
Abstract
Individuals with psychosis demonstrate high rates of suicidal behaviour [1, 2]. Few studies, however, have examined rates of suicidal behaviour among young people receiving treatment for first-episode psychosis (FEP); those that have report 1 year rates of 0.3–0.4% and 2.9–11% for suicide and suicide attempt (SA), respectively [3, 4] and 2 year rates of self-harm or SA, of 11.3% [5, 6]. Two studies have examined rates of suicide and SA over longer time periods: Clarke et al. reported a 4 year prevalence of 3% and 18.2% for completed suicide and SA, respectively [7], while Bertelsen et al. reported a 5 year prevalence of around 1% for completed suicide [8].
Risk of suicidal behaviour (including suicide, SA and self-harm) has been associated with male gender, higher social class, longer duration of untreated psychosis (DUP), substance use, depressive symptoms, younger age at onset of illness, a greater level of insight and previous suicidal ideation and attempts [3, 5–12].
To our knowledge only a few studies have assessed suicidal behaviour in an epidemiological incidence cohort of FEP, and this is the first of its kind in Australia. This is important because non-epidemiological studies lose patients who refuse study participation. These patients have been reported to have higher rates of comorbid substance use disorders (SUDs) and longer DUP as well as worse course illness [13], variables potentially linked to higher prevalence of suicidal behaviour.
The aims of the present study were to (i) examine the rates and type of suicide and SA in an incidence cohort of young people receiving treatment for FEP at a specialist early intervention centre; and (ii) examine the demographic, premorbid and clinical characteristics that predict SA during treatment.
Method
Context and sample
The initial sample consisted of an incidence cohort of 786 subjects with FEP admitted to the Early Psychosis Prevention and Intervention Centre (EPPIC) in Melbourne, Australia, from January 1998 to December 2000. EPPIC covers a catchment area of approximately 880 000 people and at the time of the study had a mandate to treat all patients aged 15–29 with FEP (today this is 12–25 years of age). In this catchment area there are no other specialist treatment facilities for this population; as such, the sample represents a true epidemiological cohort.
Information on each patient treated in EPPIC is documented in a standardized medical record. Each medical record consists of information compiled during the 18 month treatment period from various sources using assessments carried out by trained clinicians. Two experienced psychiatrists well acquainted with the EPPIC clinical service and the treatment of FEP patients assessed all medical records. The local research ethics committee approved the study [14, 15].
Of the 786 patients accepted into the service between 1998 and 2000, 82 patients’ medical records (10%) had been transferred to other services following discharge from EPPIC and were not available for the study. Of the remaining 704 patients, 43 (5%) were excluded from this analysis due to a discharge diagnosis of a non-psychotic disorder. The excluded patients did not differ in terms of diagnostic distribution or available demographic characteristics (age and gender). The final sample consisted of 661 patients.
Diagnostic assessment
Clinical diagnoses at EPPIC are assessed using DSM-IV criteria [16]. Diagnoses documented in medical records are based on repeated clinical assessments made using various sources of information and are performed by a treatment team consisting of a case manager, psychiatrist and consultant psychiatrist. Two research psychiatrists (ML, PC) assessed all information available in medical records with respect to diagnoses. The validity of the diagnoses recorded was established using the following procedure: between 1998 and 2000, 230 of the 786 patients treated at EPPIC consented to participate in prospective trials. Their main and comorbid diagnoses were assessed within 6 weeks of admission using the Structured Clinical Interview for DSM-IV (SCID-I/P [17]). The SCID and First-Episode Psychosis Outcome Study diagnoses of 115 patients randomly selected from this sample of 230 were compared. The calculated kappas indicated a very good concordance for both psychosis diagnoses (κ=0.80) and comorbid substance abuse diagnoses (κ=0.74). Detailed diagnostic process and diagnostic stability have been described previously [15, 16].
Measurement of suicide attempts
Because types of SA could not be categorized according to DSM-IV they were assessed and categorized according to ICD-10 diagnostic criteria [18].
Assessment and measures
Data were collected using a specifically designed clinical audit tool, the Early Psychosis File Questionnaire [15]. The following variables were assessed.
(1) Demographic and diagnostic variables (Table 1): (i) age, gender, education; and (ii) diagnosis (separated into five groups), comorbid SUD at baseline (separated into cannabis and polysubstance use-related) [14], and other comorbid psychiatric diagnosis [18].
Demographic and diagnostic factors of patients vs suicide attempt while in treatment
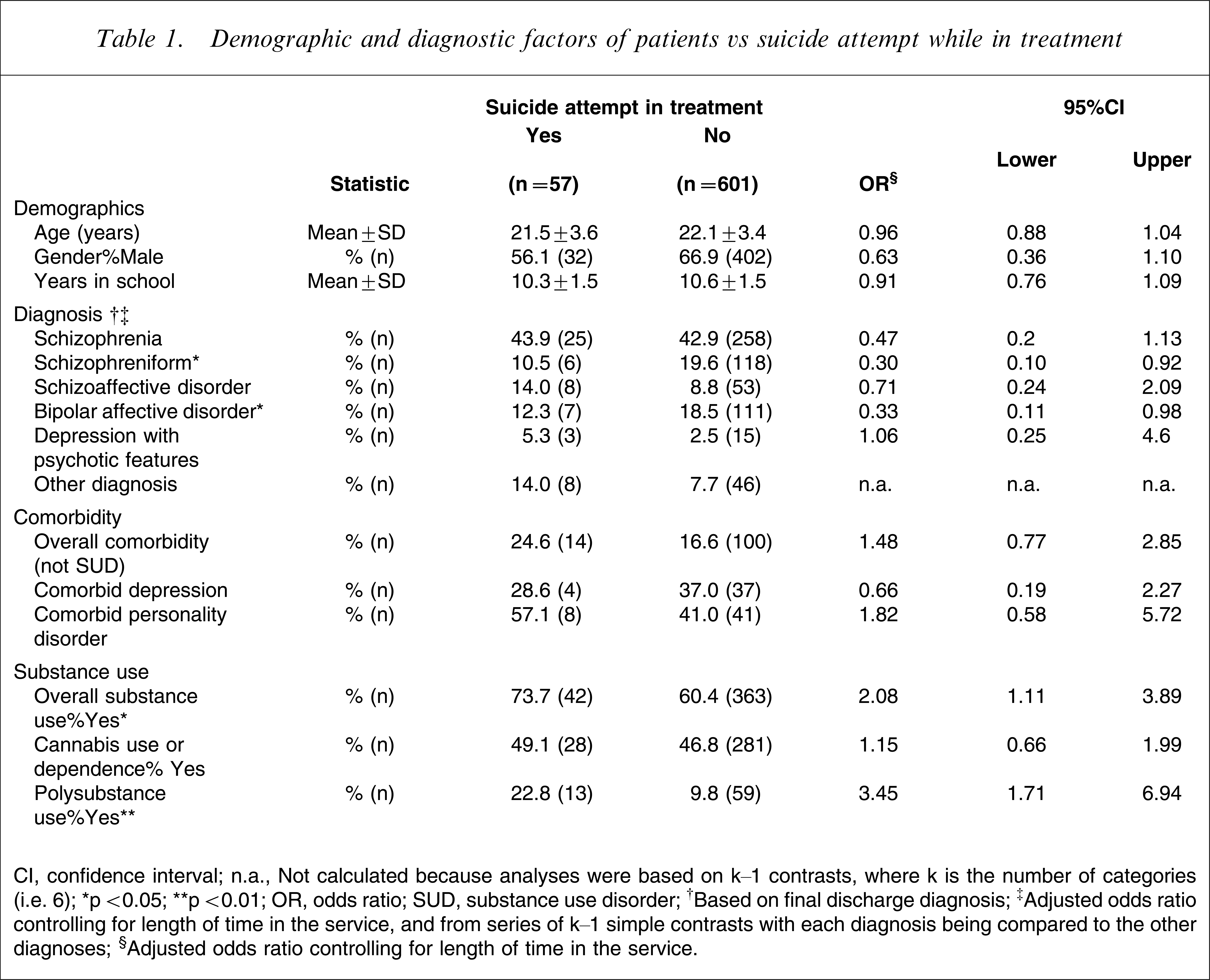
CI, confidence interval; n.a., Not calculated because analyses were based on k−1 contrasts, where k is the number of categories (i.e. 6); ∗p<0.05; ∗∗p<0.01; OR, odds ratio; SUD, substance use disorder.
†Based on final discharge diagnosis.
‡Adjusted odds ratio controlling for length of time in the service, and from series of k−1 simple contrasts with each diagnosis being compared to the other diagnoses.
§Adjusted odds ratio controlling for length of time in the service.
(2) Premorbid functioning, past psychiatric history, and life events (Table 2): (i) premorbid functioning, assessed using the Global Assessment of Functioning Scale (GAF) [19] and the Scale of Occupational and Functional Assessment (SOFAS) [20]; (ii) premorbid adjustment, assessed with one item of the Premorbid Adjustment Scale (PAS) [21] – the ‘social personal adjustment’ item; this was cross-validated by comparison with the GAF score and produced a satisfactory correlation (r=0.6) (only one item of the PAS was used because the complete scale is too complex to use to reliably extract data from files); (iii) duration of prodrome and DUP, assessed with the Duration of Untreated Psychosis Scale [22, 23]; (iv) past psychiatric diagnosis, defined on the basis of identification of file elements clearly suggesting the occurrence of an episode of psychiatric disorder in the past, whether treatment was provided or not; (v) exposure to previous trauma (life event), defined as a traumatic event occurring before initial treatment as documented in the medical records.
Premorbid functioning vs presence of suicide attempt
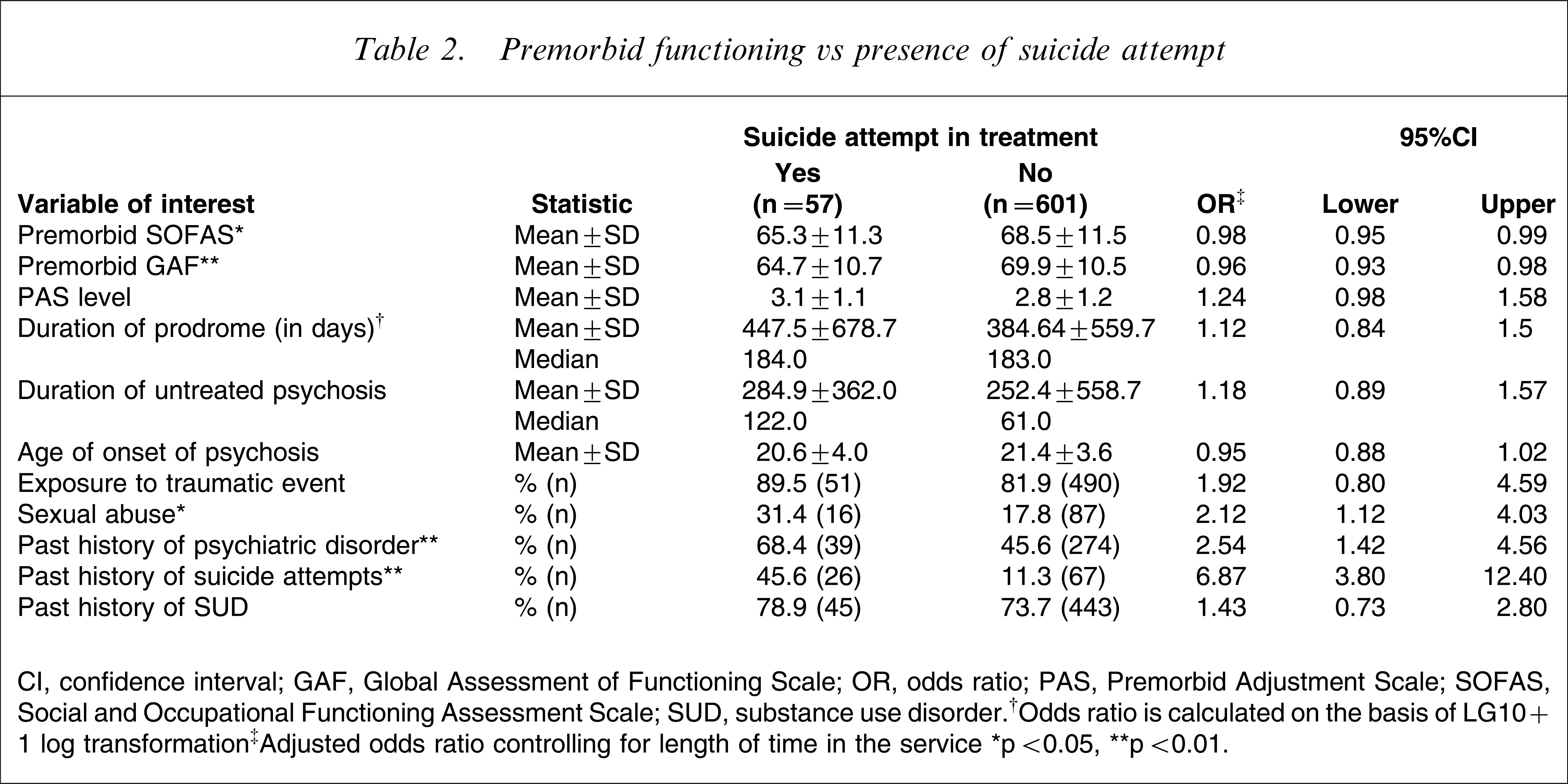
CI, confidence interval; GAF, Global Assessment of Functioning Scale; OR, odds ratio; PAS, Premorbid Adjustment Scale; SOFAS, Social and Occupational Functioning Assessment Scale; SUD, substance use disorder.†Odds ratio is calculated on the basis of LG10+1 log transformation‡Adjusted odds ratio controlling for length of time in the service∗p<0.05, ∗∗p<0.01.
(3) Symptomatic and functional level at baseline (Table 3): (i) severity of illness for non-affective psychosis, assessed with the Clinical Global Impressions–Severity of Illness scale (CGI-S) [24], and severity of illness for affective psychosis, assessed with the Clinical Global Impressions–Severity of Illness scale–Bipolar Illness (CGI-BP) [25]; (ii) level of functioning, assessed with GAF and SOFAS; (iii) level of insight: this was assessed qualitatively using the EPPIC intake mental state examination, administered at baseline, which contains a qualitative description of level of insight and was categorized into one of three groups: full, partial, or no insight; (iv) employment, defined according to the Tohen et al. Modified Vocational Status Index [26] as being part- or full-time employed or being an active student at school or university 4 weeks before entry in the service; and (v) living with family, which was also defined according to Tohen et al. as living with family with minimal or close supervision 4 weeks before entry in the service.
Characteristics at admission vs suicide attempt
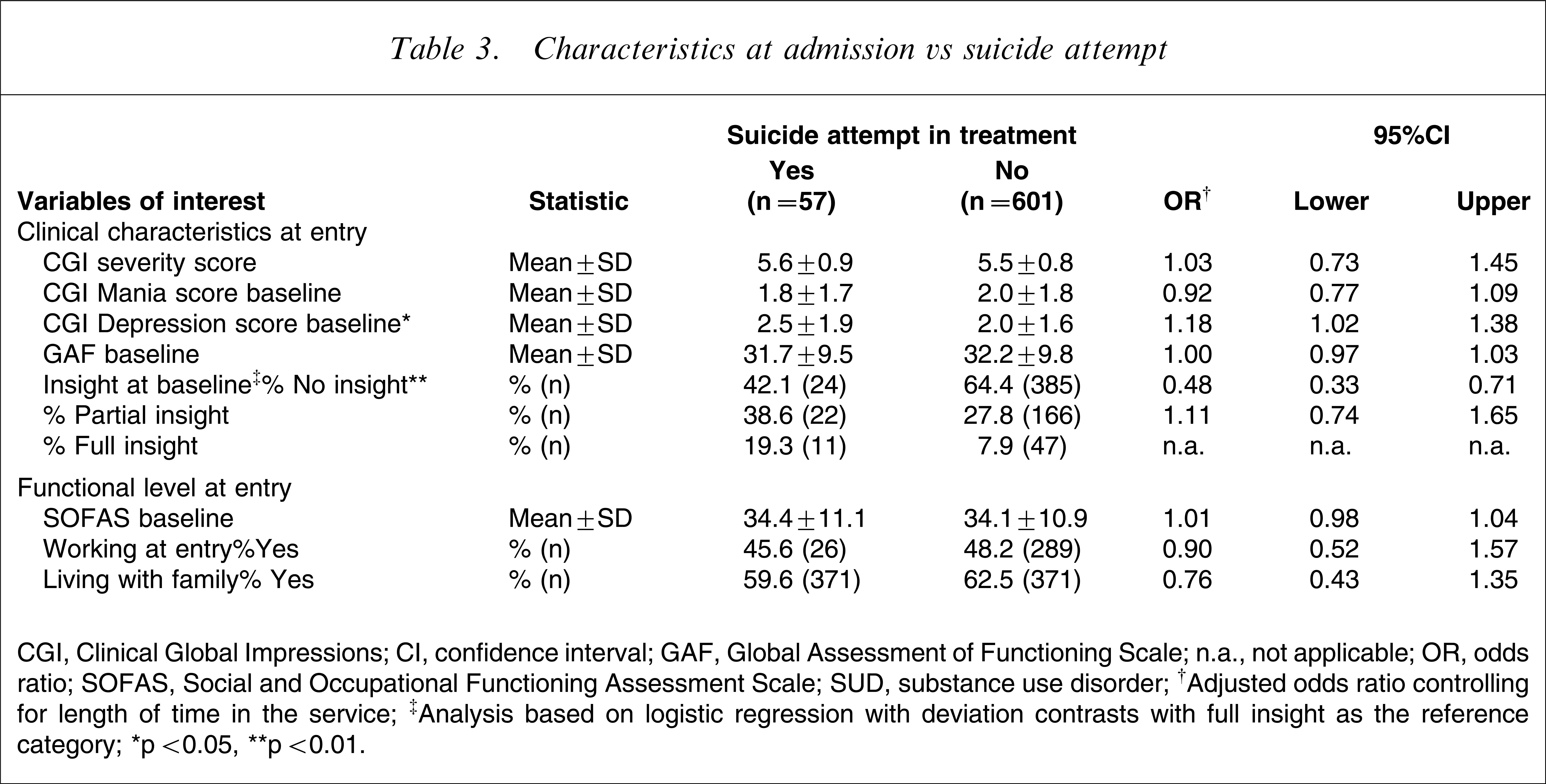
CGI, Clinical Global Impressions; CI, confidence interval; GAF, Global Assessment of Functioning Scale; n.a., not applicable; OR, odds ratio; SOFAS, Social and Occupational Functioning Assessment Scale; SUD, substance use disorder.
†Adjusted odds ratio controlling for length of time in the service.
‡Analysis based on logistic regression with deviation contrasts with full insight as the reference category.
∗p<0.05, ∗∗p<0.01.
(4) Treatment characteristics (Table 4): (i) admissions during treatment (separated into yes/no category and number of admissions); (ii) medication non-compliance, defined as failure to take medication for 1 week or longer (this definition was chosen because stopping medication for 1 week clearly indicates a problem as opposed to simply forgetting a dose); and (iii) course of SUD during treatment, categorized into no SUD, decreased or remitted SUD, or persistent SUD [14].
Treatment characteristics for the overall sample
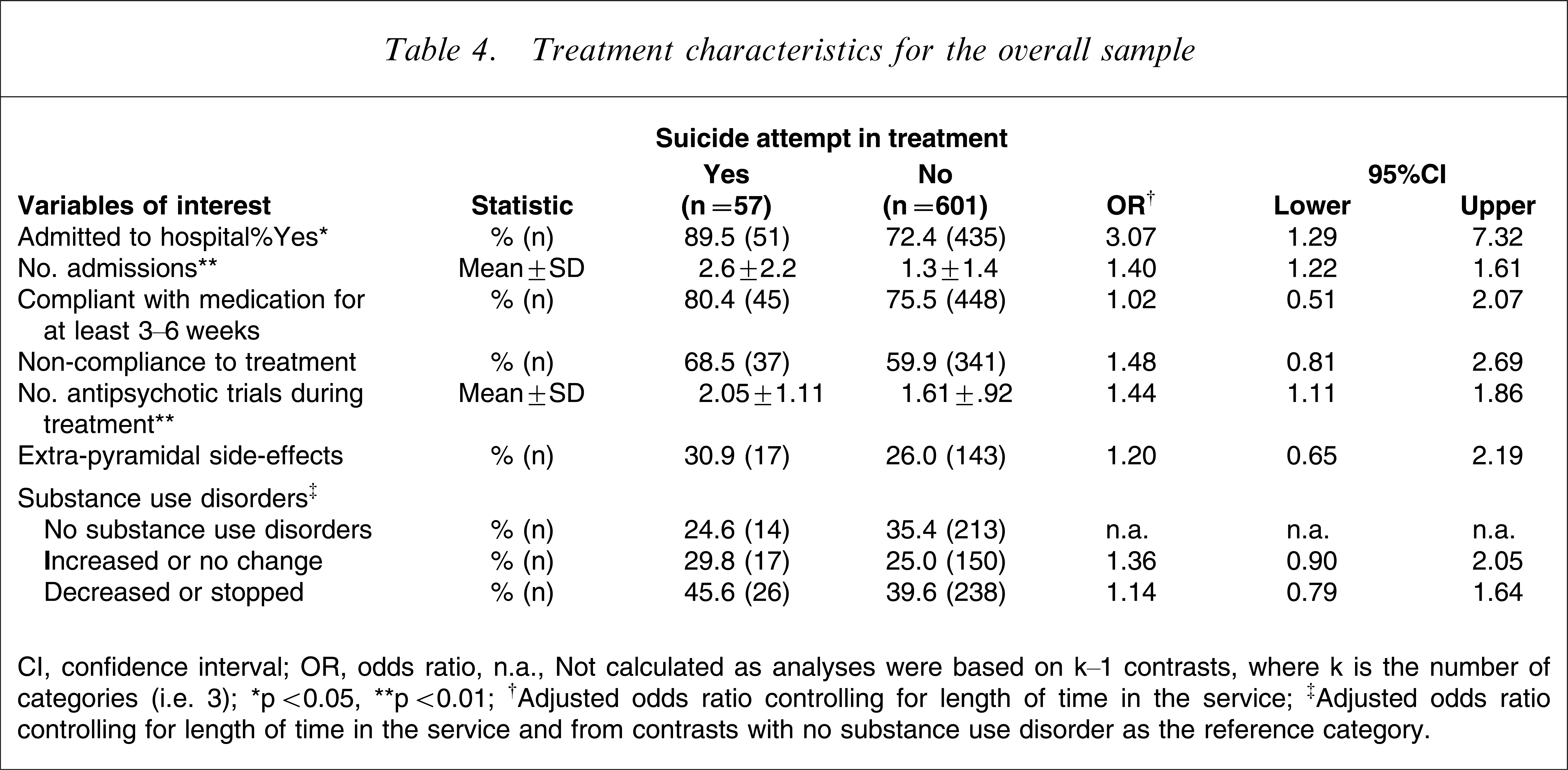
CI, confidence interval; OR, odds ratio, n.a., Not calculated as analyses were based on k−1 contrasts, where k is the number of categories (i.e. 3).
∗p<0.05, ∗∗p<0.01.
†Adjusted odds ratio controlling for length of time in the service.
‡Adjusted odds ratio controlling for length of time in the service and from contrasts with no substance use disorder as the reference category.
Statistical analysis
Descriptive statistics, that is, means, SDs, frequencies and percentages are presented for patients (based on n=661) who had or had not attempted suicide during treatment at EPPIC. For scale data that did not conform to the normal Gaussian distribution (e.g. DUP) log10 transformations (plus a constant such as one where 0 was observed in the data) were used.
A series of sequential logistic regression analyses were conducted with SA in treatment (yes/no) as the dependent variable, length of time in the service entered at the first step, and the predictor of interest was entered at the second step. Because length of time in service was variable for each patient it was necessary to covary for its effects. From these analyses, adjusted odds ratios (ORs, i.e. adjusting for time in service) and the 95% confidence intervals (CIs) of the adjusted ORs are reported. The Wald statistic (z; i.e. adjusted on the basis of the length of time in the service) is reported for significant predictors of SA. The adjusted ORs and Wald statistics are based on the 644 cases for which data on length of time in service were available.
A sequential logistic regression analysis (based on the Wald statistic) was performed to determine which demographic, premorbid, and clinical characteristics at entry best predicted SA during treatment. Only those variables that differentiated between those who did and did not attempt suicide in the preceding analyses (i.e. either significant t or χ2 or with a 95%CI of the OR that did not include the value of 1) were included in this model. Two-tailed level of significance with alpha set at 0.05 was used to judge the significance of these standardized residuals. Exact p are reported for most analyses (i.e. p=0.032), but for instances where tests statistics have a very low probability of occurring under the null hypothesis, p<0.001 was used for reporting probability.
Results
Suicide and suicide attempts
Six patients completed suicide during the course of treatment (0.9%). Of these five were male and their ages ranged from 20 to 27 years (mean=24.0 years, SD=2.8). Their diagnoses included: schizophrenia, schizophreniform, schizoaffective, delusional disorder, brief psychotic episode and major depressive episode with psychotic features.
The proportion of patients who made one or more SA either prior to entry into the service or during treatment with EPPIC (i.e. lifetime prevalence) was 18.8% (124/661). Ninety-three patients had a history of previous SA (14.3%, 93/652) with the majority of these patients having made one attempt (73.1%, 68/93). Fifty-seven patients made an SA during treatment (8.7%, 57/658), while the majority made only one attempt (84.2%, 48/57), nine (15.8%) made two or more attempts. Of the 93 patients who had made an SA prior to treatment, 26 (28%) went on to make a further attempt during treatment with EPPIC.
Demographic and diagnostic characteristics
Table 1 compares the demographic and diagnostic characteristics of patients who did and did not attempt suicide during treatment. No demographic characteristics were associated with SA. Patients with schizophreniform disorder (z=4.45, p=0.035) and with bipolar disorder (z=4.02, p=0.045) were less likely to have made an SA compared to those with other disorders. Patients who attempted suicide were more likely to have a comorbid SUD at entry to the service (z=5.25, p=0.022), in particular, polysubstance use or dependence (z=11.99, p=0.001).
Premorbid functioning, past psychiatric history and life events
Table 2 shows the premorbid functioning, duration of prodrome and DUP in patients with and without an SA. Patients who attempted suicide while in treatment were more likely to have poorer premorbid functioning, indicated by lower premorbid GAF (z=12.19, p<0.001) and SOFAS scores (z=4.39, p=0.036). It should be noted, however, that the group differences in these measures were quite small as indicated by the ORs, but the study was sufficiently powered to detect small effects. They were more likely to have experienced sexual abuse (z=5.26, p=0.022) and to have a past psychiatric diagnosis (z=9.80, p=0.002), most frequently depression. They were also more likely to have a past history of SA (z=40.83, p<0.001).
Discharge diagnosis was used for this analysis because of the known issues with instability of diagnosis [16]. Because discharge diagnosis would be expected to related to time in treatment (i.e. patients with a diagnosis of schizophreniform disorder were treated for a significantly shorter period than those with schizophrenia and schizoaffective disorder although no other differences were found), the relationship between discharge diagnosis and SA was also examined controlling of the effects of time in service in a multinomial regression. Again patients with schizophreniform and bipolar disorders were less likely to have attempted suicide.
Clinical characteristics at baseline
Clinical characteristics at entry are presented in Table 3. Those people who attempted suicide demonstrated greater severity of depressive symptoms (CGI–depression, z=4.63, p=0.031) than those who did not. Level of insight was also related to SA: those who attempted suicide were more likely to have full insight at entry than those who did not (z=13.81, p<0.001).
Treatment characteristics
Information on treatment characteristics can be found in Table 4. Overall, patients who attempted suicide had more hospital admissions (z=22.28, p<0.001) and a greater number of trials of antipsychotic medication (z=7.40, p=0.007).
Predictors of suicide attempt
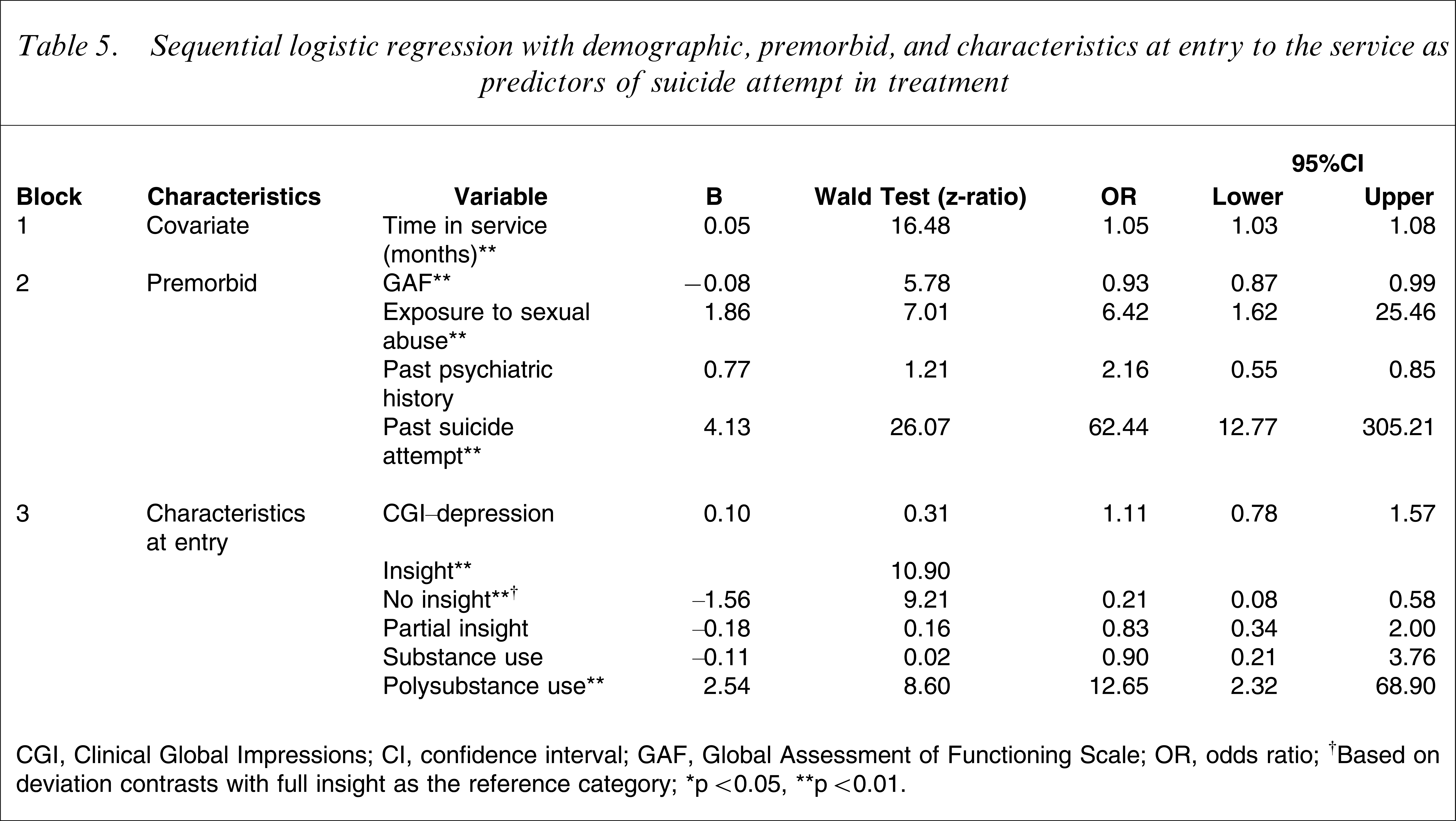
A sequential logistic regression analysis was conducted with months in service entered into the first block, premorbid characteristics entered into the second block, and clinical characteristics at entry (CGI–depression, level of insight, SUD at entry, and polysubstance use) entered into the final block. Note that 25 cases were removed because they were identified as outliers as determined by examination of standardized residuals (i.e. zresid outside ±3SDs), and diagnosis was not entered into the model because there were too few cases for some of the categories. With regard to premorbid characteristics, premorbid SOFAS was not included in the model because its high correlation with premorbid GAF (r=0.87) would result in the problem of collinearity.
At the first block the Nagelkerke R2 for time in service was minimal at 0.05 (χ2(1)=8.09, p=0.004). Addition of the premorbid factors into the second block increased the Nagelkerke R2 to 0.55 (χ2(5)=101.81, p<0.001). The addition of clinical characteristics at entry into the third block increased the Nagelkerke R2 to 0.66 (χ2(5)=22.86, p<0.001). This final model (Table 5) was a good fit (Hosmer and Lemeshow test, χ2(8)=1.56, p=0.992). Overall, correct classification of cases using this model was 96.8%. Accuracy of classification of patients who did not attempt suicide was 99.1%; correct classification of those who did attempt suicide was poorer at 53.8%. In the final model six variables were significant predictors of SA in treatment: (i) longer time spent in the service (z=16.47, p<0.001); (ii) premorbid GAF (z=5.78, p=0.003); (iii) past history of sexual abuse (z=7.01, p=0.008); (iv) SA in the past (z=26.07, p<0.001); (v) insight at entry (z=10.90, p=0.002); and (vi) polysubstance use at entry (z=8.60, p=0.003).
Sequential logistic regression with demographic, premorbid, and characteristics at entry to the service as predictors of suicide attempt in treatment
CGI, Clinical Global Impressions; CI, confidence interval; GAF, Global Assessment of Functioning Scale; OR, odds ratio.
†Based on deviation contrasts with full insight as the reference category.
∗p<0.05, ∗∗p<0.01.
Discussion
The current study provides information based on one of the largest epidemiological samples of FEP patients to date and, to our knowledge, exceeds previous studies examining suicide risk in this population. A further strength is that the study used a geographically defined area and a first contact for treatment as an incidence cohort, as opposed to a first hospital admission subject.
Key findings
The overall incidence of suicide was approximately 1% during 18–24 months, the SA rate prior to entry was 14.3%, and during treatment, 8.7%. These figures are high when compared to findings from other studies that have identified rates of suicide and SA to be between 0.3% and 0.4%, and 2.9% and 11%, respectively, over a 12 month follow-up period [3, 4] and the rate of SA to be 11.3% over a 2 year follow up period [5, 6]. Although these findings support those of other studies that have identified this population to be a high-risk group for suicidal behaviour [3, 27], they also underline that suicide and SA rates in FEP are substantially higher if epidemiological cohorts are studied because they allow for the inclusion of patients who would usually not consent to study participation.
The present data also support other studies that have identified previous SA and SUD, in particular polysubstance misuse, to be key predictors of suicide risk [3, 5]. Although previous SA was the best predictor of future risk (OR=45.54), less than half (28%) of those people who had attempted suicide prior to entry into the service made a further attempt during treatment. This is higher than has been reported by other studies conducted in specialist FEP services. For example, Addington et al. reported that none of the people who attempted suicide prior to entry into the service made a further attempt [28]. But it is lower than the rate reported in a non-specialist service by Warman et al. [2]. Such comparisons, however, are problematic because the current study assessed a representative incidence and not a hospital-based informed consent cohort. It is likely that the risk for suicide and SAs is higher in such non-selective samples because they include patients with more severe psychopathology, with more comorbid SUDs, in particular polysubstance misuse [14], or with longer DUP [13].
The present finding that poorer functioning, both prior to illness and at entry, is associated with SA is surprising and differs from other studies that have found high levels of premorbid functioning to be associated with risk [29]. A possible explanation for this difference is that patients with severe comorbid SUDs and thereby with a low functional level are normally not included in non-epidemiological informed consent studies [14].
Sexual abuse was found to be predictive of SA during treatment. This finding supports those of other studies that have found this to be a risk factor among people with SA in the general population and among people with schizophrenia [30]. There is conflicting evidence regarding the relationship between insight and suicide risk among people with schizophrenia [6, 31, 32]. Our study, however, supports others that have found a relationship between greater awareness of the illness and SA [33, 34].
Limitations
This was a retrospective audit of medical records, and related methodological limitations can included (i) poor-quality information recorded in the medical record; (ii) a lack of clinical experience among researchers extracting the data; (iii) the absence of strategies to ensure inter-rater reliability; and (iv) the validity of the data. All efforts were made, however, to reduce these limitations: (i) in EPPIC, treatment and documentation are systematized according to FEP guidelines; (ii) all medical records were exclusively assessed by two experienced psychiatrists, who have a thorough knowledge of the EPPIC service and treatment of FEP patients; (iii) inter-rater reliability was established for CGI, CGI-BP, GAF, SOFAS, PAS and insight [15] with very good reliability; and (iv) psychoses and baseline SUD diagnoses, assessed from medical records, were compared with prospectively evaluated SCID-I diagnoses from a subsample showing a good concurrent reliability. Another possible limitation was that the researchers were biased when examining exposure on the basis of already knowing the outcome status of the participant; but the files were assessed chronologically from the point of entry into EPPIC to the point of discharge. Thereby, all information on suicidal behaviour, past, baseline and the course of treatment variables were assessed blind to the final outcome of the patient. Similarly information relating to premorbid factors was recorded early in the files prior to the occurrence of suicidality during treatment. Further, this was assessed by the researchers prior to those variables relating to suicidality during treatment, again reducing the opportunity for bias. Further, the current study was unable to examine the timing of SA in relation to the course of illness or treatment because the date of SA was not recorded; nor could we examine psychopathology at the time of an attempt. Consequently we could not examine any possible associations between risk of SA and either positive or negative symptoms, or returning insight. Because of the methodology used we were not able to measure suicidal intent nor could we examine other variables known to be associated with suicide risk, such as hopelessness, or include more sophisticated measures of, for example, premorbid functioning. We recommend that further prospective studies of similarly large samples be conducted in order to address these limitations.
Clinical implications
There is debate about the efficacy of specialist early intervention services [35], but some studies have suggested that early intervention FEP services may help to reduce SA rates in this population [4, 10, 36]. Indeed the present data show lower rates of repetition of SA than might be expected, but this needs to be interpreted with caution, mainly because (i) previous prospective studies examining suicidal behaviour among people with schizophrenia over longer periods suggest that suicide risk decreases with time, and (ii) the reduced incidence of suicidal behaviour during service contact could be attributed to receipt of a service per se, hence demonstrating the value of services in general and not necessarily FEP services in particular.
Unlike among the general population we found no relationship between gender or employment and SA. We did find, however, that a history of child sexual abuse, lower levels of premorbid functioning, SUD, greater insight at entry, and in particular previous SA, are key predictors of further SA and therefore need to be taken into consideration when assessing risk and determining access to services. It has been noted that suicide risk is fleeting among this population and as a result may be underestimated by clinicians [11]; this can lead to inadequate risk assessment and management. Limitations in risk assessment among people with psychosis can also arise from a focus on psychotic symptoms at the expense of other stressors, which may trigger suicidal behaviour [37] for example, and, as shown in the current study, previous trauma.
A key risk factor for SA in treatment has been shown to be a previous SA. Examples exist of cognitive interventions that show encouraging results in their ability to reduce suicidal ideation and behaviour [11], and these are worthy of further investigation. Indeed, given that previous SA is the single greatest indicator of future risk, it would appear that developing and testing interventions designed to reduce suicidal behaviour may be our best bet at reducing suicide risk among this population.
We also found an association between SA and substance misuse at entry. This requires further investigation but suggests that successful treatment of SUD might contribute to reducing suicide risk. Thus our findings suggest that specialist early intervention services that can successfully treat people with comorbid SUD could play an important role in reducing SA among this population.
The fact that we also identified previous trauma and greater insight to be predicative of SA suggests that it is not necessarily clinical symptomatology that contributes to risk among people with FEP. Rather, factors such as poor functioning, a history of past trauma, substance misuse, awareness of the illness and a history of suicidal behaviour appear to contribute to SA, suggesting that it is also important to consider, and treat, these phenomena, perhaps with psychosocial interventions and psychoeducation, alongside symptomatology; something that the EPPIC service does as a matter of course.
The fact that insight is associated with risk and has been found to increase over time, often with the amelioration of positive symptoms [33], indicates the importance of remaining vigilant to suicide risk even once people appear to be making a good recovery. A system of regular screening of the entire patient population over the entire course of treatment, in addition to routine clinical assessment, has been shown to successfully identify those most at risk of suicide [11]. Given the high prevalence of suicide and SA among this sample, regular and thorough risk assessment and management are crucial. But targeting only those patients who appear to be at high risk has limitations. The poor specificity of risk factors associated with suicide can lead to the identification of large numbers of people who meet risk criteria but who do not attempt suicide, or, more worryingly, the focusing of resources on those who do meet the risk criteria at the expense of others who may still be at risk. For this reason broader measures that focus upon early access to services are important.
Footnotes
Acknowledgements
The study was supported by Eli Lilly Australia for special analysis of the comparison of olanzapine and risperidone in FEP (salary for 1 year for Dr Martin Lambert). Philippe Conus received a grant from the Leenaards Foundation, Switzerland. No further support was given. Analyses presented here were not published elsewhere. We thank Hok Pan Yuen, statistician in EPPIC, for database design.