
Abstract
Childhood obesity has been implicated in an increased risk of cardiovascular disease, diabetes, and all-cause mortality later in life [1,2]. Mental health problems are also increasingly cited as a potential consequence of childhood overweight and obesity [2]. Yet very little is known about long-term risk for mental health problems from childhood weight due to a lack of prospective epidemiological studies [3,4] and an almost exclusive focus on depression. The high prevalence of childhood overweight and obesity in both developed and developing countries [2], even if incidence has reached a plateau [5], adds urgency to determining whether excess weight in childhood may contribute to the future burden of adult mental disorder.
We located only three community-based cohort studies that tracked the adult mental health outcomes of overweight or obese children. In the 1970 British Birth Cohort, neither obesity limited to childhood when aged 10, nor persistent obesity, were associated with psychiatric distress as measured by the Rutter Malaise Inventory at age 30 [6]. In contrast, in the 1966 Northern Finland Birth Cohort, being consistently overweight or obese at age 14 and 31 was associated with depressive symptoms in the Hopkins Symptoms Checklist at age 31, but only among women [7]. Similarly, the Children in the Community Study conducted in upstate New York found that obesity in adolescents aged 12–18 years in 1983 predicted DSM-III/DSM-IV depression and anxiety disorders in women but not men over a 20-year follow up [8]. Two of these studies [6,7] specifically examined the role of adult weight in the association between childhood weight and adult psychiatric outcomes. This is important because childhood overweight tracks strongly to adult obesity [9], and adult obesity is associated with higher prevalence of DSM-IV depression and anxiety disorders [10,11].
Disentangling these associations over time is important to appropriately target psychiatric risk reduction strategies across the lifespan [4]. Childhood and adolescent overweight may be a psychiatric risk irrespective of adult weight [8], for example, from associated stigma from peers or reduced participation in school sports or other forms of social physical activity. Alternatively, it is possible that only those whose excess weight persists into adulthood are at higher risk [7]. In the three prior cohort studies a selected range of childhood covariates was examined, but none of the studies included childhood physical activity which might plausibly influence both weight and mental health. To our knowledge, no study has comprehensively examined the risk for all the common mental disorders (mood, anxiety, substance) from childhood overweight or obesity, and no study has examined the role of childhood weight independent of adult weight in risk of diagnosed mental disorder. Prior cohort studies also used self-report height and weight on at least one [6,7], or all [8], assessment occasions.
We estimated the risk of DSM-IV mood, anxiety, and substance use disorders in young adulthood from overweight and obesity in childhood in a national prospective cohort study with height and weight measured in both childhood and adulthood. We hypothesized that childhood overweight and obesity would be associated with adult mental disorder, especially mood disorder, with the strongest associations among individuals whose excess weight persisted into adulthood.
Materials and methods
Study population and procedures
The Childhood Determinants of Adult Health Study [9] is a 20-year follow up of 8498 school children who participated in the Australian Schools Health and Fitness Survey in 1985 when they were aged 7–15 years (full details provided elsewhere [12]). Briefly, a nationally representative sample of 109 schools was selected with probability proportional to enrolment. From each age group at each school 10 boys and 10 girls were selected using simple random sampling. Twenty years later, 6840 individuals were able to be traced, 5170 enrolled in the study, and 2410 attended clinical assessments held in all states and territories of Australia in 2004–2006. A final analysis sample of 2243 (1135 women, 1108 men) was obtained after excluding pregnant women (n = 70) or those with missing outcome data (n = 97). In 1985 written consent from parents was obtained after a complete description of the study was provided, and children provided verbal assent. The follow-up study was approved by the Tasmania Health and Medical Human Research Ethics Committee, and written informed consent was obtained.
Measurements
For convenience, measurements in 1985 when the cohort was aged 7–15 years are labelled ‘childhood’ although these span both childhood and adolescent ages.
Overweight and obesity: height in metres and weight in kilograms were measured by study technicians to calculate body mass index (BMI) as kg/m2. In childhood, height was measured in bare feet with a KaWe height tape or rigid measuring tape, and weight was measured with subjects in light clothing with beam or medical spring scales. In adulthood, a Leicester height measure and Heine scales were used. Children were classified as overweight or obese based on a BMI ≥85th centile for age and sex-specific height and weight, using internationally comparable criteria for childhood overweight and obesity [13]. Adults were classified as overweight based on a BMI 25.0–29.9, and obese based on a BMI of ≥30 [14].
Mental disorder outcomes: the 12-month version of the computerized Composite International Diagnostic Interview (CIDI-Auto, Version 2.1) [15] was completed at the follow-up clinics. The following DSM-IV [16] diagnoses were assessed, analysed in their corresponding disorder class: mood disorder (major depression, dysthymia); anxiety disorder (panic/agoraphobia, social phobia, generalized anxiety disorder, specific phobia); substance use disorder (alcohol abuse or dependence, drug abuse or dependence). As part of the CIDI interview participants were asked to estimate the age of onset of symptoms for each of the disorders.
Potential covariates: child characteristics included age and socioeconomic status as indicated by retrospectively reported maternal and paternal educational attainment (post-high school qualification versus not). Participants aged 9–15 years also completed a self-report questionnaire and these covariates were examined in secondary analyses due to the smaller sample size: negative affect as measured by the Bradburn Scale, the sum of four items (feeling lonely, depressed/unhappy, bored, upset due to criticism) with total scores ranging from 0 (low negative affect) to 8 (high negative affect) [17]; alcohol intake (never/less than weekly versus at least one or two times per week); general health status with a single item (‘Is your health usually…’) dichotomized as very good/good versus average/poor/very poor; and number of minutes of physical activity in the past week including commuting by bicycle or walking, school physical education, school sport, and sport outside of school. Adult characteristics included questionnaire assessment of marital status, educational attainment, employment status, current daily smoker versus not, any live birth in women versus none, physical health component summary scale (PCS-12) of the Short-Form Survey (SF-12v2) (a 12-item version of the SF-36) [18], and total minutes in the past seven days engaged in leisure, occupational, commuting, and household/yard activity from the International Physical Activity Questionnaire (IPAQ long version) [19].
Sample attrition
In the follow-up analysis, some significant differences at baseline were observed between participants (N = 2243) and non-participants (N = 6255). In childhood, non-participants were more likely than participants to be overweight or obese (12.8% versus 9.1%, p < 0.0001), have smoked >10 cigarettes in their lifetime (14.6% versus 11.3%, p = 0.0005), report poorer general health (22% versus 18.2%, p = 0.0008), and be slightly younger (10.8 years versus 11.1 years, p = 0.0002). There were no differences in being female (48.9% versus 50.6%, p = 0.16), minutes of physical activity in the past week (434 versus 434, p = 0.98), drinking alcohol at least once per week (8.2% versus 7%, p = 0.11), or mean negative affect score (3.0 versus 2.9, p = 0.09). At follow up, the participants had a mean age of 31.5 (SD = 2.6), 34% were overweight and 15% were obese, 68% were married, 74% were educated beyond high school, 88% were employed, and 15% were current daily smokers. Statistical analyses were weighted by non-response to test sensitivity of results to attrition (see below).
Statistical analysis
Analyses were conducted with SAS version 9.1 and statistical significance was assessed at p < 0.05. Separate analyses were conducted for each class of mental disorder outcome (mood, anxiety, substance). We tested for an interaction of sex with weight as there is some evidence of a stronger association of weight and mental disorder among women [7,8]. The prevalence of childhood obesity (BMI ≥95th centile for age and sex-specific height and weight) in 1985 was very low in our analysis sample (girls n = 13, 1.1%; boys n = 10, 0.9%), thus our exposure variable was defined as childhood overweight or obesity.
The relative risk of adult mental disorder from childhood overweight and obesity was estimated using log binomial regression [20]. To examine whether current weight status should be taken into consideration, in cross-sectional analyses we estimated prevalence ratios for each mental disorder category by weight status in adulthood (non-overweight BMI <25 as reference, overweight BMI 25.0–29.9, obese BMI ≥30). Finally, to address our key question of whether child overweight was associated with adult mental disorder category after taking into consideration adult weight, we stratified childhood overweight/obesity by adult obesity [6,7], to give four weight trajectories: neither overweight nor obese in childhood, nor obese in adulthood (reference category); overweight or obese in childhood only (overweight in childhood, non-obese in adulthood); obese in adulthood only (non-overweight in childhood, obese in adulthood); overweight or obese in childhood and obese in adulthood. We stratified childhood weight by adult obesity rather than overweight/obesity, as obesity but not overweight was associated with mental disorders in adulthood (see Results). Potential covariates were selected for further analysis on the basis of a bivariate association at p <0.25 and were retained in the model if the exposure coefficient was changed by at least 10% [21]. Adjusted models exclude individuals who were missing at least one covariate, which for most respondents was due to non-completion of the self-report questionnaire. Sensitivity analyses explored the robustness of our findings, including examining potential bias from sample attrition by conducting population-weighted analyses. The weight for each respondent was the inverse of the probability of being a participant at follow-up based on baseline variables that predicted participation and were available for the whole sample of 7–15 year olds (age, sex and weight status).
Results
At baseline, 96 girls (8.5%) and 108 boys (9.7%) were overweight or obese (Table 1). Overweight in children was associated with lower socioeconomic status as indicated by mother's educational attainment, and with less physical activity among girls and poorer general health among boys.
Childhood characteristics in 1985 for study participants by childhood weight status and sex
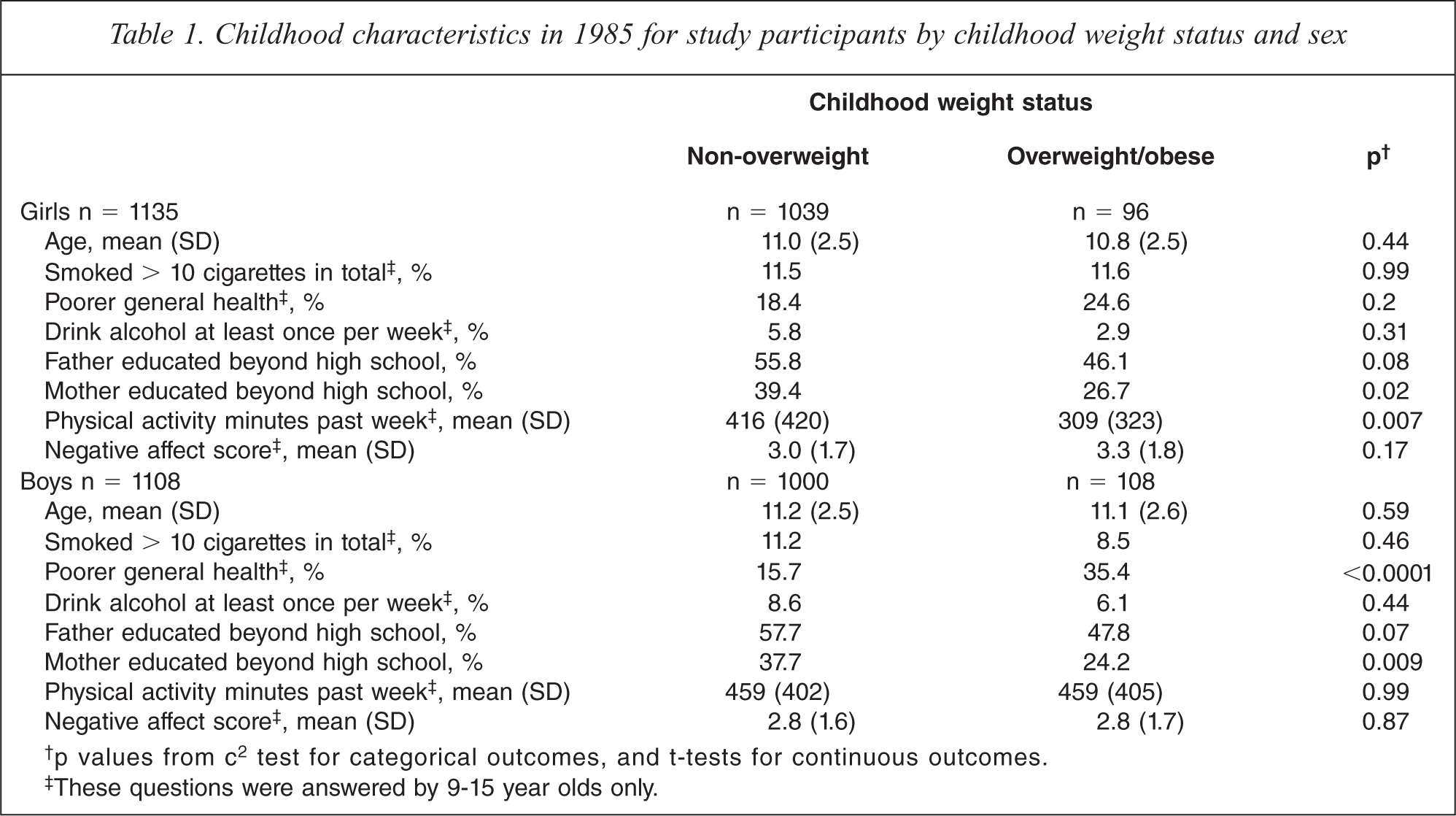
†p values from c2 test for categorical outcomes, and t-tests for continuous outcomes.
‡These questions were answered by 9-15 year olds only.
At follow up twenty years later, 207 (9.2%) participants met criteria for a mood disorder (women 12.1%, men 6.3%), 292 (13%) met criteria for an anxiety disorder (women 17.4%, men 8.5%), and 344 (15.3%) met criteria for a substance use disorder (women 10%, men 20.8%) in the past year. Prevalence of adult mental disorder by childhood weight status and the corresponding relative risk is shown in Table 2. There was no interaction between sex and child weight in the association with any mental disorder (mood p = 0.99, anxiety p = 0.49, substance p = 0.24). Overweight children were at significantly greater risk of a mood disorder in adulthood than non-overweight children, adjusted for child age and sex. No significant associations were observed with anxiety or substance use disorders. A range of potential covariates (p < 0.25) that were associated with child weight (Table 1) were examined among the subset of respondents aged 9–15 years who completed the self-report questionnaire. Father's education was associated with substance use disorders in girls and boys, while negative affect was associated with all mental disorder outcomes in girls but not boys. No other covariates, including smoking, physical activity, and alcohol use, were associated with any of the mental disorder outcomes, and adding these covariates to the models produced a negligible change in associations. Adjusting for father's education produced a negligible change in associations. Adjusting for negative affect among girls aged 9–15 years produced a small attenuation in risk of mental disorder from childhood overweight (N = 855, 68 (8%) overweight; mood unadjusted RR = 1.49, 95%CI 0.86–2.58, p = 0.15, adjusted RR = 1.41, 95%CI 0.82–2.41, p = 0.21; anxiety unadjusted RR = 1.2, 95%CI 0.73–1.96, p = 0.47, adjusted RR = 1.17, 95%CI 0.72–1.9, p = 0.53; substance unadjusted RR = 0.9, 95%CI 0.41–2.0, p = 0.8, adjusted RR = 0.87, 95%CI 0.4–1.92, p = 0.73).
Relative risk of adult mental disorder from childhood overweight and obesity
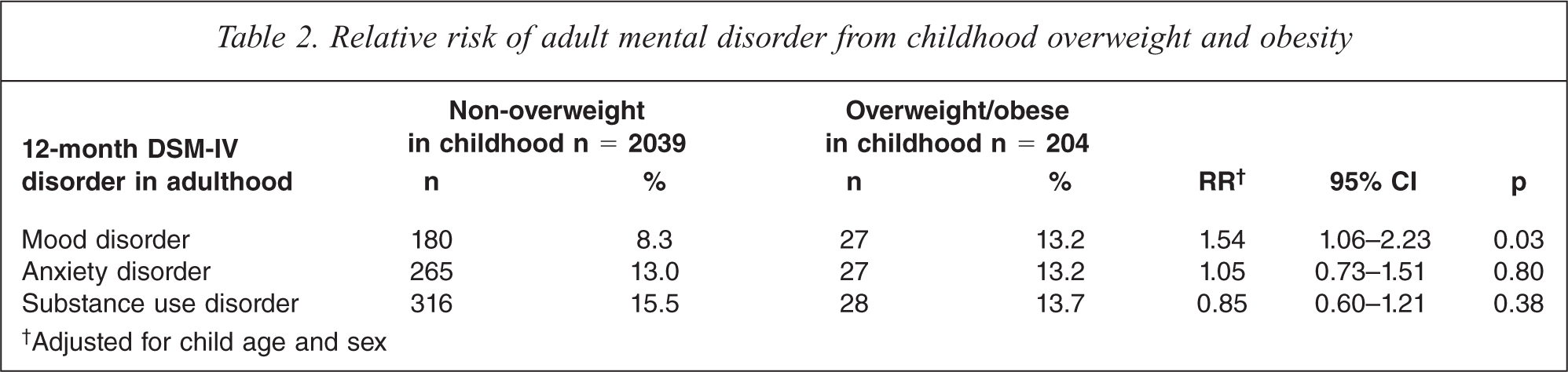
†Adjusted for child age and sex
At follow up 23% of women were overweight (BMI 25.0–29.9) and 14% were obese (BMI ≥ 30). Nearly twice as many men as women were overweight (45%) but a similar proportion were obese (16%). The role of adult weight in the association between childhood weight and adult mental disorder outcomes is of interest where there is a cross-sectional association between adult weight and mental disorder. There were weak interactions that did not reach significance between sex and adult weight in the association with mental disorder (mood p = 0.06, anxiety p = 0.1, substance p = 0.09). Neither overweight nor obesity in men was associated with any mental disorder outcome in comparison to non-overweight (all p > 0.2). Among women, overweight was not associated with prevalence of any mental disorder, but obesity was significantly associated with higher prevalence of mood (RR = 1.82, 95%CI 1.24–2.69, p = 0.003) and anxiety disorders (RR = 1.48, 95%CI 1.07–2.04, p = 0.02), and lower prevalence of substance use disorder (RR = 0.43, 95%CI 0.21–0.87, p = 0.02).
Given that an association of obesity in adulthood with mental disorder outcome was only observed among women, we examined the psychiatric risk of weight trajectories from childhood to adulthood in women only. The distribution of the sample across these weight trajectories and their characteristics in childhood and adulthood is shown in Table 3. The majority of women (n = 895, 82.1%) were non-overweight in childhood and non-obese in adulthood, 42 (3.9%) were overweight in childhood and non-obese in adulthood, 103 (9.4%) were non-overweight in childhood and obese in adulthood, and 50 (4.6%) were overweight in childhood and obese in adulthood. There were significant differences across the weight trajectories in childhood characteristics (age, general health, physical activity, and mother's educational attainment) and adult characteristics (employment, educational attainment, and physical health status).
Sample characteristics in childhood and adulthood by weight trajectory for female study participants
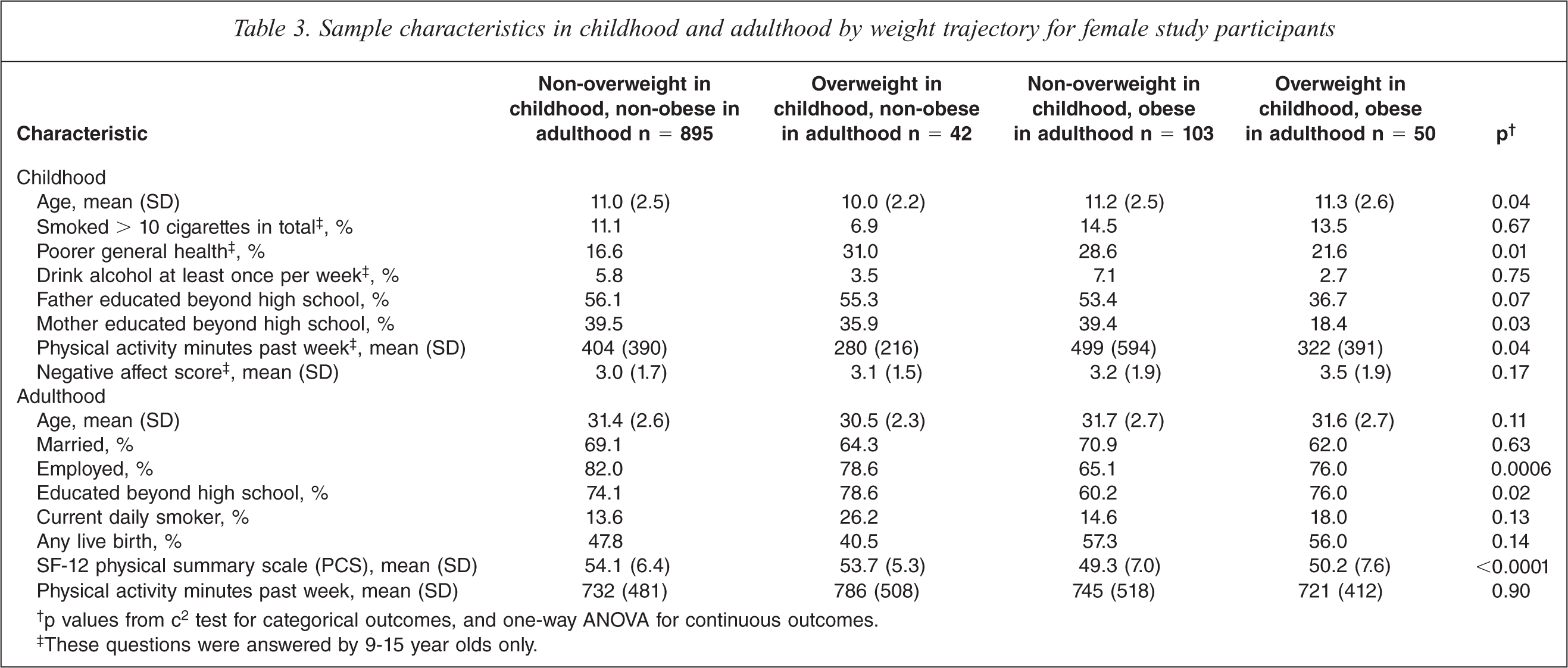
†p values from c2 test for categorical outcomes, and one-way ANOVA for continuous outcomes.
‡These questions were answered by 9-15 year olds only.
The prevalence of mental disorders and the adjusted association of weight trajectory with mental disorder are shown in Figure 1 for the 1090 women with complete data on covariates. In comparison to non-overweight girls who became non-obese adults, the only significantly increased risk for mental disorder was observed among overweight/obese girls who were obese in adulthood, with a greater than two-fold increased risk of mood disorder (adjusted RR = 2.03, 95%CI 1.22–3.66, p = 0.006). The prevalence of mood disorder for overweight girls varied markedly by their attained adult weight, with a prevalence of 9.5% for girls who became non-obese in adulthood versus 24% for girls who became obese in adulthood. The significantly lower risk of substance use disorder (p = 0.02) among obese women who were non-overweight in childhood should be interpreted with caution given the very low prevalence of substance use disorder among this group. Additional covariates from childhood (Table 3) were examined among the subset of respondents who completed the questionnaire when aged 9–15 years (n = 823). Adjustment for these produced negligible change in risks with the exception of adding childhood negative affect which attenuated the association slightly (without negative affect RR = 1.85, 95%CI 0.98–3.52, p = 0.06; with negative affect RR = 1.68 95%CI 0.89–3.15, p = 0.11).
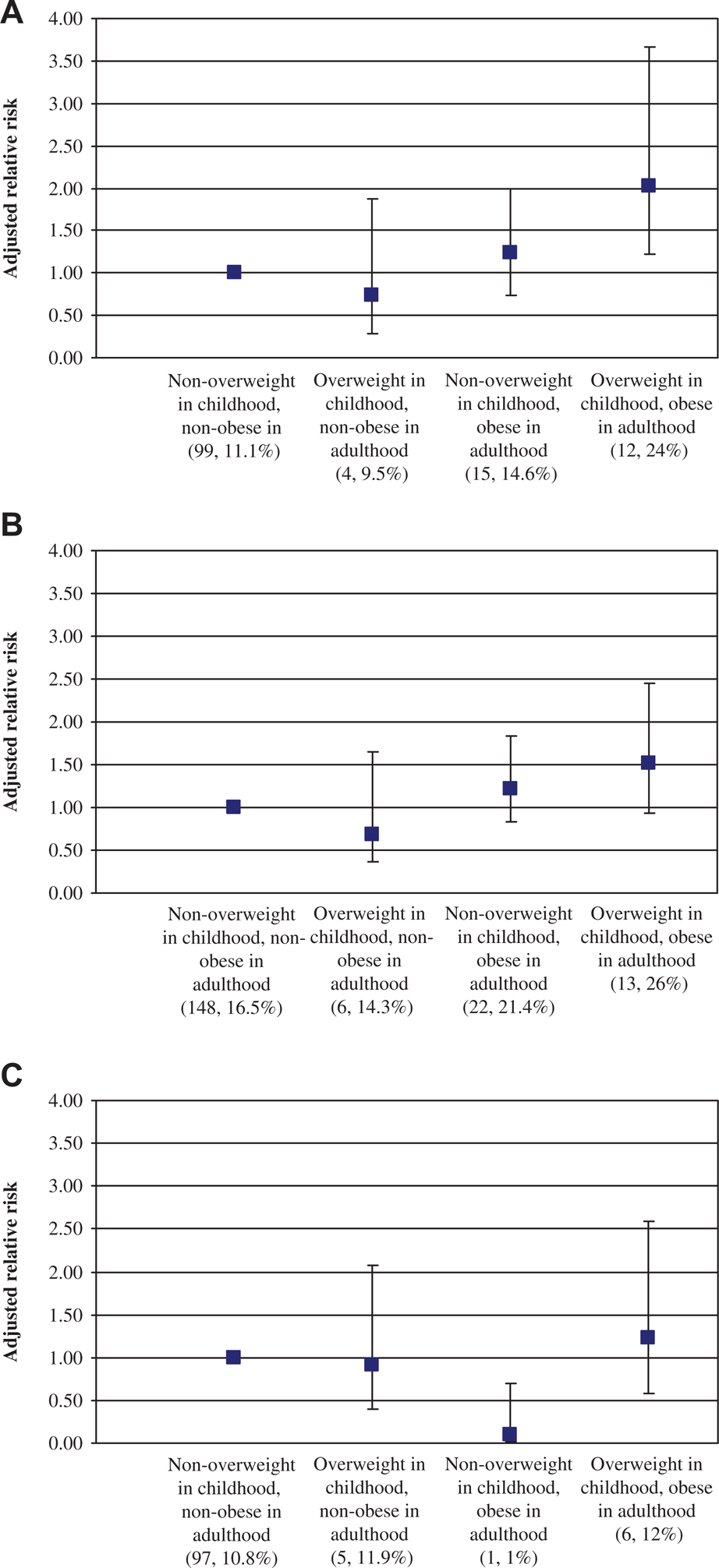
Adjusted relative risk (95% confidence intervals) for 12-month DSM-IV adult mental disorder by change in weight status among women (N = 1090). Prevalence of mental disorder is indicated beneath each weight category (n/N). (A) Mood disorder, (B) Anxiety disorder, (C) Substance use disorder, adjusted for childhood age, ever having a live birth, adult smoking, education, and employment.
The robustness of these findings was examined in sensitivity analyses. In population-weighted analyses, relative risks were only minimally changed (< 3%) suggesting that bias due to attrition was minimal. Sample size issues necessitated our definition of exposure as overweight or obese in childhood rather than restricted to the potentially more serious obesity. Using childhood obesity in our exposure variable produced a similar pattern of results although none reached significance (e.g. redoing the results for mood disorder in Figure 1 using childhood obesity rather than overweight/obesity gave the following results for persistent obesity: adjusted RR = 2.19, 95%CI 0.93–5.12, p = 0.07). Excluding participants (n = 11) who reported an age of onset for their mood disorder symptoms at or before the time of first interview in 1985 had a negligible effect on results.
Discussion
Previous developmental studies of childhood weight and mental health have largely focused on whether psychiatric symptoms in childhood are a risk factor for future weight gain and obesity [22–25]. The present study contributes to the growing evidence that a reciprocal relationship is possible [4]. We found that overweight or obesity in children aged 7–15 years was associated with an increased risk of diagnosed mood disorder in adulthood, which supports previous cohort studies among overweight [7] and obese [8] adolescents who were followed into adulthood. An increased risk of depression from obesity has also been reported in cohort studies with adults [26–28] and children [29].
As far as we are aware our study is the first to show that risk of diagnosed mood disorder in women from childhood overweight is influenced by adult weight, as a higher risk of depression was only observed among overweight girls who became obese in adulthood, and not among overweight girls who were non-obese in adulthood. While there was a relatively small sample size of overweight girls who became non-obese adults, our findings are supported by two clinical trials showing that weight reduction in children and adolescents can improve mental health [30] which may reduce risk for mental disorder in adulthood. We did not have sufficient power to report all analyses by childhood obesity; however, in sensitivity analyses we observed a similar effect when childhood obesity rather than overweight was used. We also examined a range of variables known to be associated with recovery from childhood obesity such as physical activity [24], adjusted for childhood negative affect, and our findings were robust to excluding cases of depression with childhood onset. Nonetheless, it is still possible among some participants that mental health has influenced weight changes, with those with better mental health more able to lose weight than those with poorer mental health.
Our results suggest that prevention of childhood overweight and obesity is equally important in both sexes for reducing risk of diagnosed mood disorder in adulthood, and that resolution of childhood overweight may be especially important among girls. Our findings are consistent with two of the three previous childhood–adulthood cohort studies that found an increased risk of psychiatric symptoms in adulthood from overweight or obesity among girls [7,8]. Failure to observe a stronger association in the third previous study may in part be due to use of a non-specific psychiatric distress measure (Rutter Malaise Inventory) [6]. Our cross-sectional findings of higher prevalence of mood and anxiety disorders and lower prevalence of substance use disorder in obese versus non-overweight women is consistent with evidence from large national surveys of DSM-IV disorders [10,11]. The reasons why we observed an association among women but not men when taking into account adult weight remains unclear, as the evidence for a sex difference in the obesity–psychopathology association is inconclusive [6,7,10,11]. One possible explanation is that psychosocial factors are more important among women, such that overweight and obesity in girls is associated with internalization of negative weight stereotypes and a negative body image which may increase risk for developing depression [3,8]. A hypothesized biological mechanism for this stress-related pathway is via repeated activation of the hypothalamic–pituitary–adrenal system which increases cortisol secretion; there is some evidence that cortisol reactivity explains the association between depression and BMI among girls but not boys [31].
Strengths of this study include a national sample of children and adolescents, a long-term follow up, comprehensive assessment of 10 DSM-IV mental disorders, examination of a wide range of covariates, and measured height and weight in both childhood and adulthood (prior cohort studies used self-report on at least one [6,7], or all [8], assessment occasions). These strengths are balanced against study limitations. In comparison to national data for this age group [32], study participants were less likely to be current daily smokers and more likely to be employed and educated beyond high school, but had a very similar prevalence for the key study variables of mental disorders [33] and overweight and obesity [32]. Non-participants were more likely to be overweight in childhood than participants. The analysis was weighted by variables that predicted non-response, including overweight, and conclusions did not alter, suggesting that bias due to attrition was minimal. We did not have a measure of perception of overweight or whether the participant was concerned about their weight, which has been associated with mental health problems independent of actual weight in children [34] and adolescents [35]. While we tested for a wide range of covariates in childhood and adulthood including physical activity, smoking, health status, and socioeconomic indicators, we cannot rule out alternative explanations for our findings from unmeasured confounding. It is also possible that a shared environmental [36] or pathophysiologic [37] mechanism is causing both mood disorder and obesity.
The prevalence of childhood overweight and obesity has more than doubled in many countries since our study participants were first assessed in 1985 [2]. Our findings suggest that mood disorders can be added to the list of potential longer-term risks from childhood overweight and obesity. These findings add impetus to improving the currently modest efficacy of interventions to reduce the prevalence of childhood overweight and obesity [30], and for mental health promotion and prevention among overweight and obese children and adolescents [4]. Ideally, long-term follow-up of current cohort studies and weight loss management programmes with children and adolescents will include assessment of mental disorders. This will help determine whether psychiatric risk persists in an era when childhood overweight and obesity is increasingly common in many communities.
Footnotes
Acknowledgements
The authors gratefully acknowledge the study sponsors Sanitarium, ASICS and Target, and the contributions of all study staff and participants.