
Abstract
beyondblue: the national depression initiative was established initially by the Commonwealth and Victorian State governments to promote awareness and an effective response to depression in the community [1]. In its first term (2001–2005), beyondblue has undertaken a wide range and volume of educational and promotional activities [2], which have resulted in high levels of achievement across a number of areas [3]. Fundamental to the work of beyondblue has been the establishment of key partnerships with the media to provide not only accurate clinical information, but to publicly convey the lived experience of consumers [4] and carers [5] who live with depression. beyondblue's active promotion and advocacy of these issues has also been facilitated through the formation of ‘blueVoices’, a national consumer and carer component of the organization created to give voice to the needs and experiences of those living with depression in Australia.
There is growing evidence to suggest that over the last decade mental health literacy, and depression literacy specifically, has increased in Australia [6]. Independent reports have suggested that it is possible that Australia's national initiative, beyondblue, is contributing to this increase [7]. Importantly, rapidly increasing access to depression treatments may also be playing a significant role [8]. However, it is not yet clear whether the degree of exposure to public awareness campaigns is associated directly with depression awareness or the extent to which other sociodemographic or personal or family experiences mediate such effects.
Method
A telephone survey of 3200 respondents was conducted between 18 November and 20 December 2004 and between 12 January and 13 February 2005. Respondents were randomly selected across all Australian States and Territories using Electronic White Pages (Marketing Pro 2.11, October 2000). Stratification ensured that the sample was representative of the normal population in terms of age, gender, and location across metropolitan and non-metropolitan areas by selecting respondents to match the Australian Bureau of Statistics records for age, sex and geographic location in 2001. The survey was based on an initial instrument used in 2001 and 2002 [9], and consisted of 37 core questions that were asked of all respondents. In addition to these core questions, there were 10 additional sets of questions that were randomly asked of four subsets of respondents (n=800). When introducing the survey, respondents were told that the survey was about the general health and wellbeing of the Australian community, with no indication of the specific topic of interest (depression) nor the organization who had commissioned the research (beyondblue: the national depression initiative).
The core survey was designed to measure four specific aspects of depression literacy: awareness, knowledge, attitudes and behaviours in the Australian adult (18 years and over) population. The present paper will focus on those questions specifically relating to depression awareness in the context of health andmental health problems (two items), together with prevalence rates (one item) and the debilitating nature of the illness (one item). Exposure to depression-related information (personal stories, TV programs/movies or famous people living with depression or general media; four items) was also assessed, together with direct personal experience with depression (self and/or family member; one item) and other relevant demographic and geographic variables (five items) including education/training in the health and mental health fields (two items).
Results
Telephone interview
In obtaining the final sample size of 3200 respondents, there were 9889 refusals. No contact could be made for 8503 dialled numbers (due to the number being an answer phone/fax machine, engaged, out of service or no answer) and 1283 numbers were out of scope for this survey (i.e. a suitable respondent not available, for example, out of quota; under age; business number; language difficulties). Call-backs were made five times before an interviewer ceased dialling a particular phone number. In total 384 call-back interviews were conducted.
Demographics
The 3200 interviews were equally distributed with 400 interviews being conducted across each Australian State and Territory, with more interviews conducted across metropolitan areas (69.1%, n=2212/3200). The sample consisted of 47.1% males (n=1506) and 52.9% females (n=1694) with a mean age of 45.8 years (range=18–99 years, SD=16.8). Most respondents (65.4%, n=2089/3193) indicated that either they themselves or someone in their family had experienced depression, of whom 18.7% (391/2089) reported that they themselves had experienced depression as opposed to a family member (47.6%, 994/2089). Just over one-fifth of the sample (21.7%, n=694/3199) indicated that they had professional training in a health field, with 8.8% (280/3199) reporting to have had training specifically in the area of mental health.
Exposure to depression in the media
Overall, there were relatively high levels of exposure to depressionrelated information and organizations across the sample (Table 1) with a substantial proportion of respondents indicating that they had been exposed to information surrounding depression via the various forms of media/literature and specifically within the past 12months. Furthermore, there was high recognition (spontaneous and prompted) of organizations associated with depression, in particular beyondblue. In accordance with respondents' recall of beyondblue, levels of awareness were categorized in terms of high (spontaneous/unprompted), medium (prompted), low(further prompting) and no levels of recognition. Of the 1329 who believed they knew of organizations associated with depression, the most common organizations to be spontaneously mentioned were beyondblue (22.2%, 709/3200); the Black Dog Institute (0.8%, 25/3200) and ‘other’ (14.0%, 448/3200).
Reported exposure to depression-related information and organizations associated with depression
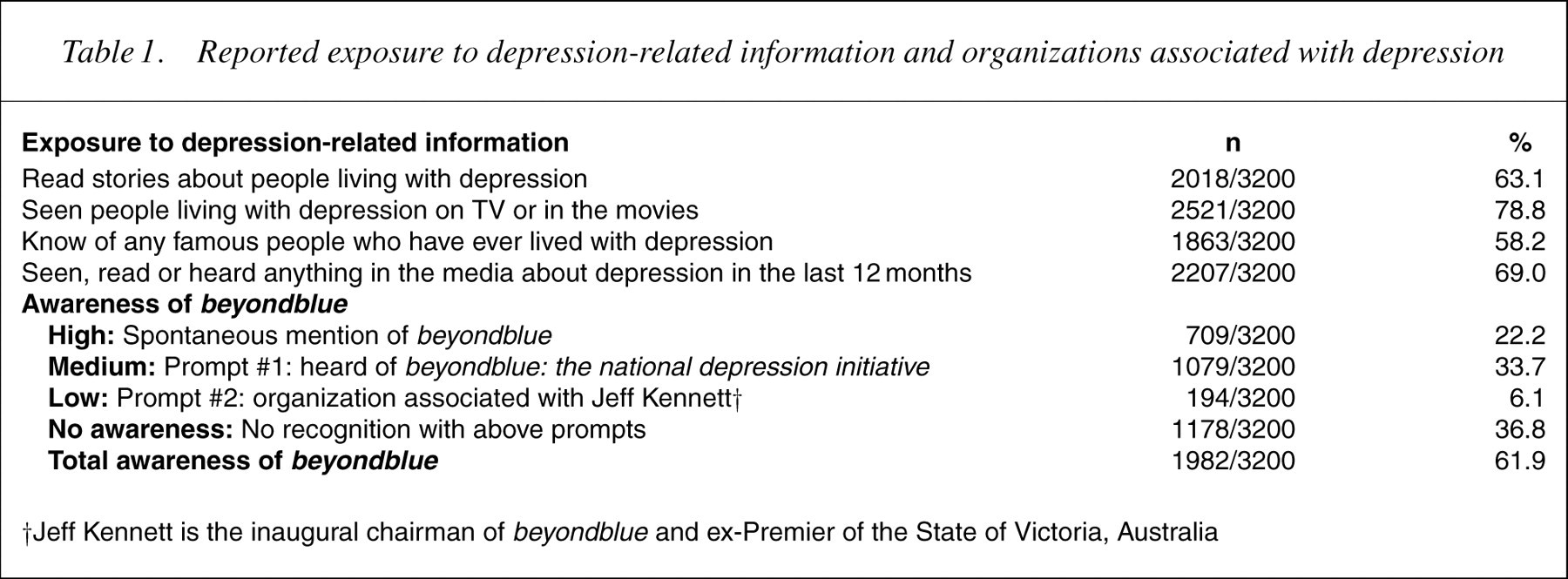
†Jeff Kennett is the inaugural chairman of beyondblue and ex-Premier of the State of Victoria, Australia
The associations between demographics, and exposure to depressionrelated information/organizations on depression awareness were assessed across the community sample.
Recognition of depression in the context of mental health
When asked to identify the major mental health problems inAustralia, just under half of all responses provided (up to four recorded per respondent; 45.4% or 1538 out of 3386 responses) spontaneously identified depression. Awareness of depression as a major mental health issue was associated with higher (tertiary) education (χ2 =88.06, df=2, p<0.001) and having trained in health (χ2 =8.21, df=1, p=0.004) or mental health (χ2 =16.67, df=1, p<0.001). Respondents with direct experience with depression (self/family member) were more likely to mention depression within this mental health context (χ2 =52.03, df=1, p<0.001). Alternatively, depression awareness was lower among males (χ2 =66.23, df=1, p<0.001) and among older respondents, particularly those aged 65 years and over (χ2 =119.78, df=5, p<0.001). Awareness also varied across geographical areas with higher spontaneous awareness of depression across various states and territories (Australian Capital Territory: 57.1%, n=225/394; Tasmania: 50.8%, 200/394; Northern Territory: 50.6%, 200/395; and Victoria: 50.0%, 198/396; χ2 =19.94, df=7, p=0.006) and acrossmetropolitan areas (χ2 =9.95, df=1, p=0.002).
Exposure to information on depression and to organizationswas associated with greater recognition of depression as amental health problem across all items. In particular, there was greater spontaneous awareness among those who had seen, read or heard information in the media (χ2 =112.00, df=1, p<0.001), read stories about people living with depression (χ2 =26.79, df=1, p<0.001), seen people with depression shown on TV or in themovies (χ2 =38.78, df=1, p<0.001), or knew of any famous people living with depression (χ2 =95.17, df=1, p<0.001). Awareness of depression within a mental health context was also higher for those more familiar with beyondblue (χ2 =51.56, df=1, p<0.001).
Spontaneous recognition of depression as a health problem
When asked to identify the major health problems in Australia, depression was unlikely to be spontaneously mentioned with only 1.3% (n=47/3720; up to four responses were recorded for each participant) of all responses including depression. Because this represented such a small proportion of respondents with spontaneous recognition of depression as a major problem in terms of general health, associations with demographics and media exposure were not explored.
Awareness of depression prevalence
When asked to rate on a four-point scale the likelihood that a person will experience depression at some point in their adult lifetime (ranging from 1 in 50 to 1 in 5), most respondents (57.1%, n=1827/3198) underestimated, or did not know (2.9%, 92) prevalence rates. This was particularly the case for older respondents (χ2 =145.55, df=5, p<0.001) with those aged 65 years and over more likely to perceive depression to affect ‘1 in 50’ (25.0%, n=136/545) or ‘1 in 20’ (25.9%, 141/545) as opposed to ‘1 in 5’ (19.4%, 106/545). More accurate estimations were given by those with higher education (χ2 =23.38, df=2, p<0.001) and with training in health (χ2 =14.97, df=1, p<0.001) or mental health (χ2 =32.37, df=1, p<0.001). Having a personal experience with depression at some time (χ2 =151.37, df=4, p<0.001) was also associated with the higher, more accurate estimations of depression prevalence, while there were no observed differences across geographical areas or between genders.
Accurate estimations of prevalence rates were associated with all assessed dimensions of exposure to depression-related information. In particular, estimates were more accurate for those who had higher levels of awareness of depression in the media recently (χ2 =47.54, df=1, p<0.001), had read stories about people living with depression (χ2 =13.69, df=1, p<0.001), were aware of famous people living with depression (χ2 =109.64, df=1, p<0.001) and had seen people with depression shown on TV or in the movies (χ2 =19.17, df=1, p<0.001). Finally as awareness of beyondblue was seen to increase, so too was the proportion of respondents who correctly estimated the prevalence of depression (χ2 =15.77, df=1, p<0.001).
Debilitating nature of depression
Despite low recognition in a general health (as opposed to mental health) context, the debilitating nature of depression compared with other specified health problems (namely diabetes, asthma, arthritis, alcohol abuse) was recognized. 47.4% (n=1480/3123) of respondents rated depression to be the most debilitating of these conditions, with a further 26.0% (803/3092) rating it as the second most debilitating condition. The following groups were more likely to assign depression as the most debilitating condition: females (χ2 =11.27, df=1, p=0.001), those with higher education levels (partially or completed high school or greater) (χ2 =21.84, df=2, p<0.001) and those with personal experience with depression (χ2 =23.51, df=1, p<0.001). Older respondents (aged 65 years and over) were less likely to assign highest ratings of disability to depression (30.7%, n=161/524) when compared with younger age groups (e.g. 18–24 years olds, 51.1%, [184/360]; χ2 =92.19, df=5, p <0.001), as were those in non-metropolitan areas (χ2 =12.40, df=1, p<0.001). Ratings of disability associated with depression did not differ across states or territories or according to training in health or mental health.
The potential role of the media in conveying the debilitating nature of depression was also indicated. The highest rating of debilitation was assigned to depression more frequently among those respondents who had seen, heard or read information about depression in themedia in the past 12 months (χ2 =20.09, df=1, p<0.001), seen people living with depression on TV/movies (χ2 =11.66, df=1, p=0.001) and knew of famous people who had lived with depression (χ2 =30.49, df=1, p<0.001). Finally, those with highest awareness of beyondblue were also likely to rate depression as the most debilitating condition (56.2%, n=388/691) as compared with those with no awareness of beyondblue(45.5%, n=275/605; [χ2 =14.77, df=1, p<0.001]).
Discussion
The current findings reveal the strong presence and recognition of depression-related activity in the Australian community, including the role played by beyondblue: the national depression initiative. Furthermore, the high level of association between reported exposure to these activities and depression awareness is consistent with the view that such public activities and initiatives are of great potential value to the Australian community [2,3].
It appears that depression is being increasingly recognized as the major mental health problem in Australia, with the percentage of persons reporting this perception having increased from 39% in 2002 [9] to 45.4% in the current study. Similarly, the proportion of people reporting that they or someone close to them has experienced depression has increased from 58% to 65.4% and the proportion who under-reported the true prevalence had dropped from 64% to 57.1% [9]. Importantly, and consistent with our 2002 results, the majority of people continue to rank depression to be the most debilitating when compared with arthritis, asthma and diabetes (and alcohol abuse in the current study).
The community reports high levels of exposure to the personal experiences of others who live with depression. The strong associations between these levels of exposure and recognition of depression support the key role for the active portrayal of the lived experience of persons with depression. This provides a strong empirical basis for the establishment and ongoing promotion of blueVoices, the national consumer and carer organization supported by beyondblue. It will continue to publicize and advocate the needs and experiences of those living with depression across Australia [2–4,7].
These cross-sectional analyses have obvious limitations, particularly when one seeks to infer direct relationships between the specific activities of beyondblue and changes in depression awareness. Further, they highlight the extent to which such public health messages are likely to initially reach some particular audiences, notably younger persons, females, those with higher educational achievement and those residing in metropolitan areas. Further, we have not yet managed to position depression (and other mental health issues) within the broader context of major general health priorities.
In conclusion, since 2002 beyondblue has been highly active in key areas of public activity, depression research and service reform [3]. The pattern of associations in the present study suggests the likely value of continuing current activities (including portrayal of the lived experience). In turn these elevated levels of awareness of depression and beyondblue may lead to improved community attitudes and increased relevant health behaviours such as active pursuit of information or effective preventative or treatment strategies.