
Abstract
Over the past few decades, sex differences in socio-demographic characteristics, clinical presentation, course, treatment response and genetics in schizophrenia have been intensively investigated [1–4]. There is compelling evidence to indicate that the pharmacokinetics and pharmacodynamics of psychotropic drugs differ between male and female schizophrenia patients, although few prescription guidelines sufficiently address the issue [5–7].
Most of the studies on sex differences in psychotropic prescription patterns in schizophrenia have been conducted in western settings. Most have found that men require higher doses of antipsychotics [8], women are more likely to take more concomitant medications [7], the dosing intervals for women are longer after a steady clinical state has been achieved [9] and women experience more drug-induced side effects [10]. Based on these findings, Seeman [7] concluded that the sex of the patient should be taken into account when prescribing psychotropic drugs.
To date, there has been no large-scale, multi-centre study that exclusively explores the sex differences in various psychotropic prescribing patterns in Asian schizophrenia patients. The aim of this study was thus to examine the sex differences in both the prescribing patterns of psychotropic drugs and drug-induced side effects in schizophrenia patients in Asia.
Methods
Subjects and setting
The study was part of the Research on Asia Psychotropic Prescription (REAP) project, which is an ongoing pharmaco-epidemiological investigation of psychotropic drug prescription trends in schizophrenia inpatients in Asia. The participating countries and regions include mainland China, Hong Kong, Japan, Korea, Singapore and Taiwan. Each centre used the same standardized protocol and data collection procedure. Centres in India, Malaysia and Thailand joined the project in 2009. The three REAP surveys to date were conducted in July 2001, July 2004 and from October 2008 to March 2009. Details of the REAP project have been described elsewhere [11–13]. Briefly, patients were included if (i) they had been diagnosed with ICD-10 or DSM-IV schizophrenia; (ii) could comprehend the aims of the study; and (iii) agreed to participate in this study, and provided written or oral consent according to the requirements of the clinical research ethics committees in the respective study sites. Those suffering from major medical conditions were excluded. Approval of the study protocol was granted by the clinical research ethics committees of the respective centres.
Eligible patients were recruited consecutively, and their basic socio-demographic and clinical data were collected using a questionnaire designed for the study. Consensus meetings on data collection and uniform data entry were held before each survey. Doses of antipsychotic drugs were converted into chlorpromazine equivalents in mg (CPZeq) [14–16]. This study explored the sex differences in antipsychotic doses, extrapyramidal side effects (EPS), tardive dyskinesia (TD), weight gain within the past three months, and six major groups or aspects of psychotropic drug prescriptions, namely, second-generation antipsychotics (SGAs), depot antipsychotics, mood stabilizers, anticholinergics, antidepressants and antipsychotic polypharmacy. TD was singled out due to its special characteristics comparing to other extrapyramidal symptoms.
Statistical analysis
The data were analysed using SPSS 13.0 for Windows. Comparisons between socio-demographic and clinical characteristics of the male and female patients were performed using the independent sample t-test, Mann-Whitney U test and chi-square test, as appropriate. Multiple logistic regression analysis was employed to adjust for relevant demographic and clinical covariates and to determine the independent contribution of sex to prescription patterns and drug-induced side effects. The one-sample Kolmogorov-Smirnov test was adopted to check the normality of distribution for the continuous variables. The level of significance was set at 0.05 (two-tailed).
Results
Six countries/regions, China, Hong Kong, Japan, Korea, Singapore and Taiwan, took part in all three surveys; hence, patients from these six locales were included in this study. A total of 6441 patients participated: 2399, 2316 and 1,906 in 2001, 2004 and 2009, respectively.
Table 1 presents the socio-demographic and clinical characteristics of the whole sample and those of the two sexes. The following factors were significantly associated with the male sex: a younger age, higher doses of antipsychotics, less severe delusions and hallucinations, more severe negative symptoms, fewer SGAs, more mood stabilizers, antipsychotic polypharmacy and depot antipsychotics, more TD, and fewer complaints of weight gain. After controlling for the confounding effects of age and severity of psychopathology using analysis of covariance (ANCOVA), a significant difference in antipsychotic drug doses remained between the two groups (F(1, 6434) = 15.5, p < 0.001). Table 2 shows the commonly prescribed SGAs.
Basic demographic and clinical characteristics of the sample (2001–2009)
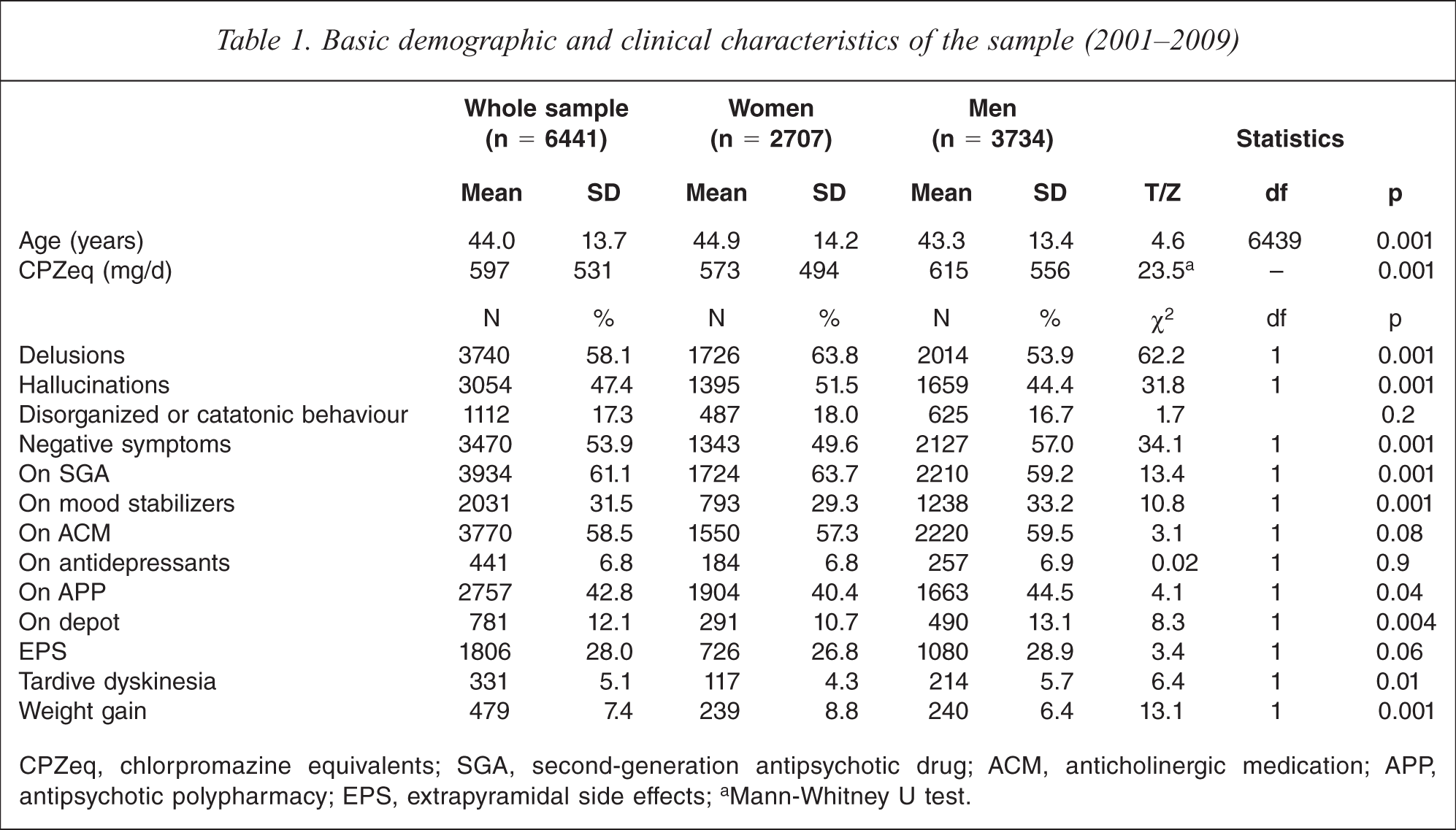
CPZeq, chlorpromazine equivalents; SGA, second-generation antipsychotic drug; ACM, anticholinergic medication; APP, antipsychotic polypharmacy; EPS, extrapyramidal side effects;a Mann-Whitney U test.
Commonly prescribed second-generation antipsychotic medications in the pooled sample (2001–2009)
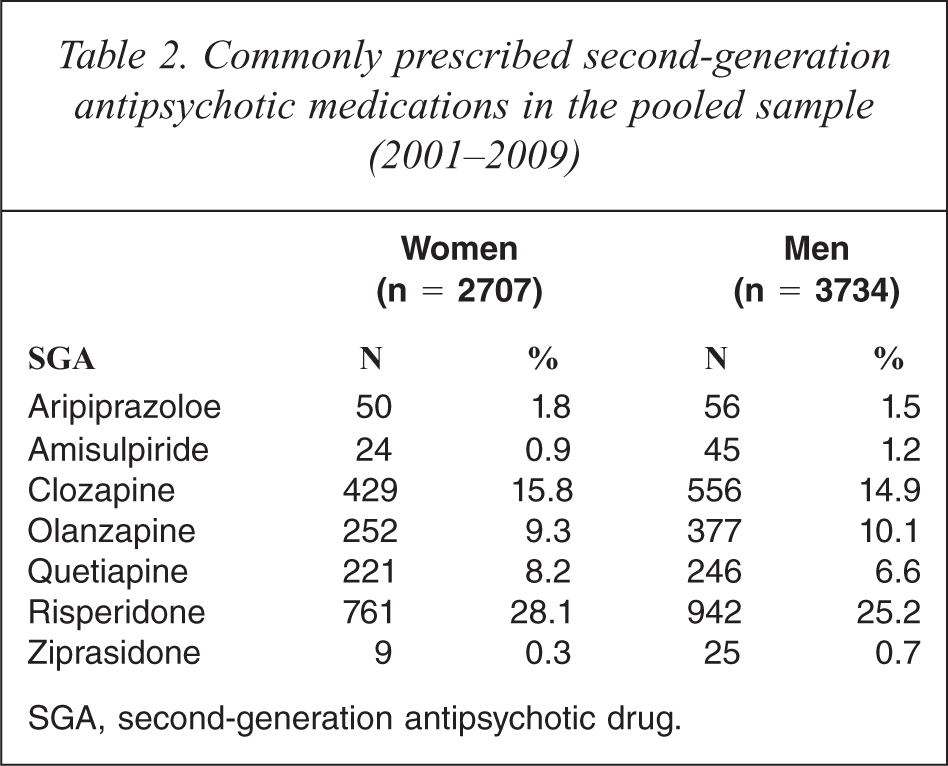
SGA, second-generation antipsychotic drug.
In stepwise multiple logistic regression analyses, the male sex independently contributed to fewer SGAs, more mood stabilizers, anticholinergics, antipsychotic polypharmacy and depot antipsychotics, EPS, TD, and fewer complaints of weight gain (Table 3).
Multiple logistic regression analyses of the impact of sex on psychotropic drug prescription in the sample (n − 6441)
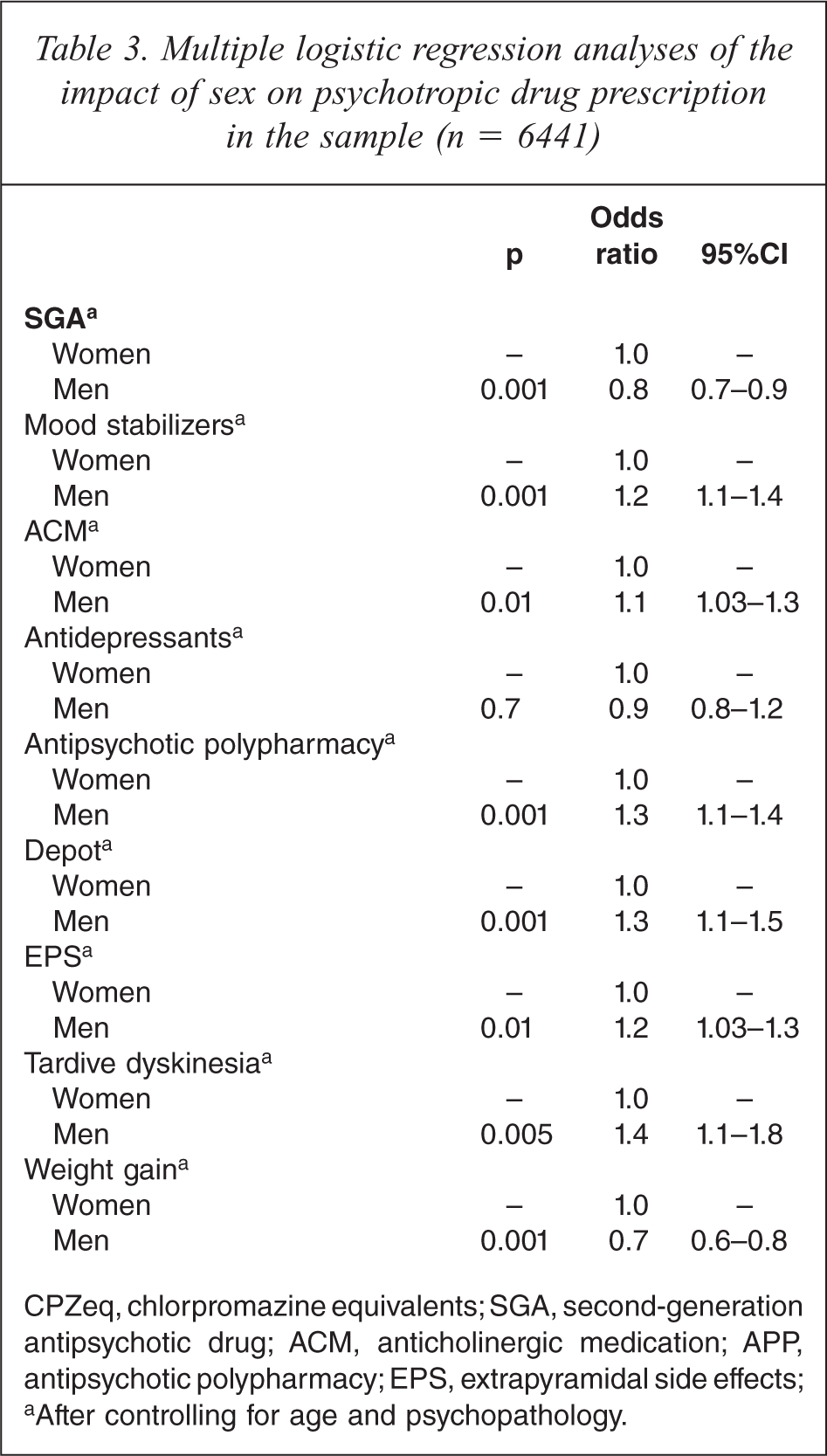
CPZeq, chlorpromazine equivalents; SGA, second-generation antipsychotic drug; ACM, anticholinergic medication; APP, antipsychotic polypharmacy; EPS, extrapyramidal side effects;a After controlling for age and psychopathology.
Discussion
The study's finding of higher doses of antipsychotics being prescribed to male patients is consistent with previous findings [7,17,18]. The disparity in antipsychotic doses between the sexes may be due to differences in treatment responses and related to a combination of pharmacokinetic, pharmacodynamic, genetic, hormonal and psychosocial factors [7]. Psychotic men more frequently present with violent and aggressive behaviour, resulting in the prescription of higher antipsychotic doses [19].
With regard to the tolerability of antipsychotic drugs, women have been reported to complain more about EPS and anticholinergic side effects [20]. In addition to being associated with less severe EPS, SGAs are also less likely to cause prolactin elevation [21], and thus are more acceptable to women, which may account for the more frequent use of SGAs found among female patients in this study.
Female schizophrenia patients present with more mood symptoms [22,23], and thus require more mood stabilizers and antidepressants [7,24]. In contrast to findings in the west, but replicating those for Asian patients [25,26], in this study, antidepressant prescriptions were similar for the two sexes, although more men than women received mood stabilizers. Male schizophrenia patients display more aggressive and violent behavior and are perceived to be more threatening [19,27]. As they augment the effects of antipsychotic drugs [28], mood stabilizers are often used to control aggressive or impulsive behavior, and they may also improve antipsychotic treatment responses [29,30].
A sizeable proportion of schizophrenia patients exhibit only a partial (30–40%) [31] or no response (10–15%) [32] to currently available antipsychotic drugs. Antipsychotic polypharmacy is frequently considered for treatment-refractory patients, although most guidelines emphasize the importance of antipsychotic monotherapy. As most [33,34], though not all [35], studies have found that female schizophrenia patients respond better to antipsychotic treatment, it was expected in this one that more male patients would be likely to receive antipsychotic polypharmacy. Our results indeed support this expectation.
Depot antipsychotics are commonly used in clinical practice to ensure treatment adherence, thereby reducing the frequency and severity of relapse and subsequent hospitalization [36,37]. Female schizophrenia patients display better treatment adherence and stronger therapeutic alliance than their male counterparts [7,38,39], which may explain why male patients receive more depot antipsychotics.
In this study, the male patients experienced more severe EPS and TD, which replicates most [18,40,41], but not all [42], previous findings. The more severe EPS may account for the more frequent use of anticholinergic medications found in our study.
Most antipsychotic drugs can cause weight gain and an elevated body mass index (BMI) [43–45], particularly in women [46], thereby increasing the risk of diabetes mellitus, hypertension, coronary heart disease and related conditions [47]. The female patients in this study complained more often than the males of recent weight gain. Antipsychotic-induced weight gain is thought to be the result of increased appetite related to the interaction between these drugs and the dopaminergic, serotonergic, and histaminergic receptors [48,49]. A recent review [50] concluded that antipsychotic-induced weight gain stems from genetic polymorphisms related to the leptin [51] and alpha 2 adrenoceptor gene [52].
The major strengths of this study are its large sample size and the ethnic diversity of the sample. Nevertheless, its results should be interpreted with caution because of several methodological shortcomings. First, the REAP study included only inpatients; hence, the results cannot be generalized to the entire schizophrenia population in Asia. Second, this study did not examine the pharmacokinetic and pharmacodynamic aspects of treatment that may have contributed to the sex differences found in prescriptions and medication-induced side effects. Third, a number of important factors that would be likely to have an impact on prescription patterns, such as substance use, length of hospitalization, height, weight were not evaluated in some of the centres. Fourth, the conversion of antipsychotic doses, particularly SGAs and depot antipsychotics, into CPZeq is not entirely accurate, which is a general problem with prescription pattern surveys, in addition to their cross-sectional nature [53]. Employing the same conversion standard to compare the sexes may mitigate this shortcoming, however. Finally, as part of an ongoing, large-scale, international project, this paper only aimed at the sex difference in the prescription patterns of major psychotropic drugs and drug-induced side effects, therefore the relationships between other demographic and clinical variables were not discussed here.
In conclusion, this study demonstrates that sex is an independent contributor to antipsychotic prescriptions and the occurrence of EPS, TD and weight gain in Asian schizophrenia patients. Its results suggest that sex should be taken into account when clinicians make decisions about the dose of psychotropic drugs and the form of their delivery. Antipsychotic treatment guidelines should pay greater attention to patients’ sex. The prescribing patterns for mood stabilizers, antidepressants and antipsychotic polypharmacy identified in this study differ from those found in western studies. Pharmacokinetic and pharmacodynamic studies are warranted to further explore the contribution of sex to psychotropic prescribing patterns and drug-induced side effects.
Footnotes
Acknowledgements
The authors are grateful to the following clinicians who were involved in data collection: Hong Deng and Wei Hao in China; Ajit Avasthi, Dipesh Bhagabati, Roy Abraham Kallivayalil, Shubhangi R. Parkar and Y.C. Janardhan Reddy in India; Tateno Masaru, Masamune Yayoi, Akiyama Tsuyoshi, Sato Soichirou, Nakagome Kazuyuki, Nakamura Jun and Kuroki Toshihide in Japan; Tae-Yeon Hwang, Seok Hyeon Kim, Yo Wang Lee and Jong-Il Lee in Korea; Tung-ping Su, Shih-ku Lin, Tzu-ting Chen, Chieh-hsin Chang, Hong-chieh Hsu, Chi-Fa Hung and Cheng-chung Chen in Taiwan; Krisakorn Sukavatvibul, Jittima Kleawtanong, Tantawan Suradechasakul, Manote Lotrakul and Usaree Srisutudsanavong in Thailand, and Norharlina Bahar in Malaysia. The authors would also like to thank the clinicians who helped to organize the study in each study site.