
Abstract
Gender differences in psychotic disorders have been noted since the time of Kraepelin [1]. The literature have suggested that men with schizophrenia had more severe negative symptoms [2–4], fewer affective symptoms [5–7], poorer premorbid adjustment, more malignant illness trajectory, inferior psychosocial functioning and worse treatment response than female counterparts [3,5,8–10]. Although previous studies consistently demonstrated that men with psychotic disorders had an earlier age of onset than women [11–13], some recent research showed contrary findings. These studies either found no such gender difference [4–5,10] or a younger age of onset in female patients [14–15]. Results of gender difference on duration of untreated psychosis (DUP) are inconsistent. Some researchers reported men having longer DUP than women [16–18] while others revealed opposite findings [6] or lack of difference between sexes [4–5,19].
Discrepancy in findings on gender differences might partly be explained by methodological variations among studies. The majority of these studies recruited participants from inpatient settings who had chronic illness. Few have evaluated gender differences across a wider spectrum of psychotic disorders at an early illness stage. Among those first-episode studies investigating gender differences, most, if not all, have been conducted in the Caucasian population. As gender effects on illness manifestation in early psychosis might be modified by complex interactions between biological and socio-cultural factors [20], whether these findings could be generalized to different ethno-cultural backgrounds has not been fully explored. Additionally, enhanced understanding of gender differences in psychotic disorders can facilitate development of gender-specific therapeutic strategies which have not been adequately addressed in current clinical practice. Therefore, we aimed to examine gender differences on pre-treatment characteristics, clinical presentation, service utilization and functional outcome over a three-year follow up period in a large representative cohort of patients presented with first-episode psychosis in Hong Kong. To the best of our knowledge, this study was the largest investigating gender differences in patients with first-onset psychosis in non-western countries.
Methods
Participants and setting
The initial sample comprised 839 patients who were consecutively enrolled in the EASY program (Early Assessment Service for Young People with Psychosis) from July 2001 to August 2003. Since 2001, this publicly funded specialized programme has been providing early assessment and phase-specific intervention for all individuals aged 15–25 years experiencing their first-episode psychosis in Hong Kong [21]. The programme consists of five treatment teams covering the whole territory of Hong Kong with population of approximately seven million and over 95% of the population is Han Chinese. The service adopts a case-management approach and assertively follows up patients for the first three years after their initial episodes (including follow up in a transitional step-down clinic in year three). Standardized clinical assessments evaluating symptom profiles and psychosocial functioning are performed for each patient. Multi-disciplinary case reviews are held regularly for close monitoring of each patient's diagnostic ascertainment, clinical progress and treatment outcome. Patients are discharged to general psychiatric service at the end of the EASY programme.
In this study we excluded patients who had mental retardation, psychotic disorders due to general medical condition or substance-induced psychosis. Individuals with more than one month of psychiatric treatment before presentation to the programme were not recruited. Patients with incomplete or missing medical files were also excluded. Of the initial cohort, 700 participants fulfilled the inclusion criteria and were retained as the study sample.
Data collection
Participants’ baseline and follow up variables were retrieved systematically according to the following standardized procedure. For each participant, outpatient and inpatient medical records as well as computerized clinical information from the medical database (Psychiatric Case Register) were retrieved. Trained research assistants acquired the data from medical files according to protocol designed specifically for data collection in the current study. Standardized data entry forms were used to systematically extract information on intake, treatment and follow up variables from consecutive medical files. Only data that could be reliably extracted from the records were targeted for retrieval and analysis. Follow up characteristics and outcome measures were determined for each month spanning the three-year follow up period following first contact to treatment.
Baseline data included socio-demographic characteristics, age and mode of onset of first psychotic episode and DUP which was defined as time interval between the onset of positive psychotic symptoms and the first contact to psychiatric service. Clinical variables consisted of number of relapses, history of suicidal attempt, substance abuse, violence and forensic records. Psychopathological evaluation included positive, negative and affective symptom levels determined individually according to scores on the Clinical Global Impression – Severity of Illness Scale (CGI-S). Treatment characteristics included number and length of psychiatric hospitalizations, service disengagement and use of second-generation antipsychotic (SGA) medications. Functional outcome was assessed by Social Occupational Functioning Assessment Scale (SOFAS) and vocational status.
Diagnostic assignment of individual participant was based on a longitudinal approach taking into consideration the fact that diagnostic change might take place over time [22]. In the EASY programme, diagnosis of each case was derived from consensus results of inter-disciplinary conference utilizing multiple sources of information, and regular diagnostic reviews were undertaken to incorporate additional clinical information emerged along the course of illness. In this study, the final three-year clinical diagnosis, which was based on ICD-10 criteria [23], was thus ascertained as participant's research diagnosis.
Weekly consensus meetings were held throughout the period of data collection to ensure strict adherence to protocol and to resolve ambiguity in clinical information during the data extraction process. Validity and inter-reliability for major variables including DUP, functional outcome and length of hospitalizations were evaluated based on 12 cases using the intra-class correlation coefficient (ICC). Validity compared ratings between an experienced psychiatrist and research staff (ranging from 0.78 to 1.0). Inter-rater reliability compared ratings between research staff (ranging from 0.7 to 1.0). Both validity and inter-rater reliability exercises yielded a satisfactory level of concordance.
The study was approved by the local research and ethics committee.
Statistical analysis
Gender effects on pre-treatment and baseline characteristics were examined by applying independent t-test, chi-square test and Mann-Whitney test, as appropriate. To assess gender differences on follow up and outcome measures, analysis of covariance and logistic regression analysis were carried out for dependent continuous variables and dependent categorical variables, respectively to control for potential confounding effects of baseline variables. All analyses of gender differences were performed for both the whole first-episode psychosis cohort and diagnostic group of schizophrenia or affective psychosis which included bipolar affective disorder and depression with psychotic features. The level of statistical significance for all analyses was set at p < 0.05.
Results
Seven hundred participants were included in the study and 51.4% (n = 360) were men. Schizophrenia was the most common diagnosis which accounted for 65.9% (n = 461, men n = 258, women n = 203) of the sample. For other diagnostic entities, 11.9% of the cohort had affective psychosis (bipolar affective disorder n = 54, depression with psychotic features n = 29), 3.9% had schizoaffective disorder (n = 27), 12.4% had acute and transient psychotic disorders (n = 87) and 6.6% had unspecified non-organic psychosis (n = 46).
Gender differences in the first-episode psychosis cohort
Concerning baseline characteristics, men with first-episode psychosis had lower educational attainment (t = −3.4, df = 696, p < 0.01), longer median DUP (Z = −3.8, p < 0.001), more prominent negative symptoms (CGI-S score, t = 2.6, df = 698, p = 0.01), less affective symptoms (CGI-S score, t = −2.8, df = 698, p < 0.01) and fewer past suicidal attempts (χ2 = 10.6, p < 0.01) than female counterparts (Table 1). Women were more likely than men to receive SGA (χ2 = 4.7, p < 0.05) and for a longer period of time (t = −2.4, df = 698, p < 0.05) over three years. A higher proportion of male patients had substance abuse (Wald z = 10.9, p < 0.01), violence (Wald z = 11.0, p < 0.01) and forensic records (Wald z = 5.2, p < 0.05) after treatment (Table 2). At follow up, men exhibited more severe negative symptoms (F = 20.3, p < 0.001) but lower level of affective symptoms (F = 5.4, p < 0.05), as measured by CGI-S, than women. Women had better psychosocial functioning than men (SOFAS score, F = 19.3, p < 0.001), and more women than men engaged in stable full-time employment or study for 12 consecutive months or longer during three-year follow up period (Wald z = 13.1, p < 0.001) (Table 3).
Baseline characteristics in men and women with first-episode psychosis
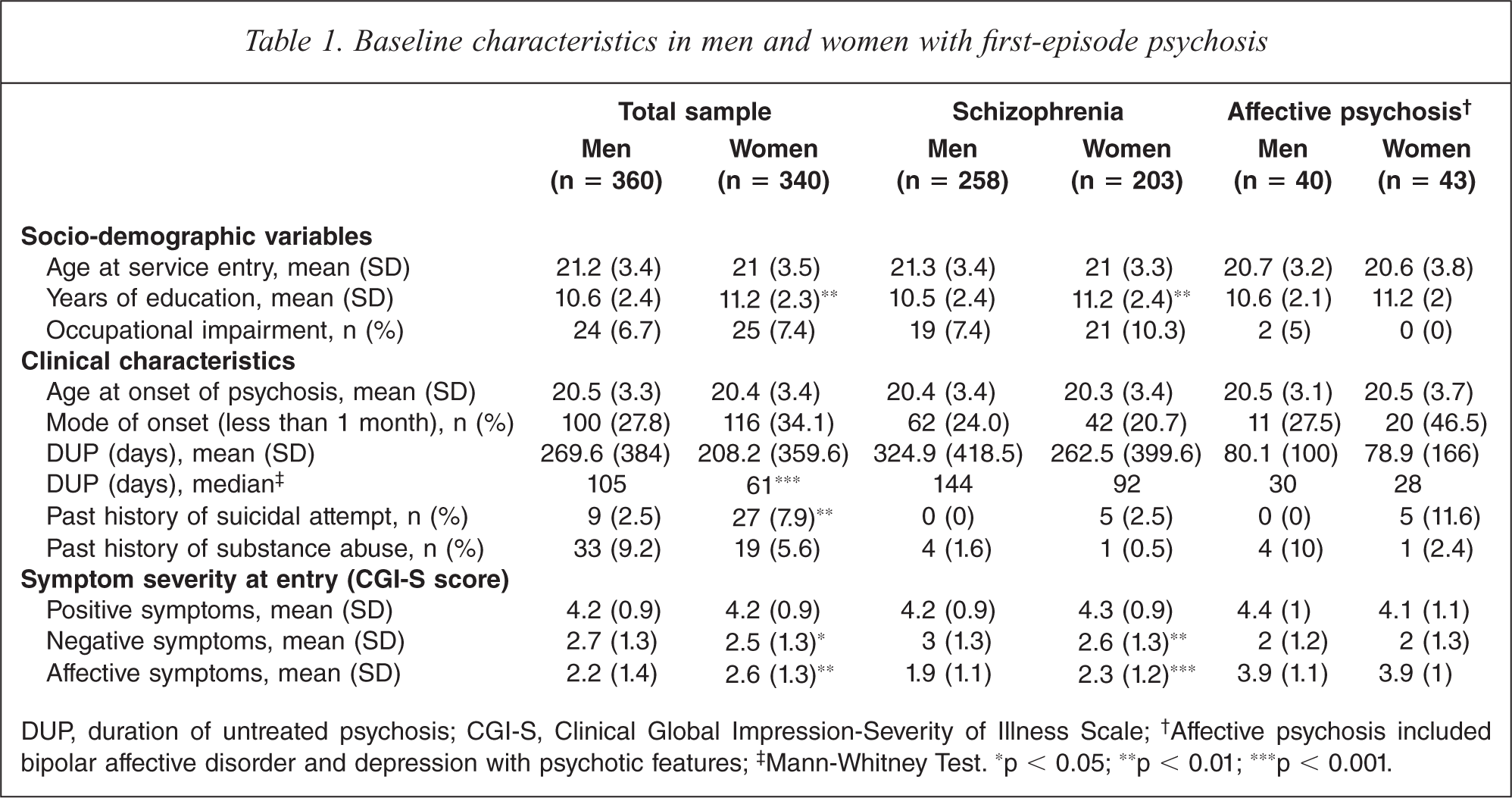
DUP, duration of untreated psychosis; CGI-S, Clinical Global Impression-Severity of Illness Scale;† Affective psychosis included bipolar affective disorder and depression with psychotic features;‡ Mann-Whitney Test. ∗p < 0.05; ∗∗p < 0.01; ∗∗∗p < 0.001.
Treatment characteristics and risk behaviour in men and women with first-episode psychosis in follow up period
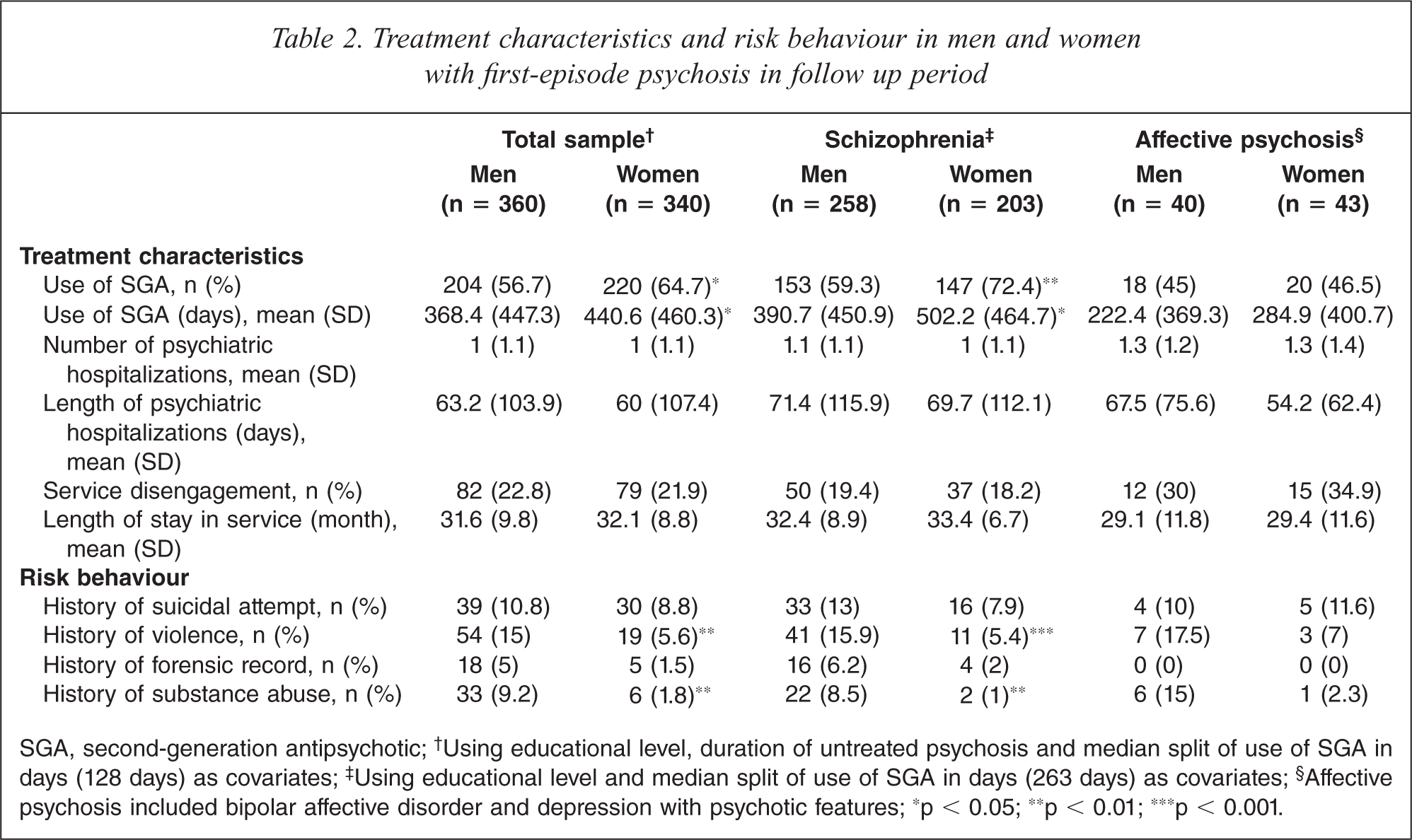
SGA, second-generation antipsychotic;† Using educational level, duration of untreated psychosis and median split of use of SGA in days (128 days) as covariates;‡ Using educational level and median split of use of SGA in days (263 days) as covariates;§ Affective psychosis included bipolar affective disorder and depression with psychotic features; ∗p < 0.05; ∗∗p < 0.01; ∗∗∗p < 0.001.
Clinical variables and functional outcome in men and women with first-episode psychosis in follow up period
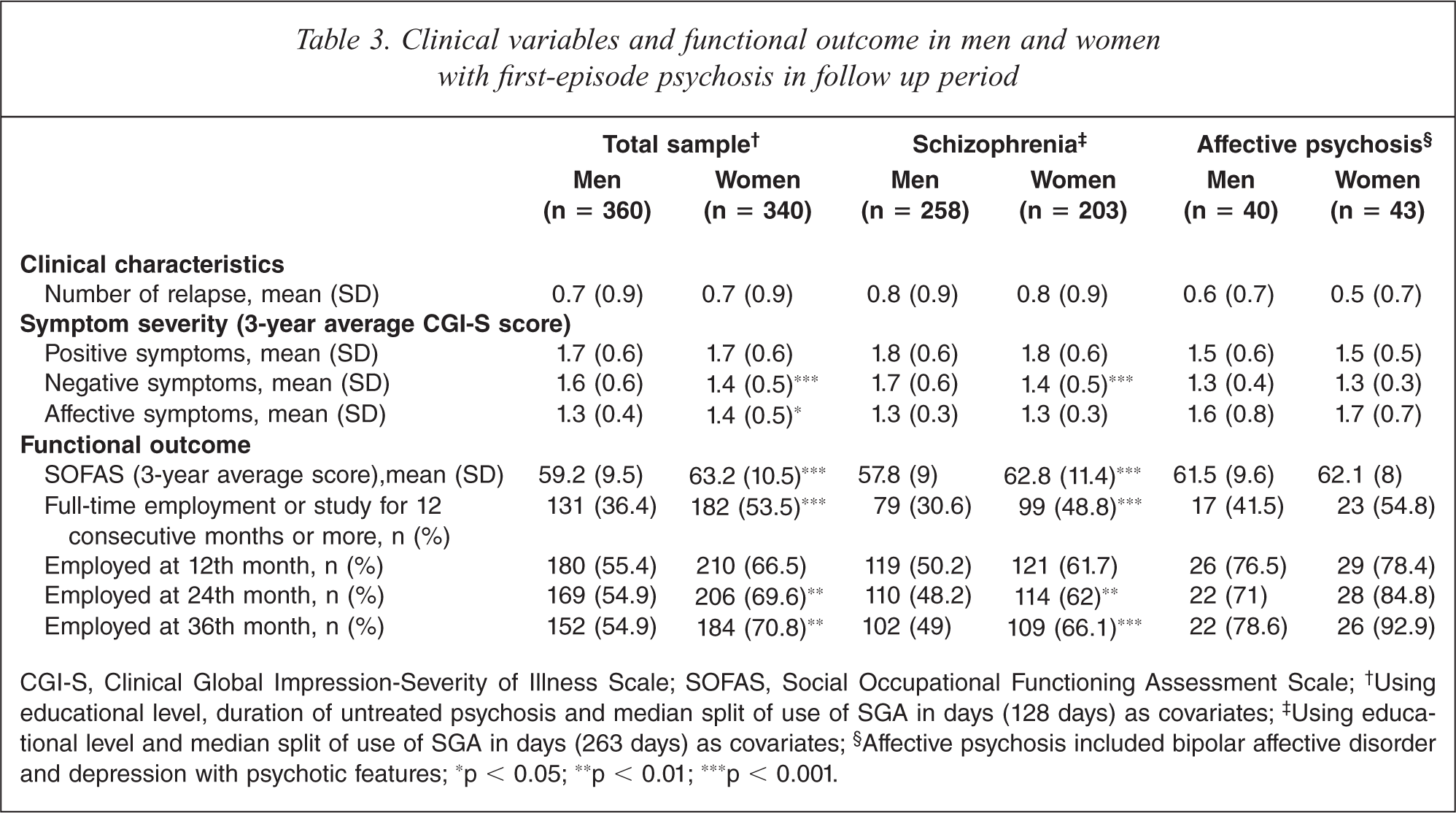
CGI-S, Clinical Global Impression-Severity of Illness Scale; SOFAS, Social Occupational Functioning Assessment Scale;† Using educational level, duration of untreated psychosis and median split of use of SGA in days (128 days) as covariates;‡ Using educational level and median split of use of SGA in days (263 days) as covariates;§ Affective psychosis included bipolar affective disorder and depression with psychotic features; ∗p < 0.05; ∗∗p < 0.01; ∗∗∗p < 0.001.
Gender differences in schizophrenia and affective psychosis
Similar gender differences were demonstrated in patients presented with first-onset schizophrenia in comparison with the whole first-episode psychosis cohort. Women achieved higher level of education (t = −2.9, df = 457, p < 0.01), were more likely to receive SGA (χ2 = 8.6, p < 0.01) and for longer duration (t = −2.6, df = 459, p < 0.05), experienced less severe negative symptomatology both at entry (t = 2.7, df = 459, p < 0.05) and during follow up (F = 20.2, p < 0.001), exhibited more florid affective symptoms at baseline (t = −3.5, df = 459, p < 0.001), committed less violent acts (Wald z = 8.3, p < 0.05), were less likely to have post-treatment substance abuse (Wald z = 13.1, p < 0.01) and had more favourable functional outcome than men (SOFAS score: F = 23.4, p < 0.001; full-time employment or study for at least 12 consecutive months: Wald z = 10.6, p < 0.01). Men with schizophrenia had longer median DUP than women though it did not reach statistical significance (Z = −1.8, p = 0.07) (Tables 1, 2 and 3).
Patients with affective psychosis showed no significant gender differences in baseline characteristics, service utilization, risk behaviours, symptom severity and functional outcome. Post-treatment substance abuse was more frequently seen in men than in women (χ2 = 4.3, p = 0.05) (Tables 1, 2 and 3).
Discussion
Our study demonstrated significant gender differences in illness manifestations and functional outcome in a large cohort of Chinese young patients presenting with first-episode psychosis. Briefly, we found that: (i) men exhibited more prominent negative symptoms but less affective symptoms than women; (ii) there was no gender difference in age at onset of psychosis but men had significantly longer DUP than women; (iii) women achieved better pre-treatment educational attainment and superior psychosocial functioning during the initial three years of psychiatric treatment.
Differences between men and women with psychosis with respect to clinical presentation have been consistently shown by the literature. Our study replicated previously reported data that male gender was associated with more severe negative symptomatology [2–4]. Consistent with past studies, our results showed that women had more mood symptoms than men [5–7]. It has been posited that higher propensity to affective symptoms, particularly depression in women with psychosis might be attributed to their lower self-esteem [4] and their tendency to internalize emotions [7]. In line with previous research we found that a higher proportion of male patients had substance abuse, violence and criminal records [5–7]. Overall, our findings of gender effects on psychopathology and risk behaviours echoed results of published literature and it is suggested that distinctive clinical profiles between sexes may partly reflect an overlay of gender differences in normal population [24].
Numerous studies have reported that men with psychotic disorders had an earlier age of onset than women [11–13]. However, in agreement with some recent large-scale first-episode studies [4–5,10], we failed to replicate this finding and revealed no such gender difference in either the whole first-episode psychosis cohort or schizophrenia. Discrepancies among studies might firstly be due to varying definitions of illness onset which has been operationalized as age at first admission, first contact to service, emergence of first positive symptom or first noticeable sign of the disorder [10,13]. Secondly, literature showed that men and women with psychosis exhibited different age of onset distribution. A single peak age of onset lying from late teens to early 20s has been demonstrated in male patients. While apart from a period of late adolescence to early adulthood, women were found to have two smaller peaks of age of onset lying above 40 and 65 years of age [3,11]. In this context, biased interpretation on gender differences in illness onset might be introduced by comparing mean values of age of onset between sexes across a broad age range. Thirdly, we recruited young people presenting with first-episode psychosis aged 15 to 25 years, thus excluding patients with older age of onset, which is more commonly seen in women [25]. A later mean age of onset in women might be obtained if a wider age range were studied.
The literature showed mixed results in gender differences on DUP. Some researchers observed no significant difference on DUP between sexes [4–5,19], while others suggested that female patients had longer DUP [6]. Our results, on the other hand, were in accord with some other studies which indicated that men with first-episode psychosis had longer DUP than women [16–18]. Consistent with several past studies, we did not observe significant gender difference on DUP in patients having schizophrenia [4–5,26], although a tendency that men had longer DUP (p = 0.068) was noted. It is suggested that earlier help-seeking behaviour in women with psychosis might be attributed to their more prominent affective symptoms and better insight to illness experience [5]. Conversely, it might be more difficult to recognize negative symptoms such as avolition and flat affect, being more frequently associated with men having psychosis, as illness manifestations, thereby causing treatment delay and prolonged DUP [27]. Additionally, inadequate mental health literacy and negative attitudes towards mental illness may impede help-seeking and early detection. In Hong Kong, male secondary school students (aged 14–21 years) were found to have a more stereotyping, restrictive and stigmatizing attitudes towards mental illness [28]. A recent study demonstrated that young men had poorer mental health literacy with respect to psychosis and were significantly less likely to value health professional assistance than women [29]. It is plausible that lower level of awareness and more negative views of young men towards psychosis might partly contribute to their treatment delay. Nonetheless, whether and to what extent the findings on mental health literacy could be applied to our population and its potential impact on delayed recognition and treatment of psychosis remained to be further explored.
Consistent with several first-episode studies conducted in western countries [4–5,30], we found that female patients had higher level of pre-treatment educational attainment and achieved better psychosocial functioning than male counterparts. Gender differences in functional outcome of psychosis have been attributed to various factors including more prevalent concomitant substance abuse, more severe negative symptoms, worse premorbid adjustment and poorer treatment response in men. Some researchers proposed that worse social functioning in men were associated with their younger age of onset and earlier disruptions in their academic and vocational developments [26]. Our findings indicated that poorer functional outcome in men could not be explained by gender difference in age of onset as we found no such difference between sexes in our sample. On the other hand, many studies suggested that female patients might be less vulnerable than men to certain cognitive impairments such as verbal processing and executive functions [31–33]. Women with psychosis were also shown to have better emotional processing capacity [34,35]. Better preservation of social cognitive competence and neuropsychological functions may therefore contribute, in part, to less psychosocial disability in women compared to men with psychosis. Given that male gender has been repeatedly demonstrated to be more frequently associated with poorer premorbid adjustment, more prominent negative symptoms, greater cognitive impairment, more structural brain abnormalities [36–38] and worse psychosocial functioning, it is thus hypothesized that men may be liable to a neurodevelopmental subtype of psychotic disorders with greater severity and poorer prognosis [39]. In fact, male gender was found to be predictive of continuous illness course at five-year follow up with less favourable functional outcome than women [40].
There are several limitations in the study. First, the study was based on medical file review which may be biased by varying degree of documentation quality. As clinical progress of each individual enrolled in this specialized early intervention service was closely monitored and all available sources of information would be ascertained via multi-disciplinary input, possibility of missing relevant clinical data for case notes documentation and diagnostic formulation was thus minimized. Moreover, errors in data extraction might be further reduced via close scrutiny of data acquisition and rating processes by regular consensus meetings. Second, as we only focused on variables that could be reliably retrieved from medical records, some other potentially important outcome variables (such as quality of life) could not be addressed in this study. Third, as the length of follow up was three years only, a longer study period is required to clarify an inconsistent finding of attenuated gender differences in long-term outcome [41,42].
In conclusion, in a large and clinically homogeneous cohort of Chinese young patients experiencing first-episode psychosis, we demonstrated that gender differences in clinical presentation and functional outcome were evident in the early illness phase. Clinically, differential needs between men and women with psychosis and therefore gender-specific therapeutic strategies should be considered in early intervention service. In addition, because of potentially different pharmacological sensitivity between sexes [43,44] and an under-representation of women in previous clinical trials [45], more research should be conducted to investigate gender differences on treatment efficacy and side-effect profiles.
Footnotes
Acknowledgements
The authors would like to thank all coordinating clinicians and staff from the participating hospitals, clinics and medical records departments for their kind assistance.