
Abstract
Most patients experiencing the initial acute phase of first-episode psychosis (FEP) are likely to be admitted to an inpatient unit despite the availability of communitybased treatment. The evidence indicates that between 63% and 81% of patients with FEP require hospitalization [1–6], with variability in estimates probably because of differences in study methodology and/or service delivery. The majority of first admissions occur soon after entry to treatment [2–5] and readmission is relatively common [2–4]. For example, Edwards et al. [2] reported that 83% of first admissions occurred during the first 3 months of treatment and that 50% of hospitalized patients were readmitted at some stage during the 18-month follow-up period. Previous FEP studies have found that admission is associated with a diagnosis of affective psychosis [1, 4], manic symptoms [5], more severe behavioural disturbance [1, 4] and more severe global psychopathology [4]. However, no association has been found between inpatient admission and demographic characteristics [1, 4, 5] or the overall severity of positive psychotic symptoms [4, 5], although paranoid or grandiose delusions and auditory hallucinations have been found to be more common in hospitalized patients [1].
To date, there has been little study of factors associated with multiple inpatient admissions during the initial acute phase of FEP. There were two aims of the current study. The first aim was to investigate the rate, pattern and correlates of inpatient admission during the initial 3 months of treatment for FEP. The pattern of inpatient admission was based on the number of admissions during this period, that is, none, one, or multiple. The second aim was to determine whether the pattern of inpatient admission during the initial treatment period predicted inpatient service use during the following 12-month period or the rate of remission at 15-month follow-up.
Method
Clinical setting
The Early Psychosis Prevention and Intervention Centre (EPPIC) is a comprehensive FEP treatment service mandated to treat all individuals aged 15–29 years experiencing a first psychotic episode who present to public mental health services in an urban catchment region of Melbourne, Australia [7]. It is an established service with a high profile; and there are few private psychiatrists or other health services in the region providing treatment for FEP. As a result, EPPIC treats a high proportion of incident cases of psychosis aged 15–29 years in the catchment region. There were approximately 848 400 residents in the catchment area at the time of data collection [8].
Assessment
One hundred and twelve consecutive patients were accepted for treatment at EPPIC between 19 March 2001 and 1 August 2001. Demographic information was obtained from patient interviews at baseline. Inpatient data for the 15-month follow-up period were derived from an electronic database of psychiatric service use. Diagnoses of DSM-IV [9] psychotic and non-psychotic disorders were made using an updated version of the Royal Park Multi-Diagnostic Instrument for Psychoses (RPMIP) [10]. Diagnostic information was derived from multiple sources at baseline and 3-month follow-up including a patient interview (n = 108) as well as an informant interview with a family member and/ or the treating medical officer and a review of the medical records (n = 112). The RPMIP was also used to estimate the duration of untreated psychosis (DUP) in days, defined as the time from onset of psychotic symptoms to entry to treatment for the current episode.
Clinical ratings were available for two-thirds of the patients (n = 71 at baseline and n = 68 at 3 and 15 months owing to three patients with missing data) who participated in a follow-up research study [11]. The inclusion criteria for the study were 15–29 years old, fluency in English, ability to give informed consent and clear evidence of psychosis. The exclusion criteria were organic aetiology, intellectual impairment, history of brain damage or epilepsy, or more than 6 months of prior treatment for a psychotic disorder. Clinical ratings were undertaken using the Health of the Nation Outcome Scales (HoNOS) [12] at baseline and 3-month follow-up and the Brief Psychiatric Rating Scale (BPRS) [13] and a measure of medication compliance at baseline, 3-month, 9-month and 15-month follow-up. The HoNOS ratings were made on the basis of a field trial version and converted to the latest version. Items 11 and 12 of the HoNOS were not considered because of concerns raised regarding their reliability [14]. The HoNOS scores were recorded to reflect a clinical or other problem of at least moderate severity (a score of 3 or 4) or less than moderate severity (a score of 2 or less). A rating of 3 or 4 on either item 1 (‘Problems with overactive, aggressive or agitated behaviour’) or item 2 (‘Problems with non-accidental self-injury’) was deemed to reflect the presence of ‘Problems with risks to self or others’ of at least moderate severity. Remission of positive psychotic symptoms was defined as a score of 3 or less for at least 2 weeks on all items of the BPRS Psychotic Subscale: hallucinations, conceptual disorganization, unusual thought content, or suspiciousness. Assessment for remission was undertaken at all follow-up assessments and, if relevant, a best estimate of the date of onset of remission was derived by asking patients to recall the date when remission criteria were first met using prompts of significant calendar dates if necessary. Medication compliance was rated on a 4-point scale: 1 for 0–24% compliance (no or irregular compliance); 2 for 25–49% compliance (rather irregular compliance); 3 for 50–74% compliance (rather regular compliance); 4 for 75–100% compliance (regular compliance). All ratings were subsequently recoded to denote compliance (a score of 4) or noncompliance (a score of 3 or less). Medication non-compliance during 15-month follow-up was subsequently defined as the presence of any score less than 4 during follow-up. All clinical ratings were based on patient interviews supplemented by information derived from informants (family members and/or clinicians) and a review of medical records. An experienced clinical psychologist (DW) undertook all clinical assessments and data collection after being trained in the administration of the RPMIP, BPRS and HoNOS by a senior research assistant prior to commencement of the study. Inter-rater agreement on the 24 BPRS items and the four BPRS Psychotic Subscale items was assessed by comparing ratings made by the first author (DW) and a research assistant on five cases. Agreement was defined as the percentage of items that were rated within one point by both raters. A minimum of 95% agreement was achieved on the 24 BPRS items and the four BPRS Psychotic Subscale items.
The research and ethics committees of the North-Western Mental Health program approved the study.
Data analysis
Assessment of group differences on nominally measured variables was undertaken by cross-tabulating the data and performing chisquared tests of independence, with exact tests used where appropriate. Group differences on continuous variables were assessed using independent samples t-tests, and for more than two groups, one-way anova was performed. Tukey's Honestly Significant Difference post-hoc test was used to isolate specific group differences where a statistically significant omnibus F-test was obtained. The non-parametric Mann– Whitney U-test or the Kruskal–Wallis test for multiple groups were employed for data that were substantially skewed. All statistical tests were two-tailed and results regarded as statistically significant at or below the 0.05 probability level.
Analyses were undertaken using SPSS for Windows (version 12.0.2, SPSS Inc. Chicago, US).
Results
Sample
Of the 112 consecutively admitted patients, 73 (65.2%) were diagnosed with a non-affective psychosis that included schizophrenia (n = 41), schizophreniform disorder (n = 17), psychotic disorder NOS (n = 5), substance-induced psychotic disorder (n = 5), delusional disorder (n = 4) and brief psychotic disorder (n = 1). Thirty-one (27.7%) patients were diagnosed with an affective psychosis that included bipolar disorder (n = 18), schizoaffective disorder (n = 11) and major depressive disorder (n = 2). Eight (7.1%) patients were not diagnosed with a functional psychosis: seven patients who reported psychotic symptoms at referral were diagnosed with a cluster B personality disorder and one patient was diagnosed with a psychotic disorder because of a general medical condition. There was almost perfect agreement (kappa = 0.91; unadjusted agreement = 95.5%) between research and file-based diagnoses of non-affective psychosis, affective psychosis, or other psychiatric disorder in 111 cases (one patient did not have a filebased diagnosis recorded). The patients not diagnosed with a functional psychosis (n = 8) were excluded from further analyses, leaving a sample of 104 patients.
No significant differences were found between participants (n = 71) and non-participants (n = 33) in the follow-up study on the following variables: gender (p = 0.91), age (p = 0.77), age at onset of psychosis (p = 0.67), educational level (p = 0.61), marital status (p = 0.10), inpatient admission (p = 0.85), or pattern of inpatient admission (none, one or multiple; p = 0.94). However, participants were more likely to live with family (81.7% vs 57.6%, p = 0.01) and to have a diagnosis of affective psychosis (36.6% vs 15.2%, p = 0.03) with shorter DUP (mean = 123.0; SD = 257.4; median = 28.0 vs mean = 281.2; SD = 434.6; median = 90.0; Mann–Whitney U-test: z = − 2.54; p = 0.01) compared with non-participants.
Rate and pattern of inpatient admission
Eighty (76.9%) of 104 patients were admitted to an inpatient unit during the first 3 months of treatment. Fifty-nine (56.7%) patients had a single admission and 21 (20.2%) had multiple admissions during this period.
Correlates of inpatient admission
Patients with no admission, one admission, or multiple admissions during the first 3 months of treatment were compared on demographic and illness variables, the duration of inpatient stay and the use of a community treatment order during the first 3 months of treatment (see Table 1).
Demographic and illness characteristics, duration of inpatient stay and use of a community treatment order for patients with no admission, one admission and multiple admissions during the initial 3-month treatment period (n = 104)
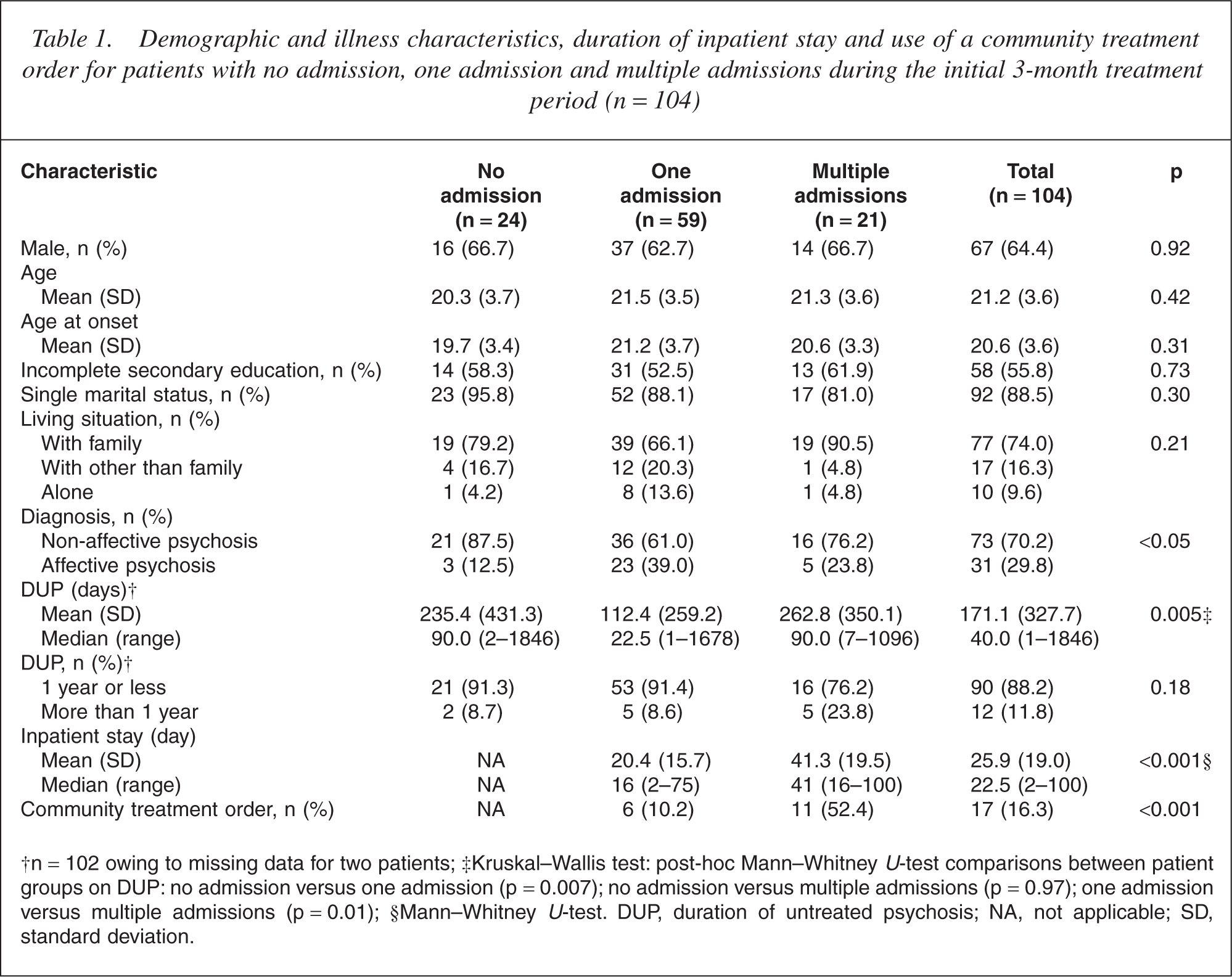
†n = 102 owing to missing data for two patients; ‡Kruskal-Wallis test: post-hoc Mann-Whitney U-test comparisons between patient groups on DUP: no admission versus one admission (p = 0.007); no admission versus multiple admissions (p = 0.97); one admission versus multiple admissions (p = 0.01); §Mann-Whitney U-test. DUP, duration of untreated psychosis; NA, not applicable; SD, standard deviation.
Demographic characteristics
There were no significant associations between demographic characteristics and the pattern of inpatient admission.
Diagnosis
Patients with a single inpatient admission were significantly more likely to be diagnosed with affective psychosis and patients with no admission were significantly less likely to be diagnosed with affective psychosis. A similar percentage of patients with no admission (n = 14, 58.3%) and multiple admissions (n = 14, 66.7%, p = 0.57) were diagnosed with schizophrenia or schizophreniform disorder. Twenty-four (92.3%) of the 26 patients who presented with a manic syndrome (eight with schizoaffective disorder and 18 with bipolar disorder) were admitted to hospital.
Duration of untreated psychosis
Patients with one admission had a significantly shorter DUP than patients with multiple admissions or no admission. However, when only patients with non-affective psychosis (n = 71 owing to missing DUP data for two patients) were included in the analysis, this association was no longer statistically significant (Kruskal–Wallis test; p = 0.23). There were no significant between-group differences on DUP in excess of 1 year.
Duration of inpatient stay and use of a community treatment order
Not unexpectedly, patients with multiple admissions had a signifi-cantly longer duration of inpatient stay and were significantly more likely to be placed on a community treatment order during the first 3 months of treatment compared with patients with one admission.
Clinical ratings for subsample of patients
Patients with no admission, one admission, or multiple admissions were compared on a range of clinical ratings at baseline and 3 month follow-up (Table 2). Patients with no admission had significantly lower BPRS total scores at baseline compared with patients with one or multiple admissions. Patients with no admission were significantly less likely to have moderate-severe cognitive problems, mental and behavioural problems (other than those associated with depression and psychosis), and problems with activities of daily living on the HoNOS at baseline compared with patients with one admission. Patients with multiple admissions were significantly more likely to have moderatesevere problems on the HoNOS with risks to self or others, including overactive, aggressive or agitated behaviour, at baseline and 3-month follow-up, compared with patients with one or no admission. At 3-month follow-up, patients with multiple admissions had significantly higher BPRS total scores compared with patients with one admission (the comparison between patients with multiple admissions and no admission was marginally insignificant). In addition, patients with multiple admissions had significantly higher BPRS psychotic subscale scores, and were more likely to have moderate-severe problems on the HoNOS with hallucinations or delusions and less likely to have achieved remission of positive symptoms, compared with other patients at 3-month follow-up. It is worth noting that patients with affective psychosis were more likely to achieve remission at 3-month follow-up compared with patients with non-affective psychosis (92.3% vs 59.5%, p = 0.003). Of those patients who were followed up at 3 months, 12 (92.3%) of the 13 patients with multiple admissions displayed moderate-severe risks to self or others at baseline, or lack of remission at 3-month follow-up, or both, compared with 17 (43.6%) of 39 patients with one admission and five (31.3%) of 16 patients with no admission (p = 0.002). Although a greater proportion of patients with multiple admissions were non-compliant and had problems with substance misuse at 3-month follow-up compared with other patients, these associations were not statistically significant.
Clinical ratings of patients with no admission, one admission and multiple admissions during the initial 3-month treatment period, assessed at baseline (n = 71) and 3-month follow-up (n = 68)
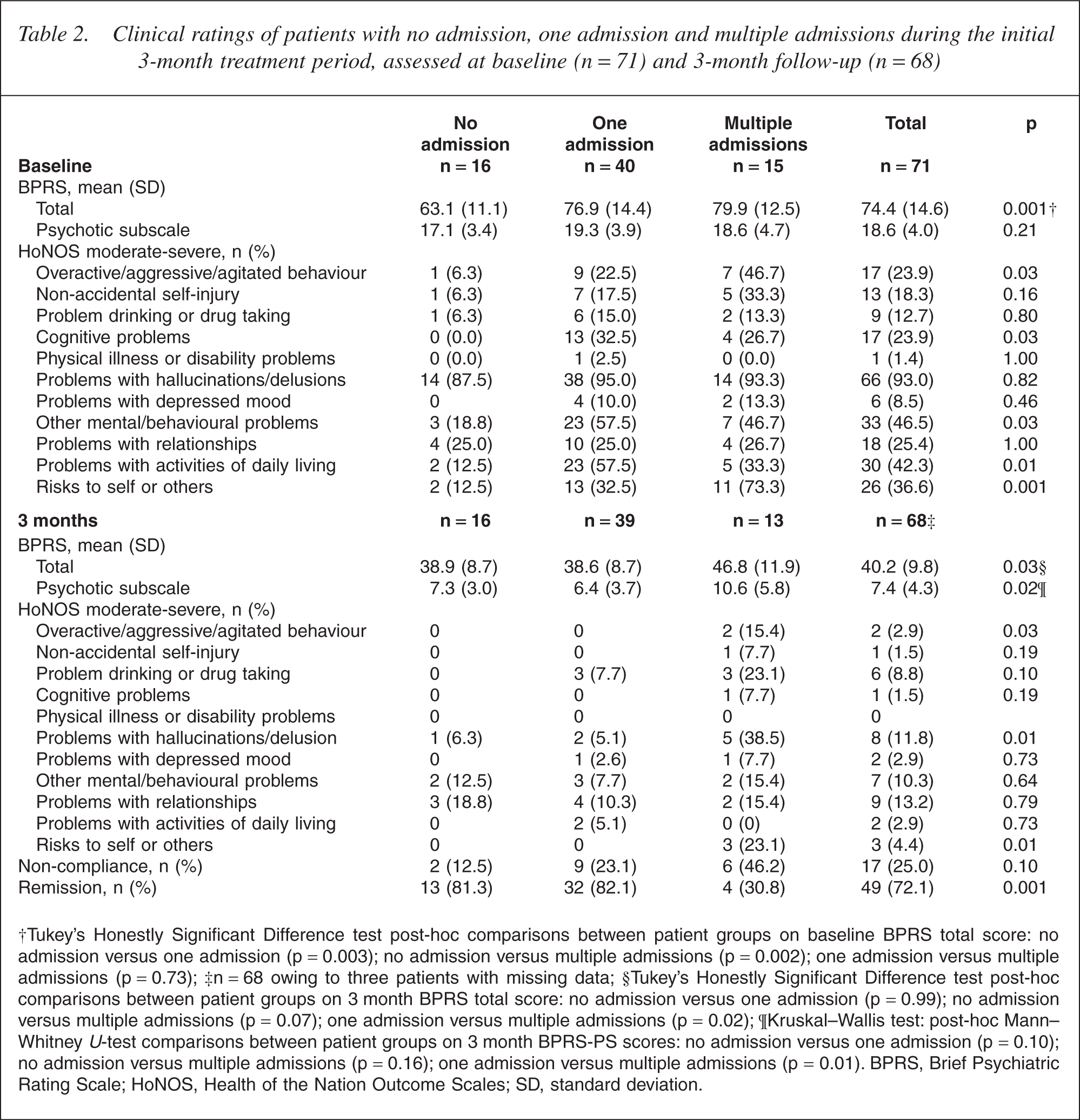
†Tukey's Honestly Significant Difference test post-hoc comparisons between patient groups on baseline BPRS total score: no admission versus one admission (p = 0.003); no admission versus multiple admissions (p = 0.002); one admission versus multiple admissions (p = 0.73); ‡n = 68 owing to three patients with missing data; §Tukey's Honestly Significant Difference test post-hoc comparisons between patient groups on 3 month BPRS total score: no admission versus one admission (p = 0.99); no admission versus multiple admissions (p = 0.07); one admission versus multiple admissions (p = 0.02); ¶Kruskal-Wallis test: post-hoc Mann-Whitney U-test comparisons between patient groups on 3 month BPRS-PS scores: no admission versus one admission (p = 0.10); no admission versus multiple admissions (p = 0.16); one admission versus multiple admissions (p = 0.01). BPRS, Brief Psychiatric Rating Scale; HoNOS, Health of the Nation Outcome Scales; SD, standard deviation.
Remission at 15-month follow-up for subsample of patients
Patients with multiple admissions were less likely to achieve remission of positive symptoms at 15-month follow-up (n = 8, 61.5%), compared with patients with no admission (n = 16, 100%) and patients with one admission (n = 37, 94.9%; p = 0.002). For remitted patients (n = 60, missing data for one patient who died during follow-up), the mean duration of remission (i.e. the period from the time that remission criteria were first met to psychotic relapse or the end of follow-up) was 363.7 days (median = 410.5, range = 70–529). Patients with affective psychosis were more likely to achieve remission at 15-month followup compared with patients with non-affective psychosis (96.2% vs 85.7%) although this was not statistically significant (p = 0.24).
Medication and non-compliance during 15-month follow-up for subsample of patients
More intensive biomedical treatment was investigated by examining the use of depot antipsychotic medication and clozapine during followup (n = 67, missing data for one patient who died during follow-up). Patients with multiple admissions were significantly more likely to be prescribed depot medication or clozapine (n = 5, 41.7%) compared with patients with no admission (n = 6, 15.4%) and one admission (n = 1, 6.3%; p = 0.04). Seven patients were prescribed depot medication: two patients with multiple admissions, four patients with one admission and one patient with no admission. Of these seven patients, one patient with multiple admissions was also prescribed clozapine. Five other patients were prescribed clozapine: three patients with multiple admissions and two patients with one admission. Rates of medication non-compliance during 15-month follow-up were similar for patients with no admission (n = 8, 50.0%), one admission (n = 20, 51.3%), and multiple admissions (n = 7, 53.8%; p = 0.98). Six of the seven patients prescribed depot medication were non-compliant.
Inpatient admission between 3-month and 15-month follow-up
A complete record of inpatient data for the 15-month follow-up period was available for 98 (94.2%) of the 104 patients. No significant between-group differences were found on the rate, pattern or total duration of inpatient admission between 3-month and 15-month followup (see Table 3).
Inpatient admission data between 3-month and 15-month follow-up for patients with no admission, one admission and multiple admissions during the initial 3-month treatment period (n = 98)
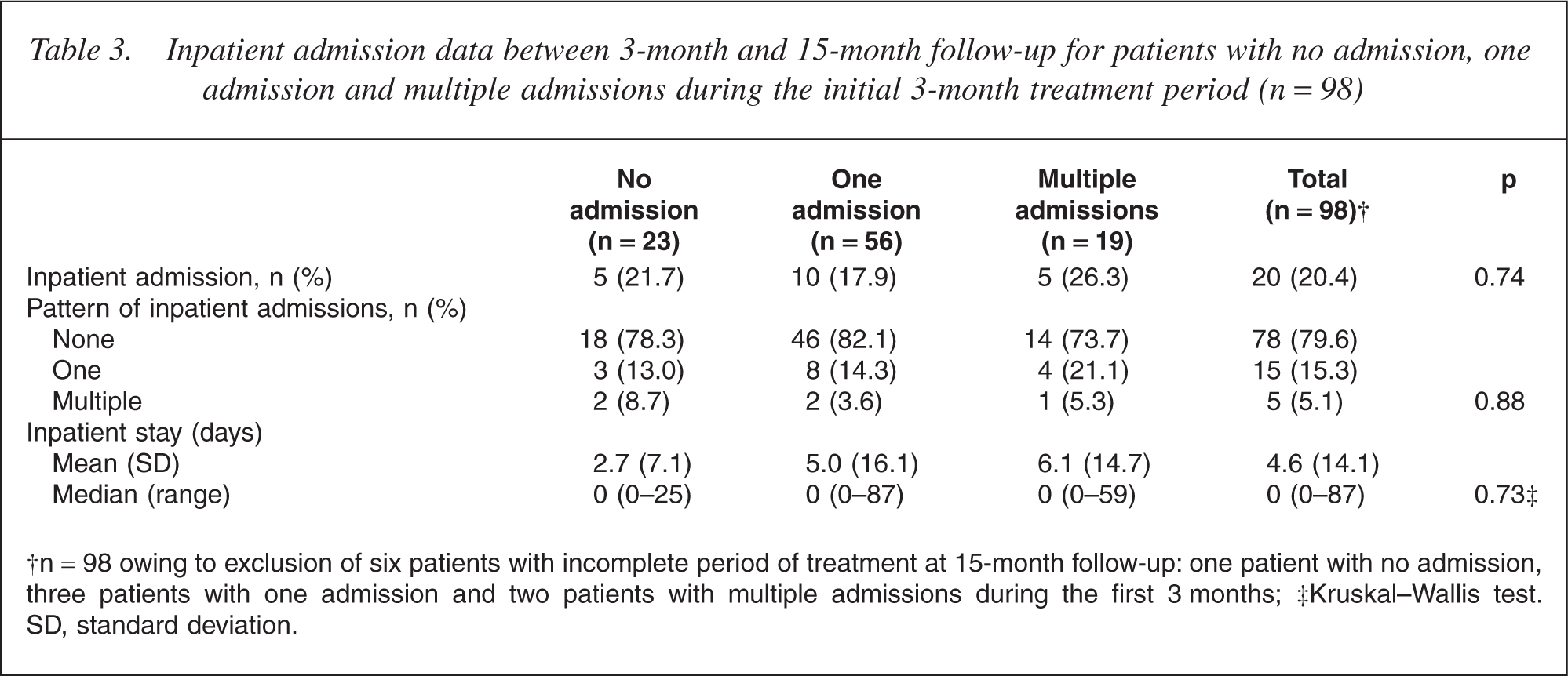
†n = 98 owing to exclusion of six patients with incomplete period of treatment at 15-month follow-up: one patient with no admission, three patients with one admission and two patients with multiple admissions during the first 3 months; ‡Kruskal-Wallis test. SD, standard deviation.
Discussion
The finding that 77% of patients with FEP were admitted to an inpatient unit confirms findings from previous studies that the majority of patients with FEP require inpatient admission at initial presentation [1–5]. The relatively high rates of inpatient admission are likely to be partly due to the need for conservative clinical management of novice and ‘unknown’ FEP patients who are a high-risk group for suicidal behaviour [15, 16]. The implication for mental health services is the requirement to develop environments, procedures and practices related to inpatient care that address the needs of these young patients [17].
The finding of an association between inpatient admission and affective (primarily manic) psychosis is similar to previous studies [1, 4, 5]. The acute onset and behavioural disturbance associated with manic psychosis often result in patients presenting in crisis, which make it dif-ficult to provide safe and effective treatment in the community. It is worth noting that the apparent association between shorter DUP and a single inpatient admission was likely to have been a reflection of the link between shorter DUP and affective psychosis. Consistent with other studies [4, 5], there was no difference in the severity of positive psychotic symptoms at initial presentation between hospitalized and community-treated patients. However, community-treated patients were less likely to be affected by cognitive, psychological and behavioural problems and problems with activities of daily living, and had less severe global psychopathology. In effect, the need for inpatient admission appears to be less dependent on the severity of psychotic symptoms per se than the presence of significant behavioural and functional disturbance that requires more intensive nursing and medical treatment available in hospital.
Although the severity of psychotic symptoms at initial presentation was not associated with inpatient admission, patients with multiple inpatient admissions were less likely to achieve remission of psychotic symptoms at 3-month follow-up compared with other patients. Further, patients with multiple admissions were more likely to demonstrate problems with risks to self or others during the initial treatment period. Both of these findings are consistent with clinical experience. Typically, patients are discharged from relatively brief inpatient admissions in an improved state but without full resolution of psychotic symptoms and with other extant problems. In this context, it seems likely that a minority of patients will require readmission soon after discharge from hospital owing to a lack of treatment response, the recurrence of risks to self or others, poor engagement with outpatient services, or some combination of these factors. Moreover, as the current findings suggest, substance misuse and medication non-compliance during the initial treatment period can often contribute to the difficulties that some patients have in maintaining community tenure [18]. More patients would be expected to meet criteria for problematic substance use if the ‘cut-point’ was less than moderate severity and/or if the period assessed was of a longer duration than 2 weeks.
The finding that multiple admissions predicted failure of remission at 15-month follow-up suggests that indicators of repeated and/or high inpatient service use during initial treatment for FEP may be a useful supplement to clinical data in the early detection of persistent positive symptoms [19]. Nevertheless, there were other findings that favour an optimistic outlook in the treatment of patients with multiple admissions during the initial treatment period. First, the rate of remission improved from 31% at 3-month follow-up to 62% at 15-month followup for these patients. Second, multiple admissions during the initial 3-month treatment period were not associated with greater use of inpatient services during the following 12-month period of treatment. These findings are likely to be at least partly due to the more intensive treatment these patients received including more frequent use of a CTO as well as depot medication and clozapine. Hence, it seems reasonable to conclude that sustained treatment can improve or stabilize the clinical recovery of these patients to the extent that the risk of continued ‘revolving-door’ hospitalizations [18] appears to be no higher for these patients compared with other patients.
The limitations of the current study included the relatively small sample size that may have limited the power to detect differences of clinical significance, the crosssectional ratings of clinical problems and the availability of clinical ratings for only a subsample of patients. Despite finding no differences between participants and non-participants in the follow-up study on most demographic and treatment variables, the participants were more likely to live with a family member and to be diagnosed with affective psychosis with shorter DUP. Hence, this subsample bias may have affected some results. For example, it is likely that the overall rate of remission at 3-month follow-up was inflated given that affective psychosis was associated with participation in the follow-up study as well as a higher rate of remission at 3 months. The strengths of the study were the collection of comprehensive information including inpatient data for a 15-month follow-up period for consecutive patients with FEP at a specialist treatment service, and the use of standardized assessment instruments to rate clinical symptoms and problems as well as remission of positive symptoms.