
Abstract
Medicines are a major modality of treatment for most mental illnesses with more than 11% of prescriptions in Australia being mental health related in 2007–2008 [1]. Pharmacists are among the most accessible health professionals and are frequently consulted for advice on psychotropic medicines [2]. Medication counselling provided by pharmacists has been shown to improve adherence to medications used for mental illnesses [3,4]. Pharmacist-led medication reviews may help identify and resolve psychotropic medication-related problems [5,6]. However, mental health stigma and lack of knowledge of mental illness can interfere with and limit professional practice [7,8]. Research has shown that there is dissatisfaction with the quality and quantity of drug information provided to people with a mental illness and there is consumer demand for advice on the use of psychotropic medicines [8,9]. Pharmacists have similar negative beliefs about depression to the general population [10] and suboptimal attitudes towards mental illness are common among health care professionals [11]. Professional services delivered by pharmacists are potentially well suited to optimizing the use of medicines for patients with a mental illness, but as yet there are no specific roles for community pharmacists in the delivery of mental health care [12].
The lack of mental health education for pharmacists has been described as a main barrier to the successful provision of pharmaceutical services for consumers with a mental illness [13]. The World Health Organization recognizes that good communication skills are essential for all health care workers engaged in mental health care [14]. Pharmacists have stated they monitor patients with mental illness less frequently than patients with cardiovascular problems [7]. Difficulties in communication, lack of knowledge about mental illness, and inadequate mental health education have been cited as barriers to pharmacists providing mental health care [7,15]. In part, these barriers may arise due to a poor understanding of the helpfulness of mental health treatments and likely outcomes.
The Australian Pharmacy Council (APC) has recently developed a set of the professional capabilities expected of pharmacists in the provision of mental health care [16]. The mental health related content of undergraduate pharmacy degree programmes in Australia has not been systematically evaluated. However, pharmacy students in Australia typically receive a brief lecture and tutorial-based overview of common and disabling mental disorders including depression, anxiety, psychosis and substance abuse. Pharmacy students are taught basic communication skills. However, only rarely does this include skills specific to communicating with people with a mental illness. It is anticipated that this mental health capability statement will be used to guide the content and conduct of pharmacy education programmes at universities around Australia and intern training programmes. The statement also describes the required knowledge and methods of application to enable pharmacists in Australia to be capable of providing appropriate care to people with a mental illness.
Jorm and colleagues have defined the term ‘mental health literacy’ (MHL) as ‘the knowledge and beliefs about mental disorders which aid their recognition, management or prevention’. MHL also includes the ability to recognize specific mental health disorders; knowing how to seek mental health-related information; knowledge of risk factors and causes, of self-treatments and of professional help available for mental disorders [17]. The consequences of poor MHL may be a hindrance of public acceptance to evidence-based mental health care and may also limit the early detection and recognition of mental disorders in the community [17,18].
There have been improvements in the mental health literacy of the Australian public over the previous decade [19,20]. In addition, previous studies have measured the MHL of a number of health care professionals including general practitioners, psychiatrists, psychologists and nurses. These studies have found that health professionals generally rate long-term outcomes more negatively and are more likely to perceive discrimination in the community as a possibility than members of the public [17,21,22]. This difference in views between the public and health professionals is thought to lead to an unwillingness to seek or accept professional help for mental health concerns [17,23]. However, currently there is no published data on the MHL of pharmacists. Hence an understanding of the mental health literacy of pharmacists will help inform the development of multidisciplinary strategies in the ongoing delivery of mental health care.
The overall aim of this study was to assess the beliefs of pharmacists about the helpfulness of interventions for schizophrenia and depression. The specific objectives were to measure the MHL of pharmacists in New South Wales (NSW) and compare to the MHL of other health care professionals in Australia and to explore the impact of age, gender, area of pharmacy practice and experience with mental illness on the MHL of pharmacists in NSW.
Materials and methods
Study design
In November 2009 a survey instrument was mailed to a random sample of 2000 out of 8328 pharmacists registered with the Pharmacy Board of New South Wales in November 2009. The Pharmacy Act of 1964 requires that all practising pharmacists in New South Wales be registered with the Board. The mail-out was conducted by an external organization and the researchers did not have access to the contact details of the pharmacists selected. A reminder letter was sent out three weeks after the initial mail-out to those pharmacists who had not yet responded. The study was approved by the Human Research Ethics Committee at the University of Sydney.
Survey instrument
The survey instrument contained a measure of mental health literacy previously developed by Jorm and colleagues [24,25]. MHL is tested using a structured interview taken from the National Survey of Mental Health Literacy [26]. The interview has previously been modified to a questionnaire for self-completion to be suitable for health professionals [24,25]. Vignettes of a person with either depression or psychosis were presented. The sex of the person described in the vignette was randomly assigned to be either male (John) or female (Mary). The vignettes are based on the DSM-IV [27] and ICD-10 [28] diagnostic criteria for major depression and schizophrenia, and participants randomly received one of four versions of the MHL vignette.
The depression vignette was as follows: ‘John is 30 years old. He has been feeling unusually sad and miserable for the last few weeks. Even though he is tired all the time, he has trouble sleeping nearly every night. John doesn't feel like eating and has lost weight. He can't keep his mind on his work and puts off making any decisions. Even day-to-day tasks seem too much for him. This has come to the attention of John's boss who is concerned about his lowered productivity.’
The schizophrenia vignette was as follows: ‘John is 24 and lives at home with his parents. He has had a few temporary jobs since finishing school but is now unemployed. Over the last six months he has stopped seeing his friends, and has begun locking himself in his bedroom and refusing to eat with the family or to have a bath. His parents also hear him walking about in his bedroom at night while they are in bed. Even though they know he is alone, they have heard him shouting and arguing as if someone else is there. When they try to encourage him to do more things, he whispers that he won't leave home because he is being spied upon by the neighbour. They realize he is not taking drugs because he never sees anyone or goes anywhere.’
Respondents are then asked an open ended question ‘from the information given, what, if anything, is wrong with John/Mary?’ Responses were coded as correct for the depression vignette if ‘depression’, ‘depressed’, ‘affective disorder’ or ‘mood disorder’ was mentioned. For the schizophrenia vignette responses were considered correct if ‘schizophrenia’, ‘schizoaffective disorder’ or ‘psychosis’ was mentioned. Respondents were then asked a series of questions about the helpfulness of various interventions, which they rated as either ‘helpful’, ‘neither’ or ‘harmful’. Further questions related to the person in the vignette's likely prognosis with and without professional help and the likelihood of the person being discriminated against. Respondents were also asked about the likelihood (‘more likely, ‘just as likely’, or ‘less likely’) of the person's long-term functioning compared to other people in the community with regard to ten potential outcomes. The ten outcomes, five positive and five negative, were: ‘to be violent’, ‘to drink too much’, ‘to take illegal drugs’, ‘to have poor friendships’, ‘to attempt suicide’, ‘to be understanding of other people's feelings’, ‘to have a good marriage’, ‘to be a caring parent’, ‘to be a productive worker’ and ‘to be creative or artistic’ [26,29].
Demographic data were also collected including age, year of registration as a pharmacist, gender, main area of practice, country of birth, parent's country of birth and personal and family experience of mental illness.
Data analysis
Data were analysed using SPSS version 17.0. Basic descriptive analyses were conducted as well as Mann-Whitney or Kruskal-Wallis tests to ascertain whether the pharmacist responses were affected by areas of practice, gender, personal and family experience with mental illness and age categories. Mann-Whitney U tests were used to identify any differences in the categorical variables gender, age and personal and family experience with mental illness in both the depression and schizophrenia vignettes. Two age categories were created for the analysis, less than 48 years of age (median age) and greater than 48 years of age. Kruskal-Wallis tests were used to identify any differences between the respondents based on their primary area of pharmacy practice. Only differences between community or hospital pharmacy practice were investigated as the numbers working in the other areas were too small to be meaningful. If a significant result was found from a Kruskal-Wallis test, further Mann-Whitney U tests were conducted to identify where the differences lie. As only community and hospital practice was compared, only one post-hoc test was conducted and therefore no Bonferroni corrections were required for multiple tests. A significance level of p < 0.05 was chosen for all other analyses.
Results
Demographics
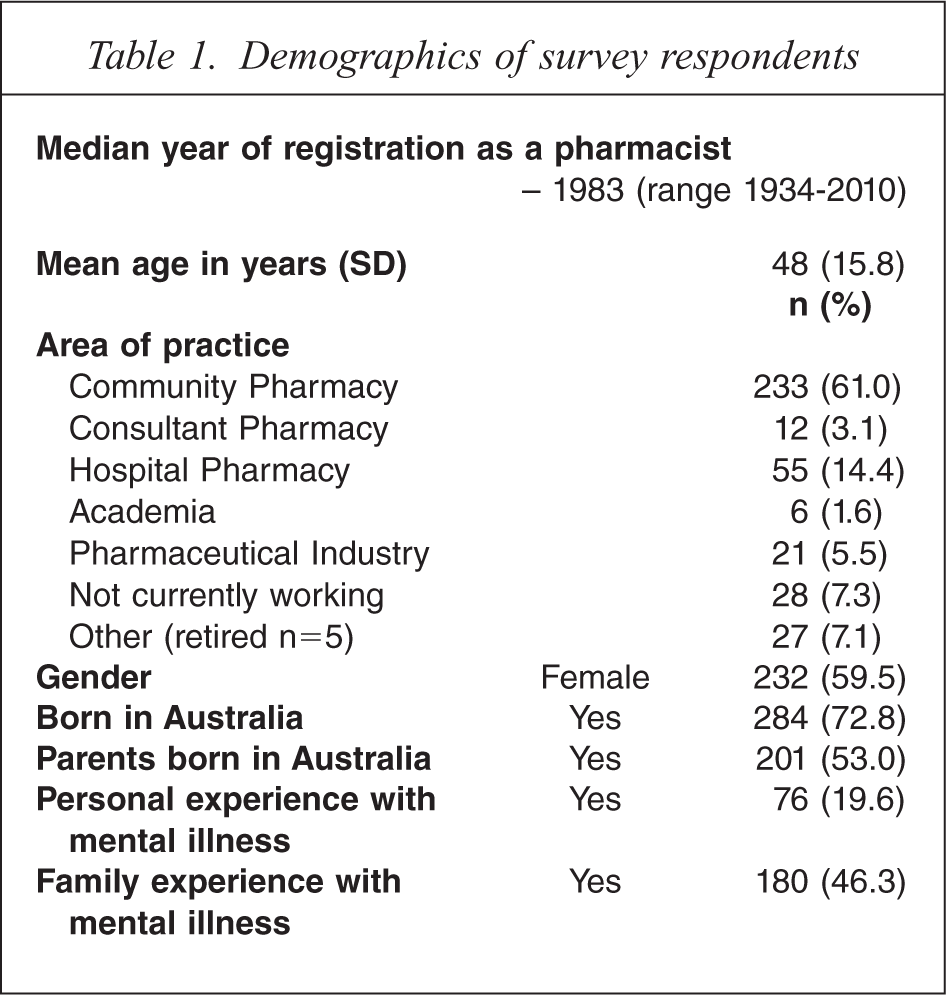
A total of 391 responses were received, representing a response rate of 19.5%. The mean age of the respondents was 48 years, the median year of registration as a pharmacist was 1983 and 60% (n = 232) were female (Table 1). The majority of pharmacists nominated community pharmacy (61%) as their main area of practice followed by hospital pharmacy (14%). Twenty per cent of pharmacists reported having personally experienced a mental illness and 54% had a member of their immediate family who experienced a mental illness. These figures are consistent with the rates of mental health problems in the Australian public [1].
Demographics of survey respondents
Identification of mental illness
Depression was correctly identified by 92% (n = 187) of pharmacists from the depression vignettes with 79% (n = 147) correctly identifying the schizophrenia vignettes as either schizophrenia or psychosis. For both vignette types 99% of pharmacists identified the need for professional help.
Helpfulness of interventions
For the depression vignettes GPs and clinical psychologists were rated as the most helpful followed by counsellors, psychiatrists, telephone counselling services then pharmacists (Table 2). Only 8% of pharmacists thought it would be helpful for John/Mary to handle their depression on their own, with 19% rating a naturopath or herbalist as helpful. For the schizophrenia vignettes psychiatrists were rated as the most helpful followed by GPs, clinical psychologists then counsellors. Younger pharmacists were more likely to rate help from family and friends and counselling services as more helpful in depression (p = 0.02) or help from a social worker in schizophrenia (p = 0.02) than older pharmacists. Pharmacists rated themselves as less helpful in schizophrenia (72%) than in depression (76%), although this difference was not statistically significant. However, community pharmacists (88%) were significantly more likely to rate their own profession as helpful in depression compared to hospital pharmacists (59%), p < 0.001. Naturopaths and dealing with problems on your own rated much lower for the schizophrenia vignettes with only 7% and 1% of pharmacists rating these interventions as helpful, respectively. Younger pharmacists were significantly more likely to rate naturopaths as helpful in both vignettes (p = 0.02). Respondents with a personal experience of mental illness were significantly more likely to rate telephone counselling as helpful (p = 0.01) and significantly less likely to rate a special diet as helpful in depression (p = 0.03) (Table 2).
Helpfulness of different interventions
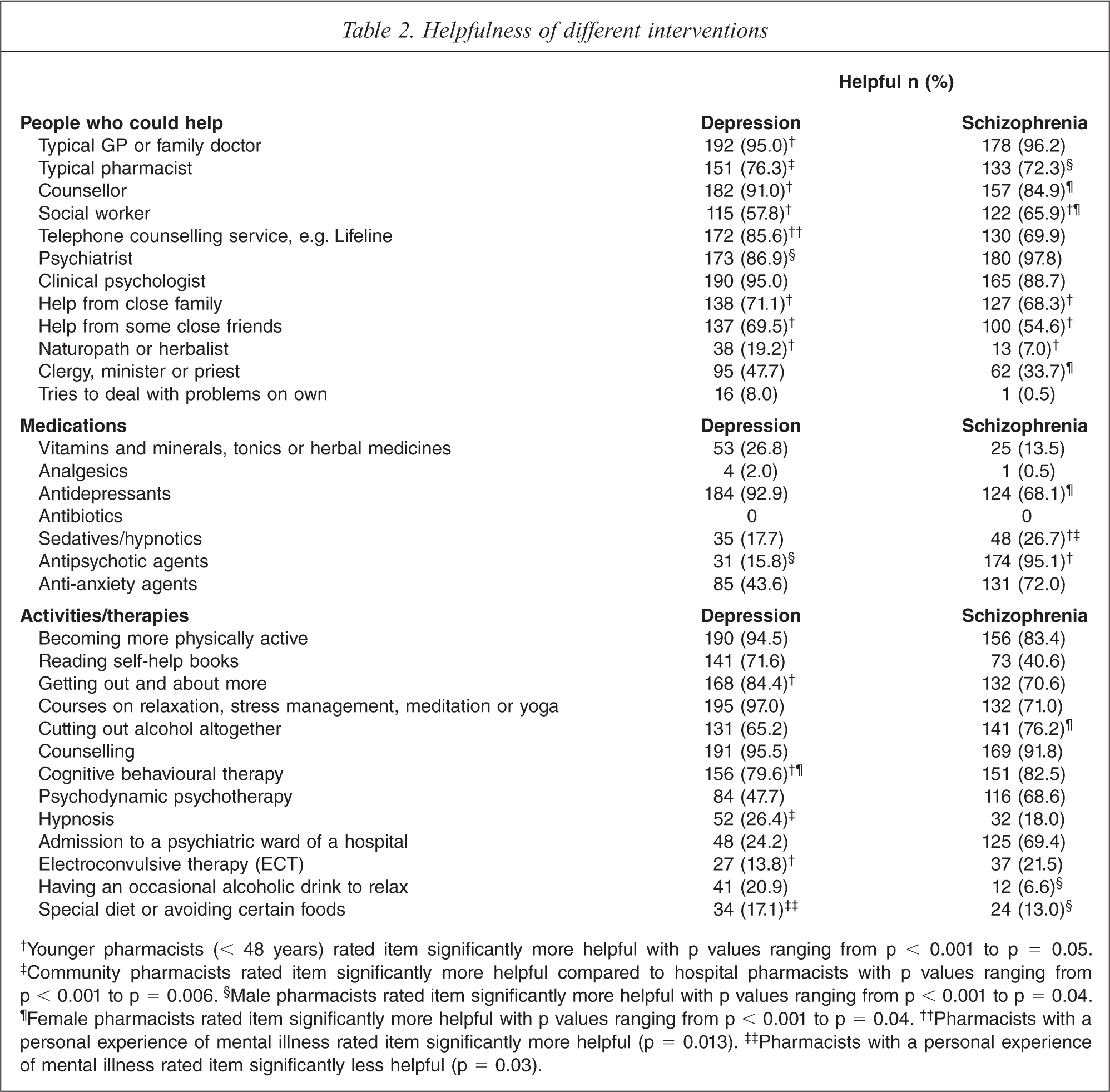
†Younger pharmacists (< 48 years) rated item significantly more helpful with p values ranging from p < 0.001 to p = 0.05. ‡Community pharmacists rated item significantly more helpful compared to hospital pharmacists with p values ranging from p < 0.001 to p = 0.006. §Male pharmacists rated item significantly more helpful with p values ranging from p < 0.001 to p = 0.04. ¶Female pharmacists rated item significantly more helpful with p values ranging from p < 0.001 to p = 0.04. ††Pharmacists with a personal experience of mental illness rated item significantly more helpful (p = 0.013). ‡‡Pharmacists with a personal experience of mental illness rated item significantly less helpful (p = 0.03).
For the depression vignettes 93% of pharmacists agreed that antidepressants would be helpful, followed by anti-anxiety agents, vitamins and minerals and hypnotics. While for the schizophrenia vignettes, 95% of respondents agreed anti-psychotic agents would be helpful followed by anti-anxiety agents, antidepressants and hypnotics (Table 2). Younger pharmacists were significantly more positive about the use of anti-psychotics (p = 0.049) and hypnotics (p = 0.008) in schizophrenia. Area of practice also influenced the helpfulness rating of the use of hypnotics in schizophrenia with 88% of hospital pharmacists identifying hypnotic use as harmful compared to only 44% of community-based pharmacists.
Courses on relaxation and yoga, counselling and becoming more physically active were the activities or therapies that were rated as most helpful for depression; while electroconvulsive therapy (ECT) and admission to a psychiatric ward were among the least helpful interventions. The result for ECT for the schizophrenia vignette was similar to depression; however 69% of pharmacists identified being admitted to hospital for schizophrenia as helpful. ECT and cognitive behavioural therapy (CBT) were looked upon significantly more favourably by younger pharmacists in the management of depression, p < 0.001 and p = 0.015 respectively (Table 2). The more positive response towards CBT is also true for the female pharmacists (who are generally younger as well).
Long-term outcomes
The majority of pharmacists thought discrimination by the community was highly likely (61% for depression and 89% for schizophrenia) and rated long-term prognosis as poor without appropriate professional help (Table 3). Respondents with a personal experience of mental illness were significantly more likely to rate the person in the depression vignette to have a full recovery with no more problems (p = 0.007). Females and younger pharmacists were significantly more negative towards long-term outcomes including the likelihood of attempted suicide, violence, illegal drug use and drinking too much; while those with a personal experience of mental illness were more likely to think the person would be more understanding of feelings (Table 4).
Long term outcomes for the person described in the vignette
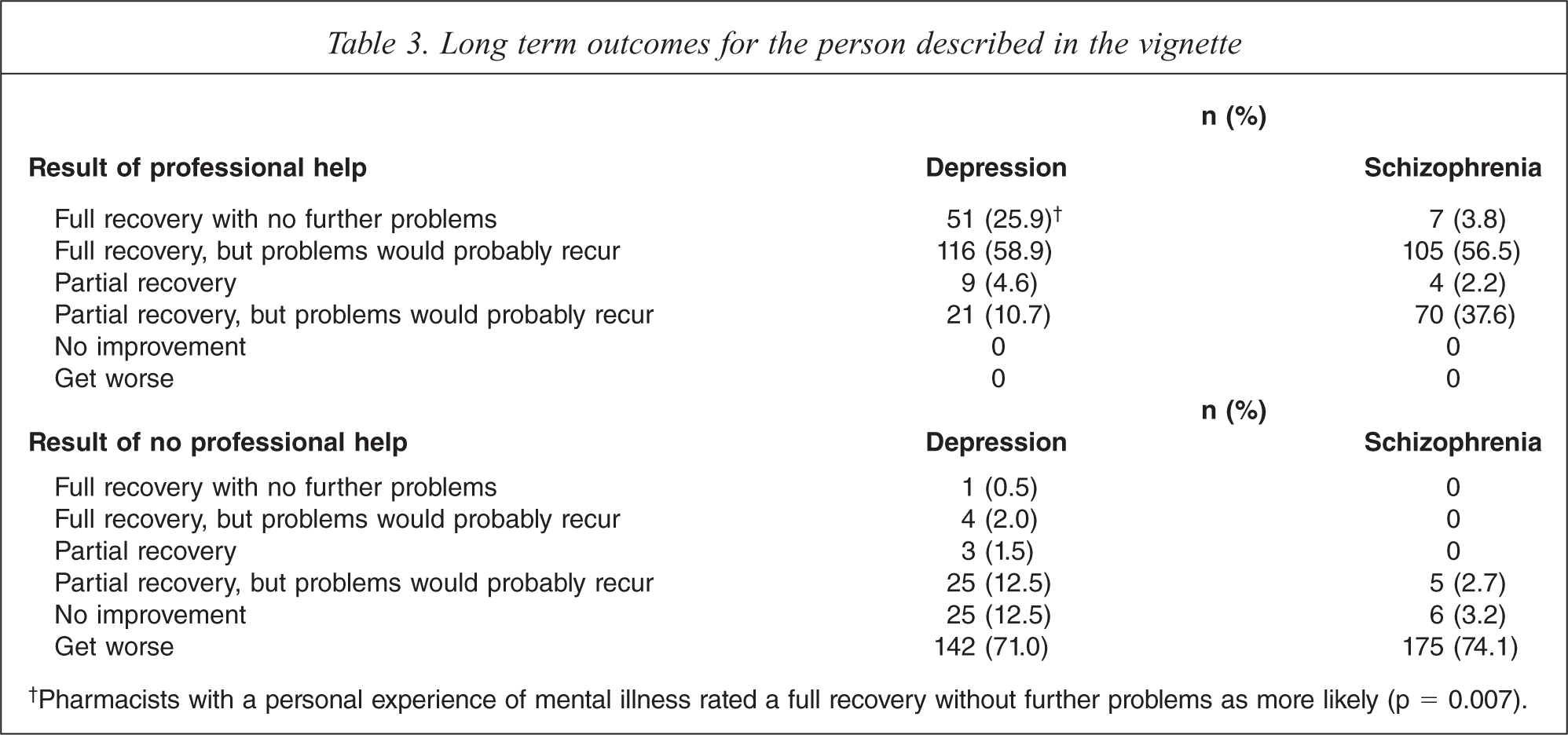
†Pharmacists with a personal experience of mental illness rated a full recovery without further problems as more likely (p = 0.007).
Likelihood of person's long term functioning compared to other people in the community if treatment is received
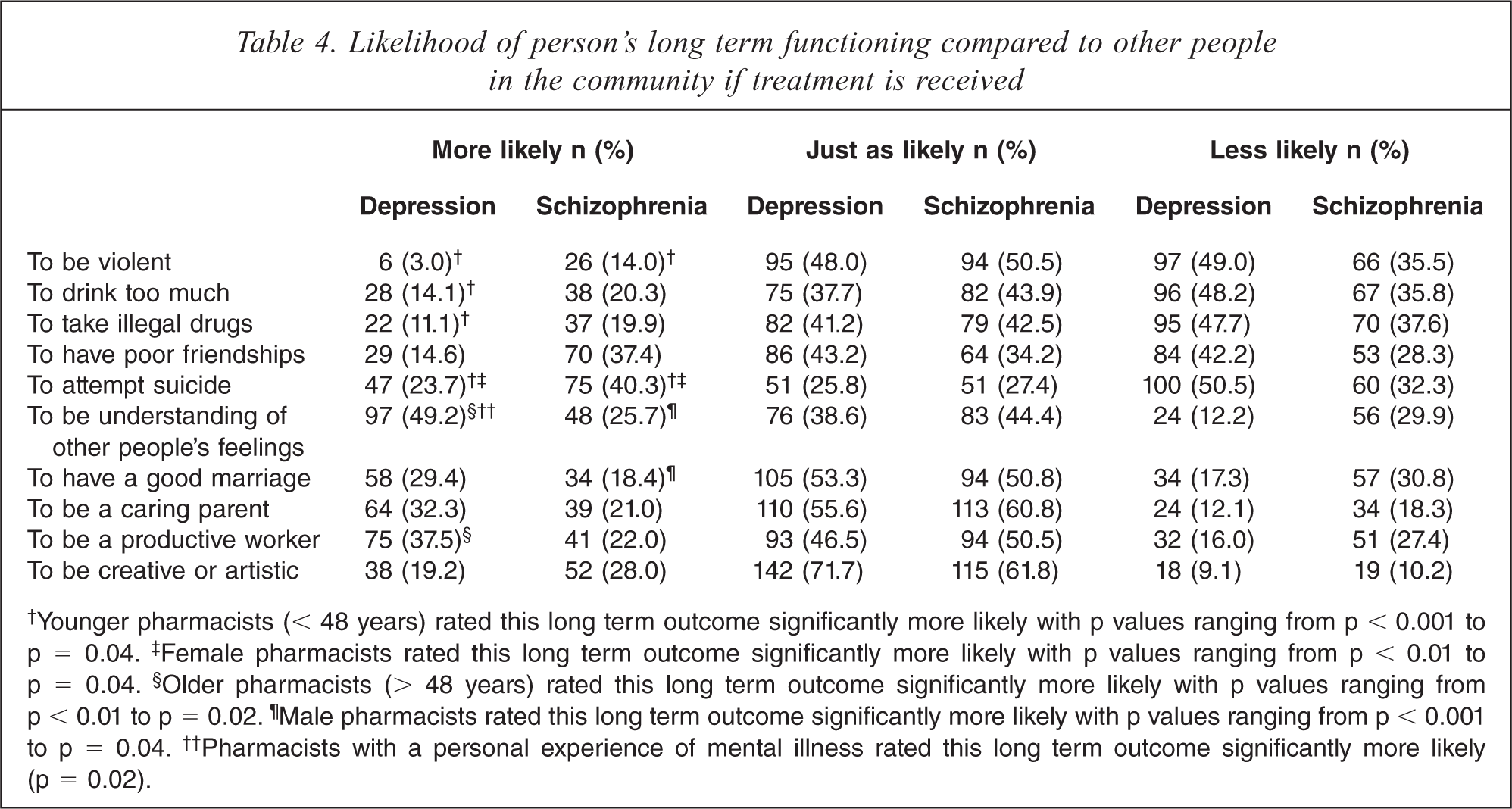
†Younger pharmacists (< 48 years) rated this long term outcome significantly more likely with p values ranging from p < 0.001 to p = 0.04. ‡Female pharmacists rated this long term outcome significantly more likely with p values ranging from p < 0.01 to p = 0.04. §Older pharmacists (> 48 years) rated this long term outcome significantly more likely with p values ranging from p < 0.01 to p = 0.02. ¶Male pharmacists rated this long term outcome significantly more likely with p values ranging from p < 0.001 to p = 0.04. ††Pharmacists with a personal experience of mental illness rated this long term outcome significantly more likely (p = 0.02).
Discussion
This is the first study to assess the mental health literacy of pharmacists. The majority of pharmacists had a high degree of MHL as indicated by the correct identification of, and support of evidence-based interventions for mental illnesses. This finding is promising as pharmacists are very accessible health care professionals, have regular contact with patients and this demonstrates their potential role in screening and referral of people to the appropriate care when there are early warning signs of a mental illness.
Pharmacists’ views of the helpfulness of interventions in depression more closely align with GPs compared to psychiatrists or clinical psychologists in previous studies of MHL [24]. Pharmacists were more likely to rate themselves as helpful than the other professions and the public. This is consistent with previous studies where respondents have rated their own professions as most helpful [24,30]. For all the vignettes pharmacists were more likely to rate pharmaceutical interventions as helpful compared to the other professions; including GPs, psychiatrists and clinical psychologists [24]. This is consistent with previous studies that show that health professionals rate the interventions they specialize in as most helpful [24,25,30].
Pharmacists views on ECT were quite negative which is similar to the views of the public and most health professionals, except psychiatrists [25]. It is worth noting that younger pharmacists had significantly more positive views on the use of ECT even though contemporary pharmacy programmes tend to focus on the pharmacological, rather than the non-pharmacological, management of mental illness. Pharmacists were also quite negative about admission to a psychiatric ward in schizophrenia, making pharmacists the only health profession that does not see the benefits of hospital admission in schizophrenia [24,30].
Pharmacists’ long term views of mental illness are similar to other health care professionals who rate discrimination as more likely, and long-term outcomes without professional help more negatively than the public [17]. It is debatable whether these views are more realistic, as opposed to negative, when compared to the public. These views may be biased as health care professionals have more contact with people with a mental illness. Pharmacists have regular contact with individuals who have a chronic mental illness which may lead to more negative attitudes. Although this contact is regular, it is also brief and pharmacists may not know patients’ complete medical histories like other health care professionals. Previous research comparing the attitudes towards mental illness of intern pharmacists and pharmacy students showed no difference between the groups indicating that more than contact in the workplace alone needs to be done to improve attitudes towards mental illness [31]. Contact with consumers in an educational setting for pharmacy students can lead to sustained decreases in mental health stigma and improvements in their attitudes towards providing pharmaceutical services for mental health consumers [32,33].
Pharmacists generally reported negative views about the general long-term outcomes or likelihood of discrimination for people with a mental illness. However, when asked about the likelihood of specific positive and negative outcomes, they reported a wide range of views. Pharmacists were more likely than any other profession to rate negative outcomes such as ‘being violent’ or ‘taking illegal drugs’ as less likely for both schizophrenia and depression [17,25]. These views are consistent with the public views of various long-term outcomes for people with schizophrenia or depression compared to anyone else in the community [17,25]. Some of these results could be seen as optimistic, as someone who has a diagnosis of schizophrenia as described in the vignette could be expected to be more likely to experience a negative outcome such as abusing alcohol or being violent. Pharmacists may be unaware of how their own views impact on the mental health care they provide.
People with schizophrenia or depression are at greater risk of suicide than the general population [34]. However 51% of pharmacists rated the risk of attempted suicide as less likely for someone with depression, with 32% of pharmacists rating the risk as less likely for someone with schizophrenia. These results are comparable to the views of the public about the likelihood of suicide [17]. There were significant influences on the likelihood of attempted suicide from both the gender and age of pharmacists. Female and younger pharmacists were significantly more inclined to rate the likelihood of attempted suicide as more likely for both depression and schizophrenia, and their responses were much more consistent with that of other health care professionals [17]. These results demonstrate that pharmacists need further training on suicide and the long-term risks of having a chronic mental illness.
Our study had a number of strengths and limitations. An important strength of the study was that the survey instrument was mailed to a random sample of all pharmacists registered in the state of NSW. The survey instrument included vignettes that have been used extensively to survey other health professional groups in Australia [17,21,24,30]. This allowed for comparisons with these previously published studies [24,25,30]. However, the survey instrument was originally developed for members of the public. Although the response rate for this study was low (19.5%), our data were comparable to the NSW population of pharmacists (mean age 48 versus 46 years, 59% versus 54% female and 61% versus 63% primarily working in community pharmacy; study population and NSW population of pharmacists respectively) [35]. The response rate for this study was also comparable to mental health literacy surveys of other health professional groups in Australia [36]. The numbers of respondents from areas of practice other than community pharmacy were low and hence it was not possible to determine whether the mental health literacy differed according to the specific areas of practice within the pharmacy profession.
Conclusion
This is the first study to assess the mental health literacy of pharmacists. The majority of pharmacists had a high degree of MHL as shown by the correct identification of, and support of evidence-based interventions for mental illnesses. In general, pharmacists’ views on the helpfulness of interventions are similar to those of GPs compared to other health care professionals. Pharmacists’ long-term views of mental illness are also similar to other health care professionals who rate discrimination as more likely, and long-term outcomes without professional help more negatively than the public, however their views on ECT and hospital admission are quite negative and their understanding of suicide risk in mental illness is mixed. Further education may be required for pharmacists on the benefits and place in treatment of hospital admissions and ECT in mental illness and the risk of suicide in schizophrenia and depression. Pharmacists should be aware that their attitudes and stigma towards mental illness may impact on the patient care they provide. Pharmacists require training in how to effectively communicate with consumers with a mental illness to be able to confidently provide pharmaceutical care to this group of patients.
Footnotes
Acknowledgements
We wish to acknowledge the advice and support provided by Professor Anthony Jorm and for providing the mental health literacy survey instrument. This study was supported by a research grant from the Pharmacy Research Trust of New South Wales.