
Abstract
In recent years, there have been growing concerns about increasing rates of youth suicide, particularly among males, in developed countries [1]. These trends have been clearly evident in both Australia and New Zealand with official statistics reporting rising rates of youth suicide since the 1970s [1–3]. International comparisons show that suicide rates for males aged 15–24 years in New Zealand (39.5 suicides per 100 000 in 1996) and in Australia (25.7 suicides per 100 000 in 1996) are at the higher range for selected developed countries [4].
These high rates of youth suicide have led both Australia and New Zealand to pay increasing public and policy attention to the issue of youth suicide. The present paper provides a summary of a larger review prepared for the NHMRC [5], and attempts to give an accessible overview of contemporary themes and issues concerning youth suicide.
Selection of studies
Evidence about risk factors for suicide and attempted suicide in young people was gathered from a review of published studies. In general, studies were included in the review if they met the following criteria: psychological autopsy or case–control studies published in English language journals or books, from the mid-1980s to early 1998, with a primary or predominant focus on youth (15–24 years), a sample size greater than 20 subjects and response rate of at least 50%. A more comprehensive account of data sources and the search strategy is given in Beautrais [5].
Methodological issues
A large, and somewhat uneven, research literature has focused on the issue of suicide since the seminal work of Durkheim in Le Suicide [6]. Despite the length of this tradition much research about youth suicide has suffered from a series of methodological limitations which include: (i) studies based on selected clinical samples; (ii) studies which lack comparisons of suicidal and non-suicidal subjects; (iii) a relative absence of longitudinal studies; and (iv) frequent failure to take into account key methodological issues relating to confounding, sample selection bias and measurement error. The net effect of these limitations is that many of the findings and conclusions drawn in this area are subject to considerable methodological uncertainty. Despite this, as will be shown later, there is generally quite good convergence of findings about risk factors and life processes that contribute to suicidal behaviour in young people.
Aims
The aims of this review are to summarise research literature and current knowledge about risk factors for suicide and suicide attempts in young people. The review examines the contribution to risk of suicide and attempted suicide of the following factors: (i) social and family risk factors; (ii) individual and personality factors; (iii) mental health factors; (iv) precipitating circumstances and stressful life events; and (iv) environmental and contextual factors.
Results
Social and family risk factors
A large volume of research has examined the extent to which suicidal behaviours are related to a range of social, economic, family and related factors (for reviews, see [7–9]). The present review groups social and family factors into a series of risk factor domains and, for each domain, summarises the findings of studies which have examined associations between these factors and risks of suicidal behaviour, with studies restricted to those which compared rates of risk factor exposure in those with suicidal behaviour and in non-suicidal control subjects. Where case–control studies have provided odds ratio (OR) estimates of the strength of association between a risk factor and suicide or suicide attempt risk, these ORs are quoted. The evidence for each risk factor domain is considered below, for both suicide and attempted suicide.
Social disadvantage
Most studies which have examined associations between measures of social disadvantage and suicide or suicide attempt have reported increased risk of suicidal behaviour among individuals from socially disadvantaged backgrounds characterised by such features as low socioeconomic status (SES), limited educational achievement, low income and poverty [10–19]. For example, odds of suicide were found to be twice as high among low SES individuals compared to those from more advantaged backgrounds [10], and risk of suicide was shown to be elevated among young people who had dropped out of school (OR = 5.1) or were not at college (OR = 7.8) [11].
Parental separation or divorce
A large number of studies have reported that young people from families with histories of parental separation or divorce have increased risks of suicide [20,21] or suicide attempt [14,17,19,22–34]. Suicide victims, for example, have been found to be more likely than control subjects to come from a ‘non-intact family of origin’, with this finding persisting after adjustment for demographic factors (OR = 1.9) [20]. Adolescents who made suicide attempts were reported to be more likely to have experienced at least three changes of parent figures from age 5 years to 15 years (OR = 2.6) compared with those not making attempts [17].
The weight of evidence suggests that while parental loss as a result of divorce and separation is associated with increased risks of psychopathology (including suicidal behaviour) in young people, loss of a parent by death is not. Parental loss by death, and by separation or divorce, may have different antecedents and potentially different consequences [35].
Parental psychopathology
A series of studies has suggested that rates of suicide and suicide attempt tend to be increased among young people with histories of exposure to parental psychopathology including depression, substance use disorders and antisocial behaviours [11,21,24,26,36–43]. Higher rates of depression (OR = 11.0) and substance abuse (OR = 10.4), for example, have been reported among families of suicide victims compared with families of control subjects [21].
Family history of suicidal behaviour
There is consistent evidence to suggest that a family history of suicidal behaviour is associated with increased risks of suicide [11,21,36–38,44] and suicide attempts in young people [26,28,42,43,45]. Of particular interest are two recent case–control studies: A study of 120 teenage suicide victims and 147 control subjects found increased rates of family history of suicidal behaviour among suicide victims (OR = 4.6) [11], and a comparison of adolescent suicide victims and control subjects found higher rates of suicidal behaviour among first and second degree relatives of the suicide victims [21].
Marital discord
A series of studies has found elevated rates of suicide attempt among young people aged 15–24 years exposed to parental discord and disharmony [23,30,40,46–48]. For example, young people who made serious suicide attempts reported higher rates of parental discord than control subjects, with this association persisting after control for confounding family factors (OR = 3.1) [23]. In addition, young people have often reported that parental discord was a precipitating factor for their suicide attempt [36,49–51]. However, parental discord has not been reported to be associated with adolescent completed suicide [52].
History of physical and/or sexual abuse during childhood
A series of studies has examined associations between histories of sexual or physical abuse during childhood and risk of suicide or suicide attempt. Those studies which have focused on suicide as the outcome of interest have tended to produce somewhat inconsistent conclusions, with these inconsistencies probably arising from the small and selected samples of suicides which have been studied [36–38]. However, a larger number of studies have examined associations between suicide attempt risk, and both physical abuse and sexual abuse, with generally more consistent findings.
Rates of suicide attempt appear to be elevated among young people exposed to childhood physical abuse [23,24,28,33,47,53–59]. The studies reviewed reported ORs between exposure to physical abuse and attempted suicide which ranged from 1.9 to 6.5 (median = 5.7), suggesting relatively strong associations between exposure to physical abuse and suicide attempt risk. However, since it is likely that physical abuse tends to occur in families in which children are exposed to a range of other adverse experiences, the association between physical abuse and suicide attempt risk needs to be adjusted for the effects of potential confounding factors. Beautrais et al. conducted one of the few studies which have controlled for confounding factors and found that, while physical abuse was associated with increased risk of suicide attempt (OR = 13.4), this measure was not a significant predictor of suicide attempt when other factors (including, particularly, childhood sexual abuse) were taken into account [23].
Rates of suicide attempt are also increased among young people with histories of childhood sexual abuse [23,24,28,53–58,60–65], with these studies yielding OR estimates between sexual abuse and suicide attempt risk which range from 1.5 to 11.8 (median = 4.8). Further, the severity of childhood sexual abuse appears to be related to suicide attempt risk, with those who report sexual abuse involving intercourse being 12 times more likely to make suicide attempts than those who do not report such abuse [62]. These differences persisted even after control for a number of prospectively collected measures of confounding factors.
These findings linking childhood sexual abuse with later suicidal behaviour are consistent with the weight of evidence from a range of studies which have examined adjustment among those who have experienced sexual abuse in childhood or adolescence. These studies have suggested both concurrent suicidal behaviour for those who are sexually abused in childhood, and generally poor mental health outcomes for those with histories of sexual abuse (for reviews of this literature see [66–68])
Parent–child relationships
There are consistent suggestions that impaired parent–child relationships, poor family communication styles, and extremes of high and low parental expectations and control are associated with increased risk of suicide and suicide attempt among young people [11,16,19,21,23,29,40,47,48,69–78]. OR estimates between parent–child relationship measures and suicide attempt risk range from 1.4 to 3.6 (median = 2.6), and two studies have reported that exposure to impaired parent–child relationships is associated with increased risk of suicide [11,21].
Summary
The preceding evidence suggests that a wide array of adverse social and family factors (spanning social disadvantage, parental separation or divorce, parental discord, impaired parent–child relationships, parental psychopathology, and exposure to childhood physical and/or sexual abuse) appear to be associated with increased risk of suicidal behaviour. This evidence has usually been interpreted as suggesting a causal process in which exposure to childhood and family adversity increases an individual's vulnerability to later psychopathology and adjustment difficulties, with this increase in turn being reflected in increased rates of suicidal behaviour.
The view that family factors play a causal role in influencing vulnerability to suicide has recently been challenged in a review by Wagner [9] who concluded that, in the majority of studies, investigators had failed to show that exposure to family adversity was temporally antecedent to the onset of suicidal behaviours. Wagner's critique is sound to the extent that well-designed longitudinal research examining the relationship between prospectively measured family factors and later suicidal behaviour would assist in drawing causal inferences. To date, there have been relatively few prospective studies in this area [17,40,46,74,79–84]. Wagner's conclusion is, however, limited by a failure to recognise that temporal sequencing is only one of a series of criteria that may be used to draw causal inferences [85,86]. Other relevant criteria include evidence of dose–response, replication, and theoretical plausibility. When this broader range of criteria is taken into account, the weight of evidence clearly points to the view that the associations between family factors and suicidal behaviour are likely to be causal.
Individual and personality factors
A further set of risk factors for youthful suicidal behaviour comprises individual and personal factors including genetic factors, neuroendocrine and biologic factors and personality and temperamental factors. Research findings in these areas are reviewed below.
Genetic factors
Higher rates of suicidal behaviour have been reported in families of young people with suicidal behaviour than among families of control subjects, suggesting that genetic factors may play a role in suicidal behaviour [11,20,21,26,28,36,42,43,45,87]. This view is also supported by twin and adoption studies which have shown: (i) an elevated risk of suicide in the biological relatives of adoptees who die by suicide compared with non-suicidal adoptees [88]; (ii) higher rates of suicidal behaviours in monozygotic twins compared with dizygotic twins [89–92]. These twin data suggest that genetic factors may be related to suicide risk, with this genetic contribution largely reflecting a genetic predisposition to the psychiatric disorders associated with suicide.
Neuroendocrine and biologic processes
There is increasing interest in the extent to which neuroendocrine and biological processes may influence suicide risk. This interest has largely focused around the extent to which low or below average levels of the neurotransmitter 5-hydroxytryptamine (serotonin 5-HT) and/or its metabolite 5-hydroxyindoleacetic acid (5-HIAA) are associated with increased risks of depression and suicidality [93–100]. Although the processes by which serotonin and suicidal behaviour might be linked remain unclear, there have been recent suggestions that low levels of serotonin might be associated, principally, with poor impulse control rather than suicidality per se [101,102], and that this linkage might best explain the serotonin dysregulation observed in both suicidal and violent behaviour.
Personality factors
Certain personality traits have often been cited as predisposing factors in suicidal behaviour. Studies have examined associations between risk of suicide and suicide attempt in young people and the following traits: low self-esteem; external locus of control; hopelessness; introversion; neuroticism; impulsivity; recklessness; aggression and impulsive violence; passive, dependent, oral, obsessive and hysterical personality traits; state and trait anxiety and anger; an aggrieved attitude; social inadequacy; and diminished cognitive ability to evaluate the consequences of one's actions [7,21,25,46,47,70,72,103–120].
While there is much interest in the relationships between the extensive array of personality and cognitive traits above and the risk of suicidal behaviour in young people, the available research evidence for any specific trait is, generally sparse and often equivocal. This arises from several major methodological difficulties in examining the contribution of personality traits to suicide attempt risk. These difficulties include the arguments that: (i) self reports of personality characteristics may be contaminated by current mental state factors (including, in particular, depression); (ii) personality characteristics might be less clearly apparent among young people than in older individuals [121]; (iii) among young people, it may be difficult to differentiate, diagnostically, between behaviours which represent mental disorders and those which are emerging personality characteristics, and to determine the extent of comorbidity between these two sets of risk factors. There is a strong need for all of these issues to be addressed in further research using rigorously designed controlled and longitudinal studies.
Sexual orientation as a risk factor for suicidal behaviour
There have been repeated claims that rates of suicidal behaviour are elevated among gay, lesbian and bisexual young people [64,122–126]. Specifically, it has been argued that, because of a series of social processes centring around homophobic attitudes, gay, lesbian and bisexual youth are exposed to serious social and personal stresses that increase their likelihood of suicidal behaviour. These claims were originally strongly articulated in a paper prepared for the US Secretary's Task Force on Youth Suicide, in which Gibson suggested that gay youth were 2–3 times more likely to attempt suicide than other young people and may comprise up to 30% of all suicides [123]. Unfortunately, these claims were not based on adequate evidence, leading researchers to comment critically (see, for example [127]).
However, in the last 3 years, a number of studies have emerged which have compared rates of suicidal behaviour in samples of gay, lesbian and bisexual youth and heterosexual control groups. In general, these studies have found an increased risk of suicide attempt among gay, lesbian or bisexual individuals [122,128]. However, studies examining linkages between sexual orientation and death by suicide have not found this association [127,129,130]. The failure to find linkages with suicide may be due to the fact that ascertainment of sexual orientation following suicide is more difficult than such assessment among those who survive suicide attempts.
Although the emerging evidence suggests clear associations between gay, lesbian and bisexual orientation and suicide attempt risk, studies in this area have faced difficulties, centring around relatively small samples of gay and lesbian youth, and issues relating to the ascertainment of sexual orientation. Because of these problems, there is a strong need for the development of a series of well-designed studies of large samples to replicate, extend and validate the evidence reviewed above.
Mental health factors
There is overwhelming evidence to suggest that mental disorders (in particular, affective disorders, substance use disorders and antisocial behaviours) play a major role in the aetiology of youthful suicidal behaviour. Evidence to support this conclusion has come from: (i) psychological autopsy studies which have examined the prevalence of mental disorders among those who have died by suicide, and (ii) case–control or longitudinal investigations which have contrasted rates of disorders between individuals with suicidal behaviours and non-suicidal subjects. The evidence from these studies is reviewed below.
Psychological autopsy studies
Psychological autopsy studies consist of interviews conducted with relatives, friends and health professionals about an individual who has died by suicide, in order to obtain information and to reconstruct a life-history for that person. These studies have invariably shown high rates of mental disorder among youth dying by suicide. For example, a review of seven psychological autopsy studies concluded that the better-designed studies with more stringent and defined diagnostic criteria consistently suggested rates of mental disorder among adolescent suicide victims that were in excess of 90% [131].
Controlled studies
The limitation of the psychological autopsy approach is that, although it clearly illustrates the high rate of mental disorder among those who die by suicide, it fails to estimate how many times more likely those with mental disorder are to attempt suicide or die by suicide than those without mental disorder. This information has been provided by a growing number of case–control studies, which have estimated ORs between the presence of mental disorder and the risk of suicide or suicide attempt. These studies have shown that those with mental disorder are at markedly increased risk of suicidal behaviour. The evidence from these studies is reviewed below for each category of mental disorder and for suicide and suicide attempt.
Affective (mood) disorders
A large number of studies have reported that young people with affective disorders have markedly increased risks of suicide, with OR estimates ranging from 11.0 to 27.0 (median = 12.0) [13,36,44,52,118,132], and of suicide attempt (OR estimates ranging from 7 to 28, median = 13) [14,40,83,133–135].
Substance use disorders
Substance use disorders are also linked with suicide in young people, with a series of studies yielding OR estimates ranging from 3.3 to 10.7 (median = 5.5) [13,52,118,136]. Similar trends have been found for suicide attempt behaviour and aspects of substance abuse, with studies yielding ORs ranging from 1.7 to 11.5 (median = 5.4) [14,40,83,133,137].
Antisocial behaviours
Significant associations have been reported between measures of antisocial behaviour (including conduct disorder, oppositional defiant disorder and antisocial personality disorder) and risk of suicide and suicide attempt in young people [14,40,41,52,118,133,137,138]. Studies of the association between antisocial behaviours and suicide attempt, for example, have reported ORs, which ranged from 3.5 to 17.3 (median = 5.4).
Anxiety disorders
Increased risks of suicide and suicide attempt have been reported for young people with anxiety disorders [14,40,83,118,133]. However, when the association between anxiety disorders and risk of suicidal behaviour has been controlled for mood disorder, anxiety disorders have not made significant contributions to suicide risk, suggesting that the observed association between anxiety disorders and suicidal behaviour may reflect mood disorders that are frequently comorbid with anxiety disorders [118,133].
Psychosis
A series of case–control studies has failed to produce consistent evidence of linkages between psychotic disorders (including schizophrenia) and suicide and suicide attempt behaviour [13,139,140]. However, it is likely that the inconsistencies in these studies reflect small sample sizes and the fact that psychotic disorders occur infrequently in the general population. Psychological autopsy studies suggest that only a small minority of young people aged less than 25 years who die by suicide have psychotic disorders, including schizophrenia [52,118,141,142]. In these studies, prevalence estimates of schizophrenia range from 0 to 4%.
It should be noted, however, that while psychotic disorders make a relatively small contribution to overall suicide rates, within the populations of those with psychotic disorders risks of suicidal behaviour are high with estimates suggesting that up to 10% of individuals with schizophrenia die by suicide [143–145].
Multiple diagnoses
High rates of comorbid or multiple mental disorders have been reported in young people dying by suicide [13,36,44,118,142,146–148]. Among these studies, estimates of the prevalence of comorbidity range from 43% to 70% (median = 45%). Similar trends are found in studies which have examined comorbidity and suicide attempt risk in young people, with these studies reporting ORs which range from 2.1 to 40.4 (median = 8.1) [17,39,83,134,149], and one study demonstrating steadily increasing risks of serious suicide attempt with increasing number of disorders [39].
Summary
The preceding review clearly shows that three disorders (affective disorders, substance use disorders and antisocial behaviours) are the major psychiatric conditions associated with suicidal behaviour. Of these disorders, affective disorders consistently emerge as being most frequently and strongly associated with suicidal behaviours, with ORs between affective disorders and risk of suicidal behaviour typically exceeding 10. However, it is also clear that risks of suicidal behaviour increase dramatically among those with multiple and comorbid disorders.
These findings are supported by the results of a series of studies that suggest that: (i) those dying by suicide or making suicide attempts often have a history of psychiatric care [36,38,44,118,135,142,148,150–154]; and (ii) those with histories of suicide attempt behaviour have markedly increased risk of further suicide attempt behaviour or suicide [14,21,36,118,133,134,142,151,152].
Stressful life events and adverse life circumstances
Evidence from psychological autopsy studies and controlled studies suggests that: (i) among those making suicide attempts there is a high rate of exposure to recent stressful life events and adverse circumstances; and (ii) exposure to such events is associated with significant increases in rates of suicidal behaviours. The evidence from these sources is reviewed below.
Psychological autopsy studies
Psychological autopsy studies of young people who have died by suicide have reported that, in the majority of cases, an identifiable stressful life event preceded the suicide attempt. Estimates of the proportions of suicides preceded by stressful life events have ranged from 70% to 97% (median, 90.5%) [131,154–156].
Controlled studies
The conclusions drawn from psychological autopsy studies are generally confirmed by the results of case–control research which has compared rates of exposure to adverse life events among those dying by suicide or making suicide attempts, and control subjects.
These studies have reported elevated rates of a range of life stresses (most commonly, interpersonal losses and conflicts, and disciplinary or legal crises) in the period preceding suicide [11,13,36,44,132,157], and suicide attempts [16,22,24,43,46,76,158–161]. For example, OR estimates of the association between life events and suicide attempts range from 1.3 to 15.8 (median = 4), suggesting that recent stresses make a moderate contribution to suicide attempt risk.
Unemployment
Recently, considerable attention has been given to the role of unemployment as a life event that provokes suicidal behaviour (see, for example [162]). There are two approaches by which this issue has been studied:
Time series studies
Linkages between unemployment and suicide have been examined through time series studies that use historical data to examine whether changes in employment rates in the population are associated with changes in suicide rates over the same period. The results of time series analyses have been equivocal, with some studies suggesting linkages between changing rates of unemployment and others failing to find this association [162–169]. A recent review examined associations between time trends in unemployment and in youth suicide in European data, and found that, contrary to the hypothesis that rising unemployment rates lead to increased youth suicide, during the early 1980s unemployment rates rose sharply for young males, but the rate of suicide fell at this time [7].
Controlled studies
Relationships between exposure to unemployment and suicidal behaviours have been examined in case–control and longitudinal studies. This research has included two studies of suicide in general population samples, which found higher rates of suicide among unemployed compared with employed subjects [170,171]. However, both studies failed to control for social, economic and personal factors associated with employment status. In contrast, controlled studies of attempted suicide have concluded that unemployment and suicide attempt risk are not significantly related after control for confounding factors [23,172,173].
Summary
There is considerable evidence to suggest that suicidal behaviours in young people are frequently preceded by exposure to stress and personal adversity, notably, interpersonal losses and conflicts, and legal or disciplinary crises. However, there is generally clear recognition that the life events that precede youth suicide occur commonly among adolescents and may act as precipitating factors for suicidal behaviour only when they occur in individuals who are vulnerable to suicidal behaviour.
There are at least three explanations for the observed linkages between adverse life events and risk of suicidal behaviour:
It could be suggested that the apparent linkages reflect a methodological bias that arises because: (i) the occurrence of suicidal behaviour sets in train an ‘effort after meaning’ to explain the suicidal behaviour, and (ii) this, in turn, leads to an over-reporting of adverse life events.
The higher rate of life events among those with suicidal behaviour may reflect the presence of other (confounding) adverse factors associated with suicidal behaviour.
Exposure to adverse life events may make a causal contribution to suicidal behaviour in one of two ways: (i) suicidal behaviour may reflect an attempt to resolve, solve or avoid personal difficulties and stress associated with life event exposure; or (ii) exposure to life events may make an indirect causal contribution to suicidal behaviour by increasing levels of psychiatric symptoms (and notably depression) that, in turn, lead to an increase in suicidal behaviour.
Environmental and contextual factors
A large volume of research has examined the extent to which suicidal behaviours are related to a wide range of environmental and contextual factors. This evidence is summarised below.
Suicide contagion and suicide clusters
It has long been recognised that suicidal behaviours tend to be contagious and to cluster (for reviews, see [174,175]). Suicide clusters are defined as the occurrence in time and geographical space of an aggregation of suicides (usually, three or more) which is greater than the number of suicides which would be expected on the basis of statistical prediction [176,177]. Suicide clusters tend to occur predominantly among adolescents and young adults. The relative risk of suicide for those exposed to an index suicide has been shown to be 2–4 times higher in 15–19-year-olds than in older age groups [177].
While the incidence of clusters of suicide is thought to be rare (approximately 5% of all youth suicides [178,179]), the extent of clustering involving suicide attempt behaviour has not been well explored.
The extent of imitative suicidal behaviour, which follows an index suicide, may, in part, be related to the perceived social status and attractiveness of the index person, and to the amount of publicity given to the story in the news media [177]. However, it is unlikely that imitation alone accounts entirely for the decision of subsequent suicides to imitate a prior suicide. It appears likely that subsequent suicides are characterised by a prior history of difficulties and/or mental disorder, which renders them vulnerable to suicidal behaviour [180].
Media influences
A growing body of evidence suggests that media publicity may encourage suicidal behaviour. This evidence includes findings from a range of international studies which generally (but not invariably) suggest that media publicity about suicide issues, whether in the form of fictional, documentary or news reports, may provoke suicidal behaviour among those individuals vulnerable to such behaviour [181–188]. In addition, there are concerns that exposure by young people to particular styles of (‘rock/metal’) music and to the large volume of suicide information, stories, games and discussion groups on the Internet may also encourage suicidal behaviour [189,190].
Despite considerable evidence suggesting that various forms of publicity may increase suicide risk, the interpretation of this evidence remains controversial. In particular, since studies tend to have been based on correlational designs and aggregate population data, direct evidence linking media coverage of suicide to increased suicidal behaviour is still lacking. Nonetheless, the frequency with which media stories of suicide have been associated with apparent, and otherwise unexplained, transitory increases in suicide rates would appear to provide reasonable support for the hypothesis that publicity about suicide may have unanticipated effects among vulnerable individuals who may model their behaviours upon the accounts of suicide presented by the print media and television.
In addition, publicity about suicide may increase suicide risk by ‘normalising’ the concept of suicide in the population, so that taboos, which have previously surrounded suicide, may be lessened, and suicide may be more widely perceived as a common and acceptable option for people under stress [191].
Access to methods of suicide
A large volume of research has considered the factors which influence choice of method of suicide, and the extent to which restricting access to specific methods of suicide might reduce method-specific and total suicide rates.
In Australia, the most common methods of suicide among youth are hanging, firearms, and motor vehicle exhaust gas. Self-poisoning is a common method for female suicide and, overwhelmingly, the most common method of serious suicide attempt with non-fatal outcome. During recent decades, youth suicides by hanging and motor vehicle exhaust gas have increased and the use of firearms and overdose has declined [192,193]. These observations suggest that suicide rates by particular methods are amenable to change. Options for reducing suicidal behaviour in the Australian context by restricting access to means of suicide, and the feasibility of such approaches, have been reviewed by Cantor et al. [192]. One of the major difficulties in attempting to reduce suicide by restricting access to means of suicide lies with the fact that the single most common method of youth suicide is hanging for which there are no clear accounts of effective interventions.
Rural, remote and urban factors in suicide
The issue of whether an excess of suicide deaths occurs in rural, as opposed to urban, regions has been recently examined in Australia and other countries [193–198]. In Australia, rates of suicide for young males are higher for those from rural and remote areas than for urban residents [193], with these rates being almost twice as high in ‘remote’ areas compared to capital cities. However, increased rates of suicide among rural youth have not been observed in all Australian states [195], and the reasons for this remain unclear.
As young males living in rural or remote regions are more likely than urban residents to use firearms as the means of suicide [194,196,197], interest in urban/rural suicides has tended to focus upon differential rates of access to firearms. This focus has tended to obscure investigation of the extent to which urban and rural youth suicides may vary with regard to a range of other risk factors.
Factors which may protect against suicide
While many studies have examined risk factors for suicidal behaviour, relatively little research has focused upon identifying individual, family and community factors which may protect against the development of suicidal behaviour in young people, although there is emerging interest in this issue. To date, studies in this area have tended to focus on the role of various social supports (for example, family cohesion or belonging to a social peer group) in buffering the impact of exposure to known risk factors for suicide [43,198].
It has been claimed that good social skills mitigate against the development of depression in young people [199,200], and it might be expected that such social competency would protect young people against suicide also.
There are suggestions that both marriage and parenthood protect against suicide (see, for example [201,202]). However, there is a need to establish whether these factors are differentially protective for males and females, and for different age groups.
At an individual level there are suggestions that those with poor coping skills and problem-solving deficits have higher risk of suicidal behaviour [49,203]. This implies that adequate or good coping skills and problem-solving behaviours, and a range of other individual and adaptive skills, may protect against suicide. Other protective factors have been suggested, including positive and life-affirming beliefs and values, high self-esteem and holding attitudes and moral values against suicide [204,205]. The role of these skills in protecting against suicidal behaviour, and the extent to which they may be encouraged and enhanced, particularly among at-risk young people, requires further evaluation.
Conclusions
A review of research studies of youth suicide reveals a number of recurrent methodological limitations, including a relative lack of controlled studies, the use of small samples, and the use of selected clinical samples. Despite these methodological problems, examination of the literature yields a generally consistent and coherent account of the risk factors and life processes that lead to suicidal behaviours. The account that emerges suggests that suicidal behaviours in young people are frequently, although not invariably, the end-point of adverse life sequences in which multiple risk factors combine to encourage the development of suicidal behaviours. The risk factor domains that may contribute to this process include:
Social and economic disadvantage, with those reared in socially disadvantaged families or subject to economic adversity being at increased risk of suicidal behaviour.
Childhood and family adversity, with those reared in families characterised by such features as marital dysfunction, impaired parenting, child abuse and parental psychopathology being at increased risk of suicidal behaviour.
Individual vulnerabilities, with those having certain personality characteristics and, perhaps, genetic backgrounds or biological predispositions, being at increased risk of suicidal behaviour.
Mental disorders, with those with disorder (particularly mood disorders, substance use disorders and antisocial or conduct disorders) being at increased risk of suicidal behaviour. In addition, those with comorbid or multiple disorders, and histories of suicide attempt behaviour and/or psychiatric care have increased risk of suicidal behaviour.
Exposure to stressors and adverse circumstances, with those exposed to adverse life event experiences (particularly, interpersonal losses and conflicts, and legal or disciplinary problems) being at increased risk of suicidal behaviour.
In addition, the influence of the risk factors above may be modified or changed by social, cultural and contextual factors that may act to encourage or discourage the development of suicidal behaviours in young people.
One way of viewing these findings is suggested by the conceptual model in Fig. 1. This model assumes that there are a series of correlated sets of factors (social background, family factors, psychiatric and personality factors) which act as broad determinants of an individual's vulnerability to suicidal behaviour. These vulnerability factors influence both an individual's susceptibility to mental illness and his or her level of life event exposure. In combination, these sets of risk factors make both direct and indirect contributions to an individual's risk of suicide or suicide attempt. Although this model is clearly only approximate, it has the advantage of providing an overview, and a preliminary means of synthesising, the large array of research data which has now been amassed in this area.
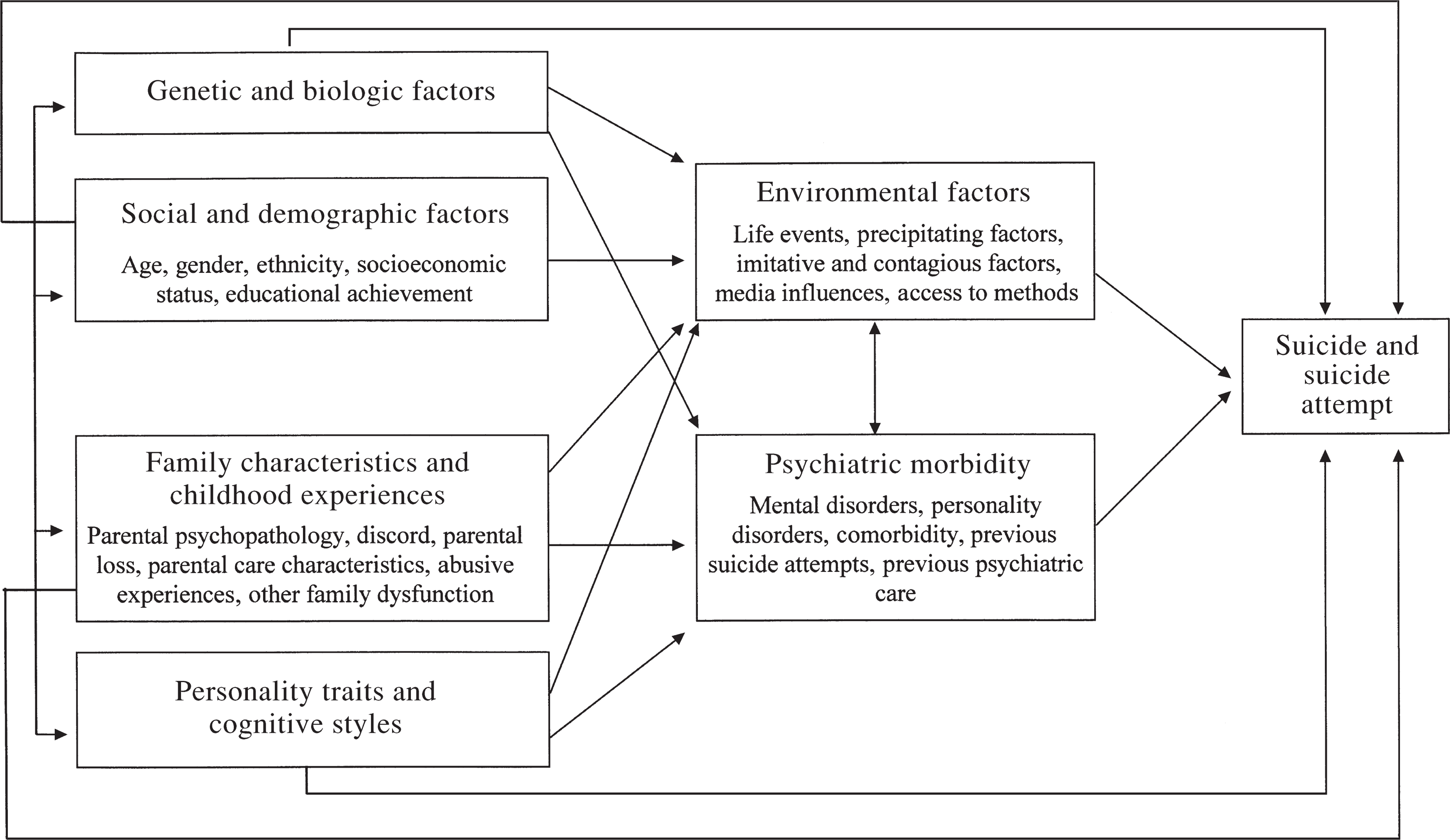
Conceptual model of domains of risk factors for suicide and suicide attempt
A further issue is whether the aetiology of youth suicide differs from that of suicide attempt. In general, the present review suggests considerable similarity and overlap between risk factors for both outcomes suggesting, as might be expected, that the factors implicated in suicide attempts are similar to those associated with suicide. These conclusions tend to support those authors who have proposed a dimensional model of suicidal behaviour in which the spectrum of suicidal behaviours ranging from suicidal ideation to death is influenced by a common set of risk factors with the extent of the individual's risk factor exposure determining the extent of their suicidal behaviour [7,206].
Clinical implications
This review suggests the need for investments in youth suicide prevention to focus on the broad domains of variables implicated in the development of suicidal behaviour, with a particular emphasis of these approaches being on youth mental health and the factors that contribute to the development of mental health problems in young people. In this area the following strategies have been suggested:
Improved public understanding of mental health issues and the efficacy of treatment, and increased appreciation and acceptance of appropriate treatment for mental health problems by both the public and by youth with such problems.
Education programs for those who work with young people that focus on increasing awareness of the extent of affective and substance use disorders, and in particular, providing guidelines for the better recognition, treatment and management of depression in young people.
Provision of adequate specialised mental health services for young people.
Development of appropriate follow up and treatment of youth known to be at high risk of further suicidal behaviour, including those who have made previous suicide attempts, and those with psychotic disorders.
Development of general mental health programs, which aim to foster good mental health skills among young people.
It should be noted, however, that, given the strong associations demonstrated in this review between individual psychopathology and suicide attempt risk, it is very unlikely that reductions in suicidal behaviour will occur unless there are corresponding changes in rates of psychiatric disorders within adolescent and young adult populations. This is clearly a very demanding agenda to meet since: (i) this field is still a long way from reaching a clear specification of the types of interventions, structures and policies which may reduce adolescent risk of psychopathology; and (ii) current evidence suggests that, in nearly all developed societies rates of mental health problems and psychosocial disorders have been increasing among young people.
Gaps in knowledge
While the available evidence provides, in broad outline at least, an account of the common risk factors and life processes that encourage suicidal behaviour, there still remain many gaps in knowledge about this complex human problem. For almost all of the risk factor domains and issues reviewed above, further and better designed research is needed to clarify key issues. Many of these difficulties could be addressed by the development of larger and more systematic studies of suicidal behaviour in young people, including: (i) the development of one or more large case–control studies of suicide and attempted suicide among young people; and (ii) the establishment of one or more large longitudinal studies of Australian youth to examine the risk factors and life pathways associated with the development of a range of mental health outcomes in adolescence and young adulthood. However, the primary justification for such longitudinal research should be its ability to inform about the spectrum of adolescent and youth problems, rather than having a specific focus on the issue of suicidal behaviours only.
Case–control and longitudinal research is likely to produce the greatest return in understanding the aetiology of youth suicide, nonetheless, there is considerable justification for supporting smaller and more specialised studies looking at specific aspects of this problem.
Finally, it should be borne in mind that aetiological research provides only one perspective on the issue of youth suicide, and that there is a need to balance investments into understanding aetiology with parallel investments in both the areas of service utilisation and preventive program development and evaluation.
The major value of risk factor research may be that it provides a basis for resolving the often competing and sometimes highly emotive claims about factors and processes that lead young people to consider suicide and to attempt to take their own lives. This process, in turn, will lead to a clearer articulation of, and justification for, prevention strategies and policies.
Acknowledgement
The preparation of this review was supported by the National Health and Medical Research Council (NH&MRC).