
Abstract
Keywords
The processes that make schizophrenia and other psychoses a long-term disorder may cause more damage in the first few years of the illness [1]. Recognition and intervention at an early stage of psychosis could contribute to quicker psychotic and negative symptom remission, delay in psychotic relapse and prevention of psychosocial deterioration [2–5]. The early phase of psychosis can be seen as a critical period with implications for the prevention of disease and psychosocial deterioration [6]. This has led to a proliferation of early intervention for psychosis services nationally and internationally in recent years.
New Zealand has enthusiastically adopted the concept of early intervention and now has more than 18 statutory mental health services that work, wholly or partly, as early intervention services for young people. Twelve of these services were established after 1997 [7]. This means that most young people with first-episode psychosis in New Zealand receive some form of early intervention. Early intervention services take all young people with first-episode psychosis, including drug-induced psychosis, affective psychosis and psychosis not otherwise specified (NOS), as well as schizophrenia and schizophreniform disorder. Their criteria therefore differ from many European and North American services, which only accept patients with schizophrenia spectrum disorders. The duration of untreated psychosis and pathways to care may vary depending on diagnosis [8–10], and therefore international reports may not be applicable to New Zealand. There are currently no published reports on early intervention services in New Zealand.
Earlier intervention may reduce suffering associated with psychosis. The time between onset of psychotic symptoms and the first effective treatment in patients with schizophrenia (i.e. the duration of untreated psychosis) usually ranges from 1 to 2 years, but can be much longer [8]. The pathways to care and duration of untreated psychosis may vary depending on a number of factors [11, 12]. In New Zealand, for example, it has been suggested that Maori have less desirable pathways to care and access services at a later stage of illness [13, 14].
Examination of a New Zealand cohort is important because different health-care systems lead to different pathways to care in first-episode psychosis [15]. The purposes of this paper are: (i) to describe the presenting characteristics and pathways to care of 200 patients with first-episode psychosis referred to an Early Intervention for Psychosis Service (Totara House) in Christchurch, New Zealand; (ii) to examine differences in pathways to care and duration of untreated psychosis between Maori and non-Maori; (iii) to examine differences in pathways to care and duration of untreated psychosis between patients with a schizophrenia spectrum disorder and other diagnoses; and (iv) to compare the characteristics of the present cohort with other international samples from Australia, North America and Europe.
Method
Totara House provides specialist, multidisciplinary support to individuals who experience their first-episode of psychosis. The service is based on best practice guidelines developed nationally [16, 17] and internationally [18]. A detailed description of the service can be found at the web site: http://www.cdhb.govt.nz/totara
Inclusion criteria
The patient is aged between 18 and 30, or is between 16 and 17 and not currently under the care of Youth Mental Health Services. The patient has suspected or confirmed psychotic features, or the patient has a suspected prodromal presentation, regardless of diagnosis. The patient is in their first-presentation of psychosis and has previously received less than 12 weeks of treatment with antipsychotics.
There are no exclusion criteria although patients with an IQ of less than 70, or currently within the criminal justice system, would not be referred to the service.
Assessment
All patients accepted into the service with first-episode psychosis are part of a longitudinal cohort. The study was approved by the Canterbury Ethics Committee. The assessment has two sections.
The psychiatrist interview assesses:
DSM-IV clinical diagnosis [19]; Symptoms of psychosis using the Positive and Negative Syndrome Scale (PANSS) [20]; Duration of untreated psychosis (time between episode onset: defined as 4+ on one of the first three positive symptom items of PANSS and onset of ‘adequate’ treatment: defined as start of antipsychotic medication).
The case manager interview assesses:
‘Pathways to care’ in the 6 months prior to Totara House; The Quality of Life Scale [21].
Statistics
In order to examine differences between median duration of untreated psychosis for those with different diagnoses, the Kruskal– Wallis test was used to test for statistically significant differences between subgroups. The chi-squared test of independence was used to test for statistically significant differences between pathways to care and ethnicity.
Results
Three of the psychiatrist interviews were incomplete, and 13 were missing (92% completion rate). Five of the case manager assessments were incomplete and 13 were missing (91% completion rate). Missing assessments were due to staff difficulties and administrative issues. The results of the present cohort are compared with first-episode psychosis cohorts from: the Early Psychosis Prevention and Intervention Centre (EPPIC) in Australia [22, 23]; the Calgary Early Psychosis Program (EPP) in Canada [24–27]; and the non-early detection areas of the Early Treatment and Intervention in Psychosis Study (TIPS) in Norway and Denmark [28].
Sociodemographic characteristics
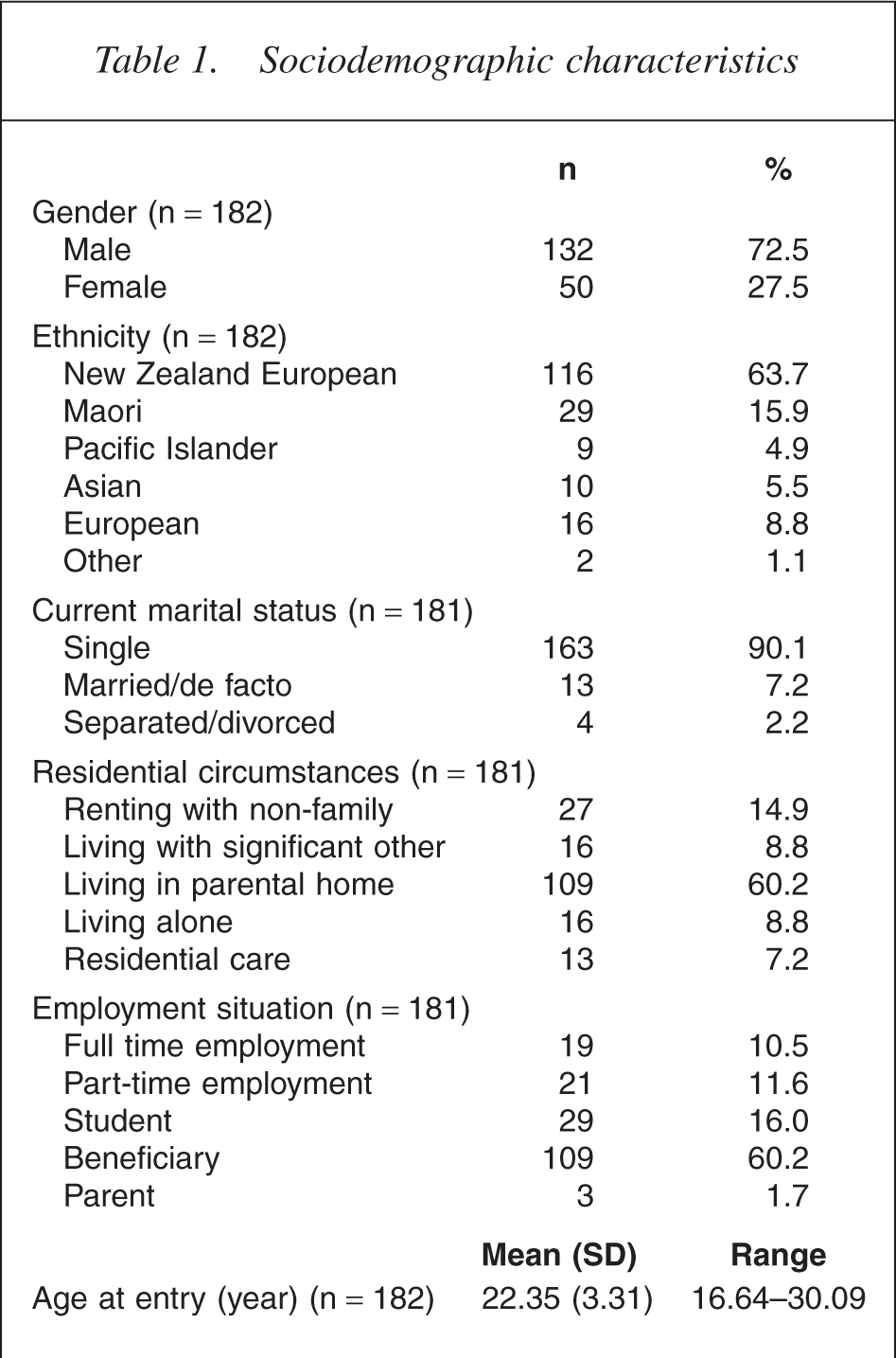
Table 1 shows the gender, ethnicity, marital status, residential circumstances and socioeconomic background of the patients as well as the mean age and age range of patients on entry to the service. Patients are predominantly male, European, single, living with parents and on some form of government benefit.
Sociodemographic characteristics
DSM-IV diagnostic category
Table 2 shows the frequencies and percentages of the principal diagnoses of patients. The most common diagnoses are bipolar disorder (20.1%), schizophreniform disorder (19.6%), schizophrenia (17.9%), depressive disorder (15.8%) and psychotic disorder NOS (13%).
DSM-IV diagnostic category
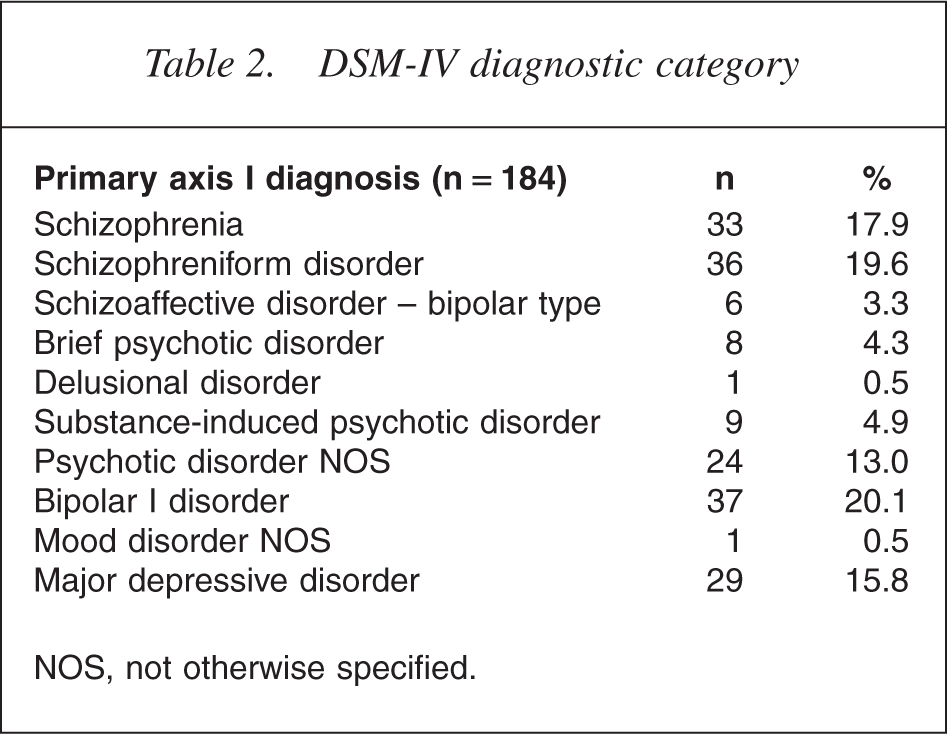
NOS, not otherwise specified.
Symptomatic descriptors
Table 3 provides a summary of the patients' quality of life scores, positive and negative symptom scores and substance misuse disorders (abuse and dependence). The present cohort had poor baseline quality of life scores (mean = 61.65) and high rates of positive (mean = 15.41) and negative (mean = 14.22) symptoms were present.
Symptomatic descriptors
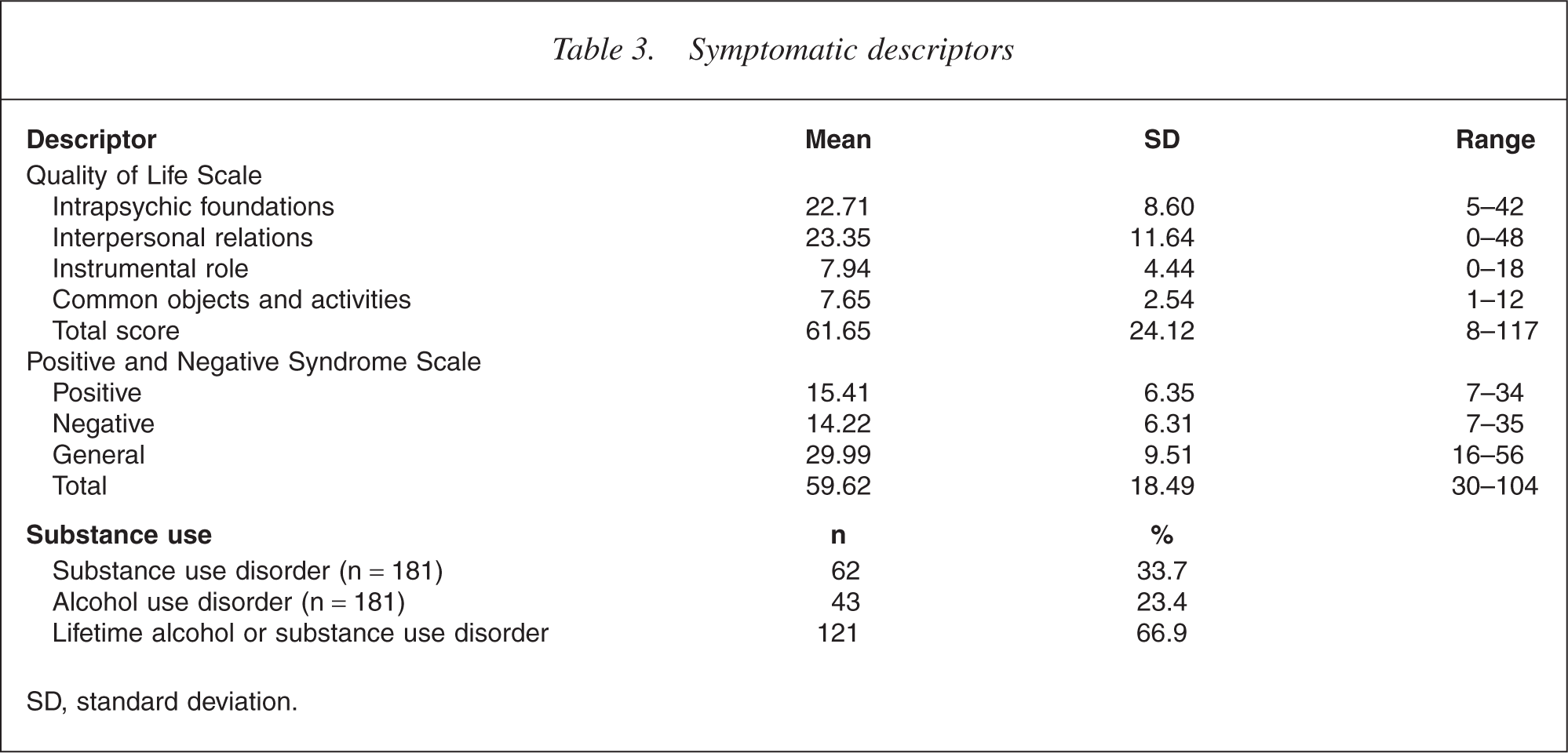
SD, standard deviation.
One-third (33.7%) of the patients were diagnosed with current substance abuse or dependence (excluding nicotine) and a quarter (23.4%) with current alcohol abuse or dependence. Overall, 39.5% present with a current substance use disorder, while two-thirds of the patients (66.9%) present with lifetime substance and/or alcohol abuse or dependence.
Pathways to care
Table 4 shows the patient contact with social agencies in the 6 months prior to admission to the service. The table shows the different types of help-seeking behaviours initiated, sources of referral, police involvement, rates of psychiatric hospitalization and compulsory admission associated with referral. Finally, the table shows the median and mean duration of untreated psychosis.
Pathways to care
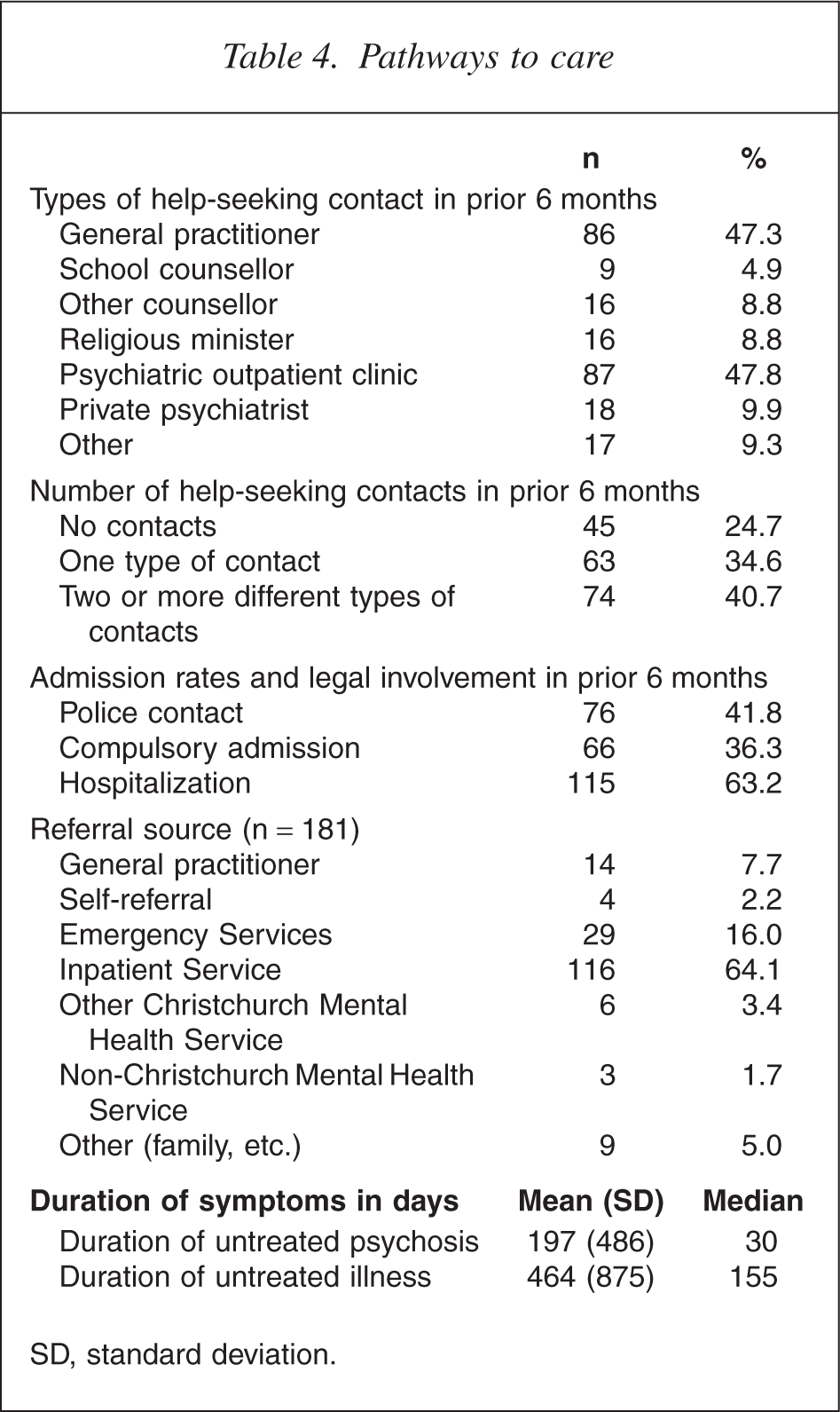
SD, standard deviation.
Patients in the present study reported making an average 3.87 (SD = 6.81) attempts at help-seeking behaviour in the 6 months prior to referral (range = 0–42). The majority (70%) of the sample had contact with a general practitioner (GP) or psychiatric outpatient clinic in the 6 months prior to referral, but these services were low sources of referral (7.7% and 16%, respectively). Most referrals (64%) came from inpatient services. The large discrepancy between the mean and median duration of untreated psychosis is due to a positively skewed distribution. A small group of patients presented with extremely long untreated periods; for example, 14 patients had a duration of untreated psychosis exceeding 4 years.
The associations between diagnostic subgroups and pathways to care
The median duration of untreated psychosis for those with a schizophrenia spectrum disorder was significantly longer at 120 days, compared with 29 days for those with affective psychosis and also 29 days for other types of psychosis (drug-induced psychosis, psychosis NOS, etc.) (see Table 5, χ2[2] = 18.66; p < 0.001). No differences were evident between diagnosis and the number of different types of help seeking (χ2= 2.08; df = 4; p = 0.72), rates of contact with police (χ2= 1.82; df = 2; p = 0.40), outpatient services (χ2= 2.77; df = 2; p = 0.25), or GPs (χ2= 0.75; df = 2; p = 0.68), rates of hospital admission during first-episode of psychosis (χ2= 1.42; df = 2; p = 0.49), or rates of compulsory admission during first-episode of psychosis (χ2= 0.49; df = 2; p = 0.78).
Relationship between the duration of untreated psychosis and diagnostic subgroup

The associations between ethnicity and pathways to care
There were no significant differences in duration of untreated psychosis for Maori and non-Maori (χ2= 1.81; df = 1; p = 0.17). No differences were evident between Maori and non-Maori in the number of different types of help seeking (χ2= 0.41; df = 1; p = 0.81), rates of contact with police (χ2= 0.09; df = 1; p = 0.76), outpatient services (χ2= 1.35; df = 1; p = 0.17), or GP's (χ2= 0.01; df = 1; p = 0.53), rates of hospital admission during first-episode of psychosis (χ2= 0.08; df = 1; p = 0.48), or rates of compulsory admission during the firstepisode of psychosis (χ2= 0.60; df = 1; p = 0.43).
Discussion
This is the first published description of the demographic and clinical characteristics of a New Zealand first-episode psychosis cohort. The majority of patients were young, single, male and referred from the regional Acute Inpatient Service. A high proportion of patients were diagnosed with a non-schizophrenia spectrum disorder at admission. The distinctive characteristics are a narrower age range for acceptance (16–30 years), broader diagnostic acceptance criteria including affective and non-specific psychosis, and acceptance of nonhospitalized patients. This results in a higher rate of affective disorders, a younger mean age at referral and a large proportion of men compared with some international samples. While those with a schizophrenia spectrum disorder had a significantly longer median duration of untreated psychosis, no other differences in pathways to care were evident in the present cohort for diagnosis or ethnicity.
Demographic and clinical features
Table 6 shows a comparison between the Christchurch cohort and international samples on selected demographic and clinical variables.
Comparison between Christchurch cohort and international samples
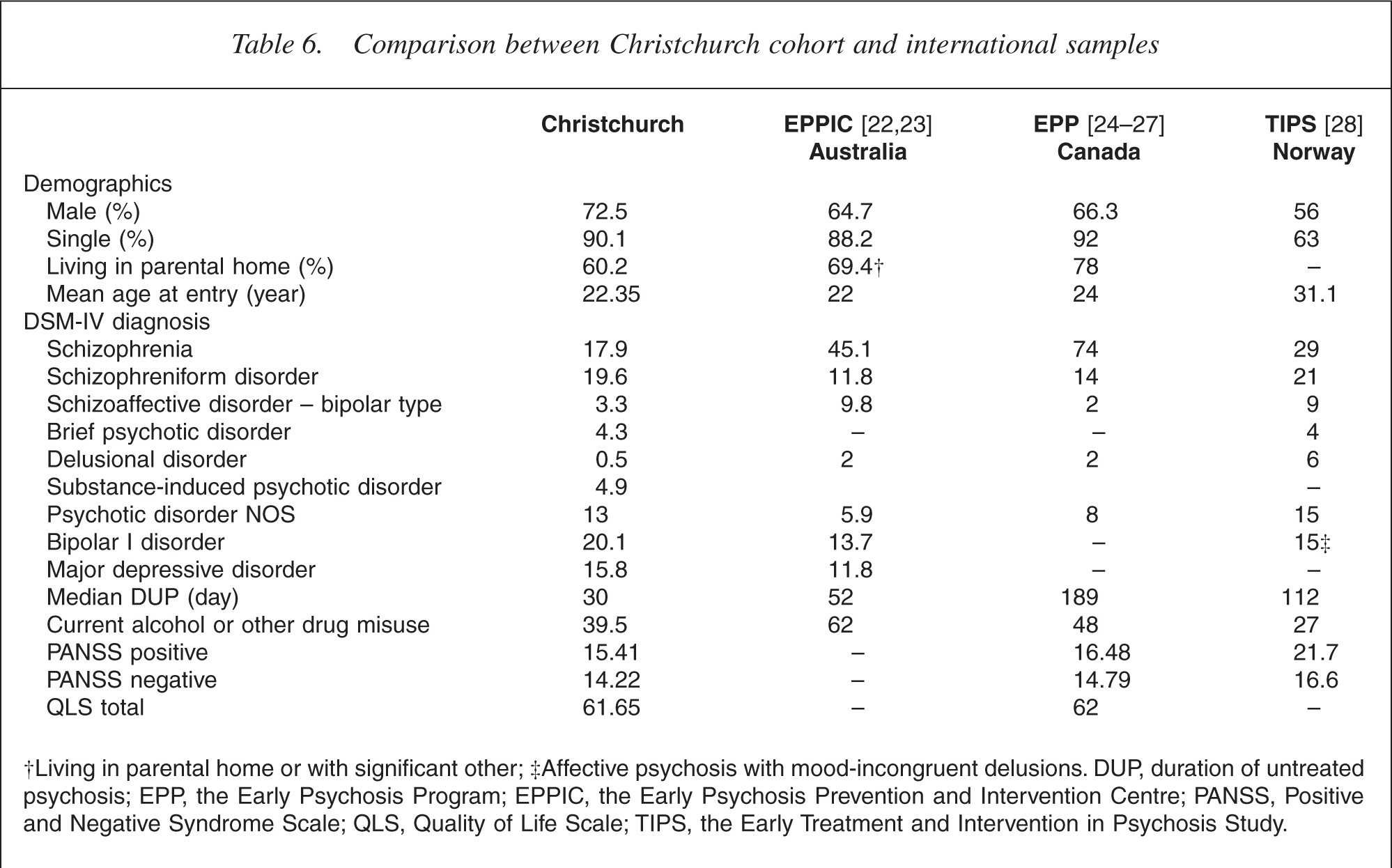
†Living in parental home or with significant other; ‡Affective psychosis with mood-incongruent delusions. DUP, duration of untreated psychosis; EPP, the Early Psychosis Program; EPPIC, the Early Psychosis Prevention and Intervention Centre; PANSS, Positive and Negative Syndrome Scale; QLS, Quality of Life Scale; TIPS, the Early Treatment and Intervention in Psychosis Study.
The sociodemographic characteristics are similar to those reported by EPP [26] and EPPIC [23]. However, the average age of the EPP [26] and TIPS [28] cohorts are older, reflecting the older age accepted by these services. As women tend to develop psychosis at an older age [29], the younger mean age of the present sample, owing to the lower age limit for acceptance, may be responsible for proportionally fewer women in the EPPIC and Christchurch cohorts. A recent meta-analysis of 26 studies involving 4490 patients [30] found the mean age at presentation was 27.8 years and that women comprised 39% of the sample.
While the diagnostic description of the present sample is similar to that of EPPIC [23], it has a greater proportion of patients with affective psychosis than reported by EPP [24] and TIPS [28]. Many services in North America [26, 31] and Europe [29, 32, 33] do not report on patients with affective psychosis.
Previous first-episode cohorts have shown similar high levels of positive and negative symptoms [24, 28, 34] and low quality of life [24, 35] at referral to early intervention for psychosis services. The high rates of alcohol and other drug misuse (predominantly cannabis) in the present sample are consistent with other first-episode cohorts [22, 27,36–38]. Overall, 39.5% present with a current substance use disorder, while two-thirds of the patients (66.9%) present with lifetime substance and/or alcohol abuse or dependence. This compares with 62% and 74%, respectively, reported by EPPIC [22]. Combined with the fact that substance misuse can have a detrimental effect on the course of psychosis, these results confirm the need for highlighting substance use comorbidity in early intervention services [39, 40]. In summary, the patients' demographic and clinical characteristics are similar to those cohorts with similar acceptance criteria [23, 34, 41, 42].
Duration of untreated psychosis
The median duration of untreated psychosis of 30 days is shorter than that reported by many early intervention services, where periods exceeding 6 months are common [8, 30]. The relatively short duration of untreated psychosis is probably due to the high proportion of patients with non-schizophrenic psychosis. EPPIC [23], which also accept those with affective psychosis, also reported a significantly longer duration of untreated psychosis in patients diagnosed with schizophrenia. In our cohort, patients diagnosed with a schizophrenia spectrum disorder had a significantly longer median duration of untreated psychosis (120 days) compared with patients with other diagnoses (29 days).
The high proportion of patients with a non-schizo-phrenia spectrum disorder in the present cohort partially accounts for the shortened duration of untreated psychosis. In addition, the broad definition of duration of untreated psychosis (i.e. initiation of adequate treatment [30]) used in the present study may shorten the median duration compared with studies that use more stringent definitions with regard to adequacy of initial antipsychotic treatment. Another contributing factor may be associated with the small population of the Christchurch catchment area (344 100) and relatively low rates of homelessness. This may lead to overt psychosis being more noticeable in the community and patients coming to the attention of services more rapidly.
Pathways to care
Patients had an average of 3.87 attempts at helpseeking behaviour in the 6 months prior to referral, with 47.3% contacting a GP and 47.8% an outpatient clinic. Only 7.7% of patients are referred directly from a GP, although most of those referred from other Christchurch Mental Health Services may have been referred to these services by a GP initially. This is similar to findings of McGorry et al. [23] who report that while 50% of subjects had GP contact prior to initial effective treatment, only 5% of referrals for specialist psychiatric care came from GPs. As with similar studies from Australia [41], the UK [42] and Canada [43], the large number of patient contacts prior to referral indicates that GPs may have a crucial gate-keeping role. Of particular concern is that the early signs of psychosis in Maori (and Pacific peoples) may be missed by health practitioners, and that Maori (and health professionals) may reframe psychosis in a cultural context (Durie M., personal communication, 2002).
The short median duration of untreated psychosis in the sample is positive, but the fact that two-thirds of referrals come from Acute Inpatient Services suggests that symptoms appear rapidly and are of sufficient severity to warrant admission. With the deleterious effects that may be associated with acute admissions [44, 45], this represents significant potential suffering for the individual and their families. The rates of compulsory admission (36.3%) in the present study are similar to those previously reported in first-episode psychosis (37.9%) [12].
Effects of ethnicity on pathways to care
Although there was a higher proportion of Maori patients in the cohort (15.9%) than in the general Christchurch population of 15–29-years-olds (8.8%) (Statistics New Zealand, 2001 unpublished Census data), no associations were found between ethnicity and pathways to care. It has been suggested that Maori access services at a far later stage of illness and are more likely to be admitted to psychiatric institutions as a result of compulsory admission [13]. However, no differences in duration of untreated psychosis, hospitalization rates, compulsory treatment or police contact were evident between Maori and non-Maori in the present sample. Less desirable routes of admission for African-Caribbean patients have been reported in London but do not apply to their first admission, instead developing over repeated contact with services [11].
Limitations
We believe that the sample is representative as it includes all those with first-episode psychosis referred into the only early intervention for psychosis service in the Christchurch catchment area. Overall, 92% of eligible patients had a psychiatrist interview completed and 91% had a case manager interview completed. As the reasons for non-completion of evaluations were largely administrative, rather than reflecting patient characteristics, this limits the probability of selection bias. The major limitation is that findings on pathways to care and duration of untreated psychosis are predominantly based on patients' self-reports, which may be prone to recall errors and selective reporting. In addition, the pathways to care data only examine the number of contacts rather than the chronology of contacts and only look at the 6 months preceding admission to the service rather than all contacts.
Conclusion
The current cohort is similar to early intervention services with comparable health-care systems and acceptance criteria [23, 42]. Many patients with first-episode psychosis are making several attempts to obtain help before admission. Education of both health professionals and the general public to attempt to reduce duration of untreated psychosis [28, 46], particularly for those eventually diagnosed with a schizophrenia spectrum disorder, is needed.
Our results suggest that pathways to care are specific to health-care systems [15]. The high proportion of patients with diagnoses other than schizophrenia in the present study suggest that overt symptoms of psychosis requiring acute, rapid hospitalization are more common in comparison with most international samples. Greater liaison with inpatient services and primary referrers may be desirable in order to reduce the negative aspects of hospitalization for those with affective psychosis, where early detection is problematic because of rapid onset.
Footnotes
Acknowledgements
This paper would not have been possible without continued financial support for the research position at Totara House from the Mental Health Division of the Canterbury District Health Board. We also thank the Totara House team for their commitment to completing the measures.