
Abstract
Aggressive behaviour is a frequent reason for admission of young people to youth mental health services [1,2]. The diverse range of psychiatric diagnoses among youths admitted to inpatient facilities results in many individuals diagnosed with disorders that include aggressive behaviour among their symptoms. Glasser (p.887) [3] defined aggression as ‘a bodily response with the intended infliction of bodily harm.’ It is not surprising that aggressive incidents are common during inpatient admission [4]. For the purpose of this research, aggression was confined to those acts against other people and property destruction.
Identification of high risk patients is crucial in the management of aggression in the inpatient population. Mental health professionals are frequently required to conduct risk assessments as part of hospital policy. Risk assessment is the evaluation of the likelihood that an individual will become aggressive and contributes to the subsequent development of interventions to manage or reduce the likelihood of aggression [5]. Risk assessment methodologies and practices have been developed to assist in the prediction and prevention of aggression.
In spite of advances in risk assessment practices, empirically validated risk assessment tools are seldom utilized in clinical practice. Furthermore, the development of aggression risk assessment tools has for the most part used adult samples. Consequently, research on youth-specific measures is limited due to their recent development. While there is growing empirical evidence on risk factors for aggression in youths, the limited number of empirically validated risk assessment tools for this age group often results in the use of adult tools in young populations. Not surprisingly, it has been suggested that adult tools should not be utilized in youth samples [6]. Lack of temporal stability and the developing nature of young people from an emotional, social and physical perspective makes it difficult to assess and characterize youths at a single point in time when making clinical judgements [7]. This suggests that the application of aggression risk assessment is more complex in young people, and adult measures cannot be directly transferable to young people. Further, a recent meta-analysis of nine commonly used risk assessment measures across 68 studies found that risk assessment measures developed for specific populations such as adolescent juveniles produced higher rates of predictive validity than measures originally developed for more general populations and types of offending [8]. The authors concluded that clinicians may select risk assessment measures that have been validated for their population and setting irrespective of the risk assessment method. This research supports the need for risk assessment measures that are specific to the child psychiatric inpatient population.
It is important that the risk factors and information in aggression risk assessments are tailored and relevant to young people to provide an accurate indication of risk for the individual. As with adults, a prior history of aggression is the single best predictor for future aggression in youths [7]. This finding has also been documented in child inpatient samples [1]. History of abuse is documented as a risk factor for aggression in youths [7,9,10]. Although diagnosis as a risk factor for aggression has been deemed inconclusive in some studies [1] a diagnosis of disruptive behaviour disorder has been found to be predictive of aggression in child inpatients [9,11]. Although there has been some disagreement, risk factors including past history of aggression, abuse and a diagnosis of disruptive behaviour disorder have all been shown to be predictive of aggression in child inpatients.
The importance of age-relevant risk assessment measures based on risk factors for aggression in young psychiatric inpatients was evident in a study conducted by Crocker, Stargatt and Denton [11]. This study formed the basis for the rationale of the current research. In addition to assessing factors associated with aggression in child inpatients, Crocker, Stargatt and Denton [11] addressed the degree to which unstructured clinical risk assessment, based on the clinician's subjective judgement of risk, predicted aggression as measured by the frequency of holds, time-outs and seclusions. Whilst the risk assessment was found to significantly predict the frequency of aggression, it did not predict the severity of aggression. A diagnosis of disruptive behaviour disorder was a better predictor of severe aggression than the risk assessment rating [11]. In addition, it was found that although risk assessment ratings and a diagnosis of disruptive behaviour disorder were the best determinants that a child would be aggressive, the combined predictive ability of the diagnosis and risk assessment only predicted approximately a quarter of the variance between children who were frequently aggressive and those that were less so. Whilst these two factors were important in predicting aggression, regression analyses suggested that additional factors contributed to a child being aggressive that were not accounted for in the risk assessment measure.
A number of weaknesses in the study were identified. Holds, seclusion and time-outs were used as a proxy for aggression. In actual fact they are often employed as an intervention response to aggression rather than measuring aggression directly. No distinction between the types of aggression was possible and it may have been that incidents of aggression were over reported, as intervention responses are often utilized in response to behaviour such as absconding or self-harm. The current research assessed aggression in terms of the actual incidents of aggression. Further, the sample was limited to only those children that engaged in aggression. The current research sought to examine the larger inpatient population and collected data on all children regardless of engagement in aggression, to determine the ability of the risk assessment to predict aggression in a sample of both high and low risk individuals.
The aim of this study was to retrospectively examine the predictive validity of unstructured clinical risk assessment of aggression, based on the clinician's expertise, prior experience and intuition by examining the association between risk assessment rankings assigned by psychiatric staff on admission and subsequent incidents of aggression recorded in critical incident reports by nursing staff occurring within the first four weeks of inpatient stay. Additional risk factors for aggression in child inpatients were also assessed, including history of physical aggression and trauma and diagnosis to determine whether unstructured clinical risk ratings were more predictive of engagement in aggression than certain risk factors alone.
It was hypothesized that higher risk ratings for aggression would be associated with higher frequency and severity of aggression in the first four weeks of inpatient stay. In addition, it was hypothesized that history of physical aggression, trauma, and a diagnosis of a disruptive behaviour disorder would be associated with more frequent and severe aggression in the first four weeks of admission.
Method
Approval was obtained from the Austin Health Human Research Ethics Committee (H2009/03562) and the La Trobe University Science, Technology and Engineering Faculty Human Ethics Committee (FHEC09/R47).
The study was conducted at the State-Wide Child Inpatient Unit (SWCIPU). The SWCIPU is a 12-bed inpatient unit at the Austin Health Child and Adolescent Mental Health Service in Melbourne, Australia, operating seven days per week and providing short to medium term assessment and treatment for children with serious psychiatric, behavioural and emotional disturbances. The SWCIPU serves children throughout Victoria under the age of 13. Children are typically admitted to the inpatient unit when all other avenues of outpatient treatment have been exhausted or a more thorough assessment and treatment of family dynamics are needed that cannot be achieved as an outpatient. In spite of implementation of management strategies, aggression on the unit remains an issue.
A file audit of admissions for the period of September 2006 to July 2009 was conducted at the SWCIPU during late 2009 examining unstructured clinical risk assessment practices. Inclusion criteria required children to be aged 8 to 13. Unit record identification codes for each patient admitted during this period were entered into the MedTRACK database to obtain demographic and clinical information including age, length of stay and admission type. Medical files for each child were accessed to obtain risk assessment ratings, diagnoses, history of aggression and trauma. Diagnostic assessments were undertaken prospectively during patient admission by child psychiatrists. Discharge diagnoses were recorded for the purpose of this study. Risk assessment ratings for aggression were recorded from the child's medical file. This rating was based on the subjective unstructured clinical judgement of the child psychiatrist or psychiatric registrar completed at the time of patient admission. Generally the psychiatrist was informed by referral information and pre-admission assessment. Risk rankings were ranked from one to four: low, medium, high and very high.
Episodes of aggression that take place on the unit are documented by nursing staff at the time of incident as standard hospital procedure. Hard copy incident report forms were documented for aggressive incidents prior to January 2007. Following that, critical incident reports on the RiskMan database and the medical record were accessed to obtain information on aggression occurring in the unit for each child. Critical incident reports are primarily recorded in response to aggression that results in an intervention response from the unit staff. As such, only the more serious incidents of patient aggression (towards staff, other patients or property) were included in this study. Frequency of aggression was rated by the number of times a patient engaged in aggression. In line with the previous study [11], the severity of aggression for any one incident was determined as not being severe if SWCIPU staff were able to manage the child, and severe if SWCIPU staff required the assistance of staff external to the unit to contain the child.
Data was entered into Windows SPSS version 16.0 for analysis and checked for errors. Descriptive statistics were conducted on demographic and clinical information pertaining to aggression. Risk factors associated with aggression were identified by correlation and chi-square analyses. Binary logistic regression was performed to investigate whether the identified risks and the risk assessment rankings were predictive of engagement in aggressive behaviour in the first four weeks of admission. An error rate of alpha = 0.05 (two-tailed) was set to determine statistical significance.
Results
A total of 154 children were admitted to the SWCIPU during the study period. Of these, 20 children under the age of eight were excluded from further analysis. Seven children were excluded due to incomplete risk assessment ratings. Ages of the remaining 127 children ranged from 8 to 13 years (mean = 10.35 years, SD = 1.32). The sample was predominantly boys (72.9%) and comprised largely of planned admissions (75.6%). The mean length of stay was 27 days (range = 1 to 53 days).
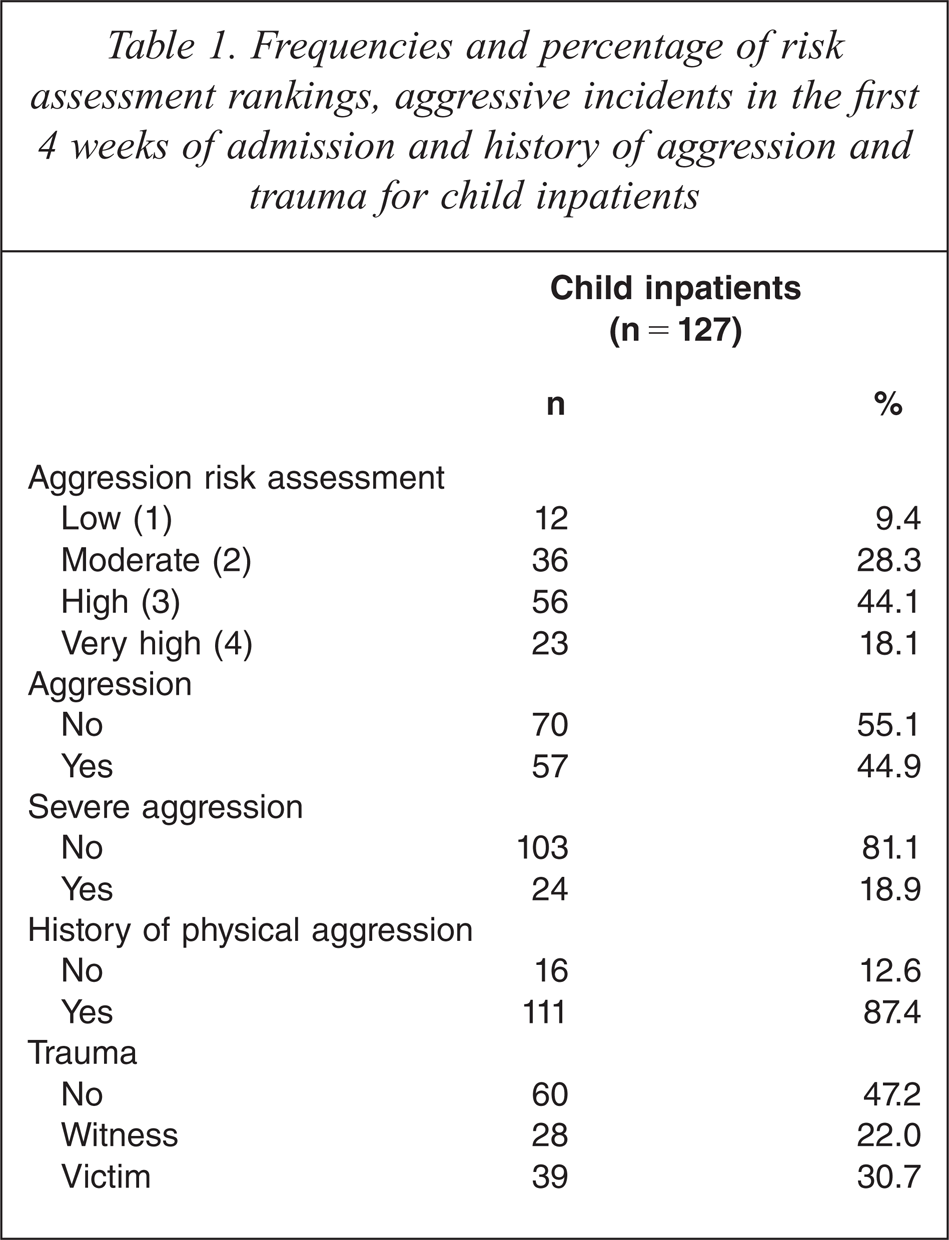
Table 1 illustrates the proportion of children assigned to each risk category, aggressive behaviour in the first four weeks of admission, and history of physical aggression and trauma. Severity of aggression was dichotomously coded as no severe aggression (absence of severe aggression) and severe aggression (one or more incidents of severe aggression). History of trauma (physical, sexual or emotional abuse, neglect, witnessing domestic violence or the suicide or death of a close family member or friend) was coded as no history, witness to trauma or victim of trauma. There were very low frequencies of patients with a history of verbal aggression or property damage only. As such, history of aggression was re-coded into a dichotomous variable, defining the presence/absence of a history of physical aggression towards others (excluding property damage). Well over half (62.2%) of the children were assigned a high or very high risk rating for aggression and just under half (44.9%) of the children were aggressive in the first four weeks of stay. Nearly one in five (18.9%) children engaged in severe aggression. A history of physical aggression was common in most children (87.4%), as was a history of trauma (67%).
Frequencies and percentage of risk assessment rankings, aggressive incidents in the first 4 weeks of admission and history of aggression and trauma for child inpatients
Primary diagnoses were grouped into six categories according to the DSM-IV [12]; mood disorders (depression and dysthymic disorder), anxiety disorders (generalized anxiety disorder, separation anxiety, obsessive–compulsive disorder, post-traumatic stress disorder and selective mutism), adjustment disorders, disruptive behavioural disorders (oppositional defiant disorder, disruptive behaviour disorder not otherwise specified, attention-deficit-hyperactivity disorder, conduct disorder and mixed disorder of emotions and conduct) relationship disorders (reactive and severe attachment disorder and parent–child relationship disorder) and developmental disorders (pervasive development disorder not otherwise specified, Asperger's, autism, mental retardation and mild intellectual disability). Two cases with primary diagnoses of anorexia nervosa and factitious disorder, respectively, could not be classified into the above diagnostic categories and were removed from further analyses including the primary diagnoses variable. The variable ‘any diagnosis of disruptive behavioural disorder’ (Any DBD) was created to account for children with multiple diagnoses and was dichotomously coded as the presence/absence of any DBD. This variable consisted of the same cluster of diagnoses as the primary diagnosis of DBD variable.
Figure 1 demonstrates that the majority of children were given a primary diagnosis of DBD. Anxiety and relationship disorders were also common in this sample.
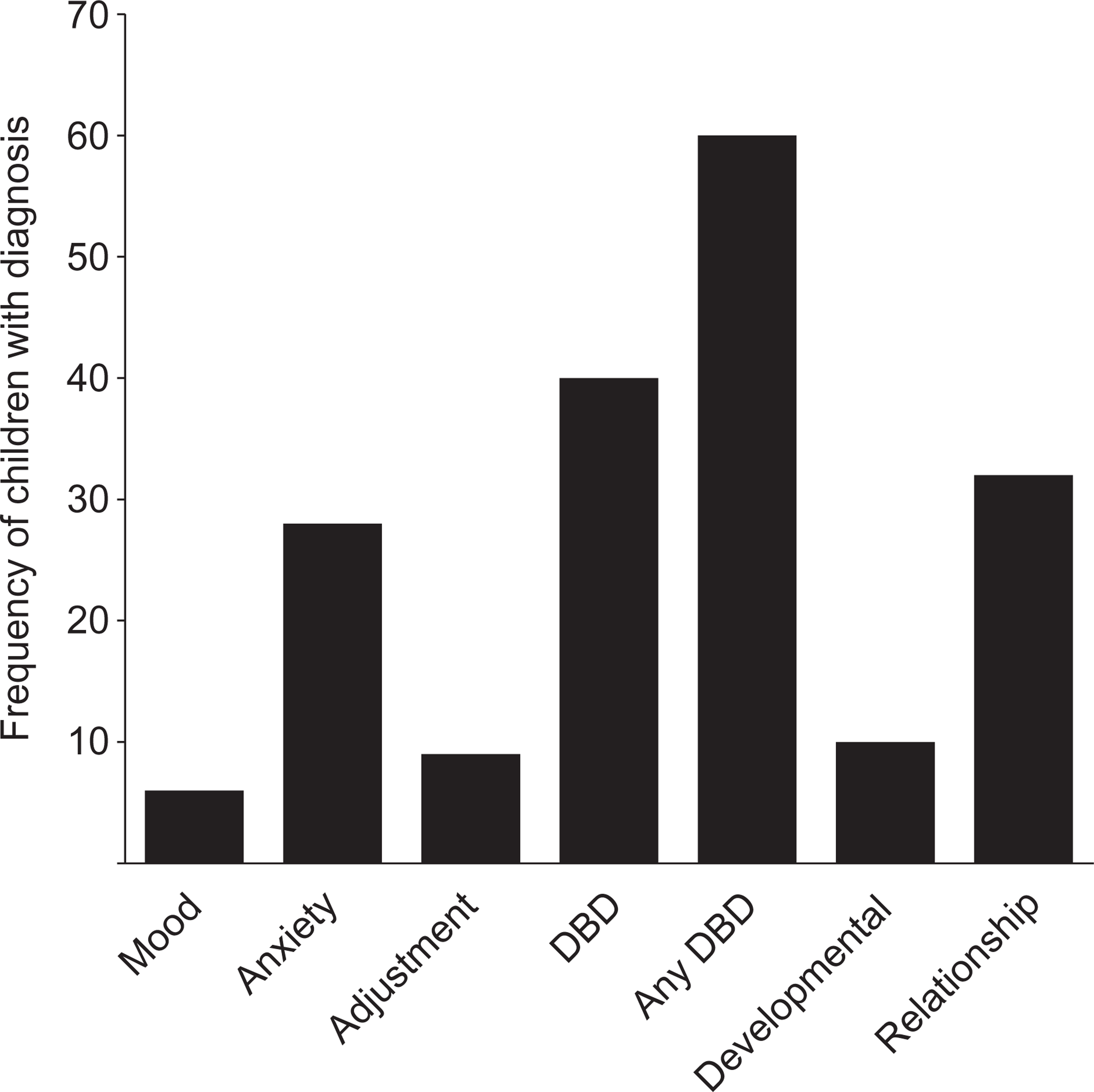
Frequency of primary discharge diagnoses and any DBD for child inpatients.
The proportion of children that engaged in aggression for each diagnostic category was explored. Table 2 indicates that 50% of children with a primary diagnosis of DBD were aggressive. Children with any DBD were more likely than those without any DBD to engage in aggression, with 58.3% engaging in aggression and 25% engaging in severe aggression. Children with a primary diagnosis of adjustment disorder were also likely to become aggressive, with 55.6% of children engaging in one or more acts of aggression and 33.3% engaging in severe aggression, as were children with a primary diagnosis of a relationship disorder with half of these patients becoming aggressive in the first four weeks of admission.
Frequencies of aggression and severity of aggression in child inpatients by primary diagnosis and any DBD
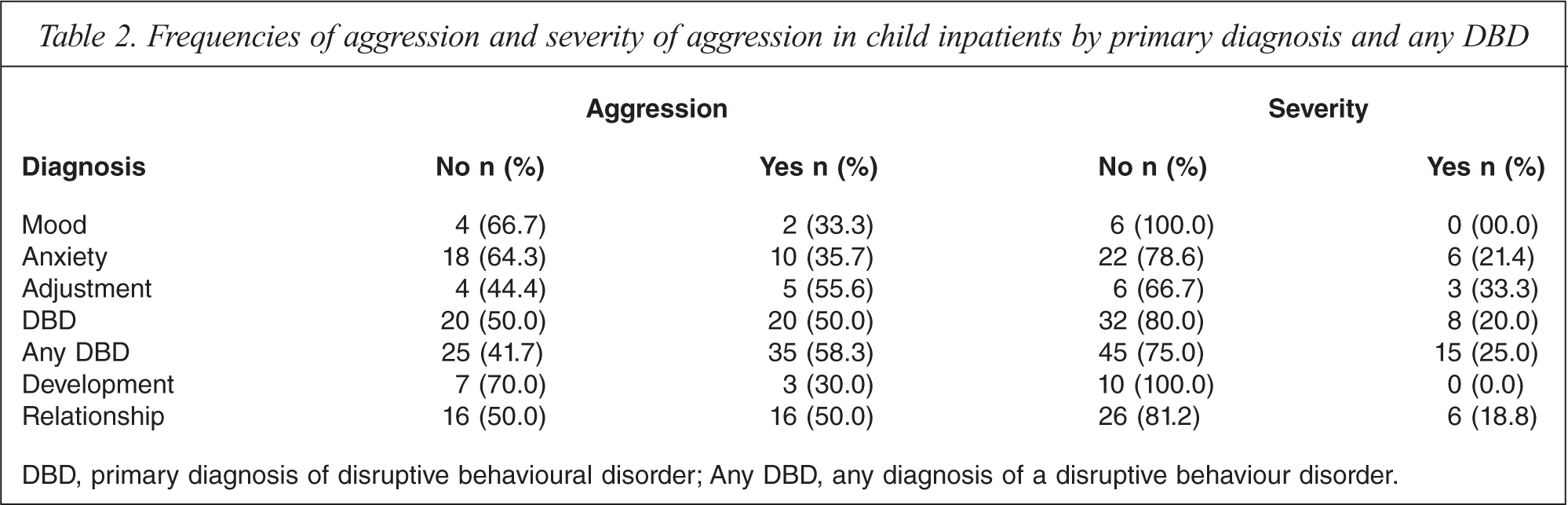
DBD, primary diagnosis of disruptive behavioural disorder; Any DBD, any diagnosis of a disruptive behaviour disorder.
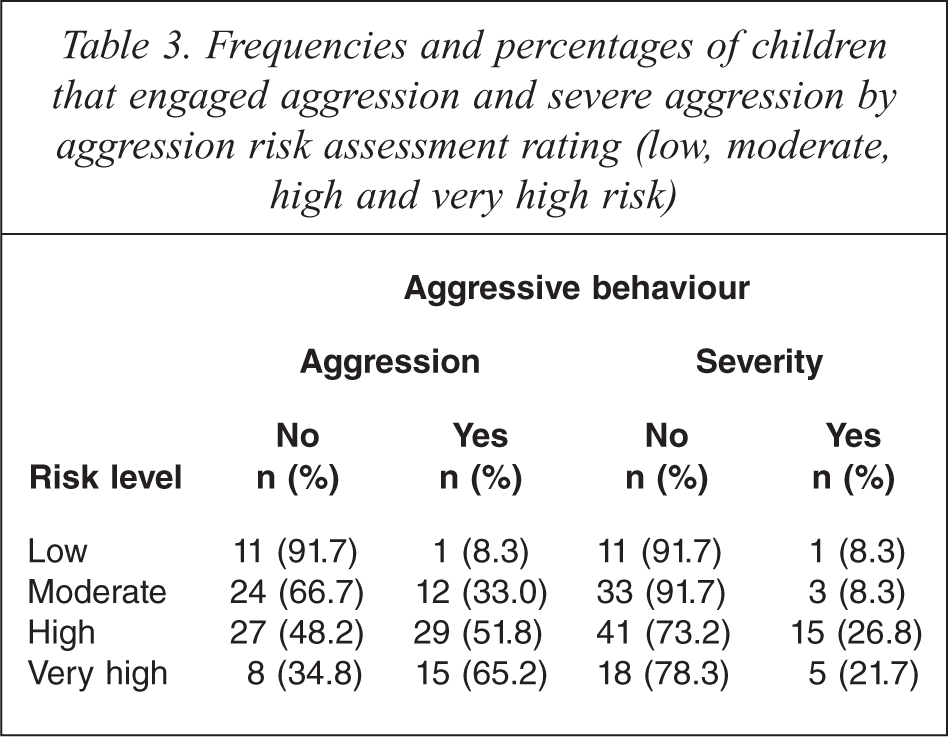
The proportion of children that engaged in aggression within the low, medium, high and very high risk groups were explored. Table 3 illustrates that children assigned as low risk generally did not become aggressive, with only one (8.3%) patient engaging in aggressive behaviour whilst over half (65.2%) of patients assigned as very high risk were aggressive. Interestingly, there was a substantial proportion (34.8%) of very high risk children that were not aggressive. Severe aggression was more common in the high and very high risk groups, however; four patients within the low and moderate risk groups engaged in severe aggression.
Frequencies and percentages of children that engaged aggression and severe aggression by aggression risk assessment rating (low, moderate, high and very high risk)
Non-parametric Spearman rank correlation analyses examined the relationship between risk assessment rankings, the additional risk factors and aggression. Dichotomous dummy variables were coded for each level of the seven diagnostic categories and the three levels of the trauma variable. Variables found to be correlated with the two outcome variables of aggression were further analysed with chi-square analyses.
Low significant positive correlations were found between engagement in aggression and aggression risk assessment, history of aggression, victim of trauma, and any DBD, indicating that high risk assessment scores and the presence of these variables were associated with aggressive behaviour. No significant correlations were found between frequency of aggression and witnessing trauma or having a primary diagnosis of DBD. The risk assessment was not significantly correlated with severe aggression. Similarly, there were no significant correlations between the severity of aggression and a primary diagnosis of DBD, nor were there any significant correlations between the severity of aggression and any DBD. Witness and victim of trauma were the only variables found to be significantly correlated with severe aggression, although correlations were low.
Chi-square analyses confirmed that the aggression risk assessment χ2 (3, N = 127) = 13.34, p = 0.00, history of aggression χ2 (1, N = 127) = 6.33, p = 0.01, any diagnosis of DBD χ2 (1, N = 127) = 7.32, p = 0.01, and victim of trauma χ2 (1, N = 127) = 5.38, p = 0.02 were all significant with engagement in aggression. Aggression risk assessment was not significant with the severity of aggression following chi-square analyses; however, it was included in regression analyses to address the hypothesis of this study. The variables of witness to trauma χ2 (1, N = 127) = 4.30, p = 0.04 and victim of trauma χ2 (1, N = 127) = 9.07, p = 0.00 remained significant with severe aggression.
Binomial logistic regressions assessed the extent to which risk assessment ratings predicted engagement in aggressive behaviour in the first 4 weeks of admission. Results are displayed in Table 4. Variables assessed for predictive validity of frequency of aggression represented a significant model, χ2 (3, N = 127) = 23.74, p = 0.00, and accounted for between 17% (Cox & Snell R square) and 22.8% (Nagelkerke R square) of the variability in aggression. The predictor variable history of aggression was removed from the regression analysis as it was not found to significantly contribute to the variability in aggression. The model correctly identified 64.3% of children that did not engage in aggression and 79.1% that did engage in aggression. The aggression risk assessment was the strongest predictor of aggression and the odds ratio indicates that those with higher risk rankings were 2.15 times more likely to become aggressive. Any diagnoses of DBD and trauma victim were also significant predictors, suggesting that these children were 2.23 and 2.53 times more likely to become aggressive, respectively.
Direct logistic regression analysis of all child inpatient presentations predicting engagement in aggression and severe aggression
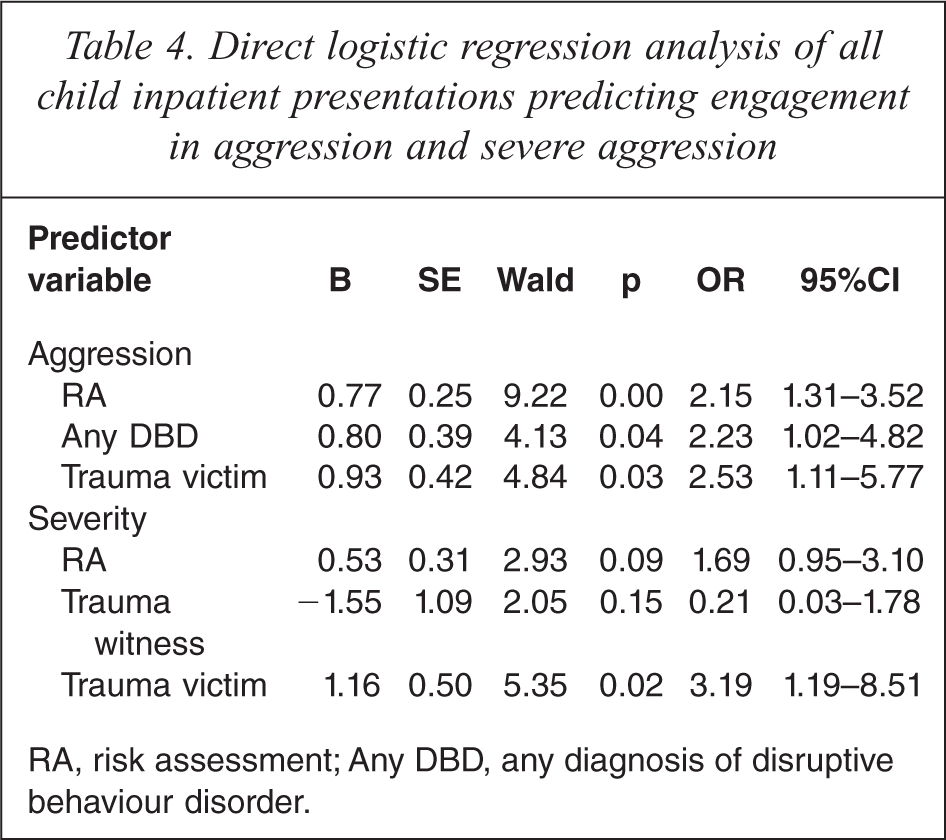
RA, risk assessment; Any DBD, any diagnosis of disruptive behaviour disorder.
Variables assessed for the prediction of severe aggression represented a significant model χ2 (3, N = 127) = 15.97, p = 0.00 indicating that the model was able to distinguish between children that did and did not engage in severe aggression. However, the model only accounted for 11.8% (Cox & Snell R square) and 19% (Nagelkerke R square) of the variability in severe aggression. Being a victim of trauma was the strongest predictor of severe aggression indicating that those with a history of victimization were 3.19 times more likely to engage in severe aggression. The risk assessment rating was not a significant predictor in the model.
Discussion
In spite of advances in risk assessment practices, research on youth-specific measures is limited due to its recent development. This research provides support for the predictive validity of unstructured clinical risk assessment of aggression in an Australian child psychiatric inpatient unit. The aggression risk assessment was found to be predictive of engagement in aggression. Hence, children with higher risk rankings on admission were more likely to become aggressive. In contrast, and in support of Crocker, Stargatt and Denton's [11] study, the risk assessment was not predictive or correlated with the severity of aggression. Low frequency of severe aggression during the study period may have impacted on the power of the analyses to define this relationship. Another plausible reason is that the variables that impact on the frequency of aggression and those that impact on the severity of aggression are quite different, and the latter were not included in this study.
In line with previous research [7,9–11] any diagnosis of DBD and a history of having been a victim of trauma were predictive of engagement in aggression in child inpatients, although not as predictive as the aggression risk ranking. It was also expected that a history of physical aggression would be predictive of aggression in child inpatients, as past aggression has empirically been found to be the best predictor of aggression [1,7]. However, although history of physical aggression was correlated with aggression, this variable did not make a significant contribution to the regression model and was subsequently removed from the regression analysis. This departure from previous research results may well be due to the nature of the sample studied. Aggression is the main reason for referral to the SWCIPU. As such, the current sample varied little in history of aggression, with a substantial proportion (87.4%) of children having a prior history of physical aggression. Nevertheless, a history of physical aggression prior to admission is one of the main risk factors considered by the clinician when conducting the clinical risk assessment and as a result more than half of the children (62.2%) were assigned a high or very high risk rating for aggression. A history of being a victim of trauma was the only risk factor that remained significant with the severe aggression following logistic regression analyses, suggesting that children with a history of being a victim of trauma were more likely to engage in severe aggression.
This research identifies implications for clinical practice with respect to the information and methods that clinicians use to make clinical judgements of aggression risk in the child psychiatric population. In spite of previous research [13–16] this study supports the use of unstructured clinical risk assessment in predicting engagement in one or more acts of aggression in child inpatients. However, as with prior studies [17,18] the association between risk assessment rankings and aggression was relatively moderate. This was evident by low correlations and the small amount of variance in aggression accounted for by the risk rankings. Even so, these results suggest that unstructured clinical risk assessment is a better indication that an individual will engage in aggressive behaviour than a prior history of aggression or any diagnosis of a disruptive behaviour disorder alone.
The current research indicated that unstructured clinical methods of assessment of aggression are generally predictive of high and low risk children. However, while children classified at risk on the extremes, that is low risk children and high to very high risk children, are generally classified with accuracy, patients classified as moderate risk are less predictable in their aggression. As expected of moderate risk, approximately half were reported to become aggressive. It is possible that aggression in children classified as moderate risk is triggered by immediate environmental factors such as the separation from their normal environment or fear of rejection as a consequence of the inpatient admission. In contrast, aggression in high risk children is more likely to be influenced by historical and other more stable factors. From a clinical perspective, this indicates that patients at moderate risk for aggression are less predictable and therefore more difficult to appropriately manage. Consequently, different strategies may need to be implemented by clinical staff in order to effectively manage these children. To achieve this, future research should endeavour to isolate this subset of individuals to examine the historical, situational and contextual risk factors for aggression and antecedents to aggressive behaviour in order to assess how to better predict and manage aggression in this group.
This research has relevant implications for considering any diagnosis as a risk factor for aggression and not merely relying on the primary diagnosis alone. Results did not find any relationship between a primary diagnosis of disruptive behavioural disorder and aggression as has been found in other studies [6,9,11,19]. However, after accounting for children with multiple diagnoses, any diagnosis of disruptive behaviour disorder was found to significantly predict engagement in aggression. These results suggest that diagnoses other than the primary diagnosis can be as influential in predicting aggression as the primary diagnosis itself. This indicates that future research on risk factors for aggression in young psychiatric samples should not be confined to primary diagnoses. Similarly, clinical practitioners should consider giving multiple diagnoses just as much weight to their judgement of aggression risk as the primary diagnosis if relying on unstructured clinical judgement.
Interpretation of the results should acknowledge the relevant methodological limitations. Data was collected retrospectively and confined to one inpatient facility. Patients were often admitted on the basis of their aggressive behaviour, resulting in a large proportion of children with a history of aggression and a relatively homogeneous sample. Patient discharge diagnoses were recorded as in many cases a diagnosis was not available on admission. It is possible that aggression during admission may be predictive of discharge diagnosis, rather than the other way around. This research did not employ standardized tools to record aggression. Rather, aggressive incidents were recorded from a critical incident report database which was employed as a proxy measure of frequency and severity of aggression. Nevertheless, critical incident reports have been found to produce reliable information on aggressive behaviour [20]. Further, details of aggressive behaviour obtained from critical incident reports were crosschecked with the incident date in the patient's clinical notes to ascertain a more detailed account of the incident. Assessing risk on admission helps to determine appropriate management of the child. Children assigned a high risk rating are likely to receive higher levels of management than children assigned as low risk. The current study did not control for different nursing management approaches. As such, it is possible that nursing management may have moderated the relationship between the risk assessment and predictors of aggression and subsequent engagement in aggressive behaviour. Finally, the baseline frequency of aggression was not accounted for in the present study and should be taken into account when interpreting the results.
Conclusions
Identification of patients at high risk for aggressive behaviour is crucial in the management of aggression in child inpatient facilities. This research sought to examine the predictive validity of unstructured clinical risk assessment in predicting aggression in child inpatients. A high risk rating was the best indication that a child would engage in aggression when compared to associated risk factors for aggression, and was a better predictor than diagnosis or history of aggression providing support for unstructured clinical risk assessment in clinical practice. The risk assessment did not, however, distinguish between children that engaged in severe aggression and those that did not. Further, the risk assessment ranking, history of being a victim of trauma and any diagnosis of a disruptive behaviour disorder only accounted for between 17% and 22.8% of the variance in aggression. Nevertheless, a high risk assessment rating was better able to predict engagement in aggression than a history of physical aggression alone.
Footnotes
Acknowledgements
The authors would like to thank the staff at the Austin Health CAMHS for their assistance with this research. We would particularly like to acknowledge Christine Denton, then Nurse Unit Manager and Jacinta Barens, Ward Clerk.