating in the labour force.
Methods of suicide attempts
A total of 116 suicide attempts, including two attempts that resulted in death [23], were identified among the 73 attempters. Most patients attempted suicide on one occasion (53/73; 72.6%), 10 (13.7%) made two attempts, and another 10 (13.7%) made between three and seven attempts. The methods of suicide attempts are summarized in Table 1.
Methods of suicide attempts in patients undergoing treatment for FEP
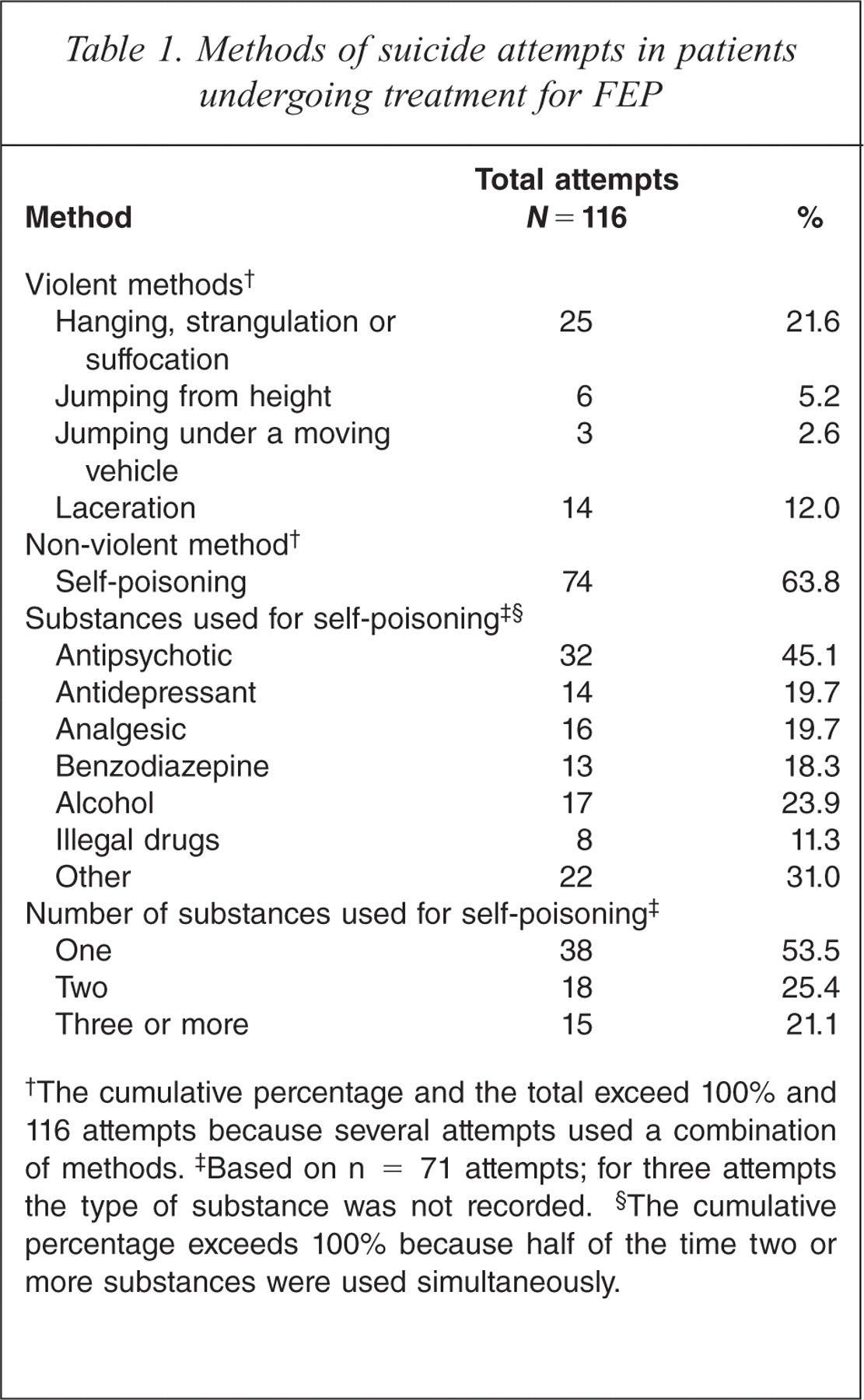
The cumulative percentage and the total exceed 100% and 116 attempts because several attempts used a combination of methods.
Based on n = 71 attempts; for three attempts the type of substance was not recorded.
The cumulative percentage exceeds 100% because half of the time two or more substances were used simultaneously.
Almost all suicide attempts (110/116; 94.8%) involved a single method, six used two methods: a combination of self-poisoning with cutting, hanging/strangulation, or jumping from a height. Two thirds of attempts employed non-violent means, most commonly self-poisoning with antipsychotic medications. When more than one type of substance was used for self-poisoning, the most frequent combinations included antipsychotic and antidepressant medications, and alcohol with antipsychotics or benzodiazepines.
Hanging, strangulation or suffocation was the second most frequently used method and was significantly more common in inpatient than outpatient suicide attempts (82.4% versus 10.1%), χ2(1) = 46.2, p < 0.01. In fact, all suicide attempts on the inpatient psychiatric unit (n = 13) were by hanging or strangulation. In all inpatient hangings the door was the ligature point and the ligatures involved bed sheets, belts, shoe laces, and pieces of clothing (e.g. pyjama pants).
Timing, location of suicide attempt and treatment setting
A total of 15% (17/110) of suicide attempts took place within 30 days of the initial contact with the service and a further 36.4% (40/110) within a period of up to 6 months. Almost half of the attempts (53/110; 48.2%) occurred after 6 months of treatment; 60% of all suicide attempts (39/65) occurred at home, 20% (13/65) on the psychiatric ward, and 20% (13/65) in a public area, most commonly in public toilets, on a bridge, or on train tracks. Most attempts (99/116; 85.3%) took place when the individual was receiving outpatient treatment, including 13.1% (14/107) that occurred within 2 weeks of discharge from the inpatient psychiatric unit. In most cases (45/58; 77.6%), the attempts occurred in the context of regular outpatient contact, that is, among individuals who had attended at least 75% of their scheduled appointments in the previous 3 months.
The nature of the act and the precipitants
Information about the nature of the suicide attempts and precipitating factors is presented in Table 2. The majority of attempts were impulsive, and few were accompanied by a suicide note (8/76; 10.1%). One third of suicide attempts were triggered by interpersonal issues, such as relationship problems or break up, peer conflict, or family discord. The second most common precipitant was distress caused by symptoms, predominantly delusional beliefs, visual or auditory hallucinations, relapse, or a lack of perceived improvement despite treatment with neuroleptic medication. However, a few suicide attempts were precipitated by persistent symptoms of obsessive–compulsive disorder and panic attacks.
Nature of suicide attempts and self-reported precipitants in patients undergoing treatment for FEP
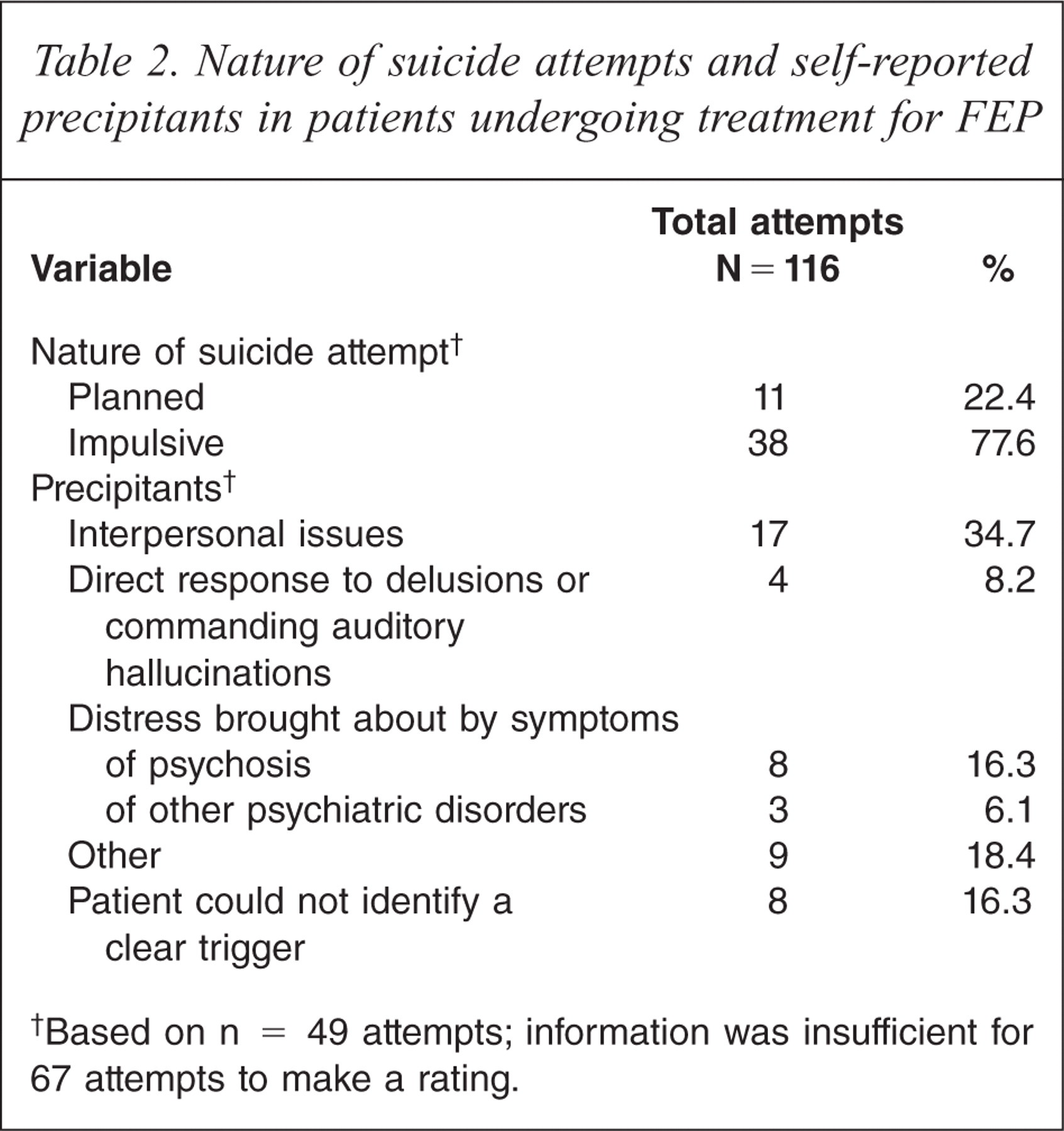
Based on n = 49 attempts; information was insufficient for 67 attempts to make a rating.
Help-seeking immediately before and immediately after suicide attempts
In seven out of 66 suicide attempts (10.6%) individuals sought help immediately before making an attempt on their life. Three attempts were preceded by contacting professionals (e.g. case manager, emergency rooms) and a further four by contacting informal supports (family member, boyfriend/girlfriend, or a friend). A larger proportion of individuals sought help immediately after the suicide attempt (17/56; 30.4%); in most cases (12/17; 70.6%) informal supports were contacted. Female patients were significantly more likely than their male counterparts to seek help before, χ2(1) = 4.72, p = 0.05, and after a suicide attempt, χ2(1) = 4.89, p = 0.03. When individuals did not seek help, family members or partners were most likely to discover them either during or shortly after the attempt (14/39; 35.9%), followed by a bystander (5/39 or 12.8%), or a housemate (4/39; 10.3%).
Degree of severity, mental state within several hours after the suicide attempt, medical assistance and psychiatric admission
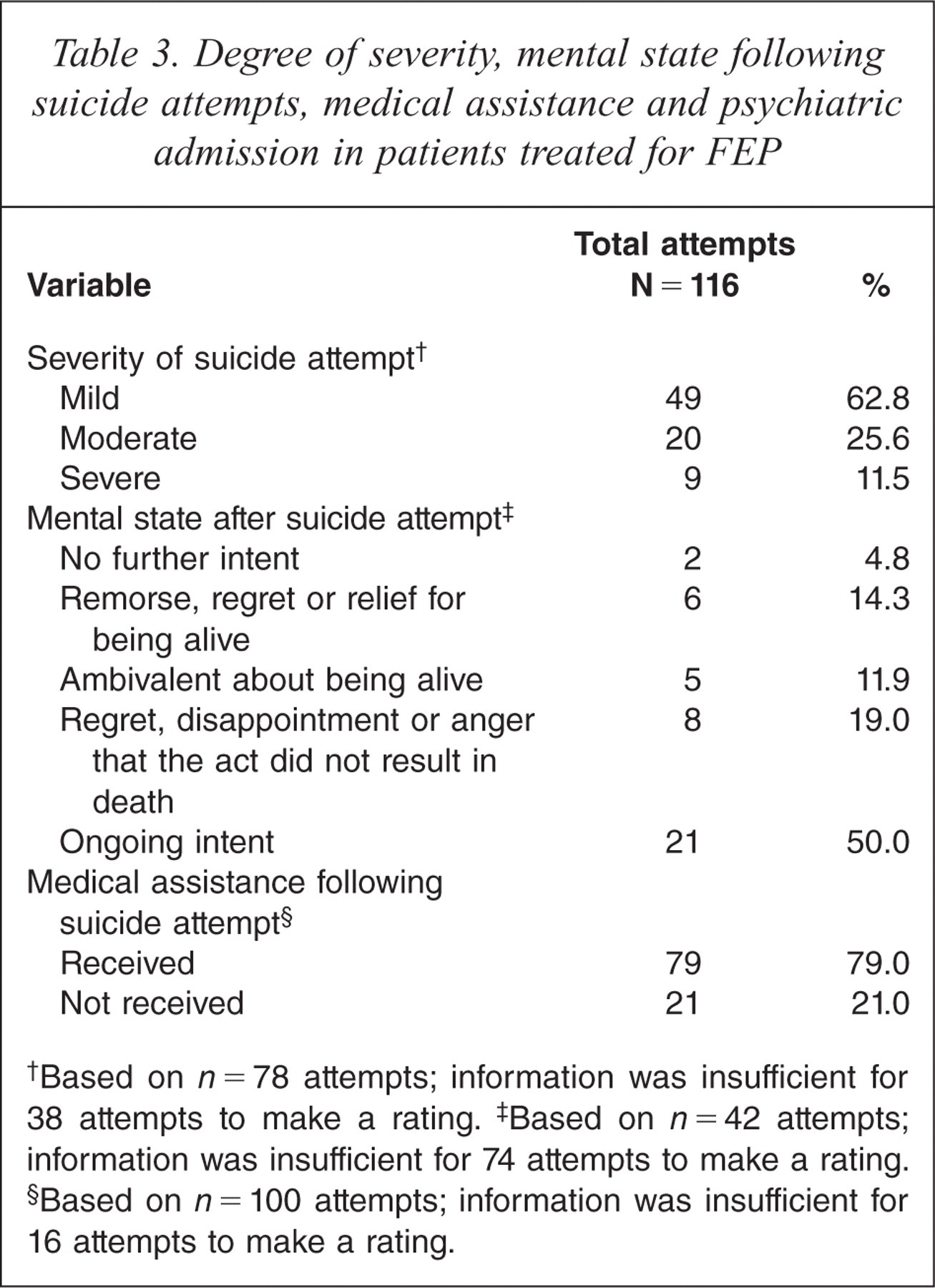
Table 3 presents information about the severity and mental state several hours after suicide attempts, and the provision of medical assistance following the attempts. Most suicide attempts resulted in mild injury. The majority of attempts were followed by ongoing suicidal intent, regret, disappointment or anger that the act did not result in death, although these reactions did not distinguish between single and repeat attempters, χ2(1) = 0.03, p = 0.90. Of the attempts that received medical assistance (79/100), 60% (48/79) resulted in subsequent admission to the inpatient psychiatric unit and 8.9% (7/79) in treatment at the emergency rooms. The average duration of a psychiatric inpatient admission was 6.65 days (SD = 4.93), with female patients having significantly longer inpatient admissions than male (M = 8.86, SD = 5.74, and M = 4.08, SD = 1.73, respectively), t(24) = − 2.96, p = 0.01.
Degree of severity, mental state following suicide attempts, medical assistance and psychiatric admission in patients treated for FEP
Based on
Based on
Based on
Single versus repeat suicide attempts
The timing of suicide attempts was compared between individuals who made a single attempt and those with repeat attempts. Patients who had two or more suicide attempts during treatment made their first attempt significantly earlier in the course of treatment than patients who attempted suicide once, 3 months after entry to the service (M = 88.48 days, SD = 85.62) versus nine months, respectively (M = 259.04 days, SD = 219), t(65) = 4.65, p < 0.001. The timing of repeat attempts was also examined; 70% (14/20) of the second suicide attempts took place within 3 months after the initial attempt, and 50% (4/8) of the third attempts occurred within 3 months from the second. In the repeat attempts, most patients (13/20; 65%) used the same method as at the index attempt at least once, however, no trend was found for increased severity of subsequent attempts. The triggers varied between the first and subsequent attempts (5/7; 71.4%).
Discussion
The study confirms that suicide attempts among people with FEP are relatively common and hence present a challenge for the mental health services. Our finding that 11.8% of patients attempted suicide during the treatment period is consistent with past research reporting 8.7% and 11.3% of suicide attempts over the initial 24 months [9,11]. Moreover, the results indicate that examination of the characteristics of suicide attempts in this population has the potential to highlight issues that are pertinent to generating meaningful suicide prevention strategies.
Before interpreting the specific findings, it is important to consider the strengths and limitations of the study. The main strengths relate to sampling and methodology, specifically, the sample comprised consecutive admissions over 3 years to a specialist service covering a large catchment area with few private psychiatric services. As the service is a first contact for treatment, the sample can be considered representative of the first episode cases in the area [9]. An advantage of the retrospective file audit methodology is that it allows virtually complete capture of all patients and avoids potential response bias due to refusal to participate. Moreover, we used a system with good psychometric properties for determination of suicide attempts and suicides, which ensured uniform criteria for assessment and classification of incidents. The main limitation is that data were extracted retrospectively from medical records. Some information related to suicide attempts was not routinely recorded, resulting in substantial amounts of missing data for precipitating factors, impulsivity, and mental state following the attempts. An insufficient number of observations in some cells precluded additional comparisons of the single and multiple attempts, and gender differences. Further, it is possible that some suicide attempts were not recorded in the patients' files. The proportion of incidents that could have been missed would be minimal, though, as EPPIC clinicians are required to document self-harming behaviours and accidents reported by the patients or third parties. Finally, the findings may not generalize to other services treating FEP individuals, particularly those with a wider range of intake age [17].
There were six key findings from the study with implications for suicide prevention in patients treated for FEP. The first is that, in line with past research [11,24,25], the most common method of suicide attempt was self-poisoning. Previous studies have not reported on the substances used; we found that antipsychotics were involved in almost half of these attempts, either alone or in combination with other prescribed medications or alcohol. This, together with the finding that the majority of suicide attempts are impulsive and therefore difficult to anticipate, suggests that restricting the amount of medication prescribed, or dispensed by pharmacists per purchase, may reduce morbidity and mortality associated with suicide attempts in this group. A meta-analysis of rates and methods of suicide in Australia [26] indicated the effectiveness of reducing access to lethal means in lowering the rates of suicide in the general population. A decrease in occurrence of suicide attempts and suicides has also been reported in countries that introduced restriction on availability of over-the-counter medications [27,28].
The second finding relates to the choice of method by individuals who were on the inpatient psychiatric unit at the time of the attempt, namely, hanging and strangulation. Restrictions to clothing items with laces, cords or belts for individuals who are identified as presenting at suicide risk could help prevent inpatient suicide attempts and suicides [29]. Moreover, regular monitoring of psychiatric wards to detect potential ligature points could maximize a safe environment for high risk individuals by way of reducing access to means [14,15]. At EPPIC, formal reviews of physical features of the inpatient unit were instituted in 2007 [Lavery C: personal communication]. Consistent with principles of good clinical practice [14–16,29], these reviews include audits of ligature points with structured checklists. The present study reports the results from the period before such stringent reviews were introduced; however, it would be valuable to determine whether the intervention improved patient safety.
The third key finding is that, as found in previous studies [20,30–32], the majority of suicide attempts took place when the individuals were in regular contact with outpatient services. Despite treatment compliance and engagement, few individuals sought help immediately prior to their attempts which might be a function of the impulsive nature of suicide attempts in young people with FEP and a compromised capacity to conceive alternative coping strategies or potential sources of help at the time. Generating individualized suicide risk management plans collaboratively with all patients entering treatment for FEP, including those who do not appear to be at immediate risk and those who do not present with any of the known suicide risk factors, may facilitate help-seeking at the time of a suicidal crisis. However, infrequent help-seeking prior to the attempt may also be reflective of individuals' genuine desire to die at the time, even if the act is impulsive rather than planned. Consistent with this explanation is the finding that help-seeking was also relatively uncommon after the attempt, and that in most cases suicidal intent or regret that the act did not result in death persisted for at least several hours. Thus, it appears that admission to the inpatient unit may ensure patients' safety and help to resolve the crisis through temporarily removing them from their daily stressors, or adjusting treatment if the attempt was brought on by psychiatric symptoms.
The fourth key finding is that when individuals sought help prior to making a suicide attempt, family members, partners, or friends were contacted. Moreover, given that two thirds of suicide attempts occurred at home, significant others were also most likely to discover individuals either whilst making the attempt or afterwards. These results suggest that informal sources of support could play a role in prevention and management of suicide attempts. Services treating young people following a FEP could consider providing education and information to the families of new patients about the most common indicators of suicide risk and appropriate responses. Family members, partners and close friends of those who have already experienced chronic suicidal ideation and/or attempted suicide before or during treatment, may benefit from psycho-education in the form of seminars with specific focus on risk recognition and management. This would need to be undertaken sensitively as we are not aware of any existing study on the impact of risk recognition and management awareness raising interventions on families. However, research has shown similar initiatives undertaken with professional groups to be an effective suicide prevention strategy [33,34]. Drawing on experiences, insights, and approaches used by significant others could be a valuable and empowering part of psycho-education by way of sharing information, peer support, confidence building, and de-stigmatizing suicide attempts and suicides.
The fifth finding, that the most common precipitants for suicide attempts were interpersonal issues and distressing psychotic symptoms, is consistent with past research [25,35–37]. Even though suicide attempts tend to be multi-factorial phenomena, understanding the triggers can inform prevention by highlighting areas where psycho-education and/or relevant skills training could strengthen the protective processes in young people with psychosis. Studies have demonstrated the effectiveness of problem solving training in reducing suicide risk in non-psychotic samples [38,39]. There is also some evidence indicating that problem solving, social skills training, stress management, and strategies improving tolerance for emotional pain, reduce suicidality in those treated for FEP [40]. Thus, interventions extending the range of and reinforcing the person's existing coping skills could provide a buffer against suicidal tendencies at times of increased stress. A decline in the rate of suicide attempts after individuals with psychosis engage in treatment, compared to the pretreatment period [5,6], indicates the need for assertive pharmacological and/or psychological treatments for patients whose psychiatric symptoms do not respond to standard interventions. At EPPIC, since 1994 such efforts are orchestrated by the Treatment Resistance Early Assessment Team (TREAT), a sub-programme for the early identification of patients who experience prolonged recovery from FEP [41].
Finally, in line with previous studies, only a minority of patients made more than one suicide attempt during the initial period of treatment for FEP [9,11,24]. Individuals who repeated suicide attempts made the first attempt early in the course of treatment, approximately 3 months after entry to EPPIC. The second attempt typically took place within 3 months of the initial attempt, consistent with the literature on suicide attempts in adolescents [42]. Thus, regular risk assessment and close monitoring of patients who have attempted suicide is indicated, particularly during the following 3 months when the risk of reattempt is highest. Moreover, clinicians should be alerted to the possibility of repeat suicide attempts in patients who make their first suicide attempt early in the course of treatment.
Individuals undergoing treatment for FEP are a challenging patient group due to an elevated suicide risk. At present, it is difficult to reliably identify patients who are most likely to attempt suicide during treatment and who could, therefore, be part of specific interventions aiming at risk reduction. However, the results of this study indicate that there are several strategies mental health services could consider with a view of preventing suicide attempts and suicides in this group.
Acknowledgements
The authors would like to acknowledge the support of the Early Psychosis Prevention and Intervention Centre (EPPIC) for providing access to the medical records of former patients. We would like to thank EPPIC senior clinical staff for their feedback on the material presented in this paper: Dr Shona Francey, Carolyn Lavery, Sylvia Collinetti, and Hannah Bloom. Thank you also to the anonymous reviewers for their feedback on the previous version of this manuscript.