
Abstract
Objective:
Social and role functioning are compromised for the majority of individuals at ultra-high risk of psychosis, and it is important to identify factors that contribute to this functional decline. This study aimed to investigate social cognitive abilities, which have previously been linked to functioning in schizophrenia, as potential factors that impact social, role and global functioning in ultra-high risk patients.
Method:
A total of 30 ultra-high risk patients were recruited from an established at-risk clinical service in Melbourne, Australia, and completed a battery of social cognitive, neurocognitive, clinical and functioning measures. We examined the relationships between all four core domains of social cognition (emotion recognition, theory of mind, social perception and attributional style), neurocognitive, clinical and demographic variables with three measures of functioning (the Global Functioning Social and Role scales and the Social and Occupational Functioning Assessment Scale) using correlational and multiple regression analyses.
Results:
Performance on a visual theory of mind task (visual jokes task) was significantly correlated with both concurrent role (r = 0.425, p = 0.019) and global functioning (r = 0.540, p = 0.002). In multivariate analyses, it also accounted for unique variance in global, but not role functioning after adjusting for negative symptoms and stress. Social functioning was not associated with performance on any of the social cognition tasks.
Conclusion:
Among specific social cognitive abilities, only a test of theory of mind was associated with functioning in our ultra-high risk sample. Further longitudinal research is needed to examine the impact of social cognitive deficits on long-term functional outcome in the ultra-high risk group. Identifying social cognitive abilities that significantly impact functioning is important to inform the development of targeted intervention programmes for ultra-high risk individuals.
Introduction
Social cognition refers to the ‘mental operations that underlie social interactions’ (Green et al., 2008). It comprises four core domains: emotion processing (perceiving and displaying emotions), theory of mind (ToM; the ability to represent the mental states of others), social perception (decoding and interpreting social cues in others) and attributional style (the way in which individuals explain the causes, or make sense, of social events or interactions) (Pinkham et al., 2014). Social cognitive impairments are a common feature of schizophrenia-spectrum disorders (Savla et al., 2013). These impairments are present not only in the established illness but are evident in the early phase of illness, at the time of the first episode of psychosis (FEP) (Thompson et al., 2012).
Additionally, over the last two decades, it has been possible to identify individuals who are at ultra-high risk (UHR) of developing a psychotic disorder such as schizophrenia (i.e. they are putatively prodromal for the illness) (Miller et al., 2002; Yung et al., 1996, 1998), and there is growing evidence that social cognitive deficits are present in this group (Barbato et al., 2015; Lee et al., 2015). Performance in each of the four core social cognitive domains in UHR individuals is generally intermediate between FEP and healthy control groups (Green et al., 2012; Thompson et al., 2012).
Social cognitive impairment is an important determinant of functional outcome in schizophrenia (Fett et al., 2011). However, relatively little is known about the relationship between social cognition and functioning in the UHR population. The few studies that have examined this relationship have all reported inconsistent results. In the largest cross-sectional study conducted to date in the UHR group, facial emotion recognition and ToM task performance were positively correlated with functioning (Barbato et al., 2013). In contrast, a smaller study reported no associations between functioning and performance on four separate ToM tasks (Stanford et al., 2011). After accounting for negative and depressive symptoms, poorer performance on a vocal but not facial affect recognition task was also reported to be modestly but significantly associated with poorer functioning (Amminger et al., 2013).
To the authors’ knowledge, no previous studies have examined the association between functioning and all four core domains of social cognition in a single UHR cohort. Studies have also tended to use functioning measures that combine both social and role functioning into a single global construct. Functioning is a broad concept that constitutes a variety of domains. While global functioning is useful as a marker of overall impairment, it is important to examine social and role functioning as separate constructs on the basis of previous evidence that dysfunction in each of these domains may be driven by different aspects of illness (Fett et al., 2011; Strassnig et al., 2015). Many functioning measures have also been developed for adults with chronic illness and therefore may not be suitable for UHR populations, which consist predominantly of adolescents and young adults who face functional demands specific to individuals at this stage of life (e.g. high school or tertiary education, starting work for the first time and embarking on romantic relationships).
Thus, the aim of this exploratory study is to investigate whether performance on a broad range of social cognitive measures is associated with concurrent social, role or global functioning in individuals at UHR for developing psychosis. On the basis of previous research in those with established psychotic disorders (Fett et al., 2011; Pinkham et al., 2015) and the largest UHR study conducted in this area to date (Barbato et al., 2013), we hypothesized that poorer performance on ToM tasks would be associated with poorer functioning.
Methods
Participants
Data were derived from a larger study, which investigated the degree of social cognitive impairment in UHR individuals in comparison with FEP and healthy control participants. This sample has been previously described elsewhere (Thompson et al., 2012, 2013). Briefly, 30 UHR participants were recruited from Orygen Youth Health, an outpatient service in Melbourne. Inclusion criteria for the UHR participants were as follows: (1) aged between 15 and 25 years, (2) be help-seeking, (3) present with a drop in functioning (or chronic low functioning for the past year) and (4) meet UHR criteria for attenuated psychotic symptoms, brief limited intermittent psychotic symptoms (BLIPS) and/or trait vulnerability, according to the Comprehensive Assessment of At-Risk Mental States (CAARMS; Yung et al., 2005). In addition, UHR participants were required to be clinically stable (i.e. not an inpatient or requiring crisis care) and be able to provide informed consent. Patients were excluded if they were being treated for a major neurological disorder, had poor English language skills or had an IQ <70. Those with impaired visual acuity (i.e. blurred vision or less than corrected 20/40 vision) or corrected auditory acuity were also excluded from the study. The study was approved by the local ethics committee. All participants provided written informed consent.
Procedure and measures
Demographics
Patient’s age, gender and number of years of completed education were recorded at the time of the assessment.
Psychopathology
Positive psychotic symptoms were assessed using the Brief Psychiatric Rating Scale (BPRS) psychotic subscale (Overall and Gorham, 1962), derived from combining scores from the unusual thought content, suspiciousness, hallucinations and conceptual disorganization items. Negative psychotic symptoms were assessed using the Scale for the Assessment of Negative Symptoms (SANS; Andreasen, 1984). Depression, anxiety and stress were measured using the Depression Anxiety Stress Scale (DASS; Lovibond and Lovibond, 1995). This is a 42-item self-report instrument which provides a total score and three subscale scores for depression, anxiety and stress. These were included on the basis that they may be associated with poor functioning and may influence the association between social cognition and functioning (Cotter et al., 2014). All assessments were conducted by two of the authors (A.P. and C.B.). Inter-rater reliability was not formally assessed; however, both raters had considerable experience administering psychiatric assessments and undertook reliability checks throughout the study period.
Social cognitive measures
Social cognitive measures were chosen that represent each of the four core domains of social cognition (Pinkham et al., 2014), described below.
Emotion recognition
The adult version of the Diagnostic Analysis of Nonverbal Accuracy-2 (DANVA-2) scale for faces and voices (Nowicki and Carton, 1993; Nowicki and Duke, 1994) was used to assess emotion recognition. The faces subtest consisted of 24 colour photographs of an equal number of happy, sad, angry and fearful facial expressions of high and low intensities. The participant was required to choose the correct facial emotion expression from the four options given. The Paralanguage subtest consisted of two alternating professional actors speaking in a way designed to express happy, sad, angry or fearful feelings by saying a neutral sentence, ‘I am going out of the room now but I’ll be back later’. There were 24 voices of an equal number of emotions of high and low intensities. Both the face and voice stimuli were presented in a randomized order using a computer program. Total scores for errors on either task (maximum 24) were computed. The DANVA-2 has good reliability and reasonable construct validity (Nowicki and Duke, 1994).
ToM
The Hinting Task (Corcoran et al., 1995) was used to assess the ability to infer real intentions based on indirect speech content. A total of 10 short passages were read aloud to the participant. Each involved an interaction between two characters and ended with one of the characters dropping an obvious hint. For each passage, the participant was asked what the character ‘really’ meant based on what they had said/hinted at. A second obvious hint was given if the participant’s first response was incorrect. A total score was calculated out of 20. In addition, a version of the visual jokes task (Corcoran et al., 1997) was also administered because it is not reliant on verbal memory or verbal comprehension. A total of 10 cartoon jokes were displayed on a computer screen one at a time. Jokes were designed to elicit either mentalizing about a character’s thoughts (five ToM jokes) or mentalizing about physical aspects of the cartoon (five control jokes). These were presented in a randomized order both within and between categories. Participants were instructed to explain the humour in the joke and could take as much time as they needed (responses were audio-recorded). Scoring was performed by C.B., A.P. and A.T. in collaboration and was based on the previously devised validated method (Corcoran et al., 1997). Higher scores were given when the participants’ explanation specifically referred to mental states (each joke scored between 0 and 3). Total mentalizing sub-scores were calculated for the control (maximum score of 15) and ToM conditions (maximum score of 15). Only the ToM jokes score was used for the analysis in this study.
Social perception
The social cognitive measure from the Measurement and Treatment Research to Improve Cognition in Schizophrenia (MATRICS) battery (Nuechterlein et al., 2008), the managing emotions module (branch 4) of the Mayer–Salovey–Caruso Emotional Intelligence Test (MSCEIT; Meyer et al., 2002), was used to measure social perception. Vignettes are read aloud to participants and they are asked various questions relating to their emotions and the emotions of others. These questions typically involve the perception of social or interpersonal situations and require interpretation of the appropriate response to these situations. The total managing emotions score on the MSCEIT is scored using a web-based scoring program (available from Multi-Health Systems, Inc., Toronto, Ontario, Canada) using unadjusted consensus norms from a large normative sample. Scores are automatically calculated and scaled with a mean of 100 and a standard deviation of 15. Higher scores represent better emotional management. The Schema Component Sequencing Task–Revised (SCST-R; Corrigan and Addis, 1995) was administered to assess social knowledge, another aspect of social perception (Pinkham et al., 2014). A total of 12 social scenarios (e.g. eating out in a restaurant) are broken down into six (short sequence) or nine (long sequence) actions. Each action was typed on a laminated card. Prior to each sequence the participant was informed of the scenario with a ‘header’ card. Each of the action cards for that given scenario was then placed in front of the participant in a predetermined random order. Participants were instructed to arrange the cards into the correct order as quickly as possible. Mean ‘juxtaposition scores’ were calculated for each sequence by dividing the number of cards correctly juxtaposed to neighbouring cards by the total possible correct juxtapositions. Scores ranged from 0 to 1 (Corrigan and Addis, 1995).
Attributional style
We used a locus of control (LOC) task to infer whether participants had a tendency towards an externalizing or internalizing bias. LOC, which is the extent to which an individual believes he or she can control events that affect them, was assessed with the Adult Nowicki Strickland Internal External (ANSIE) LOC scale (Nowicki and Duke, 1974). This is a 40-item, self-administered questionnaire requiring yes or no answers (e.g. ‘Do you believe that wishing can make good things happen?’). Scores range from 0 to 40. Higher scores represent a more externalized bias (outcome of events is determined by external factors such as the environment), while a lower score represents an internalized bias (outcome of events is related to something the individual did/thought).
Neurocognitive measures
IQ was measured using the vocabulary and matrix reasoning subtests of the Wechsler Abbreviated Scale of Intelligence (WASI; Wechsler, 1999). Information processing speed was assessed using the Trail Making Tests A and B (Reitan, 1955). Verbal working memory was measured using the letter number span test (Gold et al., 1997). Visual working memory was measured using the Wechsler Memory Scale–Third Edition (WMS-III) spatial span subtest (Wechsler, 1997).
Functioning
Social and role functioning were independently assessed using the Global Functioning Social (GFS) and Global Functioning Role (GFR) scales, respectively (Cornblatt et al., 2007). Both scales are interviewer-rated, with scores ranging from 1 (extreme dysfunction) to 10 (superior functioning). Anchors are provided for each point on the scale. The GFS scale assesses engagement in social activities and the quality of interpersonal relationships with family, friends and romantic partners. The GFR scale assesses educational or vocational engagement and performance. These scales have previously been validated in the UHR population (Cornblatt et al., 2007). Functioning was also assessed using the Social and Occupational Functioning Assessment Scale (SOFAS; Goldman et al., 1992). This is a brief and well-established interviewer-rated scale that combines assessment of both social and role functioning to provide a single global functioning score ranging from 0 to 100. Specific anchors are included for each 10-point range. Higher scores indicate better functioning.
Data analysis
Data were analysed using SPSS statistical software (IBM SPSS Statistics for Windows, Version 22.0; IBM Corp., Armonk, NY). In addition to the individual social cognitive assessments, a composite social cognitive score was computed by averaging z scores on each of the six social cognitive assessments from the emotion recognition, ToM and social perception subdomains. The attributional style data were not incorporated into the composite score as this measure was not based on social cognitive performance per se, but instead based on personal perspective of external events. This was further corroborated by the lack of correlation between the attributional data and the other three social cognitive domains, which were each in turn highly correlated with one another (all p ⩽ 0.002).
The z scores were derived based on data obtained from an age-matched healthy control group (for further details of this group, see Thompson et al., 2012). Mean scores for each of the assessments were calculated from the healthy controls and then subtracted from the scores obtained from the UHR patients for each of the individual tests; these were then divided by the standard deviation obtained from the healthy controls for that respective test. All scores were computed so that higher values indicated better performance. Scores for each of the assessments were then added together and divided by the number of assessments (six) so that equal weightings were given to each of the assessments and therefore the three social cognitive subdomains within the overall composite score.
Bivariate correlations were calculated to examine the relationships of the three functioning measures with social cognitive and neurocognitive performance, clinical symptoms and demographic variables. Variables that were significantly correlated with each of the functioning measures (p < 0.05) were input into multiple linear regression analyses using the ‘enter’ method. Correlations were uncorrected for multiple comparisons due to the exploratory nature of the research on the basis of limited and inconsistent previous findings in this area (e.g. Barbato et al., 2013; Stanford et al., 2011). Separate multivariate analyses were conducted for each of the social cognition measures that were correlated with any of the functioning assessments. Functioning measures were included as the dependent variables for all multivariate analyses. Model fit was assessed using the adjusted R2 statistic.
Results
Sample characteristics
An overview of the clinical and demographic characteristics of the sample and performance on the social cognition tasks is provided in Table 1. Of the 30 patients included in the sample, 22 patients met criteria for attenuated positive psychotic symptoms, 2 met trait criteria, 5 met criteria for both the trait and attenuated symptom groups and 1 met a combination of trait, attenuated symptoms and BLIPS criteria.
Sample characteristics.
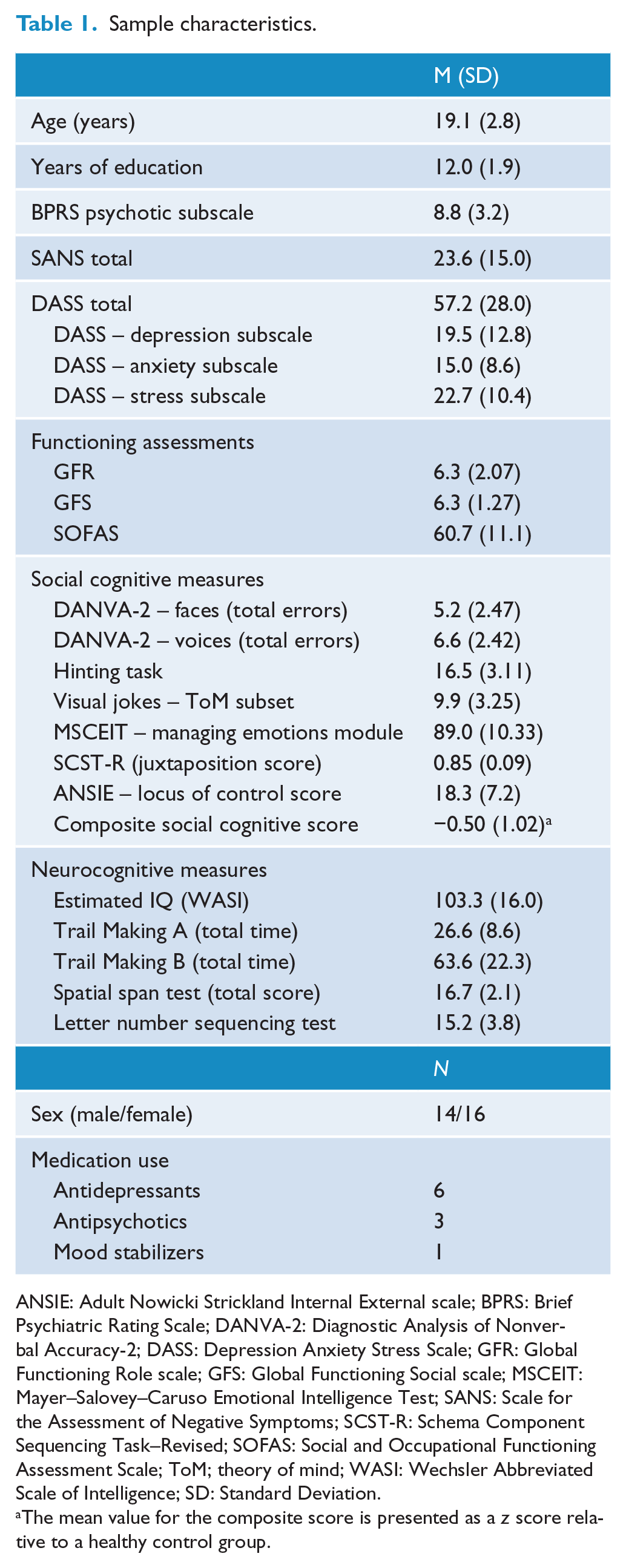
ANSIE: Adult Nowicki Strickland Internal External scale; BPRS: Brief Psychiatric Rating Scale; DANVA-2: Diagnostic Analysis of Nonverbal Accuracy-2; DASS: Depression Anxiety Stress Scale; GFR: Global Functioning Role scale; GFS: Global Functioning Social scale; MSCEIT: Mayer–Salovey–Caruso Emotional Intelligence Test; SANS: Scale for the Assessment of Negative Symptoms; SCST-R: Schema Component Sequencing Task–Revised; SOFAS: Social and Occupational Functioning Assessment Scale; ToM; theory of mind; WASI: Wechsler Abbreviated Scale of Intelligence; SD: Standard Deviation.
The mean value for the composite score is presented as a z score relative to a healthy control group.
Correlations
The results of the correlational analysis are presented in Table 2. The ToM jokes task was the only social cognition measure that was significantly correlated with any of the functioning measures. This was positively correlated with both the GFR (r = 0.425, p = 0.019) and SOFAS scales (r = 0.540, p = 0.002), suggesting that better performance on this task was associated with better role and global functioning. There was also a trend association verging on significance (r = 0.360, p = 0.051) between performance on the MSCEIT – managing emotions module and SOFAS score, suggesting that better social perception was associated with better global functioning. This was also included in multivariate analyses. None of the social cognition tasks was significantly correlated with the GFS scale, so additional multivariate analyses were not conducted for this measure. Composite social cognitive performance was also unrelated to any of the functioning measures.
Correlations between functioning measures, clinical and demographic variables and social cognitive and neurocognitive performance.
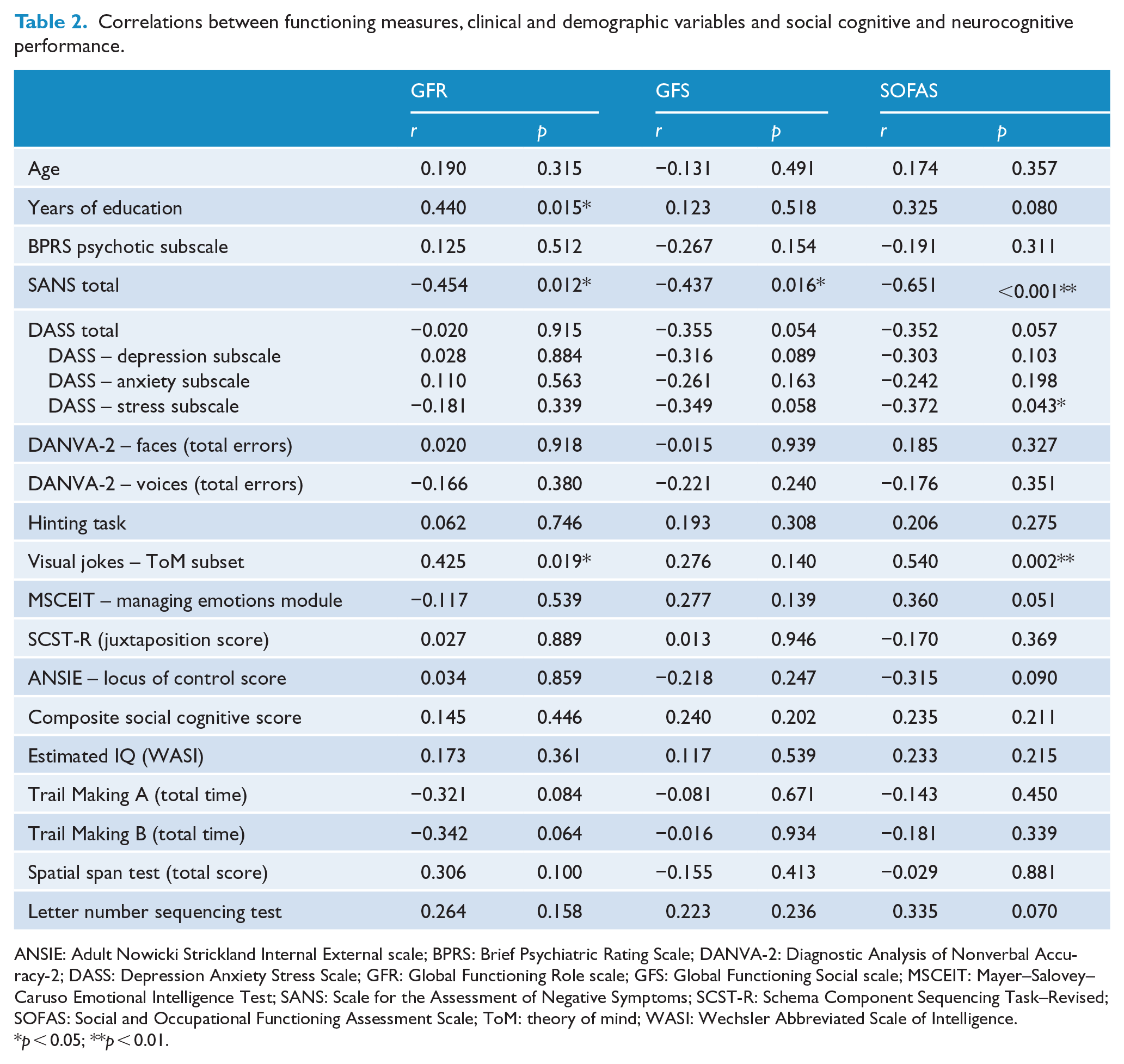
ANSIE: Adult Nowicki Strickland Internal External scale; BPRS: Brief Psychiatric Rating Scale; DANVA-2: Diagnostic Analysis of Nonverbal Accuracy-2; DASS: Depression Anxiety Stress Scale; GFR: Global Functioning Role scale; GFS: Global Functioning Social scale; MSCEIT: Mayer–Salovey–Caruso Emotional Intelligence Test; SANS: Scale for the Assessment of Negative Symptoms; SCST-R: Schema Component Sequencing Task–Revised; SOFAS: Social and Occupational Functioning Assessment Scale; ToM: theory of mind; WASI: Wechsler Abbreviated Scale of Intelligence.
p < 0.05; **p < 0.01.
Of the neurocognitive, clinical and demographic variables, levels of negative symptoms (SANS total) were significantly negatively correlated with all functioning measures and were included in all subsequent multivariate analyses. DASS stress subscale scores and years of education were significantly associated with SOFAS and GFR scores, respectively, and were included in related multivariate analyses. There was also a trend association between DASS total score and SOFAS (r = −0.352, p = 0.057); however, this was not included in subsequent multivariate analyses due to high correlation with the DASS stress subscale score (r = 0.894, p < 0.001).
We performed additional exploratory correlations to examine the strength of the relationships between each of the three functioning measures. Scores on the SOFAS were significantly correlated with both the GFS (r = 0.703, p < 0.001) and GFR (r = 0.435, p = 0.016) scales. However, the GFS and GFR scales were not significantly correlated with one another (r = 0.158, p = 0.406).
Regression analyses
Global functioning
Two separate multivariate models were created to examine the relationships between performance on the ToM jokes and MSCEIT tasks with SOFAS score (see Table 3). Performance on the ToM jokes task (β = 0.381; p = 0.009) and SANS total (β = −0.466; p = 0.003) remained significantly associated with functioning in the first multivariate model; however, the DASS stress subscale was no longer significantly associated after adjusting for these other variables. The model accounted for 53% of variance in SOFAS scores (adjusted R2 = 0.533, F(3, 26) = 12.012, p < 0.001). In the other analysis, investigating performance on the MSCEIT social perception task, total MSCEIT score was no longer significantly associated with SOFAS scores in the multivariate model after adjusting for negative symptoms and stress (adjusted R2 = 0.406, F(3, 26) = 7.603, p = 0.001).
Multivariate analyses of variables associated with the SOFAS.
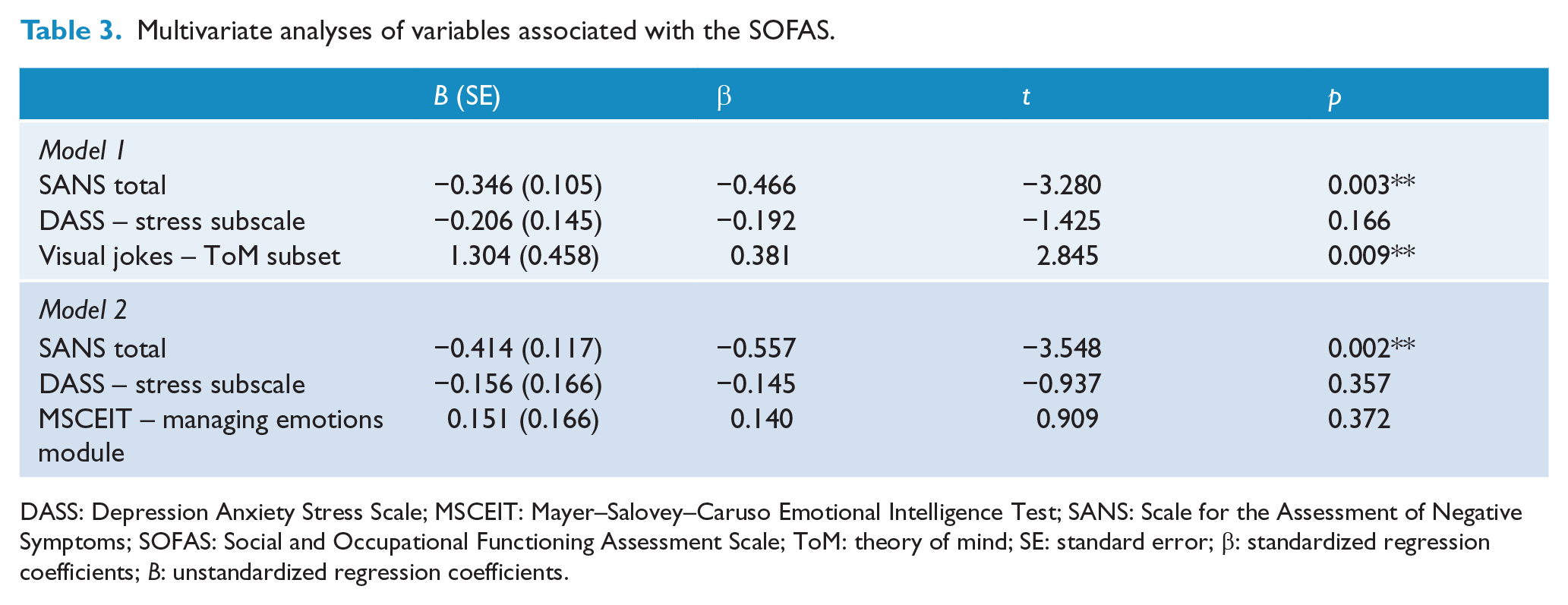
DASS: Depression Anxiety Stress Scale; MSCEIT: Mayer–Salovey–Caruso Emotional Intelligence Test; SANS: Scale for the Assessment of Negative Symptoms; SOFAS: Social and Occupational Functioning Assessment Scale; ToM: theory of mind; SE: standard error; β: standardized regression coefficients; B: unstandardized regression coefficients.
Role functioning
Performance on the ToM jokes task was not found to be significantly associated with GFR scores in the multivariate model (see Table 4). Although the model was significant, none of the variables entered into the model remained as significant independent predictors (adjusted R2 = 0.281, F(3, 26) = 4.780, p = 0.009).
Multivariate analyses of variables associated with the GFR scale.
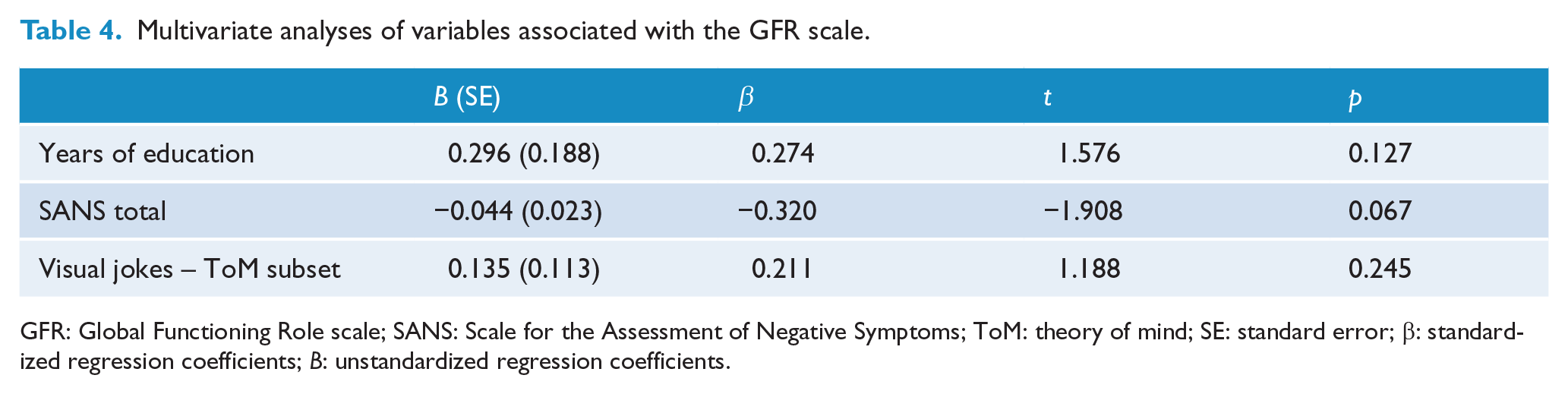
GFR: Global Functioning Role scale; SANS: Scale for the Assessment of Negative Symptoms; ToM: theory of mind; SE: standard error; β: standardized regression coefficients; B: unstandardized regression coefficients.
Discussion
Functioning has become an important outcome of interest across the psychosis-spectrum (Brissos et al., 2011; Lin et al., 2013; Yung et al., 2010). Specific investigation of factors associated with and predictive of functional outcome in the UHR population is in its infancy, but rapidly gathering interest as an alternative (or additional) outcome to transition to psychotic disorder (Cotter et al., 2014). This work has been supported by evidence that UHR individuals not only have poor social and occupational functioning at initial presentation (Velthorst et al., 2010; Yung et al., 2004) but that a large proportion continue to function poorly at long-term follow-up regardless of whether they develop a full-threshold psychotic disorder (Addington et al., 2011; Salokangas et al., 2013; Yung et al., 2015). This study sought to examine the association between performance on a broad range of social cognition tasks with social, role and global functioning.
Overview of findings
We found partial support for our hypothesis that poorer performance on ToM tasks would be associated with poorer functioning. A deficit in one measure of ToM (jokes task) was found to be associated with overall functional impairment, even after adjusting for negative symptoms. However, it was not associated with specific measures of social or role functioning.
Aside from the significant correlations between the ToM jokes task and functioning assessments, and the trend association between the social perception task and SOFAS score, all other correlations were weak and non-significant, suggesting that social cognitive performance was not generally associated with concurrent social, role or global functioning. This may be at least partially attributable to the lack of marked social cognitive deficits in this group. When our UHR group was previously compared to healthy controls, they performed more poorly on all of the social cognitive measures reported in this paper; however, performance was only statistically significantly worse on the ToM hinting task (Thompson et al., 2012). The lack of association between the poor performance on the hinting task and any of the functioning assessments is interesting in light of recent evidence showing it to be one of the social cognitive tests most strongly associated with poor concurrent functioning in a schizophrenia cohort (Pinkham et al., 2015). Mean overall performance on the ToM jokes task did not significantly differ from healthy controls, although the variability in performance was greater in the UHR group (Thompson et al., 2012). This could indicate that the severity of impairments across the other domains was not sufficient to impact functioning or could be compensated for, unlike what has been reported in patients with full-threshold psychotic disorders who exhibit much more widespread and pronounced social cognitive and neurocognitive deficits (Fioravanti et al., 2012; Thompson et al., 2012). Other factors such as negative symptoms may have a greater influence on functioning when social cognitive impairments are only minor. Alternatively, it may be that sustained negative symptoms worsen social cognitive deficits over time, resulting in further functional decline.
It is also possible that many individuals in our UHR sample were not truly at risk of psychotic disorder. Thus, any association between social cognitive impairments and poor functioning in those actually in the prodromal phase of schizophrenia may not be detectable, due to high numbers of people not at risk in whom no association would be expected. It would have been interesting to examine the differences between those who subsequently went on to develop a full-threshold psychotic disorder and those that did not; however, this was not possible in this study due to the low number of participants.
The results of this study both support and conflict with previous research in the UHR group. Barbato et al. (2013) identified a significant association between another measure of visual ToM, the Reading the Mind in the Eyes task, which is corroborated by the findings in this study. They also found no links between vocal emotion recognition and functioning. However, they did report a significant correlation between facial emotion recognition and functioning which was not found in this study. This may be due to their much larger sample size (n = 137) and a lack of power in this study to replicate this association. The measure of facial emotion recognition used in this study also included a narrower range of expressions and may have been less sensitive than the measure used in the previous study (Barbato et al., 2013). The results of this study also conflict with the findings of Stanford et al. (2011) who reported no associations between four different measures of ToM and functioning, despite using the same visual measure of ToM used by Barbato et al. (2013). Amminger et al. (2013) also reported no association between facial emotional recognition and functioning in a UHR sample, although they did identify a modest association between poor vocal affect recognition and poor global functioning. However, this study used the Global Assessment of Functioning (GAF) as the outcome variable, which conflates symptoms with functioning. It is therefore unclear whether clinical symptoms or functional impairment drove this association as results from another UHR study that used the same measure of vocal affect recognition found poor performance on this task to be significantly correlated with more severe negative symptoms (Addington et al., 2012).
Methodological considerations
This is the first study to examine the relationship between functioning and all four core domains of social cognition in a single UHR cohort. This was also the first UHR study to examine the association between social cognition and discrete measures of social and role functioning. Global functioning was correlated with both social and role functioning as would be anticipated. However, the discrete social and role functioning measures were weakly and non-significantly correlated, strengthening the argument that these should be examined as separate constructs (Cornblatt et al., 2007; Strassnig et al., 2015).
Limitations of this study include the small sample size and use of only cross-sectional data which did not permit causal links to be made. The small sample size may have led to a lack of power to detect associations. This is underlined by the non-significant correlations between neurocognitive measures such as processing speed and verbal memory which have previously been associated with functioning in larger and longitudinal UHR studies (Carrión et al., 2011; Lin et al., 2011). Additionally, because this was an exploratory as opposed to confirmatory study, we did not correct for multiple comparisons which may have increased the potential for Type I error. We also did not account for other variables that have previously been linked to poor functioning in this population, such as childhood trauma (Cotter et al., 2014; Yung et al., 2015). Longitudinal studies are needed to determine whether ToM is predictive of long-term functional disability in the same way that negative and disorganized symptoms, cognitive deficits and childhood trauma have been shown to be in the UHR group (Lin et al., 2011; Meyer et al., 2014; Yung et al., 2015).
Clinical implications
Efforts to date to improve functioning among UHR patients have proven largely ineffective (Cotter et al., 2014). Results from this study suggest that social cognitive remediation specifically targeting ToM may be beneficial for improving functioning in this group. Despite ToM involving a series of complex mental operations, efforts to improve ToM in patients with schizophrenia have demonstrated encouraging results (Bechi et al., 2015; Kurtz and Richardson, 2012). Trials are already underway to try and replicate these findings and assess their impact on functioning in the UHR population (Glenthøj et al., 2015). Oxytocin has also been shown to improve performance on higher order ToM tasks in patients with schizophrenia (Guastella et al., 2015; Woolley et al., 2014), although this effect is not always consistent (Cacciotti-Saija et al., 2015). No work has yet been published examining this effect in the UHR group, although it is a promising avenue for future research (Bartholomeusz et al., 2015).
Conclusion
Among specific social cognitive abilities, only ToM was related to concurrent functioning in our UHR sample. Although these findings should be interpreted with caution due to the small sample size and exploratory nature of the research, the results support the previous psychosis literature that has reported ToM as being the strongest social cognitive predictor of poor functioning. Further longitudinal research into the different ways in which social cognitive skills, as well as other factors, impact functional outcome in UHR is needed. This will allow for the development of targeted intervention programmes, which may be best delivered during the putatively prodromal period to reduce or prevent further functional decline.
Footnotes
Acknowledgements
The authors would like to thank Professor David Penn, Professor Rhiannon Corcoran and Associate Professor Robyn Langdon for their comments on task selection and Marija Strmota for her help in data management.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Thompson has previously received unrestricted investigator-initiated trial funding from Janssen-Cilag and Astra-Zeneca. He also held a Pfizer Neurosciences Research Grant which partly funded this study. Dr Bartholomeusz was supported by a National Health and Medical Research Council (NHMRC) Clinical Postdoctoral Research Fellowship. Dr Allott was supported by a Ronald Philip Griffiths Fellowship, Faculty of Medicine, Dentistry and Health Sciences, The University of Melbourne. Dr Nelson was supported by an NHMRC Career Development Fellowship. Professor Yung was supported by an NHMRC Senior Research Fellowship and has received research support from an NHMRC Program Grant and the Colonial Foundation, a research grant from Janssen-Cilag, honoraria from Janssen-Cilag and grant funding from NARSAD.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was partly funded by a Pfizer Neurosciences Investigator Grant. The funding source had no input into any aspect of the study.