
Abstract
Over the past 25 years, a remarkable change has occurred in Australia, whereby the public have become much more like psychiatrists in their thinking. This is seen both in the everyday use of psychiatric concepts and in beliefs about appropriate treatment. This article examines evidence for this change, discusses what might have produced it, asks whether it has benefited the mental health of Australians and considers what further changes in thinking might be needed.
Evidence for the change
In the mid-1990s, some colleagues and I became interested in what knowledge the Australian public had about mental disorders and how they could use this knowledge to benefit their own mental health or that of others. As a first step to understanding what the public knew and believed, we carried out a National Survey of Mental Health Literacy in 1995 (Jorm et al., 1997b). When we saw the results, it appeared that public thinking about mental disorders might be very different from that of mental health professionals. To confirm that this was the case, in 1996 we carried out similar surveys of national samples of general practitioners (GPs), psychiatrists and clinical psychologists using some of the same survey questions (Jorm et al., 1997a). As expected, we found some major gaps between public and professional thinking, with the public much less likely to use psychiatric terms to describe mental health problems and much less positive about the benefits of seeing psychiatrists and other mental health professionals and of receiving standard psychiatric treatments. These findings underscored the need for interventions to improve the mental health literacy of the public and to close the gap with psychiatrists and other professionals.
To monitor whether there had been changes over time, we carried out further national surveys of the public in 2003–2004 and 2011, and another survey of professionals in 2012. These showed that major changes had occurred in public thinking over a period of 16 years and that the gap between the public and professionals had reduced considerably (Morgan et al., 2013; Reavley and Jorm, 2012). A few illustrative findings comparing the public with psychiatrists are shown in Figures 1–3. Figure 1 shows the labels that respondents gave when shown a vignette illustrating a person with major depression and asked what was wrong with that person. In 1995–1996, the public were much less likely than psychiatrists to label the person as ‘depressed’, but by 2011–2012 the gap had narrowed considerably. Figure 2 shows the percentage of respondents who thought that it would be helpful for the person in the vignette to see a psychiatrist, and Figure 3 shows the percentage who thought that an antidepressant would be helpful. In both cases, the public became more like psychiatrists in their beliefs about these interventions. Similar changes in thinking were found across a wide range of interventions, with the public also becoming more similar in their thinking to other mental health professionals, as well as to psychiatrists. Similar changes were also found when a vignette illustrating a person with schizophrenia/psychosis was used.
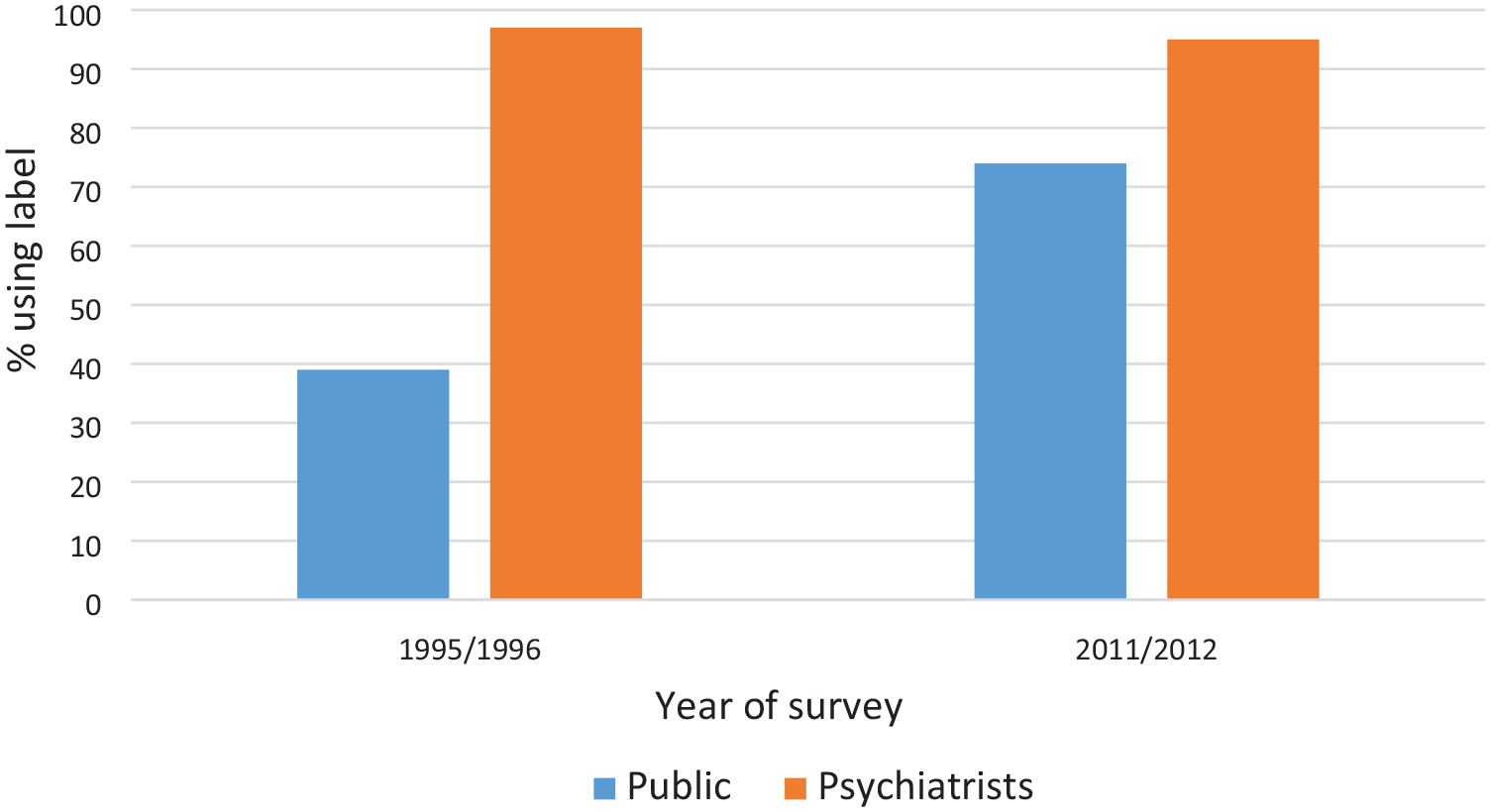
Percentage of the public and psychiatrists labelling a person in a vignette as experiencing depression.
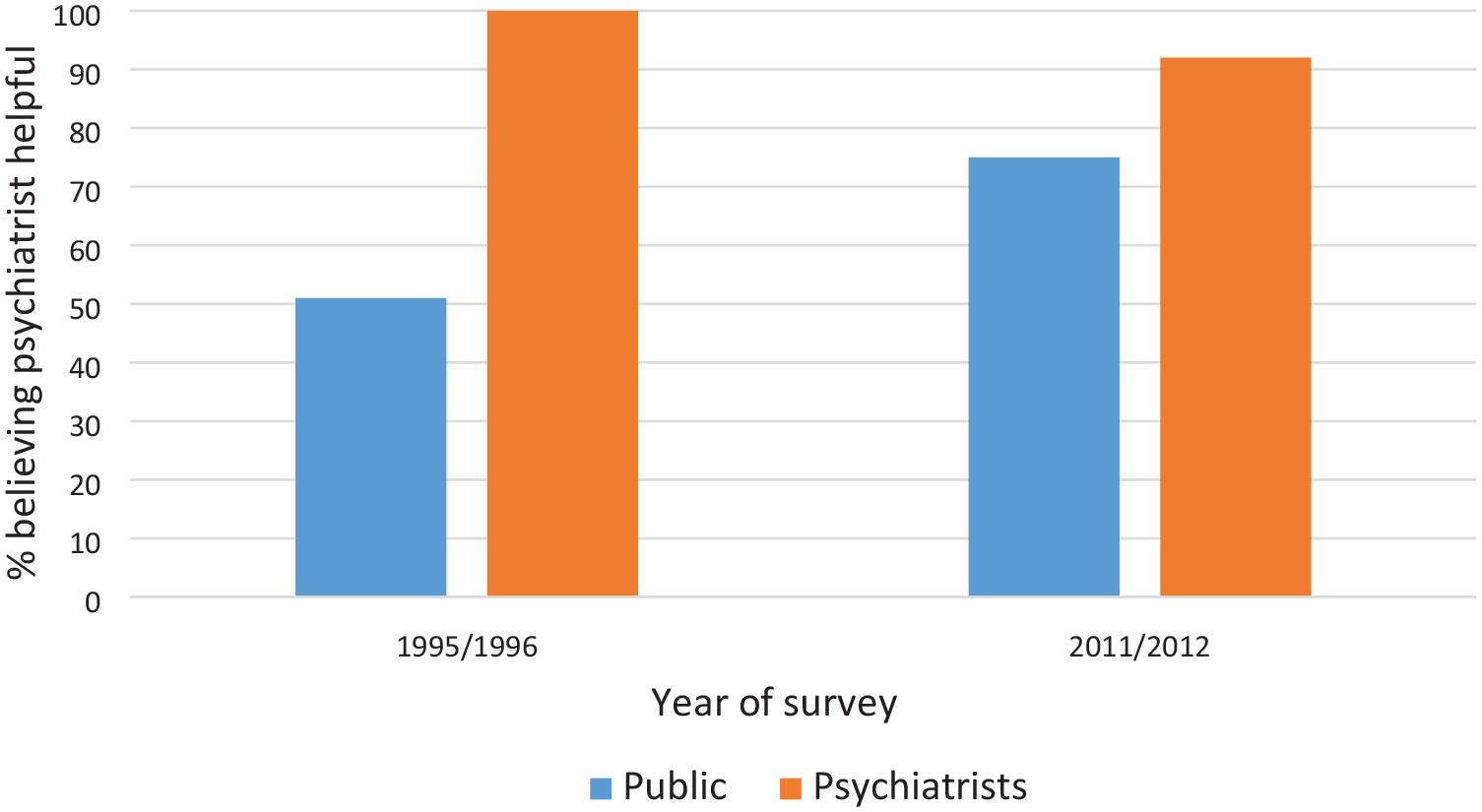
Percentage of the public and psychiatrists believing that seeing a psychiatrist would be helpful for a person with depression symptoms.
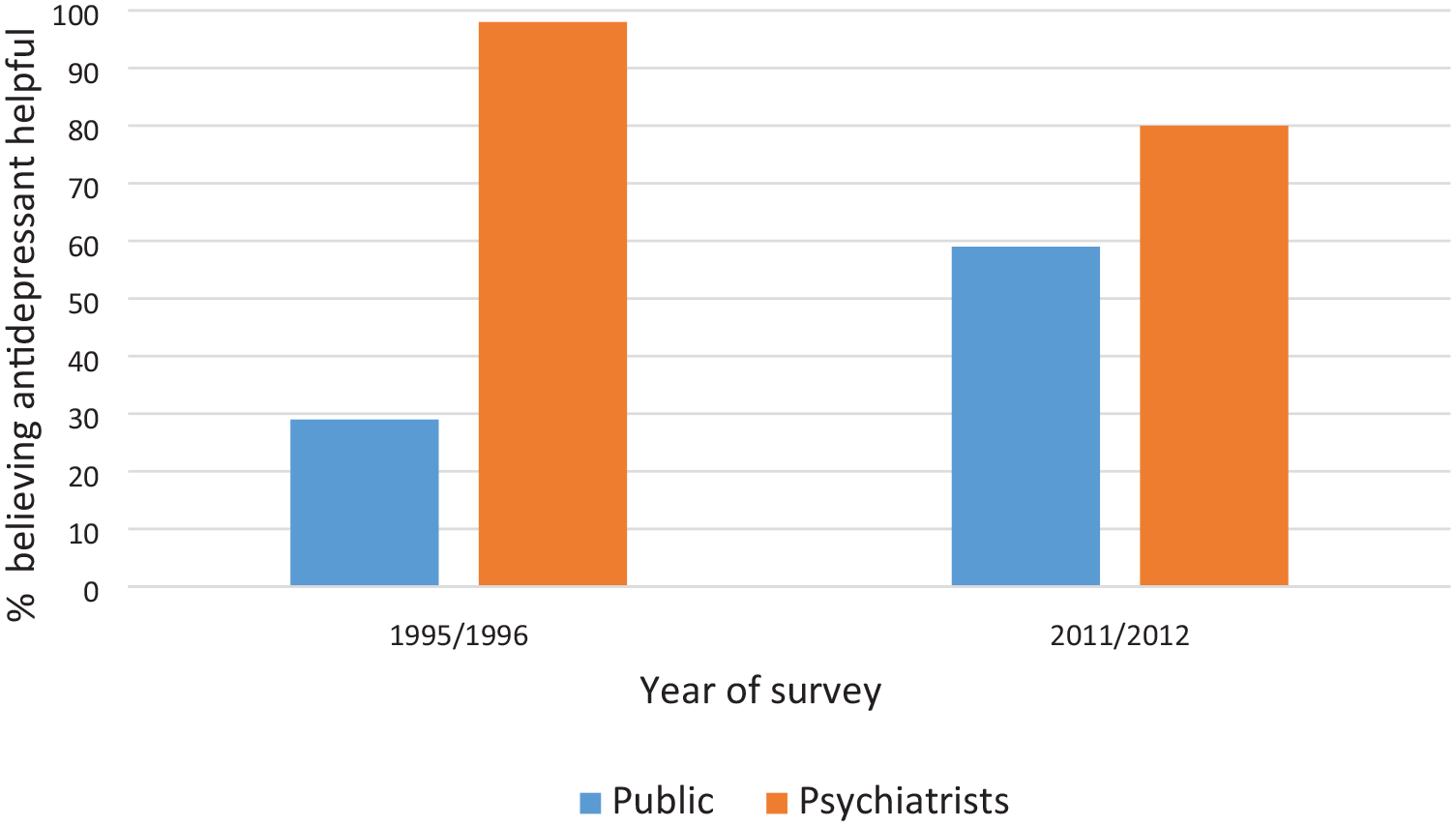
Percentage of the public and psychiatrists believing that an antidepressant would be helpful for a person with depression symptoms.
We can only speculate about whether there has been further change in public thinking since 2011, as no subsequent survey has been carried out. However, everyday experience would suggest that the trend has continued. Some relevant evidence comes from the search terms that Australians use on Google, with Google Trends showing increasing use of psychiatric terms like ‘PTSD’, ‘OCD’ and ‘autism’.
What led to these changes?
These are remarkably large changes in public thinking over a quite brief historical period. How did they come about? Unfortunately, it is not a simple matter to determine what factors produced the changes, as so much occurred over this time period. However, it seems likely that the many community interventions to improve mental health literacy that have been implemented in Australia have been important contributors. There is good evidence that Beyond Blue has had an impact, because the Australian states where Beyond Blue was more active in its early years had greater changes towards psychiatric thinking than those where it was less active (Jorm et al., 2005). Another example is training courses for the public on how to assist a suicidal person. A national community survey carried out in 2017 found that 12% of Australian adults had done such training and that those trained show beliefs and actions towards suicidal persons that are more consistent with professional recommendations (Jorm et al., 2018). However, there are many others that may have contributed, including headspace, SANE, the Black Dog Institute and Everymind, to name but a few.
It also seems likely that cultural norms have changed in a way that has been self-reinforcing. As psychiatric thinking has been articulated by influential people, such as politicians, sporting stars and media personalities, this may have led to further embedding of psychiatric thinking in the population.
If cultural norms about mental disorders are changing, then influences between professional and public thinking will be a two-way street. Looking again at Figures 1–3, not only was there a major change in public thinking to be more like that of psychiatrists, but there was also a smaller change in the opposite direction, with psychiatrists becoming more like the public. Such changes might occur because psychiatrists and other mental health professionals are influenced by what is happening in the broader society. When reporting the findings from our first national survey of mental health professionals in 1996, we noted that the younger cohort of psychiatrists had more positive views about a broader range of psychosocial interventions than their older colleagues and showed a smaller gap from the public in this respect (Jorm et al., 1997a). We predicted that ‘some of the cohort differences may lead to a greater acceptance of interventions that are favoured by the public’, which is what has occurred.
Has the public benefited from thinking more like psychiatrists?
This increase in psychiatric thinking has been accompanied by a substantial increase in the uptake of treatments for mental disorders, including both pharmacological and psychological treatments. The proportion of cases in the population not receiving treatment – what has been called the ‘treatment gap’ – has been successfully reduced. However, this increase in psychiatric thinking and reduction in the treatment gap have not been associated with any improvement in the mental health of the Australian population (Jorm et al., 2017). This is puzzling as there is substantial evidence from controlled trials for the benefits of these treatments. One explanation of this paradox is that the quality of treatment has been lacking, with many people not receiving minimally adequate treatment – what has been referred to as the ‘quality gap’. Another factor may be the neglect of prevention, which is complementary to treatment in improving the health of a population – what has been called the ‘prevention gap’.
What further changes are needed?
The rapid change observed in Australia towards psychiatric thinking shows that it is possible to change the way a whole population conceptualizes mental disorders and what should be done to reduce them. Having reduced the treatment gap, there is arguably a need to apply the same approach to reducing the quality gap and the prevention gap. We need greater public knowledge of what constitutes quality treatment and the range of options available within a stepped care framework, including self-help for milder mental health problems. We also need greater promotion of preventive actions that are targeted to different sections of the population, which is an approach that has been very successful with chronic physical diseases. The rapid uptake of psychiatric thinking over a short historical period augurs well for the possibility of further change as psychiatric knowledge evolves.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.