
Abstract
Mental disorder accounts for a small proportion of all crime [1,2]. However, there is a well-established association between schizophrenia and violence [3–8], especially homicide [9–12]. Two recent meta-analyses of studies from developed countries found that people with a diagnosis of schizophrenia commit 6.5% of homicides, irrespective of the total homicide rate [13] and that the odds ratio (OR) for all forms of violent offending when compared to the general population is 4 for men, 8 for women and 20 for homicide by either sex [14].
The relationship between schizophrenia and violence has been examined in studies that link criminal histories to records of psychiatric treatment [3,6,8,15] and in case control, longitudinal and cohort design studies [14,16,17]. The available evidence suggests that the relationship between schizophrenia and violence is largely mediated by co-existent substance abuse [16–18]. The strength of the association between psychosis and violence is greater for more serious forms of violence, in particular homicide [13,14] and appears to be related to the stage of illness, as most violence by people with psychosis is committed in the earlier stages of the illness [1,6,15]. Studies of patient cohorts have reported high rates of aggression and minor forms of violence prior to initial treatment for psychosis [19–23] and rates of homicide during first episode psychosis have been estimated to be 15 times higher than after treatment and are linked to treatment delay [24,25,26]. Studies of aggression and violence in mental health settings have generally divided violence into less or more serious categories, although the violence rated as more serious in these studies rarely includes assaults resulting in serious injury to the victim or criminal charges [23,27]. Hence, although homicide committed during mental illness and violence among patient groups is well described, less is known about the characteristics of people who commit severe forms of violence that falls between homicide and the violence reported in clinical samples.
We report an observational study of the characteristics of a consecutive sample of violent offenders with psychotic illness who were found to have committed violent offences that were severe enough to be committed for trial to the District Court of New South Wales, Australia. The assaults were often life threatening and many resulted in serious physical injuries to the victims. The aims of the study were (i) to determine the proportion of all severe violent assaults resulting in serious injury but not death that were committed by people with a psychotic illness, (ii) describe the characteristics of people with psychosis who commit severe violent offences, and (iii) to estimate the proportion of those with psychosis who commit a serious violent offence who had never received treatment with antipsychotic medication prior to the offence and could be regarded as being in their first episode of psychosis.
Methods
In New South Wales (NSW), over 95% of all criminal cases, including assaults resulting in minor injury, are dealt with in the Local Court, and homicide offences are usually dealt with in the Supreme Court [28]. Cases involving serious violent offences that result in significant injury but not death, including attempted murder, wounding and assaults causing serious injury, are heard in the District Court.
The archives of the District Court of NSW were searched for all cases that concluded between 1 January 2006 and 31 December 2007 in which there was a conviction or a finding of not guilty due to mental illness for an offence involving an act of violence towards another person. The following violent offences defined in sections of the NSW Crimes Act (1900) were included: attempted murder (s 27 to s 30), malicious wounding or inflict grievous bodily harm with intent to do so (s 33), recklessly inflict grievous bodily harm or wounding (s 35), attempt to choke (s 37), assault causing grievous bodily harm (s 54) and assault occasioning actual bodily harm (s 59). Arson, robbery and sexual assaults were not included unless accompanied by a separate charge for an assault causing injury.
Case files that included at least one report from a psychiatrist, psychologist or other mental health professional were examined in detail. In addition to the reports of mental health experts, legal documents in the case files, including the Indictment, Police Fact Sheets, history of criminal convictions, witness statements, Probation and Parole Service pre-sentence reports and written judgements were examined. The characteristics and circumstances of offenders with a diagnosis of a psychotic illness, defined as schizophrenia spectrum psychosis (schizophrenia, schizophreniform psychosis, delusional disorder, schizoaffective disorder, drug-induced psychosis and psychosis not otherwise specified), bipolar disorder and psychotic depression were examined by the extraction of the following data:
Demographic and developmental data, including age, gender, marital status, ethnicity, employment status at the time of offence, educational level, any history of childhood trauma, and any history of brain injury.
Clinical and substance use data, including reported symptoms, psychiatric diagnosis, age of onset of illness, any previous psychiatric admission or treatment, adherence to treatment at the time of the offence, any previous substance misuse, and intoxication at the time of the offence.
Offence data, including weapon use, relationship to the victim, age at first criminal conviction, the verdict and the sentence imposed.
Each case was classified according to whether the offence occurred in the first episode of psychosis or after previous treatment for psychosis, according to a stage-of-illness model [29] and the definition of first episode psychosis [30]. The term ‘first episode psychosis’ was used synonymously with ‘never treated psychosis’, and includes patients in their first weeks of antipsychotic treatment who have yet to respond to treatment. First episode psychosis was defined as the period between the onset of positive symptoms of psychosis and an adequate period of treatment, irrespective of whether there had been previous remissions without treatment. Patients were defined as having previously treated psychosis if they had ever received an adequate period of treatment with antipsychotic medication, regardless of whether there had been a remission from acute symptoms as a result of treatment, or whether the patient was adherent to treatment at the time of the offence.
Approval to conduct the study was obtained from St Vincent's Hospital Human Research and Ethics Committee, the University of New South Wales Human Research Ethics Committee and the Chief Judge of the District Court of New South Wales.
Results
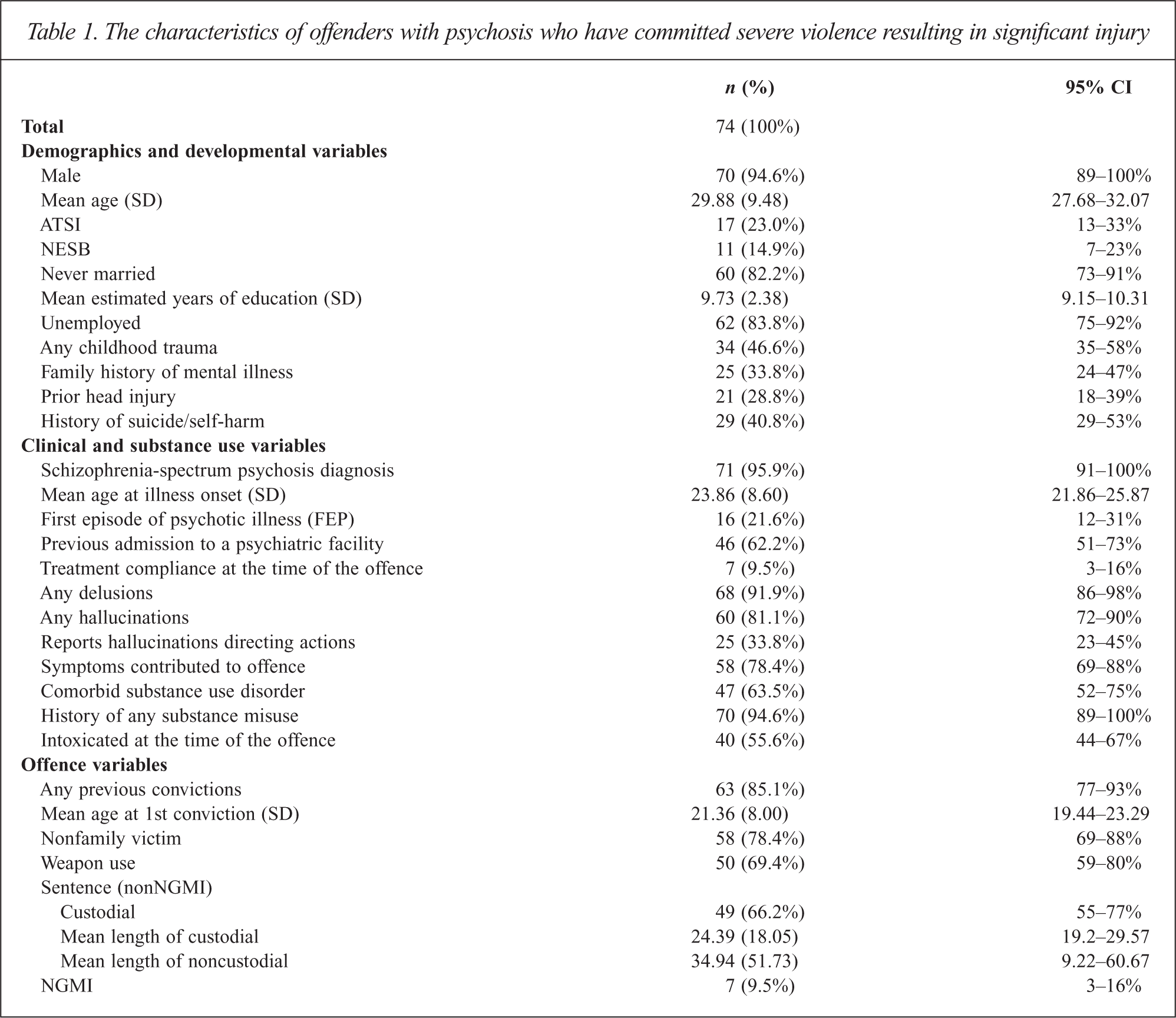
In the years 2006 and 2007, 6809 individuals charged with criminal offences had their matters concluded in the District Court of NSW. Of these, 661 were found to have committed a severe violent offence causing significant injury and in 366 cases the file contained at least one written report by a mental health professional about the defendant. Based on the diagnoses made in those reports and other documents, 74 of the 661 (11%, 95% CI 9–14%) offenders had a diagnosed psychotic illness. A conviction was recorded in 67 of those cases and in seven cases the verdict was not guilty due to mental illness. The demographic, clinical, and offence data are presented in Table 1.
The characteristics of offenders with psychosis who have committed severe violence resulting in significant injury
Demographic and developmental characteristics
The 74 subjects diagnosed with psychosis were predominantly male (95%) with a mean age of 30 years, had mostly never married (82%) and most were unemployed at the time of the offence (84%). A total of 17 (23%) were of Aboriginal or Torres Strait Islander heritage and 11 (15%) were born in a non-English speaking country. According to the court records almost half of the subjects reported some form of neglect or trauma as a child (47%) and a history of self-harm or a suicide attempt (41%). A family history of mental illness was noted in the reports about 25 (34%) offenders with a diagnosed psychotic illness.
Clinical characteristics
The diagnosis of a schizophrenia-spectrum psychosis was made in 71 (96%) cases and in three cases (4%) the diagnosis was affective psychosis (two in the manic phase of bipolar disorder and one with psychotic depression). At the time of the offence 16 subjects (22%) were in their first episode of psychotic illness. Only seven of the 58 previously treated offenders (12%) reported taking antipsychotic medication in the period preceding the offence. More than half of the offenders (62%) had previously been admitted to a psychiatric facility although four of those had not been treated for psychosis and were in the first episode of psychosis at the time of the offence.
Most of the offenders reported auditory hallucinations (80%) or delusional beliefs (92%) at the time of the offence. The delusions included beliefs that were persecutory, religious, grandiose and jealous in content. Auditory hallucinations directing the person's actions were reported by 25 offenders (34%). In 54 cases (78%), the experts concluded that the presence of positive symptoms of psychotic illness contributed to the assault.
Substance misuse
A history of substance misuse, defined as documented hazardous alcohol intake or the use of any illicit drug, was noted in almost all cases (95%), with 47 subjects (64%) receiving the additional diagnosis of a substance use disorder in the reports tendered to court. The most frequently misused drugs were cannabis (82%) and alcohol (73%). Other drugs included amphetamine, heroin, cocaine, hallucinogens and sedative medications. A total of 40 subjects (56%) reported intoxication with alcohol or another drug at the time of the offence.
Offence characteristics
More than half of the assaults (69%) involved a weapon, mainly kitchen knives, domestic implements such as scissors and pieces of wood. None of the offences involved the use of a firearm. The injuries in remaining cases were caused by punching, kicking or by strangulation.
The victims comprised 35 (47%) strangers, including two fellow patients, two mental health professionals and a police officer, 23 friends or acquaintances and 17 family members, including intimate partners. In one case, both a partner and a bystander were injured in the assault.
Some 63 (85%) of the offenders had a previous conviction for offences that included drink driving, drug-related property offences and assaults. In 37 cases (58%) the first criminal conviction predated the onset of psychotic illness (mean age of first conviction of 21 years compared to the mean age of onset of illness of 24 years).
First episode psychosis versus previously treated psychosis
Of the offenders with a diagnosis of psychotic illness, 16 (22%, 95% CI 12–31%) had never received treatment with antipsychotic medication and could be regarded as being in the first episode psychosis. The never treated patients comprised 2.4% (95% CI 1.5–3.9%) of all the severe non-lethal assaults in the two years of the study. The small number of first episode psychosis cases prevented any meaningful statistical comparisons between those with never-treated psychotic illness and those who had received treatment. However, the first episode subjects were more likely than previously treated patients to be female (13% versus 3%), to be from non-English speaking country (31% versus 10%), were less likely to have a previous criminal conviction (63% versus 90%) and were older at the time of the onset of the psychotic illness (mean age 27 years versus 23 years).
Discussion
To our knowledge, this is the first study to specifically report on the characteristics of a complete sample of individuals with psychotic illness charged with a severe violent offence resulting in serious injury. The findings confirm the presence of an association between psychosis and severe violence, as the proportion of individuals with psychotic illness among offenders (11%) is approximately 20 times higher than the estimated prevalence of psychotic illness in the general population of 0.5% [31]. This result is similar to an earlier finding that 8.8% of homicide offenders in NSW were psychotic at the time of the offence [12]. Only two of 661 violent offenders were identified to be in the manic phase of bipolar disorder, which suggests that mania is not associated with severe violence.
Of the severe violence offenders with psychosis, 22% had never received treatment with antipsychotic medication. Despite the relatively small number of cases and hence the wide confidence intervals for the proportion of untreated cases, the ratio of treated to untreated cases of 5:1 is higher than expected. Based on the epidemiology of the incidence and prevalence of psychosis [31] or the average duration of untreated psychosis and the generally life long course of schizophrenia [32] the expected ratio of treated to untreated cases would be about 20:1. Hence the risk of severe non-lethal violence appears to be moderately elevated in first episode psychosis relative to previously treated psychosis [33]. However, the proportion in first episode psychosis in this sample of severe non-lethal violence was lower than the proportion of never treated psychosis among those found not guilty due to mental illness in NSW for non-lethal violent offences between 1992 and 2008 (54 of 134, 39%) [34]. It is also lower than the proportion of first episode patients found in studies of other forms of severe violence in psychosis, including homicide (61%) [12], child homicide (58%) [35], stranger homicide (64%) [36], violent suicide attempts (49%) [33], attempted suicide by jumping from a height (44%) [37], attempted suicide by self-stabbing (57%) [38], major self-mutilation (54%) [39] and self-enucleation (49%) [40]. This suggests that the most serious forms of violence in psychosis are more strongly associated with first episode psychosis.
The characteristics of the offenders convicted of serious non-lethal offences differ from those of homicide offenders with psychotic illness in NSW [12]. They were more likely to have criminal convictions, and to be intoxicated at the time of the offence, and the victims were more likely to be strangers than family members or close associates. Furthermore, most of the homicide offenders were found to be not guilty due to mental illness, whereas only 10% of the severe violence offenders with psychosis received a verdict of not guilty by reason of mental illness. The lower rate of not guilty by reason of mental illness verdicts among offenders committing severe violence offenders might be because these offences were less likely to be directly linked to symptoms of psychotic illness than homicides. Alternatively, some offenders facing non-homicide charges who had the defence of mental illness open to them might have elected to enter a plea of guilty in order to avoid indefinite detention in a secure hospital. In other respects, the characteristics of the violent offenders with psychotic illness in this study were similar to criminal populations without psychotic illness. Being single, male, indigenous, unemployed, having a history of previous criminal convictions and a history of substance abuse are all risk factors that have been associated with criminal behaviour and recidivism in the general population [41].
There are a number of studies showing that the association between violence offences and severe mental illness is mediated by a range of factors in addition to the effect of symptoms of mental illness [8,13]. For example, in their population-based study, Elbogen and Johnson [42] found that violence by the mentally ill was associated with a range of historical (past violence, physical abuse, parental arrest record), clinical (recent substance use, perceived threats), dispositional (age, gender, income), and contextual (recent divorce, unemployment and victimization) that were present during each phase of illness. The findings of this study support the view that violence by people with psychotic illness is complex in its origins and is not well explained by one single factor. However, the high proportion of offences committed by people with active symptoms of psychotic illness and the low rates of adherence to treatment in these offenders was striking.
Substance use has emerged as an important factor mediating the relationship between psychosis and violence, as both large population-based studies and meta-analyses of smaller studies have consistently shown that co-morbid substance use greatly increases the risk of violence in individuals with psychotic illness [4,6,8,14,20,41]. Fazel and colleagues [14] found that the odds ratio of violence in those with psychosis and co-morbid substance abuse was about 9, similar to risk associated with substance use alone in the absence of psychosis, whereas the risk among non-substance using patients was only modestly elevated (OR = 2). In our sample, almost every offender with psychosis also had a history of some form of substance abuse, in particular abuse of cannabis. Although much attention has been given to the role of alcohol as a causal factor in violence in the community, there is evidence to suggest that cannabis has a particular contributing role in acts of violence committed by patients with psychotic illness [23,43,44].
The combination of high rates of substance misuse and poor treatment adherence suggests that to be effective in reducing the incidence of serious violence by those with established psychotic illness, mental health services need to concentrate on preventing disengagement from services in order to both improve treatment adherence and encourage patients to reduce substance use. At a community level, prevention strategies should address the common factors that give rise to all forms of violent offending, including the quality of housing, access to weapons (including knives), supported employment and access to treatment for mental illness and substance abuse [45].
The main limitation of this study is that we relied on cases where psychiatric evidence was available and we were unable to estimate how many undiagnosed cases of psychotic illness there were among the 45% of violent offenders who did not have a report by a mental health professional. It is not uncommon for the presence of psychotic illness to be overlooked until after a trial, or for defendants to instruct their legal representatives not to raise the issue of mental illness, especially if they claim they did not commit the offence. Hence our finding might be an underestimate of both the rate of psychotic illness among severe violence offenders and the proportion of subjects who were in the first episode of psychotic illness. Other researchers faced with a similar dilemma have suggested that the underestimation of mental illness in samples of violent offenders is similar to the underestimation of mental illness in community prevalence studies [1]. Another limitation is that the study relied on the diagnoses made for the court by a range of mental health professionals. However, many of the cases had more than one expert report as well as information from treating agencies. In those cases in which written reports were available, it is likely that the diagnosis was reliable because a recent study conducted in the same jurisdiction found a high level of inter-rater agreement about psychiatric diagnosis [46,47] as well as the availability of the mental illness defence [48].
Conclusions
The high proportion of violent offenders with a diagnosed psychotic illness found in this study confirms the association between psychosis and serious non-lethal violence. This is consistent with the findings of studies of homicide and violence in patient populations. However, the results of this study suggest that the factors associated with lethal violence might differ from those of less serious violence. Lethal violence is strongly associated with severe and untreated psychosis, whereas less severe violence is also associated with the same factors that contribute to violent offending in general, particularly substance abuse and a pattern of antisocial conduct. As about 10% of severe non-lethal violence is committed by people with either never treated or under treated psychosis, earlier treatment of emerging psychosis, and measures to improve adherence to antipsychotic medication and reduce substance abuse by people with psychotic illness could result in a modest reduction in levels of serious violence.
Footnotes
Acknowledgements
The authors wish to thank the Chief Judge of the District Court of New South Wales, Tyler Qin of the District Court Registry and staff at the New South Wales Bureau of Crime Statistics and Research (BOCSAR) for their assistance.