
Abstract
Mental health literacy refers to ‘knowledge and beliefs about mental disorders which aid their recognition, management or prevention’ [1]. Inherent in this concept is the assumption that individuals who have a higher level of mental health literacy will be more willing to seek professional help for themselves or for people they know who may be suffering from a mental health problem. Jorm and colleagues pioneered several studies that examined the mental health literacy of Australians [2,3]. In one study, they found that over 42.5% of the 913 Australians respondents were able to correctly identify schizophrenia as described in a case vignette [2]. Over 76% and 86% considered a family doctor and a counsellor to be helpful in the case, respectively, and 34.4% cited taking anti-psychotic drugs as beneficial for schizophrenia. Furthermore, 32.8% suggested that inpatient treatment could be helpful for the person in the schizophrenia vignette. In Germany, Gaebel et al. found that the German public was not sufficiently informed of the causes of schizophrenia, and that only 33% of respondents in a population survey could name those causes [4]. Lauber and associates conducted a study on the mental health literacy of Swiss people and found that 73.6% of the respondents could identify a schizophrenia vignette as depicting a condition of illness [5]. While the differences in schizophrenia literacy found in the above cited studies may be related to the different instruments used to measure schizophrenia literacy, these differences may also be related to the specific sets of socio-cultural factors in each of these societies; which operate to shape people's perception of schizophrenia and the preference for treatment options.
Very few studies have explored knowledge of schizophrenia among mainland Chinese. Zhang et al. reported that of the 258 participants in their study, 73.6% believed that mental illness is schizophrenia/psychosis; and 20.2% confused dementia with schizophrenia [6]. They also suggested that psychiatric stigma had stopped people from actively seeking proper knowledge of mental illness. However, the lack of information on research designs and measurements in the above-cited study makes it difficult to compare its results with those of overseas investigations. Indeed, given the fact that Chinese socio-cultural contexts and developments are quite different from those in Hong Kong and overseas, it would be interesting to explore knowledge of schizophrenia and variations in preferences surrounding types of professional help, medication, and treatment methods among Chinese people living in mainland China. Such an understanding will help us to generate knowledge facilitating the design of specific public education programmes on schizophrenia-related knowledge among Chinese people residing on the mainland. In the study reported in this paper, we adopted the concept of mental health literacy first proposed by Jorm to conceptualize issues surrounding knowledge of mental illness (specifically, schizophrenia) and preferences surrounding medication and professional help. Using the schizophrenia vignette constructed by Jorm, the findings of this study were compared with those of two recent studies conducted by the first author on schizophrenia literacy among Hong Kong Chinese (Wong D and colleagues: unpublished data, 2010) and Chinese living in Melbourne, Australia [7].
Objectives
To understand the schizophrenia literacy of Chinese people in Shanghai, China.
To explore preferences surrounding professional help, medication, and treatment methods among Chinese people in Shanghai, China.
Method
Sample
A multistage cluster sampling method in which participants were randomly selected from six of the 20 districts in Shanghai, China, was adopted for this study. One resident committee was randomly selected from each district before 1% of the households in each of the six chosen districts were approached. The first adult between the ages of 18 and 60 the research assistants met was then asked to fill out the questionnaire. Potential participants who were interested in the study were briefed on its purposes and procedures and told they could withdraw at any time during the data collection process should they wish to do so. Prospective participants had to be aged 18 or over and be Shanghai Chinese with local residency status (HuKou) to be eligible for inclusion in the study. A total of 644 residents initially agreed to participate and signed the consent form; 76 of the residents ultimately withdrew from the study, while 46 failed to fill out the questionnaire properly (i.e. too many missing data). Eventually, a total of 522 completed questionnaires were collected. The questionnaire took about 40 minutes to complete. The study was endorsed by the Research Ethics Committee of the East China University of Science and Technology, Shanghai, China.
A cluster convenience sampling method was used for both the Hong Kong and Australian studies, and a total of 572 and 200 samples were recruited respectively. All of them were adults over the age of 18 who were permanent residents or citizens of Hong Kong and Australia. The Hong Kong samples were comprised of participants of social activities/programmes run by the various social service organizations in Hong Kong. Data collection was conducted between June 2008 and February 2009, and covered all major districts in Hong Kong. In the sample there were disproportionately fewer men than women (33.1% and 66.9%, respectively). They were relatively well educated, having received secondary and tertiary education, and their mean age was 32.55. Lastly, more than three quarters of the respondents were born in Hong Kong, and only 5.8% had lived in Hong Kong for less than seven years (Wong D and colleagues: unpublished data, 2010).
In the Chinese Australian sample, the data were collected in 2008 from Chinese people living in four major areas of metropolitan Melbourne where most Chinese-speaking Melbournians reside. In the sample, there were more women than men (69.5 versus 30.5%). The majority of the participants were married, with a mean age of 46, spoke mainly Cantonese and Putonghua, and were relatively well educated, having received a senior secondary or tertiary education. Most of them were born in Hong Kong or mainland China and, on average, had migrated to Australia about 10 years previously. About 40% of the participants had full-time or part-time jobs, and their average weekly income was around AUD450. Whereas 41% mentioned that their English proficiency was average, over 46% said they had poor to very poor English [7].
The survey questionnaire
The questionnaire employed in this study was divided into two parts: the first was designed to collect the socio-demographic characteristics of the respondents and the second centred on the mental health literacy scale (schizophrenia vignette). The same questionnaire was used in the above-mentioned mental health literacy studies on the Australian and Hong Kong Chinese, which formed the data base for comparison in the present study.
Schizophrenia literacy
This instrument was adapted from the one used by Jorm et al. in their study of mental health literacy among Australian samples [8]. The original instrument included four vignettes about people with chronic schizophrenia, acute schizophrenia, chronic depression, and major depression. Only the vignette about the person with acute schizophrenia was chosen for this study. The schizophrenia vignette was written to satisfy the diagnostic criteria for schizophrenia according to DSM-IV and ICD-10.
The schizophrenia vignette
John is 24 and lives at home with his parents. He has had a few temporary jobs since finishing school but is now unemployed. Over the last six months he has stopped seeing his friends, and has begun locking himself in his bedroom and refusing to eat with the family or to have a bath. His parents also hear him walking about in his bedroom at night while they are in bed. Even though they know he is alone, they have heard him shouting and arguing as if someone else is there. When they try to encourage him to do more things, he whispers that he won't leave home because he is being spied upon by the neighbour. They realize he is not taking drugs because he never sees anyone or goes anywhere.
After reading the vignette, respondents were asked a series of questions to assess their recognition of the disorder: some questions were aimed at assessing their awareness of mental illness, with others focusing on beliefs about the helpfulness or harmfulness of different professions, medications, and treatment methods. To explore the cultural dimension of Chinese respondents’ beliefs on professional help, medication, and treatment methods, the research team added additional items to the list of options. For example, under ‘professional help’, ‘Chinese medical doctor’ and ‘Chinese traditional healer’ were added to the list. ‘Chinese herbal medicine’ was included as an additional option under ‘medication’ and the traditional Chinese methods of ‘eating nutritious Chinese food/taking supplements’, ‘qigong’, ‘changing feng shui’, and ‘traditional prayer’ were included as choices under the ‘treatment methods’ heading. The English version of the scale was translated into Chinese (Putongua) and back-translated into English by an experienced professional translator.
Statistical analysis
In order to compare the difference in the endorsement of “helpfulness’ of the type of professionals, medications and intervention methods between the three groups of Chinese, a mean score was computed by using a ‘0-1’ method, with ‘1’ denoting a choice of ‘helpfulness’ and ‘0’ for selecting other choices found in each item. Comparisons between Shanghai and Australian Chinese, and Shanghai and Hong Kong Chinese were then conducted using Mann-Whitney U tests. Statistical data management and analyses of the data were carried out using Statistical Package for Social Sciences (SPSS 18.0 for Windows).
Results
In this study, there were slightly more women than men in the sample (53.3% versus 43.5%). The respondents had an average age of 39.1, spoke mainly Putonghua and Shanghai dialect, and were relatively well-educated, having received senior secondary to tertiary education. About 60% of the respondents were married and more than 80% were born in Shanghai. About 78% of the respondents had an annual personal income of RMB40 000 or below (i.e. about US$6500). Over 60% owned a flat and were in full-time employment. In terms of occupation, 31% held technical jobs and 35% did clerical or administrative work.
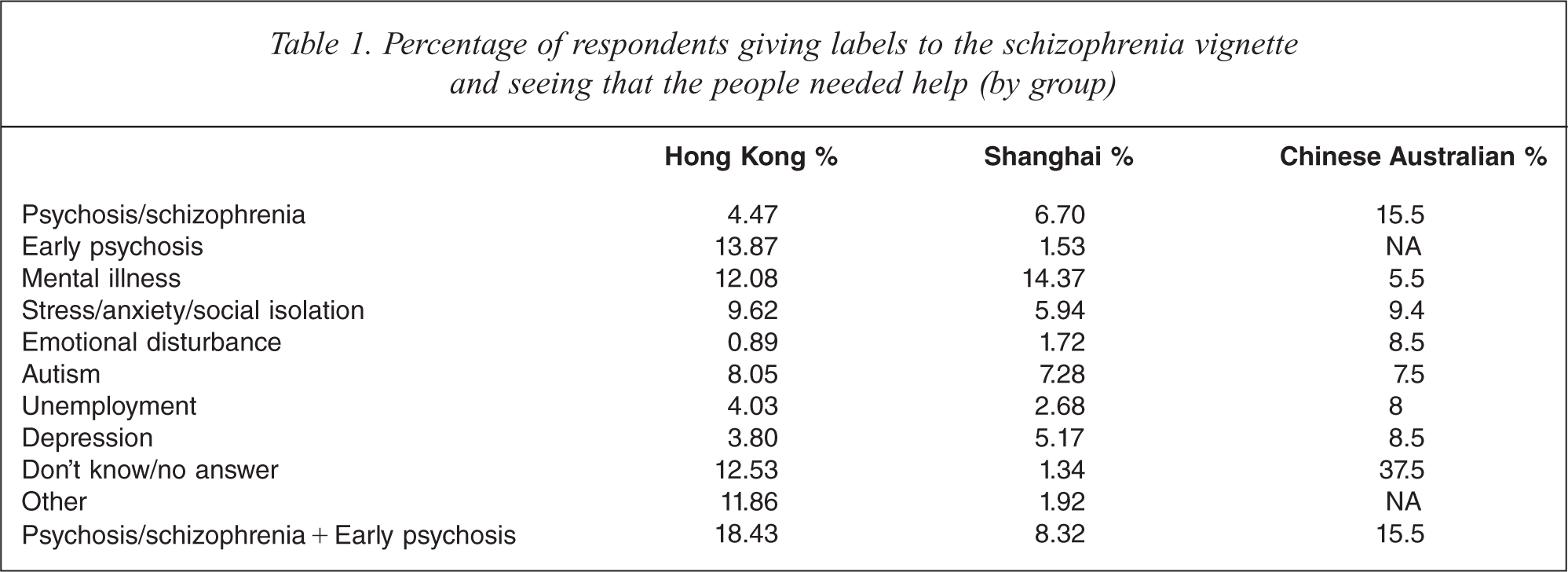
Table 1 shows the percentage of correct identification of the vignette as a condition of schizophrenia by the respondents. A written answer is counted as correct when the respondents wrote in the blank space one of the following three words: schizophrenia, psychosis or early psychosis. The results suggest that there was a lower percentage of Shanghai Chinese (8.32%) than Hong Kong Chinese (18.43%) and Australian Chinese (15.5%) who could correctly identify the condition described in the vignette as a case of acute schizophrenia. However, in comparison with the percentage found in an Australian general population sample (about 64.2%), far fewer people in the Shanghai sample (and indeed fewer than in all Chinese samples previously examined) recognized the vignette as one of schizophrenia. Interestingly, a substantial percentage of Chinese in the Hong Kong sample ascribed the label ‘psychosis’ to the person in the schizophrenia vignette, but only less than 2% and 0% among Shanghai Chinese and Chinese in Australia. In all three samples, similar percentages of respondents (7–8%) considered the vignette a condition of autism – a common misconception held by the Chinese.
Percentage of respondents giving labels to the schizophrenia vignette and seeing that the people needed help (by group)
Fewer Shanghai Chinese endorsed the engagement of professionals (e.g. general practitioners, counsellors, and social workers) or informal network members (e.g. close family members and friends, or religious practitioners) as helpful for the person depicted in the schizophrenia vignette than did so among the Hong Kong and Chinese Australian samples. In particular, counselling professionals (except clinical psychologists) were much less preferred by the Shanghai Chinese than by the Chinese living in Hong Kong and Australia. On the other hand, they had a significantly higher tendency than the other two groups of Chinese to endorse the use of Chinese medical doctors and Chinese traditional healer (Table 2). While the percentage of Shanghai Chinese who endorsed the strategy of ‘deal with it alone’ was significantly higher than the percentage of Chinese Australians who advocated this method, it was more than double that observed in the Hong Kong Chinese sample (Table 2).
Percentage of respondents rating each type of professional as ‘helpful’ for the person in the schizophrenia vignette (by group)
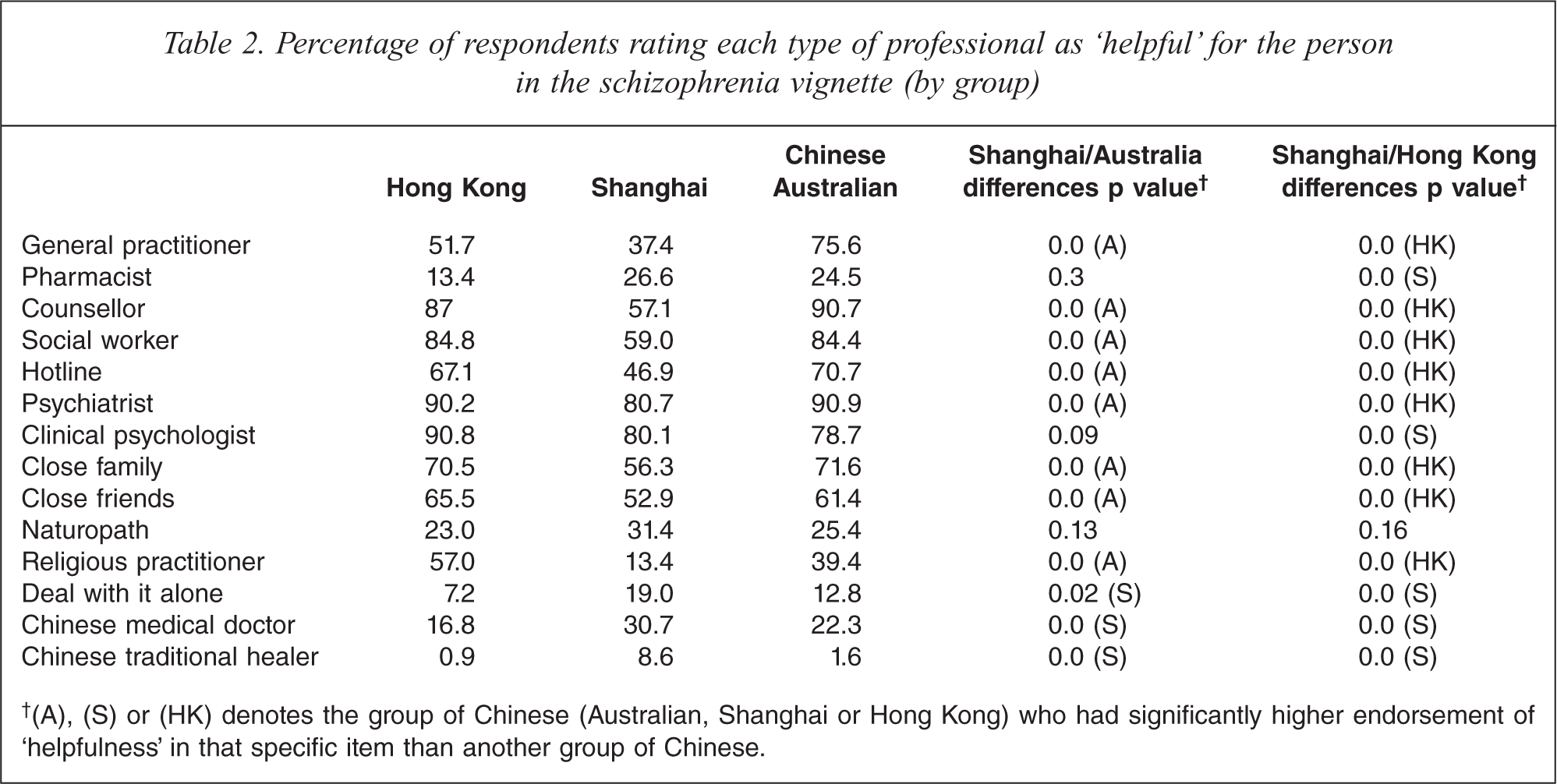
†(A), (S) or (HK) denotes the group of Chinese (Australian, Shanghai or Hong Kong) who had significantly higher endorsement of ‘helpfulness’ in that specific item than another group of Chinese.
Table 3 reveals that the percentage of Shanghai Chinese who endorsed the use of anti-psychotics was similar to the percentages of Chinese living in Australia and Hong Kong who did so (i.e. about 51%). The proportion of Shanghai Chinese who endorsed the use of Chinese herbal medication was significantly higher than the proportion who did so in the other two groups. Table 4 reports the finding that a lower percentage of Shanghai Chinese endorsed ‘lifestyle changes’ for the person described in the schizophrenia vignette than did the other two groups. Generally speaking, a significantly higher percentage of the mainland group advocated psychiatric treatment (i.e. admission to a psychiatric ward and electro-convulsive therapy) and the traditional Chinese practices of ‘eating nutritious food/taking supplements’ and ‘changing fungshui’ than did so in the other two groups of Chinese. Shanghai Chinese and Chinese in Australia had similar percentages of endorsement of ‘qigong’ and the percentages were much higher than that of the Hong Kong Chinese.
Percentage of respondents rating each type of medication as ‘helpful’ for the person in the depression and schizophrenia vignette (by group)
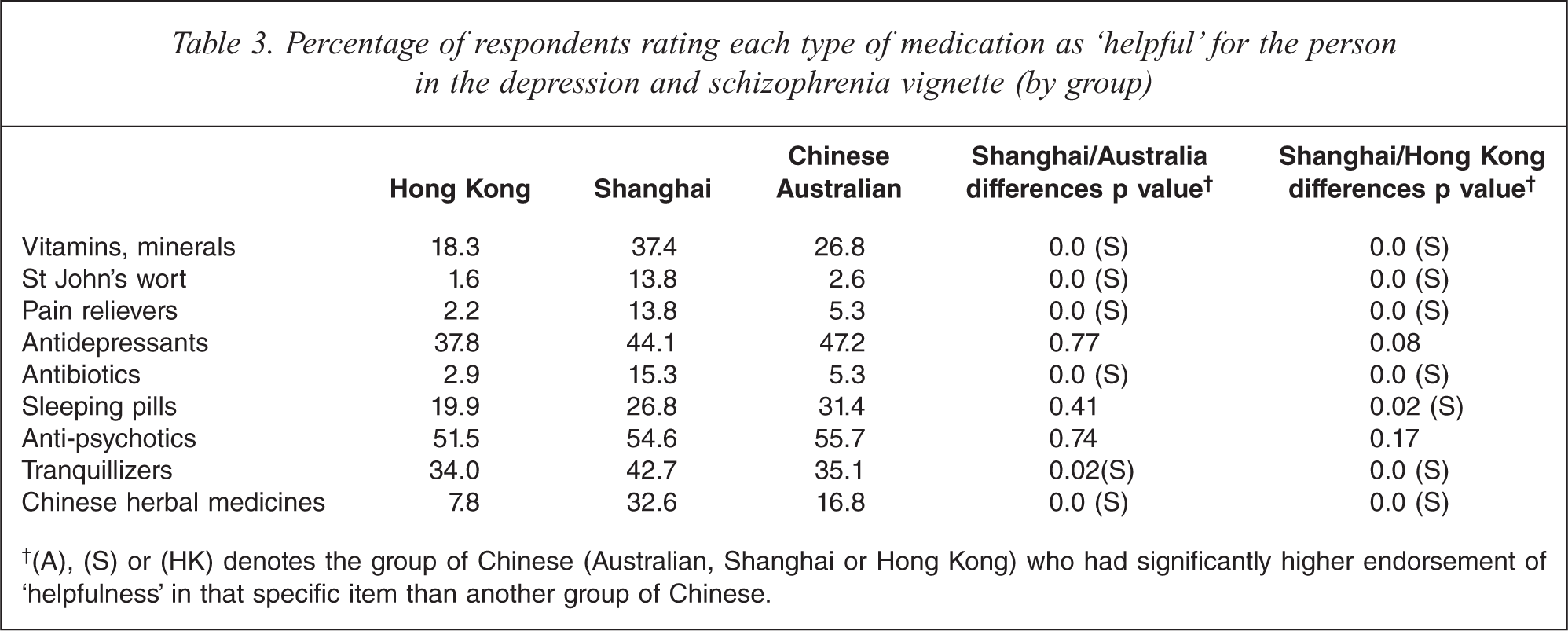
†(A), (S) or (HK) denotes the group of Chinese (Australian, Shanghai or Hong Kong) who had significantly higher endorsement of ‘helpfulness’ in that specific item than another group of Chinese.
Percentage of respondents rating each type of intervention as ‘helpful’ for the person in the schizophrenia vignette (by group)
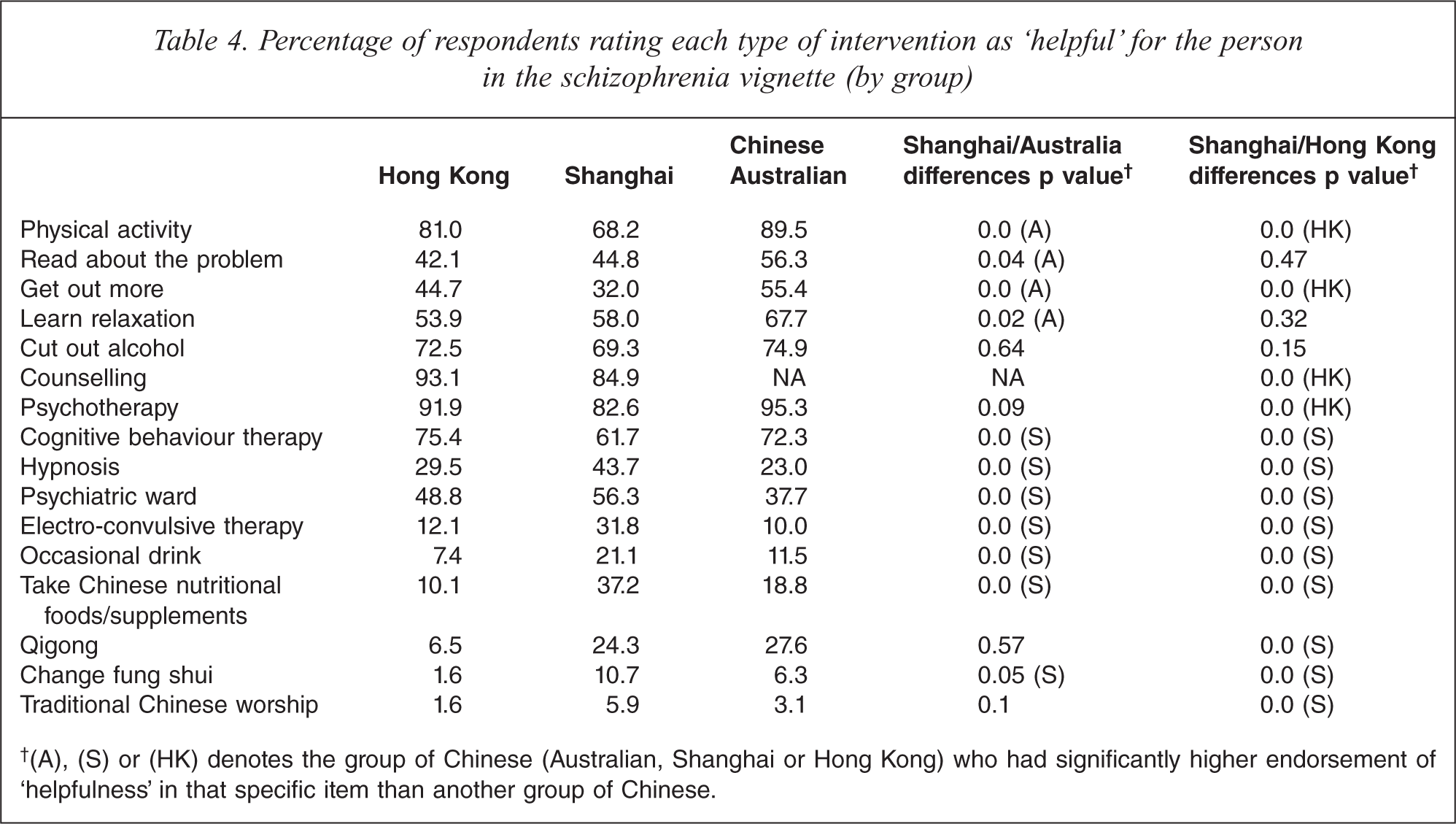
†(A), (S) or (HK) denotes the group of Chinese (Australian, Shanghai or Hong Kong) who had significantly higher endorsement of ‘helpfulness’ in that specific item than another group of Chinese.
Discussion
About 8% of the Shanghai Chinese participants in this study attached a schizophrenia and psychosis label to the vignette, a percentage that was lower than those observed in the Chinese-Australian and Hong Kong Chinese samples. These figures suggest that Shanghai Chinese have a lower level of mental health literacy than do the rest of the comparison samples. Two reasons may be ascribed to explain the findings. First, mental illness is heavily stigmatized in the Chinese culture [10,11]. Traditional beliefs suggest that mental illness is a result of being possessed by demons; improper child bearing practice; or the wrongdoing of one's ancestors [12]. Moreover, mentally ill people are often perceived as dangerous, unpredictable, and incurable [11]. Hence, generally speaking, Chinese people may be hesitant, whether consciously or unconsciously, to perceive and describe a person's condition as one of mental illness. Secondly, in China, due to a lack of public education on mental health and mental illness, mainland Chinese may be more traditional and biased than Chinese in Hong Kong and Australia in viewing mental illness. Indeed, an interesting comparison study of Japanese and mainland Chinese concerning social distance from schizophrenia patients and knowledge of mental illness found that mainland Chinese scored significantly higher in social distance from schizophrenia patients and lower in knowledge of symptoms of schizophrenia than the Japanese people [13]. Given the above information, it is not surprising to find that Shanghai Chinese had a relatively lower percentage of recognition of schizophrenia and psychosis than those of the Hong Kong and Australian Chinese in Melbourne. Public education is therefore needed to enhance the mental health literacy of the general public in order to foster proper attitudes towards people with schizophrenia and psychosis.
Another observation deserving attention is that: all of the three Chinese population groups in this study had on average a 14% correct identification of schizophrenia; a percentage which is much lower than that found in other countries such as Australia (i.e. 42.5%) [2]. Such a lower rate of correct identification may be related to the Chinese cultural conception of schizophrenia. In Chinese culture, severe mental illness is characterized by two different states: dian, which is a psychotic condition without excitation, and kuang, which is a psychotic condition with excitation [14]. These two psychotic states are both perceived to be signs of madness, with kuang in particular denoting a sense of unpredictability, dangerousness and bizarre and uncontrollable behaviour. Chinese people perceive schizophrenia very negatively, and there is a great deal of personal and social stigma attached to the schizophrenia label [11]. It is not uncommon for Chinese people to deny the existence of psychotic illness and to ascribe alternative and more socially acceptable labels to describe a condition [14,15]. The possible consequences of denial or avoidance may include a delay in seeking professional help and a reinforcement of the stigmatizing label, because the fear generated by the stigma drives the general public away from people with mental illness [16] and limits the public's understanding of mental illness.
Generally speaking, psychosocial treatments were less preferred than medical treatments by the Shanghai Chinese. Specifically, the counselling professionals (except clinical psychologists) were much less preferred by the Shanghai Chinese than by the Chinese living in Hong Kong and Australia. Moreover, there was a relatively low percentage of Shanghai Chinese who endorsed the notion of ‘lifestyle changes’ as helpful for the person depicted in the vignette than did so among the Chinese Australian and Hong Kong Chinese groups. Socio-cultural factors may be put forward to explain these findings. In China, counselling is a fairly new profession and the general public may not be aware of its existence. Nor are mainland Chinese aware of the roles and functions of counselling professionals. Taking social work as an example, although many social work schools have been established in China over the past 20 years, the number of government-funded social work positions is still very low [17]. In contrast, the counselling professions have become an integral part of the helping professions in modern urban societies such as Hong Kong and Australia.
The relatively low percentage of endorsement of ‘lifestyle changes’ among Shanghai Chinese may be explained in two ways. First, in modernized societies such as Australia and Hong Kong, ‘being active’ is a sign of good health [18]. Individuals in these societies pay to participate in physical and relaxation activities such as going to the gym, massage, and pilates to enhance their sense of wellbeing and feel relaxed. However, Shanghai Chinese have probably not caught up with this trend and therefore did not endorse a strategy of ‘lifestyle changes’ as strongly as their counterparts. Secondly, community-based psychosocial treatment facilities are fairly new and underdeveloped in China [19]; the general public are usually unaware of the nature and functions of these activities. In the past two years, the Chinese government has begun to dedicate more resources to develop community-based psychosocial treatment facilities and to train community mental health workers in a few major cities in China. It becomes very important to educate the general public so that they can acquire better understanding of the nature, functions and roles of these facilities and the personnel involved in the holistic treatment of a person with schizophrenia.
As mentioned, this study finds a higher percentage of Shanghai Chinese who endorsed medical treatments (i.e. ‘admission to a psychiatric ward’ and ‘ECT’) than Chinese in Hong Kong and Australia. Moreover, the proportion of Shanghai Chinese who endorsed Chinese herbal medicine as helpful for the person described in the schizophrenia vignette was much higher than in the Chinese Australian and Hong Kong Chinese groups (32. 6%, 16.8%, and 7.8%, respectively). Indeed, about 30% of the participants in this Shanghai study believed that ‘Chinese medical doctors’ could be helpful to the person depicted in the schizophrenia vignette. Thus, it seems that Chinese people living in Shanghai are more ready to accept western and traditional Chinese medicine (TCM) as options for people with schizophrenia. In China, Chinese people do not see traditional Chinese medicine and western medicine as incompatible [20], and it is not uncommon to adopt both western and Chinese medicine in treating certain illnesses. On the other hand, they believe that Chinese medicine is useful in maintaining health and preventing illness from occurring. Therefore, not only is it important to educate Shanghai Chinese on the roles; and advantages and disadvantages of taking Chinese herbal medicine and other treatments such as qigong alongside western medication, but it is also essential to foster knowledge of psychiatric illness among traditional Chinese medical doctors.
Limitations
This study is subject to several limitations. First, the three samples are not totally comparable in that the Hong Kong sample was slightly younger than the other two samples; this might affect interpretation of the comparison data. Second, the findings based on the Shanghai sample may not be generalizable to other parts of China due to evidence of regional differences.
Conclusion
This study demonstrates that socio-cultural and structural factors might have subtly influenced the different preferences surrounding the endorsement of different types of counselling professionals, medication, and treatment for people with schizophrenia among Shanghai Chinese and Chinese in Australia and Hong Kong. Effective public education campaigns that have been successful in improving mental health literacy among Chinese communities in Australia and Hong Kong may be adopted or modified to enhance knowledge and awareness of mental health issues among Shanghai Chinese.
Footnotes
Acknowledgements