
Abstract
Jumping from a height is a relatively uncommon way to commit suicide in Australia, accounting for only 75 (4%) of 1880 suicides in 2007 [1]. However, jumping from a height is a comparatively lethal way to attempt suicide, as it has been estimated that 60% of suicide attempts by jumping in Australia result in death [2].
There are several Australian studies that demonstrate an association between schizophrenia and suicide by jumping. In a series of 32 suicides by jumping in Adelaide, 38% were known to have schizophrenia [3], in Brisbane 45% of suicides by jumping from bridges had established diagnoses of schizophrenia [4], and in Melbourne, 37% of people who jumped from the Westgate Bridge had previously received treatment for schizophrenia [5]. In Sydney, 17 of 31 patients admitted to hospital after surviving a suicide attempt by jumping were found to be psychotic [6] and in a separate study from Sydney, people with schizophrenia were over-represented among the survivors of deliberate jumps that resulted in spinal cord injuries [7].
An association between schizophrenia and suicide by jumping has also been reported in a national sample from the United Kingdom [8], in other English studies [9] and studies from The Netherlands [10] and Switzerland [11]. Further, jumping from a height has been reported to be the most common method of suicide chosen by patients with schizophrenia in studies from the United States [12] and Hong Kong [13].
Suicide and attempted suicide by all methods are well-recognised sequelae of schizophrenia. A recent meta-analysis estimated that 5.6% (95% confidence interval, 3.7–8.5%) of all patients with schizophrenia commit suicide after the onset of their illness [14]. Although suicide can occur at any time during the patients’ illness, suicide is more common in the period following diagnosis and is less frequent in patients with a long history of schizophrenia [14–16]. It is also likely that the first episode of schizophrenia, defined as the period between the onset of psychosis and the initiation of effective treatment, carries an increased risk of suicide. The average duration of untreated psychosis in schizophrenia is over a year in high-income countries [17] and between 10 and 25% of first episode patients attempt suicide prior to initial treatment [18]. If serious suicide attempts are common after the onset of symptoms but prior to initiation of treatment, suicide could be an under-recognised cause of mortality in schizophrenia. Moreover, the extent of the contribution of schizophrenia to suicide mortality might not have been fully appreciated in studies that were based upon posthumous file reviews, or psychological autopsies.
We hypothesised that suicide by violent methods might be more common in untreated psychosis after considering the findings in two systematic reviews of other forms of violent behaviour in psychosis, which found 38.5% (95% confidence interval [CI] 31.1%–46.5%) of homicides [19] and 53.5% (95%CI 43.7%–63.2%) of reported cases of major self-mutilation [20] occurred during the first episode of psychosis.
It is not possible to determine exactly how many people commit suicide before treatment for psychotic illness because only a proportion will have been diagnosed prior to committing suicide. However, in a pilot study we found that approximately half of the survivors of violent suicide attempts admitted to an inner-city trauma centre were diagnosed with a psychotic illness and that 48.6% of those (95% CI 32.3–65.0%) had never received treatment with antipsychotic medication [18].
In this study we report the findings of a retrospective examination of the medical records of the survivors of suicide attempts by jumping from a height admitted to nine trauma centres in the state of New South Wales (NSW). A multi-centre study covering a long period of time was undertaken to obtain a large and representative sample. The main aim of the study was to determine the proportion of survivors diagnosed with a psychotic illness who had never received treatment with antipsychotic medication. If the rate of suicide attempts by jumping were similar before and after initial treatment, based on the incidence and prevalence of psychosis, the expected ratio of treated to untreated patients would be about 20:1.
There are no current figures for the incidence and prevalence of psychosis in New South Wales. Hence, we used the established estimates for the incidence and prevalence of schizophrenia from two recent systematic reviews and meta-analyses. McGrath and associates found that the pooled estimate of the incidence of new cases of schizophrenia worldwide was 21.9 per 100,000 per year and the pooled period prevalence was 440 per 100,000 population [21]. Hence, in any given year in a population with a typical incidence and prevalence of psychosis there will be about 20 times more people with an established psychotic illness than new presentations (440/21.9=20.1). Another way of conceptualising a risk prior to treatment for psychosis is to consider studies of the duration of untreated psychosis and the duration of the illness after treatment. The pooled estimate of the duration of untreated psychosis from population-based studies is about a year [17]. Less is known about the average duration of schizophrenia after initial treatment but it is generally considered to be a prolonged or lifelong condition. Hence, as schizophrenia usually begins in early adult life, even an average duration of untreated psychosis of over a year is a small fraction of the total duration of illness. If the risk of suicide attempts by jumping were the same throughout the course of illness, untreated patients would make up a small fraction of patients who survive suicide attempts.
The subsidiary aim was estimate the contribution of psychosis to suicide by jumping by calculating the proportion of all survivors of suicide attempts by jumping who were found to have a psychotic illness.
Methods
Data collection
An audit was conducted of the medical records of patients who survived a suicide attempt by jumping from a height and were admitted to hospitals that were designated trauma centres in inner Sydney (St Vincent's and Royal Prince Alfred Hospitals), the greater metropolitan area of Sydney (St George, Sutherland, Liverpool, Bankstown, Royal North Shore and Hornsby Hospitals) and in a rural area (Coffs Harbour Hospital). These hospitals serve approximately half the population of NSW.
We examined the medical records of patients classified as having attempted suicide by jumping from a height of more than 3 m. Patients who were reported to have jumped less than 3 m, who were prevented from jumping, or who were thought to have been pushed or to have fallen by accident were excluded.
The international classification of diseases (ICD) version 9 and version 10 codes (E957 and X-80, Suicide attempts by jumping from a height) were used to locate medical records in the 16 years from the beginning of 1992 to the end of 2007. In several hospitals the medical records were only readily available from the year 2000. We did not use the ICD coding to identify the psychiatric diagnosis because we aimed to estimate the proportion of all jumping survivors who were diagnosed with a psychotic illness.
OB and ML examined the files retrieved from St Vincent's, Sutherland and St George Hospitals without any disagreement about the presence of psychosis or whether the patient was believed by the treating team to have been in a first episode of psychosis (FEP). Data were collected at the remaining hospitals by DA, AG, NG, and ON.
The clinical diagnoses recorded in the medical records were used. Psychosis was defined as schizophrenia-spectrum psychosis, bipolar disorder, psychotic depression, or psychotic disorder associated with substance abuse. In schizophrenia-spectrum psychosis we included schizophrenia, schizophreniform disorder, schizoaffective disorder, delusional disorder and psychosis not otherwise specified. The terms first episode psychosis and untreated psychosis were used synonymously to describe patients with a psychotic illness who had never received treatment with antipsychotic medication, regardless of whether there had been previous remissions from symptoms without treatment. Hence, it is possible that a proportion of patients coded as first episode in this study might have recovered from an earlier episode of psychosis without medical treatment. Patients were referred to as ‘previously treated’ if they had ever received treatment with antipsychotic medication, irrespective of whether they had experienced a remission from symptoms as a result of treatment, or their degree of adherence to prescribed medication at the time of the suicide attempt.
All but a few medical records had entries by a trainee or specialist psychiatrist describing the mental state of the patient, as well as the entries by other treating doctors, nurses and social workers. The psychiatric diagnoses found in the notes were generally made using DSM classification terminology. Demographic data, the patients’ symptoms, substance use, the recorded psychiatric diagnosis and whether there was a history of previous psychiatric treatment was collected systematically using the same methods described in a prior study [18].
The seriousness of the patient's injuries we measured using the length of stay in hospital for surgical care and the Injury Severity Score (IS score) [22]. The IS Score uses a five-point scale (minor=1, moderate=2, serious=3, severe=4, critical=5) to grade injuries in six bodily regions and is calculated by the sum of the squares of the most severe injuries in any three bodily regions. Hence, scores for injured people range from 1 in the case of a person with a single minor injury to 75 in the case of a person with three or more critical injuries. The IS Score is predictive of subsequent mortality and has been used in previous medical record audits [18,23]. The IS Score has been found to be associated with other markers of injury severity such as the likelihood of treatment in an intensive care unit and the length of stay in hospital [24].
Permission to conduct the study was obtained from the St Vincent's Hospital Human Research Ethics Committee as the lead committee and confirmed by the relevant committees in each of the hospitals included in the study.
Statistics
Categorical variables were examined with an uncorrected chi-square test, or chi-square contingency table. Student's t-test was used to examine differences in the distribution of age and IS score. Mann–Whitney tests were used to compare the distribution of the height of jumps and length of hospital stay because of marked skewness associated with some patients with high jumps into water and patients with long length of stay in hospital, respectively. No correction was made to significance testing for multiple comparisons. All tests were performed in their two-tailed form using SPSS for Windows version 15.0.
Results
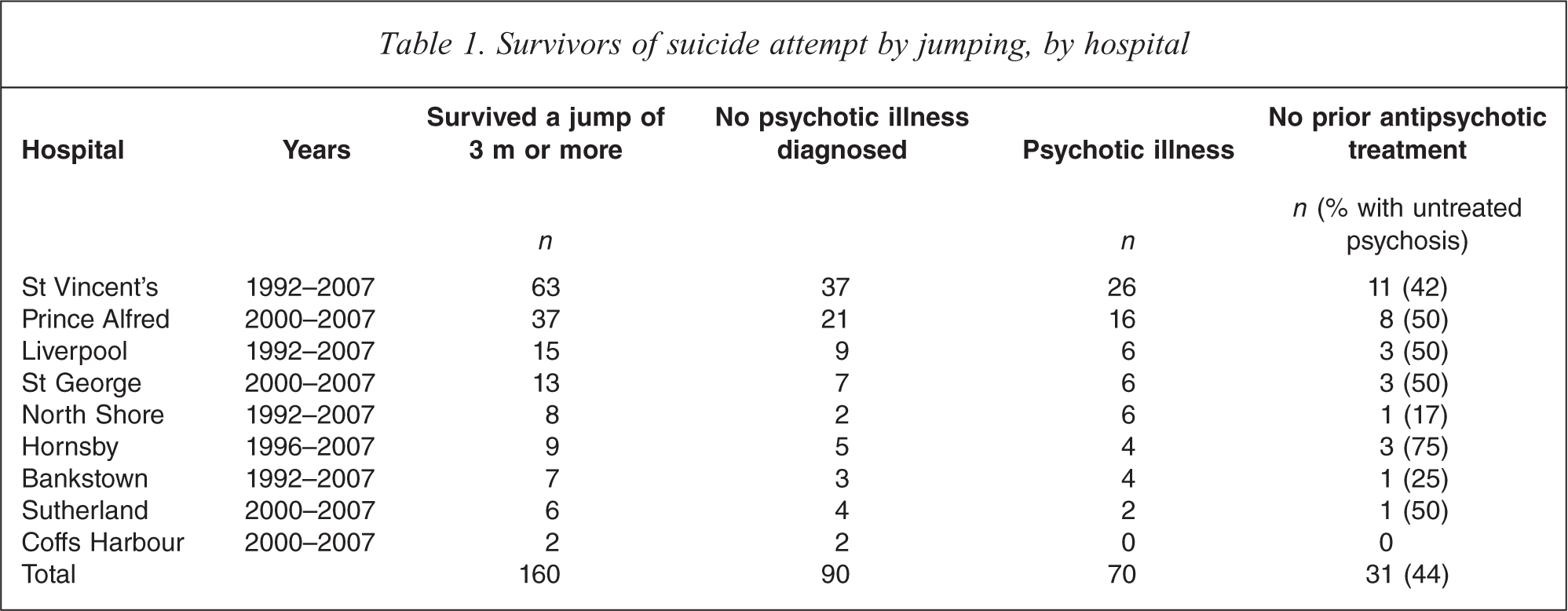
We located 160 survivors of suicide attempts by jumping from a height of more than 3 m by searching the discharge codes of the nine NSW hospitals (Table 1). One hundred of these were from two inner city hospitals (St Vincent's and Royal Prince Alfred Hospitals), whose catchment areas include a large number of high-rise buildings and the three commonly used jumping points (a seaside cliff known as The Gap and two high bridges, the Anzac Bridge and the Sydney Harbour Bridge).
Survivors of suicide attempt by jumping, by hospital
A total of 95 (59%) of the jump survivors were male and the average age was 34.4 years (SD 14.4 years). The average fall was 9.6 m, but the distribution of falls was skewed by a small number of falls from more than 50 m into water. The median fall was 6 m.
All 160 survivors were diagnosed with a psychiatric disorder, including 70 (44%) who were diagnosed with a psychotic illness (Table 2) and 90 who had other axis I or axis II diagnoses. Forty-nine of the 70 (70%) jumpers with psychotic illness were male, a significantly higher proportion than the 48 (53%) of the 90 jumpers not diagnosed with psychosis (χ2=4.582, df=1, two-tailed P=0.03). Jumpers with psychosis had the same mean age (34.4 years, SD 12.5) as those without psychosis (34.4 years, SD 15.9, t=0.0014, df=158, P=0.999). Those with a diagnosis of psychotic illness jumped from a median height of 8 m, which was significantly higher than the median height of 6 m by those without psychotic illness (Mann–Whitney U=3843, Z=−2.38, P=0.017).
Characteristics of survivors of suicide by jumping diagnosed with a psychotic illness
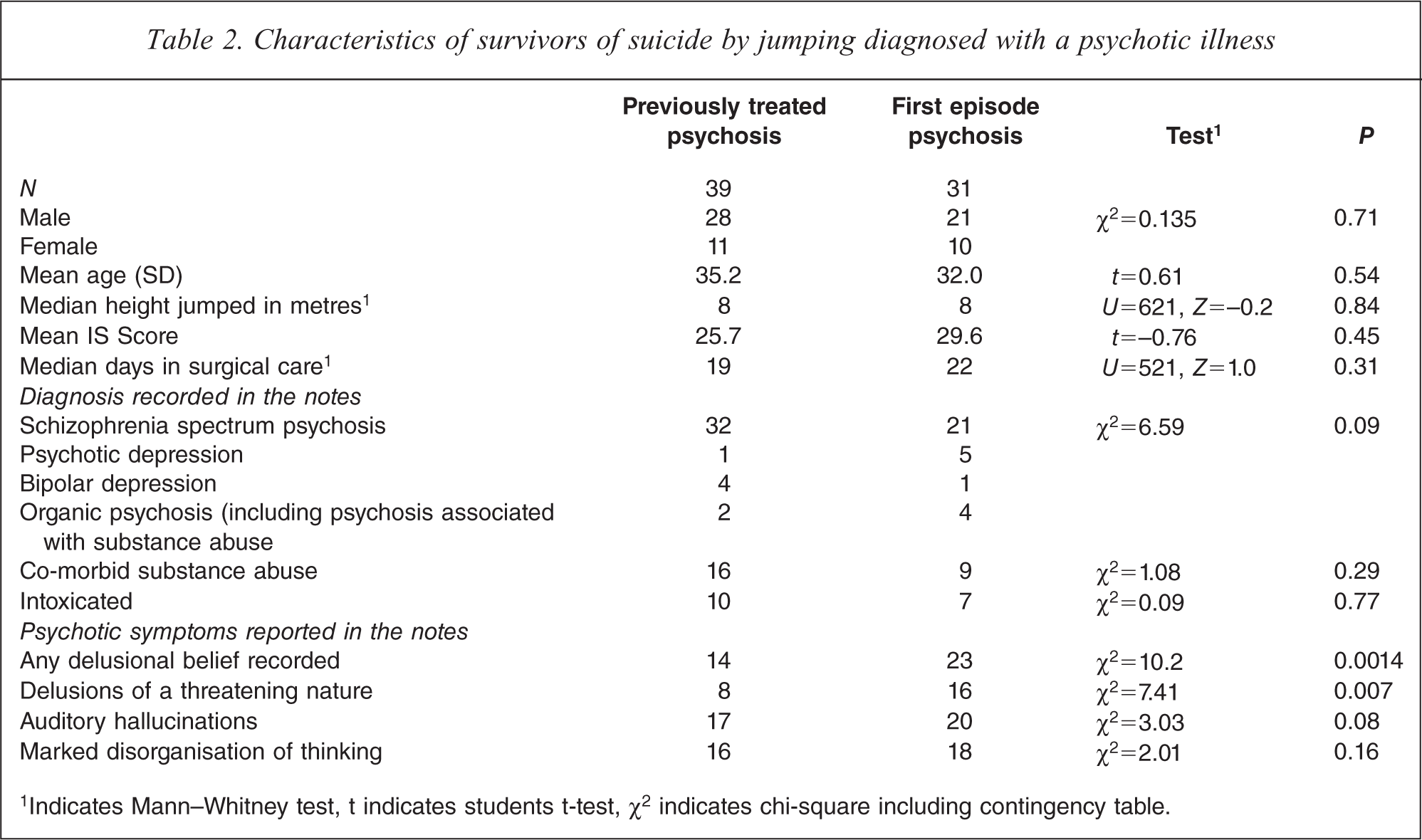
1Indicates Mann–Whitney test, t indicates students t-test, χ2 indicates chi-square including contingency table.
A schizophrenia-spectrum psychosis had been diagnosed in 53 (76%) of 70 patients with psychosis. Six (9%) were diagnosed with psychotic depression, five (7%) were diagnosed as being in the depressed phase of bipolar I disorder, four (6%) had a psychosis that was attributed to substance abuse, including a case of alcoholic hallucinosis and two (3%) had a psychosis that was secondary to medical conditions, including a case of psychosis in association with a primary brain tumour and an elderly patient with early dementia. A total of 31 of 70 (44%, 95% confidence interval [CI] 32–56%) were recorded as not having previously received treatment with antipsychotic medication and were classified as being in their first episode of psychosis. The 31 untreated patients included 21 of the 53 patients (40%, 95% confidence interval [CI] 26–53%) who were diagnosed with a schizophrenia spectrum psychosis.
The patients who were in first episode psychosis were non-significantly younger than those who had previously received treatment with antipsychotic medication. There were no significant differences between the groups of first episode and previously treated patients in the proportion of males, the height jumped, the psychiatric diagnoses, the patterns of substance use, the mean IS Score or the number of days in surgical care. The records of patients in first episode psychosis were more likely to include an account of a delusional belief, and delusions with personally threatening content (Table 2).
Entries in the medical records of 13 of the 31 patients in their first episode of psychosis described previous treatment for depression, either with antidepressant medication or counselling. Entries in a further three files indicated that the patients’ families or close friends were not aware of symptoms of psychotic illness prior to the suicide attempt, but believed the patients were depressed.
The psychiatric diagnoses recorded in the medical records of the 90 non-psychotic jump survivors were depressive disorders (41), alcohol dependence or abuse (27) other substance use disorder (10), adjustment disorder (4), dementia (2) and anorexia nervosa (1). Fifteen people were diagnosed with a personality disorder and two had an intellectual disability. One patient had human immuno-deficiency virus and another had epilepsy. Thirty-seven (41%) of the patients who were not diagnosed with psychosis were reported to be affected by alcohol or other drugs at the time of the suicide attempt, compared with 17 (24%) of those diagnosed with a psychotic illness (χ2=4.261, df=1, two-tailed P value=0.039).
Discussion
This study confirms the association between psychotic illness, especially schizophrenia, and attempted suicide by jumping from a height. One in five (19.4%) of all survivors of a suicide attempt by jumping had an undiagnosed and untreated psychosis. This finding indicates that a thorough psychiatric assessment should be performed on all the survivors of deliberate jumps in order to diagnose or exclude a psychotic illness. The finding of a significant occurrence of previously undiagnosed psychosis among survivors suggests that the true proportion of people who commit suicide by jumping in the course of a psychotic illness is higher than has previously been suspected or reported.
The finding that 44% of all survivors of suicide attempts by jumping have a psychotic illness confirms that psychosis is a particular risk factor for attempted suicide by jumping from a height. Patients with a psychotic illness make up a much smaller proportion of those who make serious suicide attempts by other means, including other highly lethal means such as by self shooting [6].
The study found that almost half of the survivors of a suicide attempt by jumping from a height who were found to have a psychotic illness had never received treatment for psychosis and were in their first episode of psychotic illness. Hence, the null hypothesis was rejected because we did not find a ratio of treated to untreated patients that was similar to 20:1 as would be expected from studies of the epidemiology of psychosis, if the risk of suicide was similar before and after treatment. Instead we found 44% of those with a psychotic illness had never received treatment. Assuming that there is no differential effect of phase of illness upon the likelihood of survival of a jump, this suggests that almost half the lifetime risk of suicide by jumping occurs before treatment, and that the risk of this type of suicide attempt in the first episode psychosis is of the order of 20 times higher than the annual rate after treatment. In this respect, attempted suicide by jumping, and quite possibly completed suicide by jumping is similar to homicide [19,26,27] and major self-mutilation [20,28] in psychotic illness.
Studies of completed suicide in psychosis are subject to selection bias because they generally only identify cases with a previously diagnosed and treated illness and usually exclude patients who died prior to a diagnosis. The finding that 16 of the patients who found to be in the first episode of psychosis after admission were thought to have depressive illnesses prior to attempting suicide raises the possibility that their suicide would have been attributed to depressive illness had they not survived. Hence, untreated psychosis might be an under-recognised cause of violent suicide.
A relationship between the patient's mental state and a preference for a particular method of suicide might explain why there is limited substitution of methods when access to methods of suicide is restricted. For example, patients with psychosis who have the idea to suicide by jumping might not be sufficiently organised to obtain a firearm or a lethal substance, or even to be able to hang themselves. Furthermore, most substituted methods of suicide, in particular by overdose of medication, are less likely to have a fatal outcome. It is widely believed that preventative measures that reduce access to popular jumping points reduce the total number of people who kill themselves by jumping [29]. The findings of this study support the proposal that restricting access to jumping sites might be particularly helpful in reducing suicide by patients with schizophrenia.
A limitation of this study was its naturalistic design, as the clinical information and diagnoses recorded in the notes were for patient care rather than for research. It is possible that the symptoms and circumstances of well-known patients may not have been recorded in as much detail as newly diagnosed patients. A second limitation was that we were unable to locate medical records from the period 1992–1999 in four of the nine hospitals. Based on the number of later cases from these hospitals, these could be expected to have reduced the sample size by approximately 25%. However, we have no reason to believe that the missing cases would have differed in a systematic way from cases occurring between 2000 and 2007. Thirdly, the entry of an ICD code for a suicide attempt by jumping could have been influenced by knowledge of the existence of a psychiatric diagnosis, reflecting potential reverse causality. Finally the extrapolation of our findings in jump survivors to jump-related suicide assumes that the likelihood of surviving a jump is similar between those with psychosis and other disorders. However, the significantly lower heights jumped by those who were not diagnosed with a psychosis suggests this is a cautious conclusion.
There has been little systematic research addressing the extent to which treatment is effective in reducing suicidal behaviour in schizophrenia [30]. There is growing evidence that early intervention programs implemented early in the course of schizophrenia are associated with a reduced suicide risk [31,32]. This study further suggests that early treatment of psychotic illness is likely to be an effective way of reducing suicide by jumping.
Footnotes
Acknowledgements
The authors would like to thank Janssen-Cilag for a grant in aid. GSM acknowledges support from NHMRC Program Grant 510135. NG receives support from NHMRC Program Grant 566529