
Abstract
It has long been suggested that positive psychotic symptoms exist on a continuum, with schizophrenia at one end and non-clinical psychotic symptoms (or ‘psychotic-like experiences’: PLE) at the other. Two models of continuity have been proposed: the quasi-dimensional model and the fully dimensional model. The quasi-dimensional model conceptualizes PLE as forme frustes or variants of disorder, for example, incompletely expressed schizophrenia. This suggests discontinuity with the normal population. A proponent of this quasi-dimensional model was Meehl, who proposed the existence of a ‘schizoid taxon’, which would have different phenotypic expressions including schizophrenia [1, 2]. This model also implies that those with PLE would be at increased risk, or vulnerable to, developing psychotic disorder. For example, the work of Chapman et al., and Chapman and Chapman suggests that individuals in the normal population with certain features, including PLE but also social and physical anhedonia, are psychosis prone [3–5]. Others also concur with this forme fruste or psychosis prone idea [6–15]. The theory is that if the psychosis prone or schizotypal individual is subject to sufficient psychosocial stress, then onset of psychotic disorder may occur, consistent with the stress vulnerability model [16]. There have even been treatment trials of these hypothetically vulnerable individuals [17, 18]. Clinical services have been developed for help-seeking individuals with PLE [19–24], and have been the setting for several interventions trials [25–27].
The fully dimensional model of psychosis proposes that PLE are part of personality [28, 29]. For example Claridge et al. described schizotypal features (including positive psychotic symptoms and anhedonia) as ‘healthy diversity’ and noted that they range from disorder to normal functioning [30]. This model implies no discontinuity from the normal population. It has even been proposed that schizotypy may confer an advantage on some individuals, with the suggestion that the schizophrenia spectrum displays an inverted-U relationship with creativity [31]. That is, the presence of some schizotypal features are associated with heightened creativity, whereas further along the schizophrenia spectrum, towards frank schizophrenia, the relationship is attenuated. Positive schizotypal traits (such as unusual perceptual experiences and magical beliefs) have been found to be of particular relevance to artistic creativity [31–33], whereas negative schizotypal traits (such as physical and social anhedonia and introversion) have been related to mathematical or scientific creativity [33]. This has led some researchers to suggest that creative advantage, among other benefits, may be a major reason that genes related to psychopathology remain in the gene pool, despite the costs of psychopathology to individual fitness [32, 34–36].
There is evidence for the continuum theory in the findings of high prevalence of PLE in the general population [8, 11, 37–41]. So is the continuity due to healthy diversity? That is, could some PLE not be associated with any distress or other problems in living, and not indicate underlying vulnerability to schizophrenia or other psychotic disorders in the longer term? Or is the continuity due to a group in the community who have heightened vulnerability to schizophrenia or other psychotic disorders but who do not manifest the full clinical syndrome at the time of assessment, but who may do so in the future if sufficiently stressed? That is, these vulnerable individuals may never develop a full psychotic disorder if not sufficiently stressed. It is therefore difficult to distinguish between the models. Perhaps endophenotypic measures on, and detailed phenomenological exploration of, those with PLE but no clinical disorder may shed some light on this issue [42].
Another central question is whether all psychotic symptoms are the same. That is, could some psychotic-like symptoms be an indication of underlying vulnerability, while others might be benign and be due to healthy diversity? Longitudinally we could begin to answer this question by following up individuals with different types of PLE to see if any are more likely to be associated with onset of psychotic disorder. We know that subthreshold PLE in general confer increased risk of development of psychotic disorder, in both community [8, 15] and clinical samples [43–46]. But the literature varies about which particular PLE are associated with increased risk. The clinical studies, based on individuals considered to be at ultra-high risk (UHR) or prodromal for psychotic disorder, found that unstable ideas of reference, and visual and auditory perceptual disturbances [47, 48] and elevated scores on measures of unusual thought content, suspiciousness, perceptual disturbance and conceptual disorganization were associated with increased risk of development of psychotic disorder within UHR groups [21, 45].
We previously investigated a clinical sample of help-seeking non-psychotic young people who were not thought to be at risk of psychotic disorder [49]. This largely depressed group had high levels of undetected subthreshold psychotic experiences. We found that three distinct subtypes of PLE could be identified: bizarre experiences (BE), persecutory ideas (PI), and magical thinking (MT). BE included symptoms such as subthrehold forms of thought broadcasting and perceptual abnormalities (PA). PI included suspiciousness and other subthreshold versions of PI. MT included, for example, belief in the occult and thoughts that telepathy could exist (without actually experiencing it). Cross-sectionally in this sample, BE and PI were associated with distress, depression and poor functioning, but MT was not.
Unlike in clinical samples, community samples have tended to focus on PLE in general, without distinguishing between different types of PLE. Similar to our study of apparently non-psychotic help-seekers [49], we could postulate that PLE found in community samples would be of different subtypes, and that cross-sectionally those that are most likely to be indicative of underlying vulnerability will be those associated with problems in living, such as distress, depression and poor functioning. The aim of the present study was to investigate this issue by measuring PLE in a community sample of adolescents. We chose to study PLE in a sample of adolescents aged 14–16 years, because this would capture a group largely before the onset of first-episode psychosis, which typically begins in late adolescence–early adulthood. Additionally, it was also felt that this would enable us to identify large numbers of adolescents with subtle attenuated psychotic symptoms, because these are thought to be more common in adolescents than adults [15, 50–52].
The purpose of the present study was therefore to determine if different subtypes of PLE could be identified in a community sample of adolescents, and to investigate if particular subtypes were more likely to be associated with psychosocial difficulties, that is, distress, depression and poor functioning, than other subtypes. The hypotheses were as follows.
(1) That different subtypes of PLE would be identified in the sample. We postulated that by factor analysis three subtypes would emerge: BE, PI, and MT. This was based on a factor analysis conducted on a clinical sample of non-psychotic young people [49].
(2) That BE and PI would be associated with distress, depression and poor functioning, but that MT would not. This was based on the findings in the clinical sample.
Method
Procedures and sample
Subjects were recruited via schools that were asked permission to survey their Year 10 secondary students. Sixty secondary schools in the western metropolitan region of Melbourne were approached to participate in the study and 34 consented to participate (20 government, five Catholic and nine independent schools). Students from each school were assessed via questionnaire during one 48 min study period. Trained research assistants were present in the class room to answer queries. The study was approved by Research and Ethics Committees at the University of Melbourne, Victorian Department of Education and the Catholic Education Office. All participants provided written informed consent from themselves and their parent/guardian.
Instruments
PLE were assessed with the Community Assessment of Psychic Experiences (CAPE) positive symptoms scale [53]. This self-report scale measures the occurrence of PLE in the past 12 months on both a frequency scale (1=never, 4=nearly always) and a distress scale (1=not distressed, 4=very distressed). The Centre for Epidemiologic Studies Depression Scale (CES-D) was used to assess level of self-reported depressive symptomatology in the past week. The CES-D consists of 20 items that rate frequency of depressive symptoms from 1 (rarely) to 4 (mostly) [54]. Scores of ≥24 have been used to indicate caseness of depression. The Revised Multidimensional Assessment of Functioning Scale (RMAFS) was used to assess functioning. This is a 23-item self-report scale that generates a Total Functioning score and three subscale scores: General Functioning, Peer Relationships and Family Functioning. For a more detailed description of the RMAFS see [49].
Data analysis
Analyses were conducted using SPSS version 12.0 for Windows (SPSS Inc., Chicago, IL, USA). Data were initially screened for missing values and for the assumptions of normality, linearity, homogeneity and outliers. Six participants had >25% of data missing and were subsequently removed from further analyses, leaving 875 with valid data.
The correlations matrix of the CAPE items was examined. There were many significant correlations between items, indicating that factor analysis was a meaningful technique. A factor analysis of the frequency scale for the CAPE items was run using the maximum likelihood technique with direct oblimin rotation to determine the appropriate number of factors. Two tests were conducted to determine whether the dataset was factorable. First the Kaiser–Meyer–Olkin measure of sampling adequacy tests was used to measure the size of the partial correlations among variables. Values ≥0.60 are required for good factor analysis [55]. The second test was Bartlett's test of sphericity, which assesses whether the factor model is appropriate. The oblique rotation was chosen because it was predicted that the CAPE factors would be correlated.
A number of methods were used to determine the optimum number of factors for the current dataset. First, five factors had eigenvalues >1. Second, the scree plot was inspected. There was a noticeable drop-off at the second and third factors. Both these methods, however, have been criticized as having shortcomings [56], therefore a parallel analysis using a Monte Carlo simulation was conducted.
Once the factor structure was identified, correlations were conducted to assess the relationship between the CAPE total score and subtype scores and measures of functioning and symptomatology. χ2 and t-tests were run to compare scores with variables such as age and gender.
Results
Sample characteristics
From a total potential sample of 4797 Year 10 students, 946 students agreed to participate, a response rate of 19.7%. Sixty-five participants were absent on the day of assessment, reducing the total sample to 881, and six participants had >25% of CAPE data missing, so were excluded from further analysis, making the total number of subjects 875 (response rate 18.2%). There were 411 boys (46.9%), 462 girls (52.8%) and two participants with gender not recorded. Mean age was 15.64 years. Participants were aged between 13.7 and 17.6 years (SD=0.46 years), with one significant outlier of 19.6 years. Only 36 (0.9%) non-consenters returned demographic forms. Given this small sample size demographic details of non-consenters were not examined.
Twenty out of 28 Government schools that were approached agreed to participate, compared to five out of 17 Catholic schools and nine out of 15 independent schools. Government schools were significantly more likely than Catholic schools to participate (χ2(1)=7.563, p=0.006).
Subtypes of psychotic-like experiences
Four subtypes of PLE were found using a Monte Carlo simulation (Table 1). Closer inspection of factor loadings confirmed this solution as best representing the current data. The four-factor solution offered low numbers of cross-loading items (r>0.30 across factors) and low-loading items (r<0.25).
CAPE positive items: factor loading and frequency
CAPE, Community Assessment of Psychic Experiences.
Factor 1 related to BE, Factor 2 to PA, Factor 3 to PI and Factor 4 to MT. Item 13 (‘Have you ever felt that you are a very special or unusual person?’) had equal loading on Factors 3 and 4. A sensitivity analysis was carried out examining the impact of removing item 13 or including the item in either Factor 3 or 4. The internal consistency of the CAPE scale and subscales was maximized by retaining item 13 in Factor 4.
Table 2 presents the means and standard deviations for the total CAPE score and the BE, PA, PI, and MT subscales. There was a significant difference between boys and girls for the total CAPE score and PI, with girls scoring higher.
Descriptive statistics for CAPE total and subscales
BE, Bizarre Experiences; CAPE, Community Assessment of Psychotic Experiences; PA, Perceptual Abnormalities; PI, Persecutory Ideation; MT, Magical Thinking.
Psychometric properties of the four CAPE factors
Inter-correlations between identified subscales were analysed using Pearson's correlation coefficient. Correlations between all subscales were positive and significant (Table 3). BE, PA and PI subscales demonstrated good internal consistency with Cronbach's alphas >0.70, but MT was lower. This was not surprising given the difficulty in obtaining convergence among a low number of items for a subscale with heterogeneous content. The internal consistency of the total CAPE scale was excellent (r=0.85). Only item 11 (have you ever felt as though you were destined to be someone very important?) demonstrated a low item-total correlation (r=0.29). Removing this item did not improve the total alpha, thus all 20 items were retained for further analyses.
Internal consistency and inter-correlations between CAPE subscales (Cronbach alpha)
BE, Bizarre Experiences; CAPE, Community Assessment of Psychotic Experiences; PA, Perceptual Abnormalities; PI, Persecutory Ideation; MT, Magical Thinking.
∗∗p<0.001.
Prevalence of psychotic-like experiences in the sample
To determine the prevalence of each PLE item in the sample, participants’ responses were dichotomized. Responses were recoded to 0 (never) or 1 (at least sometimes). PLE were common in this sample, but prevalence rates varied according to PLE subtypes and frequency (Table 1). PI and MT were the most commonly experienced PLE. More than half of the sample reported that they had experienced one of these PLE ‘at least sometimes’. The prevalence rates for BE and PA were lower and less varied; the majority of participants reported that they had ‘never’ had one of these PLE.
Responses of ‘always/almost always’ were also analysed. Prevalence rates substantially decreased as the frequency rate increased. Very few endorsed experiencing an item within the BE, PA or PI subtypes for a large proportion of time. MT was the most common subtype of PLE experienced ‘always or almost always’.
Distress associated with PLE
Correlations between distress and frequency scores of the CAPE were examined for each subscale and the total CAPE scores. The distress score is a measure of distress associated with the PLE (not a general distress score). The correlation between frequency and distress score for total CAPE score was very strong (r=0.78, p<0.001). The correlation between frequency and distress was very strong for BE and PI (r=0.79, p<0.001 for both), high for PA (r=0.68, p<0.001) but only moderate for MT (r=0.45, p<0.001). Correlations between frequency and distress for the different subscales were compared to determine whether they were statistically different from each other. Subscale totals were converted to z-scores to allow for the different scale ranges. Z-scores were compared using a formula described by Hinkle et al. [57] to examine the difference between two independent correlations. There was no significant difference between BE and PI (z=0, p=1.0). The correlation between frequency and distress for BE and PI was significantly higher than that for PA (z=5.06, p<0.001 for both) and MT (z=12.25, p<0.001 for both). The correlation between frequency and distress for PA was significantly higher than that for MT (z=7.19, p<0.001).
Relationship between PLE and depression
Self-reported depressive symptoms were moderately and significantly correlated with total CAPE scores (r=0.54, p<0.001). Depressive symptoms were moderately and significantly correlated with all subscales, but more weakly correlated with MT than the other subscales (BE r=0.44, PI=0.59, PA=0.35, MT=0.20; p<0.001 for all). Standard linear regression was used with CES-D scores as the dependent variable. Age and gender significantly explained 4% of the variance in CES-D scores (R2=0.04, F(2,861)=19.50, p<0.001). After controlling for the effects of these variables, a series of univariate regression analyses were conducted. Total CAPE score and each subscale were individually input in the second block to determine whether PLE were associated with self-reported depressive symptoms. All CAPE scales significantly explained variance in CES-D scores, indicating that as PLE increased, depressive symptoms also increased (Table 4). BE, PI and PA, however, were associated with a greater increase in depression than MT. That is, for example, for each unit increase in PA, there was a 2.71 unit increase in CES-D score, but for each unit increase in MT there was only a 0.85 increase in CES-D score, indicating that MT had a weaker association with depressive symptoms than did the other types of PLE.
Association between PLE and depressive symptoms
BE, Bizarre Experiences; CAPE, Community Assessment of Psychotic Experiences; CI, confidence interval; PA, Perceptual Abnormalities; PI, Persecutory Ideation; PLE, psychotic-like experiences; MT, Magical Thinking; sr2, amount of unique explained variance in depression scores for each independent variable.
Depression measured by Centre for Epidemiologic Studies–Depression Scale (CES-D).
Relationship between PLE and functioning
Correlations between PLE and self-reported functioning were generally negative and significant, indicating that higher PLE scores were associated with poorer functioning (Table 5). This finding was weaker for the Friends subscale of the RMAFS that measures peer relationships. MT showed a lower correlation across each of the RMAFS scales than CAPE Total, BE, PA and PI.
Correlations between PLE and self-reported functioning
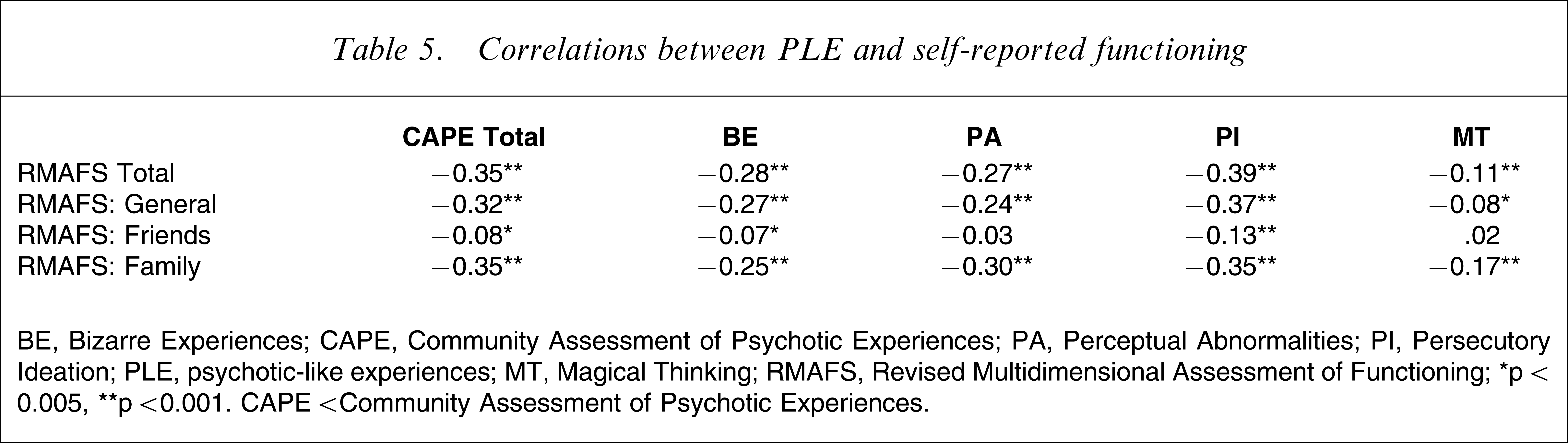
BE, Bizarre Experiences; CAPE, Community Assessment of Psychotic Experiences; PA, Perceptual Abnormalities; PI, Persecutory Ideation; PLE, psychotic-like experiences; MT, Magical Thinking; RMAFS, Revised Multidimensional Assessment of Functioning.
∗p<0.005, ∗∗p<0.001. CAPE<Community Assessment of Psychotic Experiences.
Discussion
Intermittent PLE were common in this sample, but more frequent PLE were less common. For example, nearly 28% of the group reported sometimes hearing voices, but only 1.9% reported this always or nearly always. The rate of 28% is higher than that found in other community studies, with the median hallucination rate in a recent met-analysis being 4% [58]. More than 26% of the present sample reported feeling that their thoughts were being taken away or were not their own but only 0.9% described this as occurring always or nearly always. This is similar to the prevalence found in a representative sample of the Australian population, in which 0.7% experienced thought interference in a way others would find hard to believe [51]. The higher rates in this sample may be due to sampling error, or to certain demographic factors known to be associated with higher reporting of PLE that were consistent with the present sample, such as low socioeconomic status [51], urban environment [11, 59, 60], and younger age [15, 50–52].
As hypothesized, different subtypes of PLE were evident in this community sample. Unlike the clinical sample analysed previously [49], however, an additional factor was found in the present cohort. This was due to the BE factor in the clinical sample being divided into first-rank-type symptoms (such as thought insertion and withdrawal), and PA (such as hearing voices), in this community sample. It is possible that the difference in samples (i.e. community vs help-seeking sample) could account for this finding. It may also be due to the higher numbers in the present sample compared to our previous study.
The second hypothesis was also largely supported, with the findings that BE, PI and PA were more strongly associated with distress, depression and poor functioning than MT. MT was also more commonly and frequently experienced than the other subtypes of PLE.
The present findings suggest that PLE should not be regarded as a homogenous entity. They therefore require greater subtlety in our understanding.
In a given individual, PLE might either be: (i) an expression of an underlying, more fundamental disturbance, such as self or ‘ipseity’ disturbance (a disrupted sense of ‘myness’) at the psychological level [61], or an expression of some neurological disturbance suggesting vulnerability to a psychotic disorder such as schizophrenia; (ii) clinical noise around a non-psychotic syndrome and not necessarily associated with distress, disability, or risk of schizophrenia, these symptoms might be expected to remit with treatment of the non-psychotic illness [62]; we have previously called these ‘incidental’ PLE’ [63]; or (iii) present in non-clinical normal individuals, and not associated with distress or disability or increased vulnerability to psychotic disorder.
In terms of clinical care, PLE belonging to the first category would be of greatest concern, followed by PLE in the second category. PLE in the third category may reflect a form of ‘happy’ [64] or ‘benign’ [65] schizotypy and probably do not warrant clinical attention. In fact, clinical attention for these forms of PLE may have a counterproductive effect by raising anxiety about essentially benign experiences.
A theoretical implication is that both the fully dimensional model of PLE [29, 30] and the quasi dimensional model [1, 2] may be correct. That is, MT may be a normal healthy variant, with no impact either cross-sectionally or longitudinally on mental health, whereas BE, PI and PA may be indicative of underlying vulnerability and may actually, both cross-sectionally and longitudinally, be ‘bad for you’. That is, they are associated with problems in living cross-sectionally, consistent with other community studies. For example Van Os et al. found that more frequent PLE were associated with worse functioning than less frequent PLE [11], and Shevlin et al. found that those with most PLE were more likely to be living alone, unemployed and on a low income [9]. These studies, however, did not distinguish between different types of PLE.
One study limitation was that we relied on a self-report instrument, the CAPE, to assess PLE. Some have suggested that self-reporting and use of lay interviewers may over-estimate the prevalence of PLE, because participants may misinterpret questions [39]. For example Kendler et al. found that 28.4% of the cohort in the US National Comorbidity Survey endorsed one or more probes for psychosis [39]. Only 0.16%, however, were diagnosed as having a narrowly defined psychotic illness. Kendler et al attributed this discrepancy to misinterpretation of probes by subjects or lay interviewers. But there is also evidence that self-report measures can give valid estimates of PLE. Konings et al. and Liraud et al. both showed good correlation between the CAPE [53], and interviewer-rated psychosis [66, 67]. Poulton et al. used self report to assess psychotic symptoms [8]. Responses were reviewed by psychiatrists and clinical psychologists, and the researchers commented that they ‘seemed genuine in content’. Bak et al. re-interviewed 142 subjects who had reported incident PLE and found that 83 of these had genuine PLE [68]. Thus 59 were false positives (i.e. approx. 60% truly had PLE, and 40% did not).
Hence, even allowing for some degree of misinterpretation, these studies suggest a high prevalence of PLE in the community, and thus support for the continuity of psychosis. A recent meta-analysis draws the same conclusion [58].
A major limitation of the present study was the low response rate and lack of demographic details about non-consenters. This is possibly related to needing active consent from participants and their guardians. Furthermore, all adolescents were recruited from the western metropolitan region of Melbourne, a relatively socially disadvantaged group. These two issues raise concerns about the generalizability of our findings. We could speculate that more disturbed and unwell adolescents did not consent, thus underestimating the prevalence of PLE in this population. The overrepresentation, however, of low social economic status could have led to an overestimation. Additionally, only self-report measures were used, possibly resulting in some participants misinterpreting questions and leading to an overestimation. Given these limitations caution is required with generalizing our findings.
Nonetheless, there are two further implications from this research. The first is a practical one. There are many services around the world, including our own, the Personal Assessment and Crisis Evaluation clinic [24], which recruit individuals with PLE on the grounds that they may be at UHR or prodromal for psychotic disorder [21, 23]. This study highlights that, because they are common, PLE are unlikely to be a specific risk factor for onset of psychotic disorder in community samples. Thus the sample, that is, community versus clinical, needs to be considered when taking into account the potential risk of PLE and the need for intervention. This is a base rate issue: the base rate of onset of psychotic disorder in a community sample is much lower than in a clinical sample. Hence, it is much less likely that someone with PLE in the general population will develop a psychotic disorder compared to someone with PLE seeking help [63]. A further practical point is speculative. It may be that not all subtypes of PLE confer the same degree of risk for onset of disorder, for instance, BE, PI and PA may be more strongly associated with increased risk of poor outcome in contrast to MT, given that they were more strongly associated with distress and depression. Further longitudinal research is needed and is currently under way with this sample and clinical samples, both UHR and non-UHR, in order to investigate the developmental course of PLE and their association with onset of psychotic disorder.
Finally, our ability to identify which of the three categories of PLE mentioned earlier (fundamental disturbance, incidental PLE, normal variant) appears in clinical presentations remains poor. This is reflected in our limited capacity at present to predict which UHR patients with attenuated psychotic symptoms will go on to develop full-blown psychotic disorder. A clinical and research challenge remains to further close in on risk factors for psychosis onset by identifying phenotypic factors that predict psychosis onset in addition to PLE. It may be that the presence of PLE in combination with other factors, such as functional decline [45, 48, 63], high levels of distress [69–71] or self-disturbance [72, 73], may place an individual at greater risk of full-blown psychotic disorder. Also, the particular combination of PLE with other factors may be related to onset of particular types of psychotic disorder. The evidence to date suggests the PLE in combination with self-disturbance may be predictive of schizophrenia spectrum conditions [72, 73]; PLE in combination with some other factors, such as mood or personality disturbance, may be more predictive of mood disorder with psychotic features or psychotic episodes in the context of personality disorder. Additionally, identification of endophenotypes or genotypes, in addition to PLE, may aid our prediction of risk within the UHR sample.
The challenge to achieve further specificity in our understanding of PLE is salient given recently observed declining rates of transition to full-blown psychotic disorder in UHR samples [74]. We cannot complacently continue to believe that the UHR criteria indicate prodromal schizophrenia, and that those who do not make transition to psychotic disorder have somehow been prevented from doing so by our intervention.
Conclusion
In the PLE literature there has been a tendency to lump all PLE together. Some PLE, however, could confer higher risk for psychotic disorder than others. There is also a need to consider PLE in adolescents somewhat differently from those in older adults. It seems that PLE are much more common in adolescents [15, 50–52]. Can they be grown out of? These issues can be further explored in longitudinal studies.
Footnotes
Acknowledgements
This research was funded by the Colonial Foundation and an NHMRC Program Grant (350241). The authors gratefully acknowledge the participation of the students and the schools in this research project.