
Abstract
Social functioning includes the capacity for and the breadth of social relationships [1]. Deficits in social functioning have been considered one of the key features of schizophrenia and have been correlated with social adjustment [2–4] and social skills [5]. For many patients, poor social functioning was more debilitating than was the presence of positive symptoms, and tended to be resistant to pharmacotherapy after the illness had become chronic [6,7].
Additionally, abnormal social functioning has been reported not only in patients with schizophrenia but also in individuals at ultra-high risk (UHR) for psychosis. The ‘prodromal period’ or ‘at-risk mental state’ has been characterized by lack of stability and a course of increasing psychopathological and social impairments preceding the onset of frank psychosis [8–10]. Previous retrospective studies have reported that social withdrawal was a pervasive and frequently presented symptom in those at UHR for psychosis [11–13]. Recently, Addington et al. [14] suggested that the degree of social functioning deficits in those at UHR for psychosis was similar to that of individuals with first episode psychosis and patients who had experienced multiple episodes of schizophrenia. Another study found that people at UHR were more socially impaired than were those with genetic high risk [15]. These results suggest that the social functioning of those at UHR for psychosis is already impaired before the onset of the illness. Yung and colleagues [9] reported that a Global Assessment of Functioning (GAF) score of 50 or below was associated with conversion to psychosis at a 12 month follow up period, and added this to the three criteria for the identification of UHR. However, to our knowledge, no study has investigated the longitudinal course of social functioning in subjects at UHR for psychosis. Prospective studies on the social functioning of individuals who later develop psychosis are important for exploring the potential risk markers for conversion to psychosis. If deficient social functioning is a risk marker for psychosis, UHR subjects who do and do not subsequently develop psychosis may follow different courses in terms of social functioning. Thus far, no follow-up studies have tested this assumption among individuals at UHR.
Improvement in social functioning has been an important target for the cognitive rehabilitation of patients with schizophrenia [16,17], in view of its impact on coping with daily living. Atypical antipsychotic medications have also been associated with the enhancement of social skills in patients with schizophrenia [18]. However, no longitudinal study to date has explored the impact of pharmacological treatment on the social dysfunction of UHR subjects, although pharmacotherapy has been suggested as having protective or delaying effects on the transition to psychosis [19,20].
The present study aimed to prospectively investigate the longitudinal course of social functioning in subjects at UHR for psychosis and to identify differences in social functioning between UHR subjects who did (‘converters’) and those who did not (‘non-converters’) develop psychosis. We hypothesized that social dysfunction would be more evident in UHR individuals than in healthy controls at baseline and that converters would show more deterioration in social functioning as time passed, as compared to non-converters. Additionally, we examined the effects of pharmacotherapy on the course of social dysfunction. The relationship between clinical symptom severities and the changes in social functioning were also assessed.
Materials and methods
Participants
In total, 70 subjects at UHR for psychosis who visited the Seoul Youth Clinic between November 2004 and October 2009 were initially enrolled. The UHR subjects were assessed using the Comprehensive Assessment of At-risk Mental States (CAARMS) [10,21] and met at least one of three following UHR criteria: (i) attenuated psychotic symptoms, (ii) brief limited intermittent psychotic symptoms, and (iii) trait and risk factors. Of these, 57 subjects participated in the longitudinal study. The remaining 13 did not agree to participate in the longitudinal study or did not complete the initial questionnaire. UHR subjects who participated in this study were followed up regularly (weekly to monthly) for more than 1 year (mean: 2.8 years; range: 1–5.2 years). A total of 58 healthy controls were also recruited from the community via newspaper advertisements. They were screened using the Structured Clinical Interview for DSM-IV, non-patient version (SCID-NP) [22]. Exclusion criteria for all subjects were as follows: any lifetime diagnosis of psychotic illness, substance dependence, seizure disorder, history of head injury or medical illness with documented cognitive sequelae, or mental retardation. The healthy controls were screened with the additional exclusion criterion of having any first- or second-degree relatives with a psychotic disorder.
The present study was approved by the institutional review board at Seoul National University Hospital, and written informed consent was obtained from all subjects after the procedures had been fully explained.
Evaluations
Social Functioning Scale
The 79-item Social Functioning Scale (SFS) was administered to assess level of social functioning [1]. The scale was completed at intake and after 1 year. The SFS has been widely used to evaluate the most relevant areas of social functioning in schizophrenic patients and has shown adequate reliability, validity and sensitivity. In this study, the Korean version of the SFS was used to assess the seven areas of functioning: (i) social engagement/withdrawal, (ii) interpersonal behaviour, (iii) prosocial activities (frequency of activities that imply social interaction), (iv) independence–competence (competence in activities of daily living), (v) independence–performance (frequency of performing activities of daily living), (vi) recreational activities (solitary leisure activities), and (vii) employment/occupation. Each subscale score was standardized and normalized using a T-transformation to a mean of 100 and a standard deviation of 15, with the unemployed schizophrenia group as the reference population [1].
Clinical evaluations
The severity of the clinical symptoms of UHR subjects was assessed with the CAARMS and the Positive and Negative Syndrome Scale (PANSS) [23] at intake and every 6 months. Besides the CAARMS and the PANSS, the clinician-administered Hamilton Depression Rating Scale (HAM-D) [24] and the Hamilton Anxiety Rating Scale (HAM-A) [25] were administered to measure the severity of current depression and anxiety, respectively. All participants were also evaluated according to their GAF to assess overall functioning, and the Korean version of the Wechsler Adult Intelligence Scale (K-WAIS) [26] was administered to estimate intelligence. Family histories of psychotic disorders were determined using the Family Interview for Genetic Studies [27].
Statistical analysis
Comparisons of three groups in terms of demographic variables were performed using analysis of variance (ANOVA) with Tukey's post hoc analysis or a chi-square test. A t-test was used to compare the converter and non-converter groups with regard to clinical variables. ANOVA was also employed to evaluate the variables measured by the SFS at baseline. A repeated-measures, 3 (group) × 2 (time: baseline and 1 year follow up) ANOVA was used to compare changes in SFS scores during the follow-up period. We used logistic regression analysis to examine the discriminative power of social functioning at intake on the introduction of treatment with psychotropic medications. Pearson correlation analysis with Bonferroni's correction (p < 0.0029) was performed to examine the relationship between clinical variables and SFS scores.
Results
Demographic and clinical characteristics
The demographic and clinical characteristics of the participants are presented in Table 1. During the 1 year follow-up period, 13 of the 57 UHR subjects converted to full psychosis according to operationalized criteria for the onset of psychosis [10]. The DSM-IV diagnoses for the 13 converters were as follows: schizophrenia, paranoid type (n = 6); schizophrenia, undifferentiated type (n = 3); and bipolar disorder with psychotic features (n = 4). The numbers of UHR subjects who converted to psychosis during the first 12 months, between 12 and 24 months, and after 24 months were six, four, and three, respectively. The mean time to conversion from inclusion in the study was 14.3 months. We found no significant differences among healthy control, non-converter, and converter groups in demographic characteristics such as sex, age and years of education. We also found no significant differences between non-converter and converter groups in any of the clinical scales at baseline.
Demographic and clinical characteristics of subjects at ultra-high risk for psychosis and healthy controls
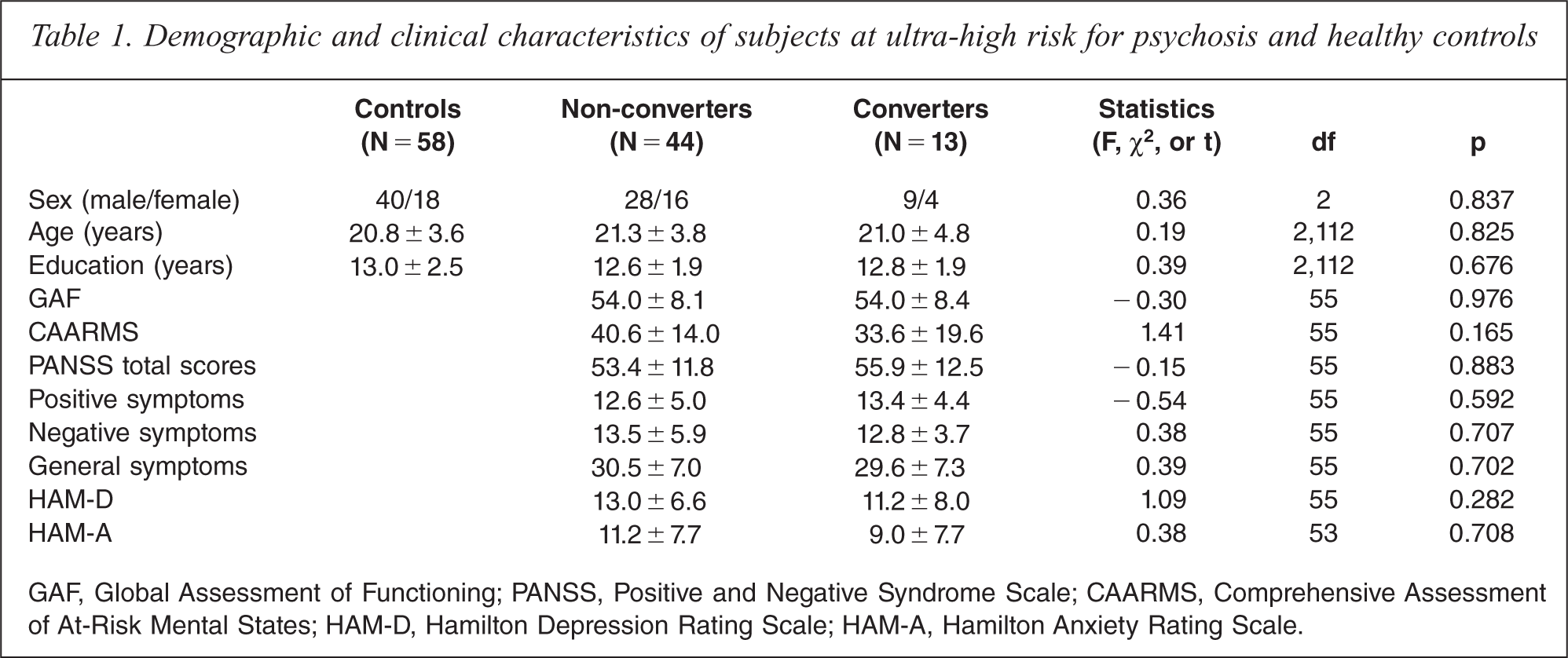
GAF, Global Assessment of Functioning; PANSS, Positive and Negative Syndrome Scale; CAARMS, Comprehensive Assessment of At-Risk Mental States; HAM-D, Hamilton Depression Rating Scale; HAM-A, Hamilton Anxiety Rating Scale.
Social functioning at baseline
The ANOVA revealed significant group differences in all seven subscales and on average total scores (p < 0.01 for all variables). The post hoc analysis revealed that both UHR groups, i.e. non-converters and converters, showed significantly lower average scores and significantly lower scores on the subscales addressing social engagement/withdrawal, interpersonal behaviour, independence–performance, independence–competence, and prosocial activities compared with controls (Figure 1). Additionally, the non-converter group had significantly lower scores than the control group on employment/occupation and recreation. There was no significant difference in social functioning between converters and non-converters at baseline. We found a significant positive correlation between GAF scores and the independence–competence (r = 0.42, p = 0.001) and average total (r = 0.50, p < 0.001) scores of the UHR subjects. A significant negative correlation was also found between CAARMS scores and the independence–competence (r = − 0.42, p = 0.001) and average (r = − 0.44, p = 0.001) scores.
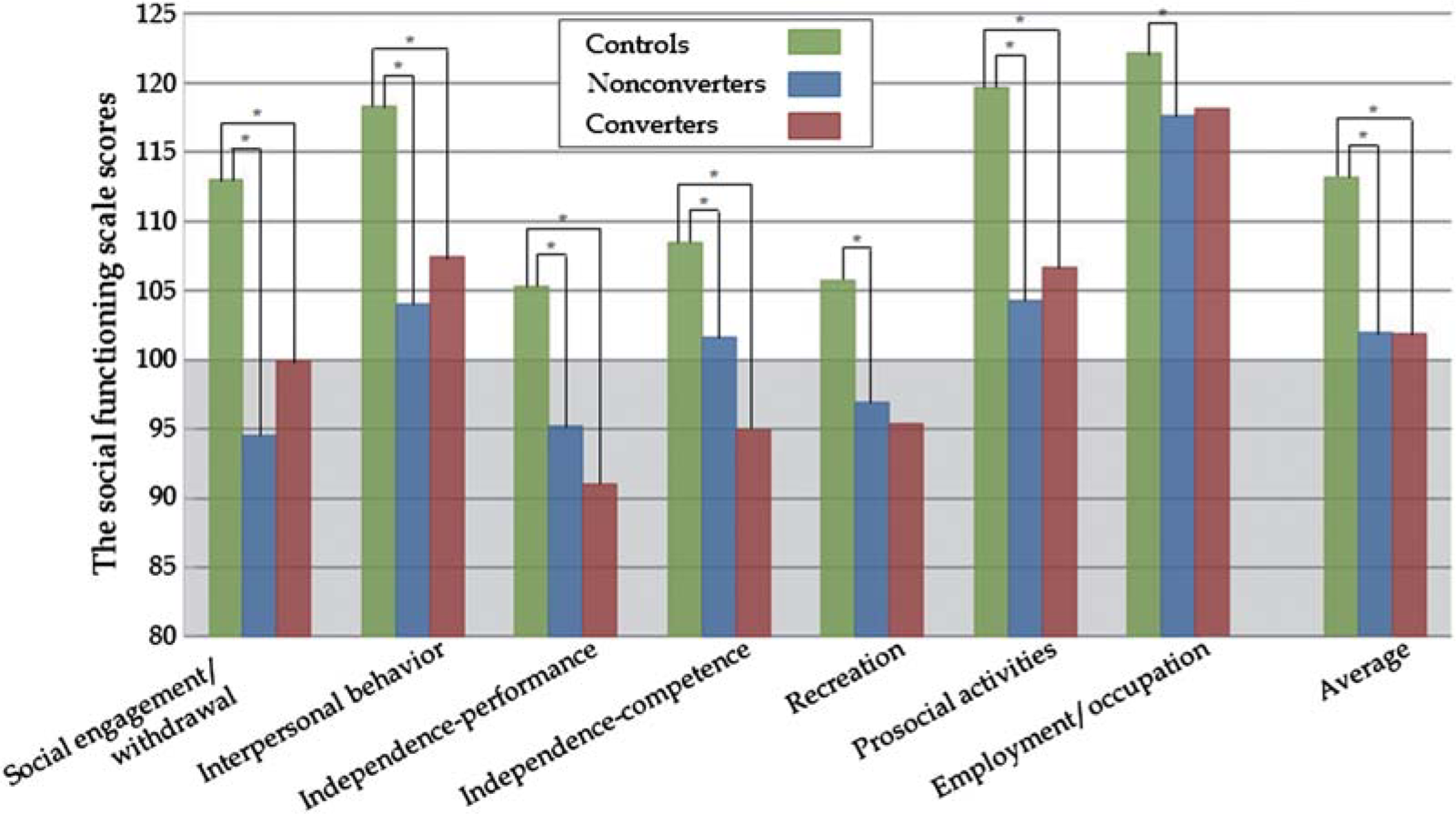
Social functioning scale scores at baseline for the three groups. *Statistically significant.
Longitudinal changes in social functioning
Of the 57 UHR subjects, 34 (28 non-converters and six converters) completed the SFS at both baseline and the 1 year follow up. No significant differences in demographic data, clinical symptoms, and baseline SFS scores were observed between subjects who did and did not complete the 1 year follow-up evaluation. A repeated-measures ANOVA was conducted to examine changes in social functioning during the 1 year follow-up period in the converter and non-converter groups. We found no significant main effects of group and time on SFS scores. However, the interaction of time × group was statistically significant for scores on the interpersonal behaviour subscale (F (1,32) = 10.43, p = 0.003) and for average scores (F (1,32) = 7.85, p = 0.009). An analysis of the simple main effects showed that there was a trend level of significance in the effect of time on the non-converter group (F (1,46) = 3.41, p = 0.071, Cohen's d = 0.53), with the average score being higher at the 1 year follow up. There was also a trend level of significance in the effect of time on the converter group (F (1,10) = 3.51, p = 0.091, Cohen's d = 1.08), with the interpersonal score being higher at baseline. These results indicated that the scores of the converter group decreased over time, whereas those of the non-converter group increased over time (Table 2). We examined the relationship between clinical symptoms and the rate of changes in SFS scores ([SFS scores at 1 year follow up − SFS scores at baseline]/the SFS scores at baseline × 100). Pearson correlation analysis showed a significant negative correlation between changes in the scores on the employment/occupation subscale and PANSS total scores (r = − 0.53, p = 0.001) and positive symptoms scores (r = − 0.51, p = 0.002) at baseline. However, no significant relationships between changes in the scores on clinical variables and in scores on the SFS were found.
The SFS scores at baseline and 1 year follow up in converters and non-converters
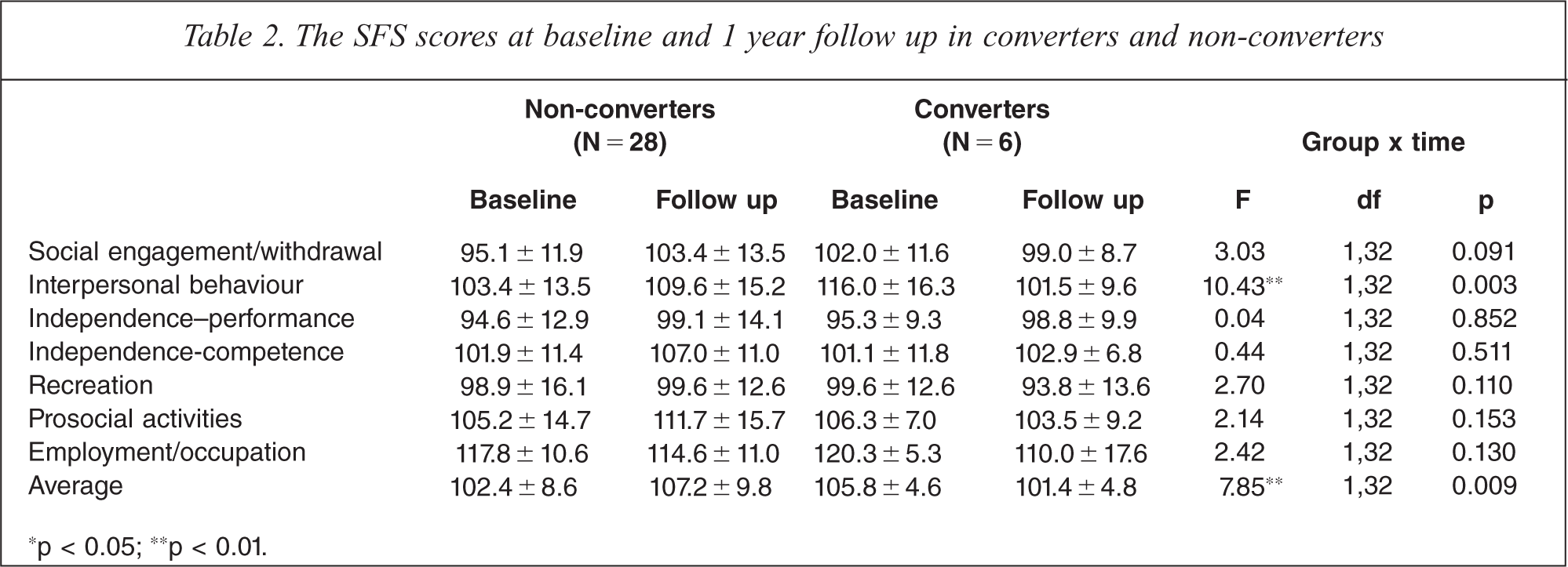
*p < 0.05; **p < 0.01.
Effect of medication on changes in social functioning
To evaluate the effects of pharmacotherapy on changes in social functioning, we divided UHR subjects into two subgroups according to whether they had received medication since the baseline assessment. Working under the hypothesis that drug treatment would require time to influence social functioning, only subjects who took medication until the 6 month follow up were included in the medication group. Of the 34 UHR subjects who completed the follow-up assessment, 17 were placed in the medication group (non-converter, n = 13; converter, n = 4) and 17 were in the non-medication group (non-converter, n = 15; converter, n = 2). Ten subjects were taking low doses of atypical antipsychotics (mean daily dose: 68.75 mg/day of quetiapine (n = 4), 7.50 mg/day of aripiprazole (n = 3), 1.75 mg/day of risperidone (n = 2), 2.5 mg/day of olanzapine (n = 1)), and three subjects received antidepressants (10 mg/day of escitalopram, 40 mg/day of citalopram, and 12.5 mg/day of paroxetine, respectively). Additionally, two subjects were taking both atypical antipsychotics and antidepressants (150 mg/day of quetiapine and 5 mg/day of escitalopram; and 2 mg/day of risperidone and 25 mg/day of escitalopram, respectively). The remaining two subjects took 1 mg/day of lorazepam and 10 mg of zolpidem (intermittently), respectively. We found no significant differences between medicated and non-medicated subjects in scores on the SFS subscales and average scores at the initial assessment. Additionally, no significant association between symptom severities at baseline and prescription of pharmacotherapy were observed.
We explored the effect of medication on changes in social functioning over time using a repeated-measures ANOVA. It was found that there was no significant main effect of group and time on the SFS scores. However, we found a significant time × medication group interaction effect on scores on the prosocial activities subscale (F (1,32) = 4.66, p = 0.038) (Figure 2). An analysis of the simple main effects indicated that there was a marginally significant difference in the effect of time in the medication group, with prosocial activities score being higher in a follow up than baseline (F (1,32) = 3.79, p = 0.061, Cohen's d = 0.68), whereas there was no significant difference in the non-medication group. We further investigated the predictive power of baseline scores on the SFS subscale measuring prosocial activities for the introduction of pharmacotherapy in UHR subjects. Logistic regression analysis revealed that scores on the prosocial activities subscale were not significantly associated with the introduction of medication.
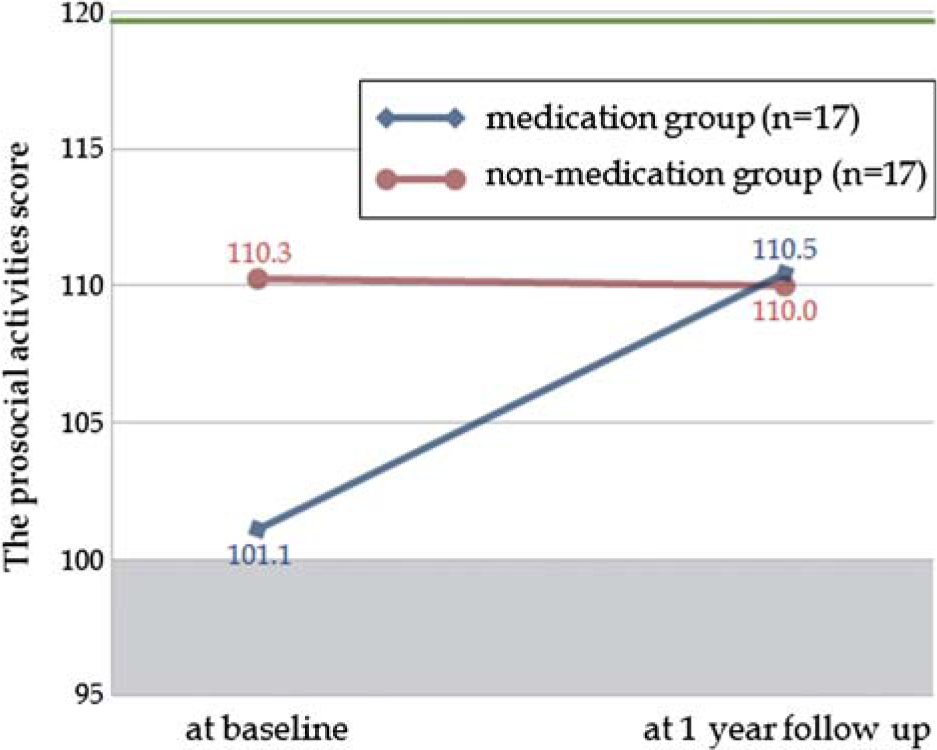
The effect of pharmacotherapy on change of social functioning in subjects at ultra-high risk for psychosis. The green line refers to the average prosocial activities scores of healthy controls (119.7).
Discussion
To the best of our knowledge, this is the first prospective study to investigate longitudinal changes in social functioning over the course of 1 year in subjects at UHR for psychosis. UHR subjects who did and did not subsequently develop psychosis showed a distinct pattern of changes in social functioning. This finding suggests that the pattern of changes in social functioning over time may differentiate between UHR subjects who will and will not convert to psychosis. Furthermore, we found evidence that different patterns of changes in some domains of social functioning were associated with pharmacological treatments.
Consistent with results of previous studies showing the presence of social dysfunction in UHR subjects [14,15], this study found that the social functioning of UHR subjects was significantly more impaired that that of controls at the baseline assessment. Retrospective studies have also reported social isolation to be one of the most frequent prodromal symptoms, preceding the first positive symptoms by years [11,28,29]. Our study further indicated that those at high risk for psychosis, regardless of whether they converted to psychosis in the near future, may experience impairments in their ability to engage in social interactions and independent living at the time of help-seeking.
Poor social functioning has been suggested as a predictive marker of future psychosis in subjects at high risk [10,30,31]. During the 1 year follow-up period, the UHR subjects who subsequently developed psychosis showed a different pattern of decline in social functioning than did the UHR subjects who did not develop psychosis, especially as reflected in scores on the SFS subscale measuring interpersonal behaviour as well as on average scores. Additionally, pharmacological treatment was related to increases in scores on the SFS subscale measuring prosocial activities. Considering that the average SFS score is 100 in chronic patients with schizophrenia [1], these results implied that the social functioning of the converter group had deteriorated as much as that of patients with schizophrenia during the 1 year follow-up period even in the absence of a formal diagnosis of schizophrenia. It has been postulated that the social functioning of UHR subjects is impaired before the initiation of the prodromal phase and that it further declines during this phase. Our study revealed that the social functioning of converters (true positive) was impaired before the onset of the psychotic phase and further declined during the prodromal or at-risk phase. Additionally, this result indicated that the onset of full-blown psychosis may be more strongly related to the pattern of change in social functioning than to baseline severity.
In the UHR group, the subscales measuring interpersonal behaviour reflected the most distinctive differences as a function of time, and that measuring prosocial activities reflected the strongest influence by medication. The interpersonal behaviour domain evaluates the number of friends and heterosexual contact and the quality of communication. Social cognition may be a potential mediator of this deterioration in social functioning [5,32]. There have been studies reporting deficits in social cognition, mostly in theory of mind and emotional recognition, in UHR subjects [14,33,34]. Emotional recognition has been linked to social activities such as interpersonal relationships and community involvement [35,36]. Recently, Mehl et al. [37] reported that the deficit in the theory of mind was a better predictor of social performance than psychopathological symptoms and other neurocognitive deficits in schizophrenia spectrum disorders. In addition, a study revealed that disruptions in white matter integrity could predict deterioration in social functioning, indicating that early alteration in microstructural brain developments may underlie in UHR subjects [38]. Such findings, taken together, indicate that deficits in social cognition and functioning may be vulnerability markers or endophenotypes of schizophrenia. Additionally, the absence of a significant relationship between changes in clinical variables and social functioning in this study may imply that changes in the level of social functioning are dependent on complex mechanisms that require more complex measures.
Even if the most effective type of intervention for UHR individuals has not yet been established, it has been suggested that early interventions including medication, social support, and stress management may delay or prevent psychosis [19,20]. A recent study reported that treatment with antipsychotic medications resulted in improvements in social competence among patients with schizophrenia [18]. Non-pharmacological treatments have also been associated with improvements in various domains of social functioning and cognition [17,39]. Thus, the results of this and previous studies indicate that appropriate combinations of pharmacological and non-pharmacological treatments, such as social skills training programmes and cognitive-behavioural therapies, can offer clinical benefits to this at-risk population.
The present study had several limitations. First, the small sample size of the converter group precluded investigation of the effect of medication on changes in the social functioning of this group. However, given the difficulty of following UHR subjects and the similar conversion rates reported by recent studies and this study [30,40], our findings offer appropriate clinical impressions and directions for future research. Second, it is important to note that some current non-converters may develop psychosis in the future. However, the UHR subjects in this study were examined for an average of 2.8 years, and previous longitudinal studies have reported that UHR subjects who did not convert in 2–3 years have a relatively low probability for the later conversion to psychosis [30,41]. Finally, the SFS instrument was originally developed to assess social functioning in a population of those with schizophrenia, and it may not be appropriate for the accurate evaluation of social dysfunction among young, pre-psychotic UHR subjects.
In conclusion, our prospective study found that individuals at UHR for psychosis who later converted to psychosis showed worse change of social functioning compared with those who were at risk but did not convert. These data suggest that a series of longitudinal social functioning indices may be helpful in predicting conversion to psychosis in individuals at UHR. We also confirmed that pharmacological treatment can be one of the methods for improving social functioning. Further research with larger samples and longer follow-up periods will help elucidate the direct association between early intervention and improvements in functioning.
Footnotes
Acknowledgements