
Abstract
‘Mental health literacy’ has been defined as the public's knowledge and beliefs about mental disorders which aid their recognition, management or prevention [1]. Low levels of mental health literacy contribute to the large amount of unmet need for treatment of these disorders [2, 3] with its associated heavy emotional and economic burden [4]. The failure to recognize mental health problems and lack of knowledge about mental illness is also an important reason for the often lengthy delay in seeking assistance following the onset of a mental health problem [5, 6]. Misconceptions regarding mental health problems are associated with the widespread stigma towards people with mental illness in the community with a range of negative consequences including a reluctance to commence treatment [7, 8]. However, given our current knowledge of effective treatments, much of the burden of and damage caused by untreated mental disorders could be averted [2, 4]. In addition, the early recognition of, and intervention for mental health disorders has the potential to improve outcomes for patients and their families and prevent secondary complications [9, 10].
Previous surveys of mental health literacy in Australia have found the level of knowledge to be low [1, 11, 12] although improvement has been recently demonstrated following the implementation of national campaigns designed to increase public knowledge about depression including beyondblue: the national depression initiative [13, 14, 15]. While effective at a national level, there are limited data regarding the effectiveness of these initiatives in rural communities and the current level of mental health literacy in those areas is not known. There is some evidence that the attitudes of rural Australians to mental health issues differ from those who live in metropolitan areas [16, 17] and given the very specific culture of rural and remote communities, there is a need to know more about the mental health experiences and needs of rural and remote communities if their needs are to be adequately addressed.
Aim
The aim of the present study was to assess the mental health literacy of rural dwelling Queensland residents prior to the implementation of Australian Integrated Mental Health Initiative (AIMhi) - an evidence-based health promotion strategy. This initiative is directed towards improving the health outcomes of people with chronic or recurring mental disorders. It is also intended that the outcome of the study will inform policy makers of the extent to which the goal of increased community awareness and understanding of mental health issues through promotional activities, as embodied in the National Mental Health Plan 2003-08 [18] is being achieved. This study extends the survey work that has previously been conducted in Australia [1] by including questions designed to assess residents' awareness of mental health agencies in their community and their opinion regarding the quality of the services offered. Additionally, in light of the beyondblue and other similar initiatives, questions were included to determine whether residents were aware of any media reports about depression in the past 12 months. Thus, the results of this survey will add to both the existing knowledge base of mental health literacy in Australian communities and provide a baseline against which the effectiveness of AIMhi can be evaluated.
Method
Four pairs of towns in rural Queensland (Biloela/Bundaberg, Chin-chilla/Emerald, Goondiwindi/Mackay, Oakey/Stanthorpe) are participating in AIMhi, with one member of each pair randomly allocated to an immediate or delayed intervention. Towns are spaced so as to avoid contamination of effects and sets are matched for size, percentage of indigenous people, per cent aged 15 years and under, per cent born overseas and per cent employed as at the 2001 Census [19]. For this survey, a sample of 2% (n = 2132) of the estimated adult population was randomly selected from each town and invited to participate in the survey. The adult population in each town was determined from the 2001 Census [19] and the initial sampling frame was sourced from the local telephone directory as this provided the most readily available resource of residential addresses. The final sample was then selected using random number tables.
The survey was based on a vignette describing a person ‘John’ suffering from major depression which has previously been used in similar surveys [1,12,20–23]. Past research with the vignette has found that the gender of the sufferer made little [21] or no difference [22] to attitudes and thus only the male vignette was used. Although vignettes describing mental health problems other than depression could have been used, the depression vignette was selected, as depression is highly prevalent in the community [24] and it was considered that a majority of people would be able to relate to the vignette. Respondents were asked a series of questions in relation to the vignette including: What do you think is wrong with John (if anything)? Do you think John requires professional help? If John were to receive help from different sources (e.g. a counsellor or general practitioner [GP]), would that be helpful or harmful or neither? They were asked whether a range of strategies including becoming more physically active or going on a special diet would be helpful, harmful or neither and were asked questions regarding the likely outcome of the intervention. They were also asked to estimate the percentage of people in their community with a mental health problem, whether they previously knew or now know anyone with a mental health problem and whether John would be likely to encounter discrimination in the community as a consequence of his difficulty. In addition, questions were asked regarding awareness of agencies or services in their community to assist people with mental health disorders, their opinion as to the quality of those services and whether they had seen or heard anything in the media about depression within the past 12 months. Respondents were also asked basic, nonidentifying demographic questions.
In 2004, the surveys were posted to the selected sample with reply paid envelopes for return. A separate reply paid card was also included for the respondents to notify the research team that they had completed and returned their survey. If no card was received within 3 weeks post mail-out, a reminder letter was sent with a reply paid card on which they could indicate whether they required another survey mailed or desired no further contact. The study was approved by the University of Queensland Research Ethics Committee prior to commencement of the project.
Data analysis
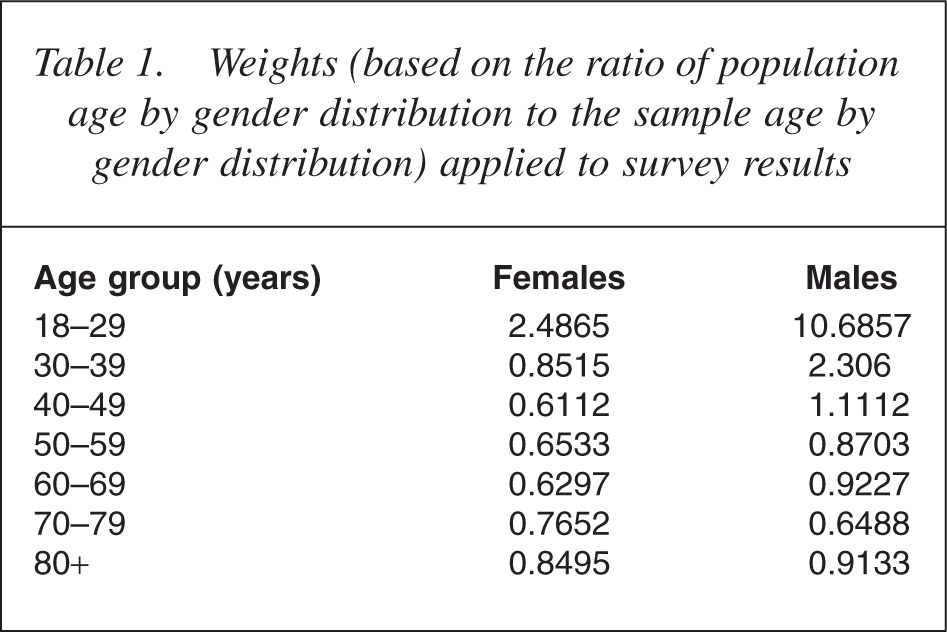
In the first instance, Chi-square analyses were performed to compare the demographic characteristics of respondents across towns. As few relatively minor differences were found, all responses to the survey were grouped together for subsequent analyses and were compared in terms of all demographic variables and in terms of whether the respondent knew anyone with a mental health problem, either currently or previously. The analyses were conducted using SPSS for windows, version 12 (SPSS Inc., Chicago, IL, US). To adjust for probabilities of selection and to reduce non-response bias, the results were weighted based on a ratio of the population age by gender distribution to the age by gender distribution of the sample. With the exception of the demographic data, weighted results are reported in all instances and the weights are presented in Table 1.
Weights (based on the ratio of population age by gender distribution to the sample age by gender distribution) applied to survey results
Results
Of 2132 surveys distributed, 304 (14%) were returned ‘not at this address’, deceased or not contactable for another reason; 666 (36%) were completed and returned. The response rate varied across towns and ranged from 31% in Emerald to 85% in Oakey. There was, however, no consistent relationship between the response rate and level of mental health literacy in each town.
The majority of respondents were female (59.5%) and the median age fell within the 50-59 years age band with the largest group of respondents aged between 40 and 49 years (24.5%). Approximately two-thirds of all respondents were either married or in a de facto relationship and 39% had completed a Technical or Trade certificate level of education or higher. The median annual income reported by respondents was in the range $20000-30000 and the majority of respondents (66%) reported some religious affiliation. The towns were found to differ significantly only in terms of marital status (χ2 (21) = 83.9, p < 0.001) and educational attainment (χ2 (42) = 99.3, p < 0.001). While most respondents were either married or in a de facto relationship in all towns, there were proportionately more single, widowed and divorced or separated people in the larger rural areas of Bundaberg and Mackay. Similarly, there was greater variability in educational attainment in those two areas.
Recognition of depression
Comparisons of the survey responses in terms of demographic variables and in terms of whether the respondent knew anyone with a mental health problem, either currently or previously, revealed few differences. Chi-square values are only presented where results were significant. Overall, 81% (n = 507) of the sample correctly identified John as suffering from depression, while 4.2% (n = 27) thought he had a physical illness and 14.3% (n = 91) thought he had some other problem. Respondents who indicated that they either now (72%; n = 450) or in the past (82.5%; n = 524) knew someone with a mental health problem were more likely to make the correct diagnosis of depression (83.2%; n = 437) than were those who had no such contact (69.9%; n = 65 χ2 (1) = 9.2, p < 0.002). People aged over 70 years were the least likely to report such contact (73%; n = 56) while those aged between 40 and 49 years were the most likely to report such contact (91.3%; n = 115). Almost all respondents (96%; n = 597) felt that John needed professional help and that if he were to seek help from a GP, most respondents (86.4%; n = 532) considered that this would be helpful. A large majority of respondents also considered that assistance from a counsellor would be helpful (88.2%; n = 538) with women more likely to agree with this (92.6%; n = 286) than men (84%; n = 252 χ2 (2) = 11.2, p < 0.004). In comparison, a small majority of respondents (55.2%; n = 341) thought that it would be harmful if John attempted to deal with the problem on his own. Those who had some contact with someone with a mental health difficulty (58.8%; n = 303) were more likely to endorse this view than were those without such contact (35.1%; n = 33 χ2 (2) = 20.5, p < 0.001).
Views regarding treatment and outcomes
Responses to the questions ‘What would be the likely result if John had the sort of professional help you think is most appropriate?’ and ‘What would be the likely result if John did not receive professional help?’ are presented in Table 2. The majority of respondents (79%) thought that, with assistance, John would make a full recovery although the problem would probably reoccur. Without assistance, approximately half of all respondents (50.3%) thought that he would get worse. When asked whether a variety of other strategies might be helpful or harmful or neither, ‘attending courses on relaxation, stress management, meditation or yoga’ was endorsed by the majority of respondents (84%) as being helpful with more women than men endorsing this option. In comparison, undergoing electroconvulsive therapy (ECT) and being admitted to a psychiatric ward were considered to be harmful by most respondents (65.8% and 55.8%, respectively). Those who had contact with someone with a mental health problem were more likely to consider ECT harmful (68.9%) than those without such contact (51.6%; χ2 (2) = 17.7, p < 0.001). These results are presented in Table 3.
Number and percentage (%) of responses to the question ‘What would be the likely result if John had/did not have the sort of professional help you think is most appropriate?’
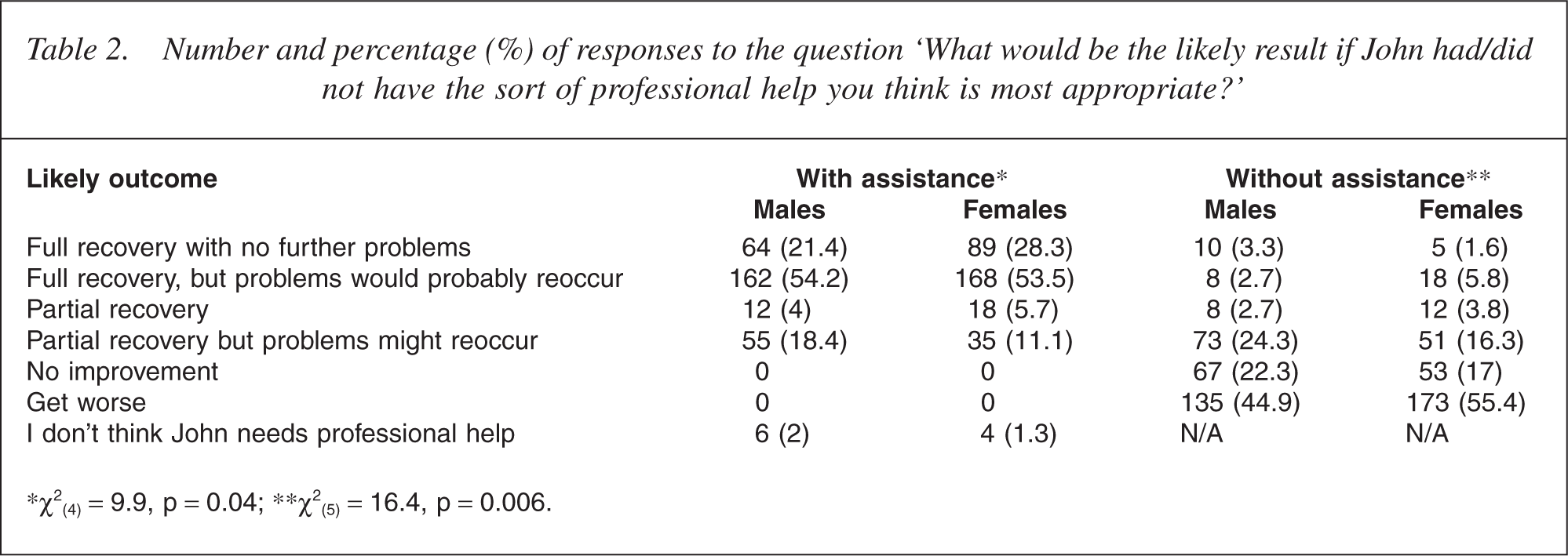
∗χ2 (4) =9.9, p =0.04; ∗∗χ2 (5) =16.4, p =0.006.
Number and percentage (%) of respondents who considered that a strategy would be either helpful or harmful
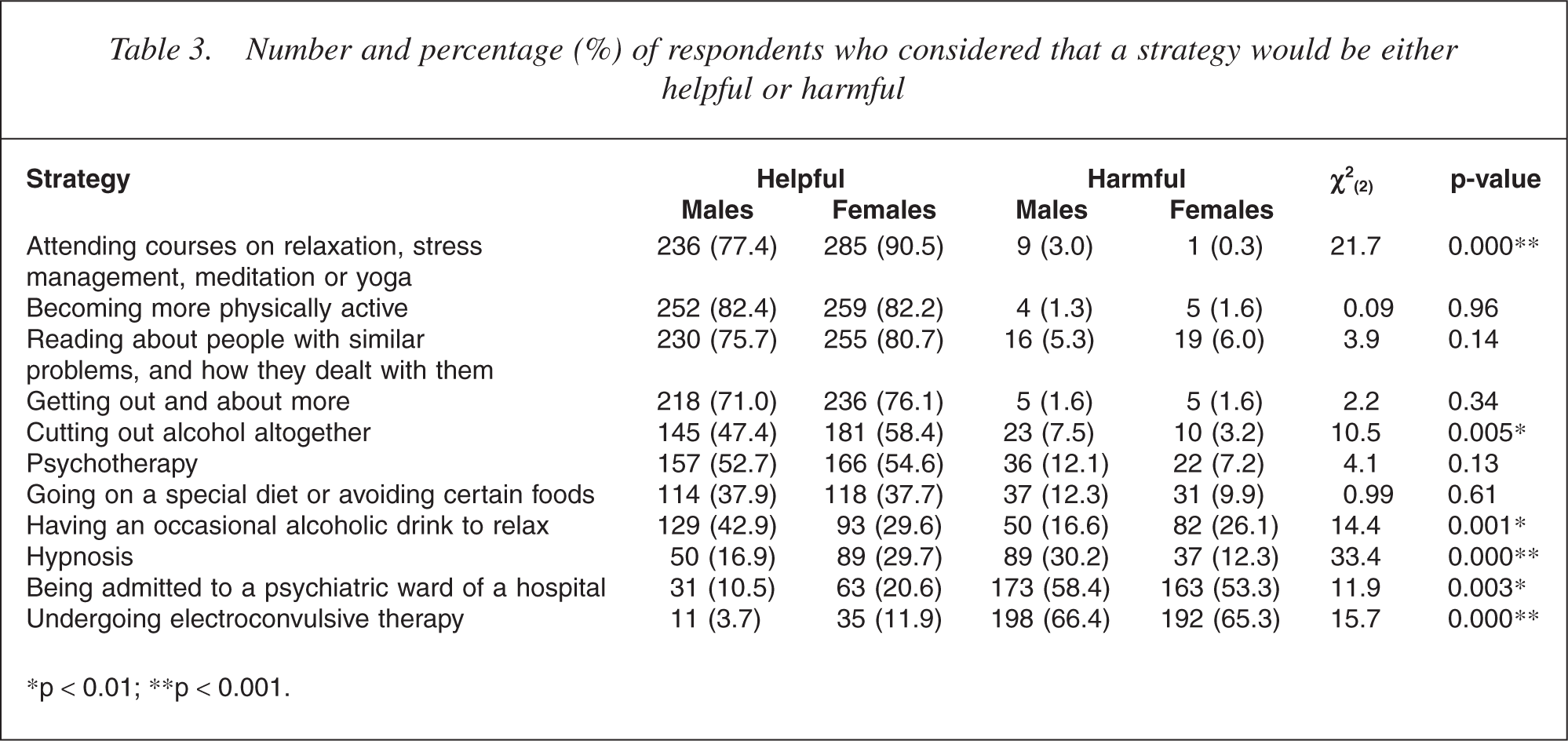
∗p < 0.01; ∗∗p < 0.001.
Community awareness
Results of questions assessing the level of awareness of mental health issues in the community are presented in Table 4. Thirty-four per cent of respondents (n = 207) estimated that more than 20% of their community had a mental health problem while 38% (n = 228) estimated that the prevalence was between 0 and 10%. Women gave higher estimates than did men (χ2 (4) = 13.4, p < 0.009) as did younger people compared with older people (χ2 (4) = 36.8, p < 0.001). Similarly, those who either knew or had previously known someone with a mental health problem gave higher estimates than those without such contact. Nearly two-thirds of respondents thought that John would be discriminated against in the community should his problems be known. When asked whether the respondent would experience difficulty in gaining employment if they had a mental health problem, 44.9% indicated that they would have a lot or extreme difficulty, with more older people (aged over 49 years) endorsing this view (62%) than younger people (aged less than 49 years) (34%; χ2 (4) = 47.3, p < 0.001). In comparison, the majority considered that there would be less difficulty in joining either a sporting team or a social group.
Community awareness of mental health issues according to contact/no contact with someone with a mental health problem (number and percentage)
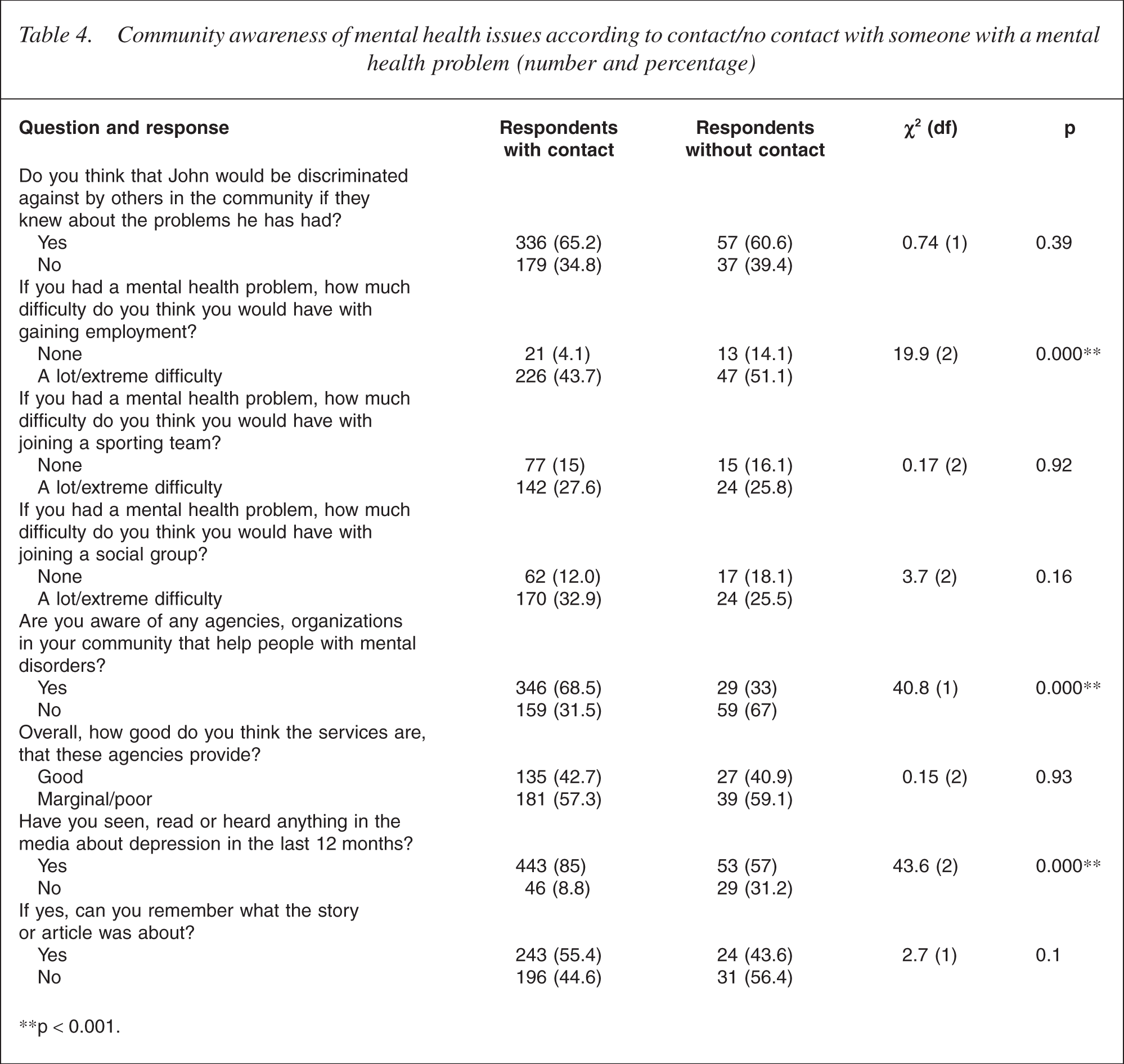
∗∗p < 0.001.
Sixty-three per cent of respondents were aware of agencies to assist people with mental health issues. Respondents who had some contact with a person with a mental health problem were far more likely to be aware of such agencies (68.5%) than were respondents without such contact (33%). The agencies most frequently identified as such were Community Mental Health Services provided by the State Government (33.9%) or Community organizations such as Centacare and Lifeline (30.0%). When asked how good the services provided by each organization were, 42.4% of all respondents considered that the services were good while a large percentage of the total (57.6%) considered that the services were either marginal or poor. In response to the question ‘Have you heard something about depression in the media in the last 6 months?’ 80.8% indicated that they had heard something, with people having some contact with someone with a mental health problem far more likely to respond in the affirmative (85%) than respondents without such contact. Only 54% of the respondents, however, were able to remember the content of the story or article.
Discussion
A very high per cent (81%) of the respondents in our sample correctly identified and labelled the problem in the vignette as depression. This level of recognition is much higher than the rate of 39% reported in a 1995 survey of mental health literacy in Australia using the same vignette [1] and is consistent with other research that indicates that there has been recent growth in mental health literacy in Australia [15, 20]. For instance, Jorm and his colleagues reported that, following the implementation of the beyondblue initiative, 67.8% of respondents in states with a high level of exposure to the initiative correctly identified the problem as depression in their 2004 survey although the improvement could not be attributed to the initiative per se. Other less pronounced differences between the results of that study and the current study include differing beliefs regarding discrimination and whether John would get worse without assistance. In comparison to the 67% of respondents in our study who considered that John would be discriminated against in his community should his problems be known, 53% of the sample surveyed in 2004 considered that discrimination would be likely. In the present study, approximately half of the respondents (50.3%) considered that John would get worse without assistance compared with 64% of the respondents who endorsed this view in the 2004 survey. Although these findings may reflect real differences in beliefs across regions of Australia, there are also important methodological differences in the two studies to be considered. For instance, the present study assessed the attitudes of rural Queensland residents by inviting them to respond to a written survey while Jorm and his colleagues sampled residents on an Australia-wide basis and face-to-face interviews were conducted.
Otherwise, many of the responses of rural Queensland residents to the remaining survey questions were similar to other recent Australian findings [14, 20]. These include the high per cent (79%) of respondents who predicted a full recovery for John although a relapse could be expected; the perception that GPs and counsellors would be helpful; the view that strategies including courses on relaxation, stress management, meditation or yoga, becoming more physically active, reading about people with similar problems, and how they dealt with them and getting out and about more would be helpful; and the view that hospitalization in a psychiatric ward and ECT are harmful.
An important finding in the current study was that a majority of respondents underestimated the prevalence of mental health problems in the community, with only 34% correctly estimating the prevalence to be greater than 20% [4, 23]. Similarly, approximately 40% of respondents were not aware of any agencies in their community to assist those with mental health issues. Not knowing where to access assistance has been identified as an important reason for the delay in seeking treatment once a mental health problem becomes apparent [5]. Furthermore, the majority of respondents (58.6%) considered that the services offered were either marginal or poor, leading to the conclusion that people in need are unlikely to utilise those services. While it would be useful to know upon what basis this opinion was derived, it appears that there is a need for both Government and Community agencies to better promote their services and/or improve the services provided. Finally, although a high proportion of respondents in the present study indicated that they had heard something about depression in the media within the past 12 months, only half were able to recall the content of the article or news item. This suggests that the development of strategies to enhance the retention of information that is disseminated through the media is an important area for future research.
Although this study is, to our knowledge, the first to explore the views of rural Queensland residents regarding mental health issues in the community and provides baseline data against which to evaluate the effectiveness of AIMhi, it is not without weaknesses. For instance, it is possible that there may have been some response bias in the present study. This would be the case if residents with either knowledge of and/or interest in mental health issues were more likely to complete the survey than less informed and less interested residents. A bias in this direction could account for the high rate of recognition of depression and is also suggested by the high percentage of respondents who indicated either past or current knowledge of someone with a mental health problem. Equally, however, this could reflect the likelihood that a majority of people will have some contact with mental health issues at some point during their lifetime, given the very high lifetime risk of mental health difficulties [4]. If such a response bias has occurred, it could mean that our results reflect the upper end of the spectrum of mental health knowledge in rural Queensland.
Another potential source of bias lies in the selection of the sample frame from local telephone directories, which excluded people who did not have a telephone number listed. People are likely to not have a telephone number listed for non-random reasons - either because they are unable to afford one or because of a desire to maintain their privacy, so it is possible that our selection method may have introduced some selection bias into the study. Caution is therefore warranted in generalizing the results of this study to the wider community. In addition, given the research focused upon depression, it cannot be assumed that the results of this study reflect the attitudes to and knowledge of other mental health problems including schizophrenia which may be quite different and warrant additional investigation. An additional limitation lies in the format of the questions that were included in the survey, and it is conceivable that quite different results may have been obtained had the questions been phrased differently. For instance, the question ‘Do you know anyone with a mental health problem…’ was asked which is very broad in scope and encompasses people with intimate relationships with someone with a mental health problem as well as those with only a very tenuous relationship. The knowledge and experience of mental health issues in the two cases is likely to be very different and the results would provide a more comprehensive picture of mental health literacy in rural Queensland residents had it been possible to identify these responses according to the closeness of the relationship. This may be a useful addition to future research in this area.
In conclusion, although there were a few exceptions, in general the findings of this study are consistent with the results of other recent Australian studies [14, 20] that demonstrate that the level of mental health literacy in Australia is currently higher than it was in the mid- to late 1990s [12, 21]. It thus appears that some progress has been achieved towards the goal of increased awareness and understanding of mental health issues in the community through mental health promotion that is embodied in the National Mental Health Plan 2003-08 [18]. It is also clear, however, that there is a continuing need for mental health education in rural Queensland.
Footnotes
Acknowledgements
This survey was conducted as part of the AIMhi and was funded by the National Health and Medical Research Council (Project ID: 2003000079). The valuable contribution of the AIMhi Rural Team to various stages of this survey is acknowledged, including Professor David Kavanagh, Professor Cindy Gallois, Professor Chris del Mar, Dr David King, Heidi Sturk and Melissa Haswell.