
Abstract
Objective:
This study examined the use, demographic and clinical correlates of antipsychotic polypharmacy (APP) and its associations with treatment satisfaction and quality of life (QOL) in schizophrenia patients in China.
Method:
A total of 4239 patients in 45 nationwide Chinese psychiatric hospitals/centers were interviewed in 2012 in the third cross-sectional study, with the first two having been conducted in 2002 and 2006. Patients’ socio-demographic and clinical characteristics, including psychopathology, side effects, satisfaction with treatment and QOL, were recorded using a standardized protocol and data collection procedure.
Results:
The proportion of APP prescriptions in 2012 was 34.2%, which was significantly higher than the frequency of APP in 2002 (26.1%) and 2006 (26.4%) (p<0.001). Of patients on APP, 91.1% received two antipsychotics, 8.6% received three and 0.3% received four or more antipsychotics. Multiple logistic regression analyses revealed that compared to those on antipsychotic monotherapy, patients on APP and their families had lower satisfaction with treatment, had higher QOL in the mental domain, younger age of onset, more side effects, higher doses of antipsychotics and were more likely to receive first-generation antipsychotics and less likely to receive benzodiazepines (total R2=0.31, p<0.001).
Conclusions:
APP was found in about one in three schizophrenia patients. The prevalence of APP seems to have been increasing since 2002. Considering the increased frequency of drug-induced side effects and the patients’ and their relatives’ dissatisfaction with antipsychotic treatment, further examination of the rationale and appropriateness of APP and its alternatives is warranted.
Introduction
The concurrent use of two or more antipsychotic drugs, also called ‘antipsychotic polypharmacy’ (Tapp et al., 2005), is common in clinical practice (Faries et al., 2005). The frequency of American schizophrenia patients on APP increased from 32% in 1998 to 41% by 2000 (Ganguly et al., 2004). A meta-analysis of 147 studies (Gallego et al., 2012a) found that APP was more common in Asian schizophrenia patients compared to their Western counterparts.
The use of APP has been controversial. Although two meta-analyses suggested that APP may have superior efficacy compared to antipsychotic monopharmacy (AMP) (Barbui et al., 2009; Correll et al., 2009), results were ultimately inconclusive. In a recent meta-analysis of antipsychotic augmentation of clozapine, benefits were only apparent in open label studies (Barbui et al. 2009). In another meta-analysis, the superiority of APP over AMP was demonstrated only by individual trials which initiated antipsychotic co-treatment at the start of antipsychotic treatment rather than after non-response to antipsychotic monotherapy (Correll et al. 2009). Furthermore, although APP has been associated with markers of greater illness acuity, severity and refractoriness that may justify its use (Correll and Gallego, 2012), criticism of APP has included variability across cultures and regions, indicating subjective reasons, the potential for increased hospitalization rates, increased side effects, higher treatment costs and increased mortality (Elie et al., 2010; Gallego et al., 2012b; Tiihonen et al., 2012). Based on these findings, several attempts have been made to reduce inappropriate APP in clinical practice settings (Essock et al., 2011; Tani et al., 2013).
In order to rationalize its use, it is important to understand the place of APP in clinical practice. Despite its frequent use, there have been only a few studies investigating the prevalence and correlates of APP in schizophrenia in China. In a cohort of 398 schizophrenia patients in Beijing and Hong Kong, 17.6% received APP (Xiang et al., 2007a). In the Research on Asian Psychotropic Prescription Pattern project, the frequency of APP in schizophrenia in Beijing was 25.2% in 2001, 23.8% in 2004 and 35.9% in 2009 (Xiang et al., 2012). However, the two studies above only included two and four psychiatric hospitals, respectively, and therefore their findings are unlikely to reflect nationwide patterns.
This study set out to: (1) examine the use of APP in schizophrenia in a national survey on the prescription of psychotropic medications; and (2) explore the demographic and clinical correlates of APP and its associations with treatment satisfaction and quality of life (QOL).
Method
Study design and participants
This study was part of a national, iterative, cross-sectional pharmaco-epidemiological survey project conducted in China and initiated by the Chinese Society of Psychiatry. The initial survey was conducted in May 2002 and was followed by two further surveys in May 2006 and July/August 2012 using the same design and a standardized protocol (Si et al., 2004). Consensus meetings on data collection and uniformity of data entry were held prior to each survey. Altogether, 45 mental health centers/units located in 10 provinces and municipalities, including Beijing, Guangdong, Hebei, Hubei, Jiangxi, Jiangsu, Jilin, Shaanxi, Shanxi and Sichuan, participated in each survey. The 45 mental health centers/units included in this study were the same sites included in the previous two surveys (Si et al., 2004; Zhang et al., 2012).
In- and outpatients receiving treatment in the participating hospitals during the study period of 8 weeks were consecutively referred by their treating psychiatrists to the research team to be screened for eligibility. All members of the research team were trained psychiatrists. Inclusion criteria included: (1) Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) or International Classification of Diseases, 10th Revision (ICD-10) diagnosis of schizophrenia based on a review of medical records and a clinical interview; (2) age 15 years or older; (3) taking antipsychotic drugs; and (4) the ability to understand the aims of the survey and a willingness to provide written informed consent. The study protocol was approved by the Ethics Committees of the participating centers.
Assessments
Basic socio-demographic and clinical characteristics were collected using a form designed for the study. Information about the types and doses of all psychotropic drugs were collected from the medical records. Doses of antipsychotic drugs were converted into chlorpromazine equivalent milligrams (CPZeq) (American Psychiatric Association, 1997; Kane et al., 1998; Woods, 2003). The cumulative doses of all antipsychotics prescribed were used for analyses. For the purpose of analysis, high doses of antipsychotic medications were defined as ≥600 mg/day CPZeq (Xiang et al., 2014). APP was defined as the concurrent prescription of two or more antipsychotics, irrespective of the duration or reason for such prescriptions (Xiang et al., 2007a, 2012). Age at onset of illness younger than 25 years defined early-onset schizophrenia (Paillere-Martinot et al., 2001).
Following the same procedures of the Research on Asian Psychotropic Prescription (REAP) project (Chong et al., 2004; Xiang et al., 2012), delusions, hallucinations, disorganized speech or behavior, and negative symptoms in the past month were evaluated and recorded in the diagnostic interview. Global illness severity was evaluated with the Chinese versions of the Clinical Global Impressions–Severity scale (CGI-S) (Guy, 1976). The Treatment Emergent Symptom Scale (TESS) (National Institute of Mental Health, 1985) was used to record side effects. QOL was assessed with the validated Chinese version of the Medical Outcomes Study Short Form 12 (SF-12) (Jenkinson and Layte, 1997; Zhang et al., 2011). The SF-12 is a multidimensional generic instrument with 12 items addressing eight health domains: physical functioning, role limitations due to physical problems, bodily pain, vitality, and social functioning as well as role limitations each related to emotional problems and mental health. For the purpose of statistical analysis, the first four domains were collapsed into a physical component score, while the remaining four domains formed a mental component score. A higher score on SF-12 indicates better QOL. Patients’ and their families’ satisfaction with the current treatment was evaluated with a self-rated, 7-point Likert scale, scoring from 1 (extreme dissatisfaction) to 7 (extreme satisfaction).
Chinese hospitals are classified into three levels according to the degree of specialization in clinical care and research. Level-III hospitals have the highest staff–patient ratio and the best medical equipment. Level-II hospitals are regional medical centers that treat patients with severe diseases, while Level-I hospitals are small, community level hospitals providing basic medical care (Liang et al., 2004). There was no Level-I psychiatric hospital at the time of the study in the areas included, and thus only Level-III/II medical facilities were involved in this study.
Prior to the study, all 135 raters were trained in the use of the above-mentioned assessment tools in 20 schizophrenia patients. The inter-rater reliability of the rating instruments and the judgment of APP between the raters yielded satisfactory to good agreement (>0.75).
Statistical analysis
The statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS), version 20.0 (IBM Corp., Armonk, NY, USA). Samples are reported as numbers and percentages, averages as means ± standard deviations (SD). Comparisons between APP and AMP in terms of demographic and clinical variables were conducted by chi-squared tests, independent-samples t-tests or Mann–Whitney U-tests, as appropriate. Furthermore, patients’ and their families’ satisfaction with the current treatment and QOL were compared between the APP and AMP groups after controlling for the potentially confounding effects of variables that significantly differed between the two groups in univariate analyses using analysis of covariance (ANCOVA). Univariate analyses were conducted first because they could identify covariates that potentially confound the associations of APP use with treatment satisfaction and QOL.
In addition, multiple logistic regression analysis with the ‘simultaneous’ method (i.e. all specified independent variables were entered at one time) was used to determine the demographic and clinical variables significantly associated with APP. APP was the dependent variable, while inpatient status, negative symptoms in the past month, use of first-generation antipsychotics (FGAs) and benzodiazepines, early onset of illness, TESS total score and number of patients on high doses of antipsychotics were entered as independent variables; other variables that significantly differed between the two groups in univariate analyses were entered as covariates. These independent variables were examined because they are clinically relevant to APP use. Statistical significance was set at p<0.05 (two-tailed).
Results
A total of 5386 patients from 45 psychiatric hospitals/centers were invited to participate in the study: 4334 met study entry criteria, resulting in a participation rate of 80.5%. Of the participants, 95 (2.2%) did not complete the interview, so that 4239 were included in the analysis.
The APP group comprised 1448 patients (34.2% of the whole sample): 1319 (91.1%) received two, 124 (8.6%) received three and five (0.3%) received four or more antipsychotics.
Table 1 shows the socio-demographic and clinical characteristics of the whole sample and separately by APP and AMP groups. Compared to the AMP group, patients on APP were significantly younger, had an earlier age of onset and a longer illness duration, higher CGI-S scores, more delusions, hallucinations, and disorganized and negative symptoms, were more likely to be inpatients and receive FGAs or second-generation antipsychotics (SGAs), but were less likely to receive benzodiazepines (BZDs). In addition, they had higher TESS scores, CPZ equivalent doses of antipsychotics, and QOL mental domain scores, but lower patient and family treatment satisfaction scores. After controlling for the potentially confounding effects of variables that significantly differed between the two groups (inpatient status, delusions or hallucinations, disorganized speech or behavior and negative symptoms in the past month, use of FGAs, SGAs and benzodiazepines, age, age of onset, duration of illness, scores of CGI-S and TESS total and CPZeq) using ANCOVA, APP was still associated with lower satisfaction with treatment by patients (F(1,4226)=7.9, p=0.005) and their relatives (F(1,4226)=9.4, p=0.002) and higher mental QOL (F(1,4226)=11.2, p=0.001), while there was no significant difference with respect to physical QOL (F(1,4226)=2.2, p=0.13).
Comparison between antipsychotic polypharmacy (APP) and antipsychotic monotherapy (AMP) with respect to basic demographic and clinical variables.
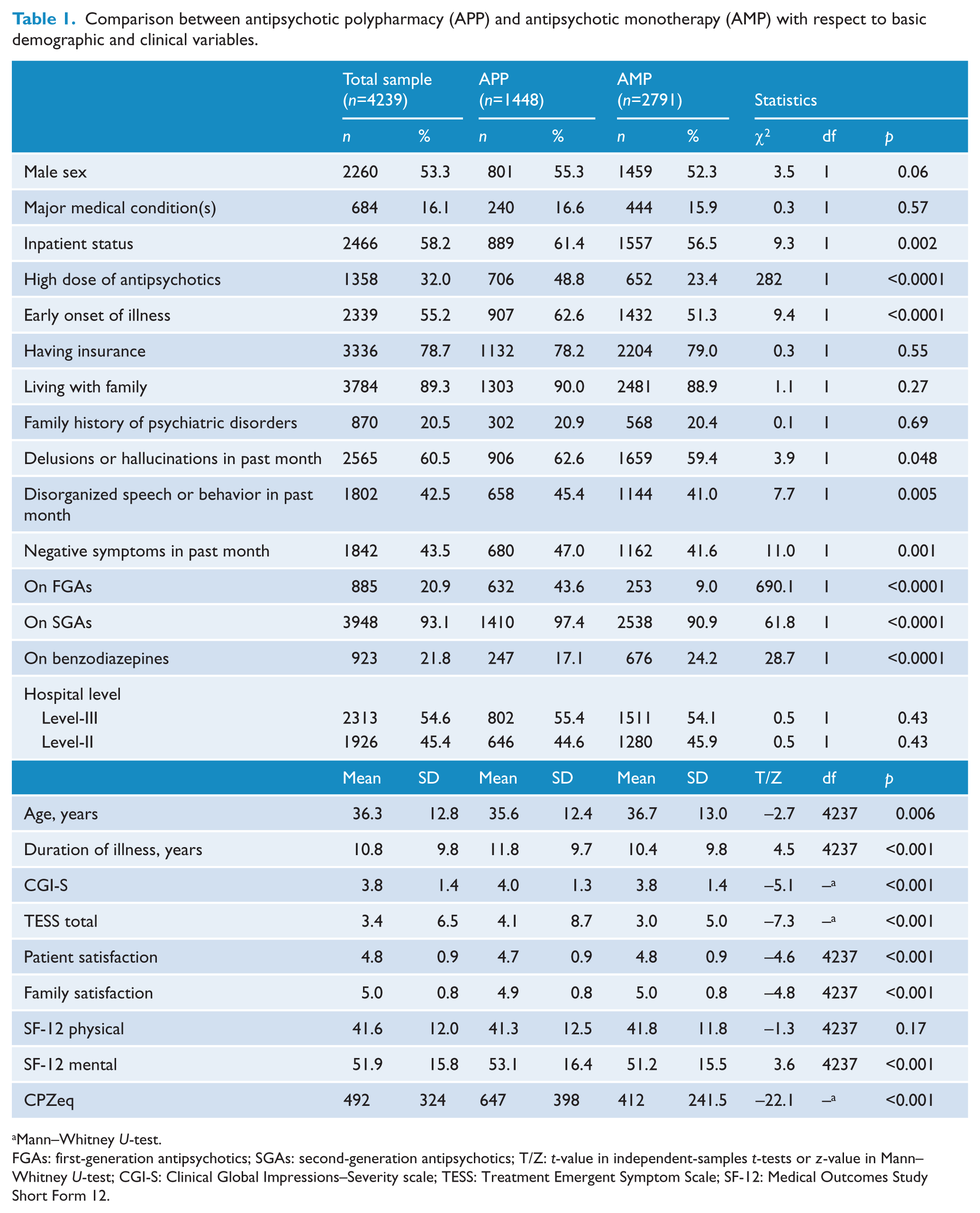
Mann–Whitney U-test.
FGAs: first-generation antipsychotics; SGAs: second-generation antipsychotics; T/Z: t-value in independent-samples t-tests or z-value in Mann–Whitney U-test; CGI-S: Clinical Global Impressions–Severity scale; TESS: Treatment Emergent Symptom Scale; SF-12: Medical Outcomes Study Short Form 12.
Table 2 shows the prescribing patterns for the number of antipsychotic drugs, combined use by antipsychotic class, and of individual antipsychotics across the three surveys. Overall, the frequency of APP increased significantly from 2002 (26.1%) and 2006 (26.4%) to 34.2% in 2012 (p<0.001). The combinations of SGAs with SGAs increased significantly, while the combinations of FGAs with FGAs and FGAs with SGAs decreased over time.
Comparison of prescribing pattern of antipsychotics in the three national surveys on use of psychotropic medications (Si et al., 2004; Zhang et al., 2012).
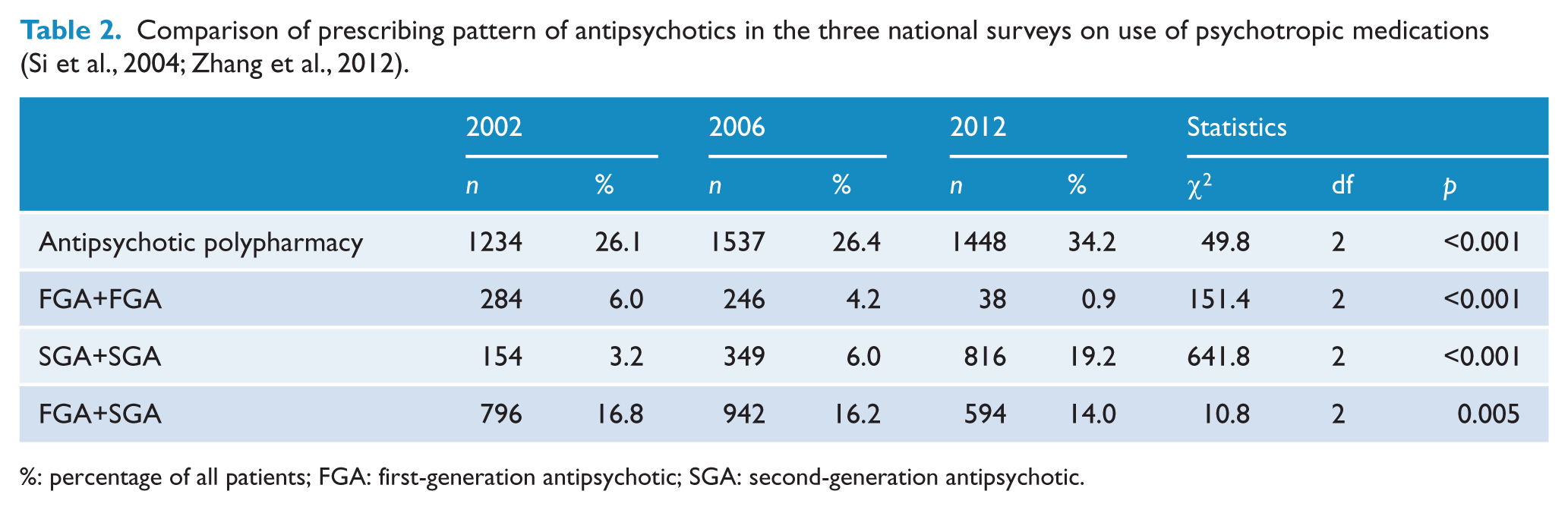
%: percentage of all patients; FGA: first-generation antipsychotic; SGA: second-generation antipsychotic.
Table 3 presents the frequently prescribed antipsychotic drugs in the 2012 survey. Risperidone and clozapine were the most commonly prescribed SGAs, while sulpiride and chlorpromazine were the most commonly prescribed FGAs. Table 4 displays the factors independently associated with APP in logistic regression analyses. Patients on APP had an earlier age of onset, more side effects, higher doses of antipsychotics and were more likely to receive FGAs, but less likely to receive BZDs. Together these variables account for 31.0% of the variance of APP use (p<0.001).
The five most commonly prescribed SGAs and FGAs in China in 2012.
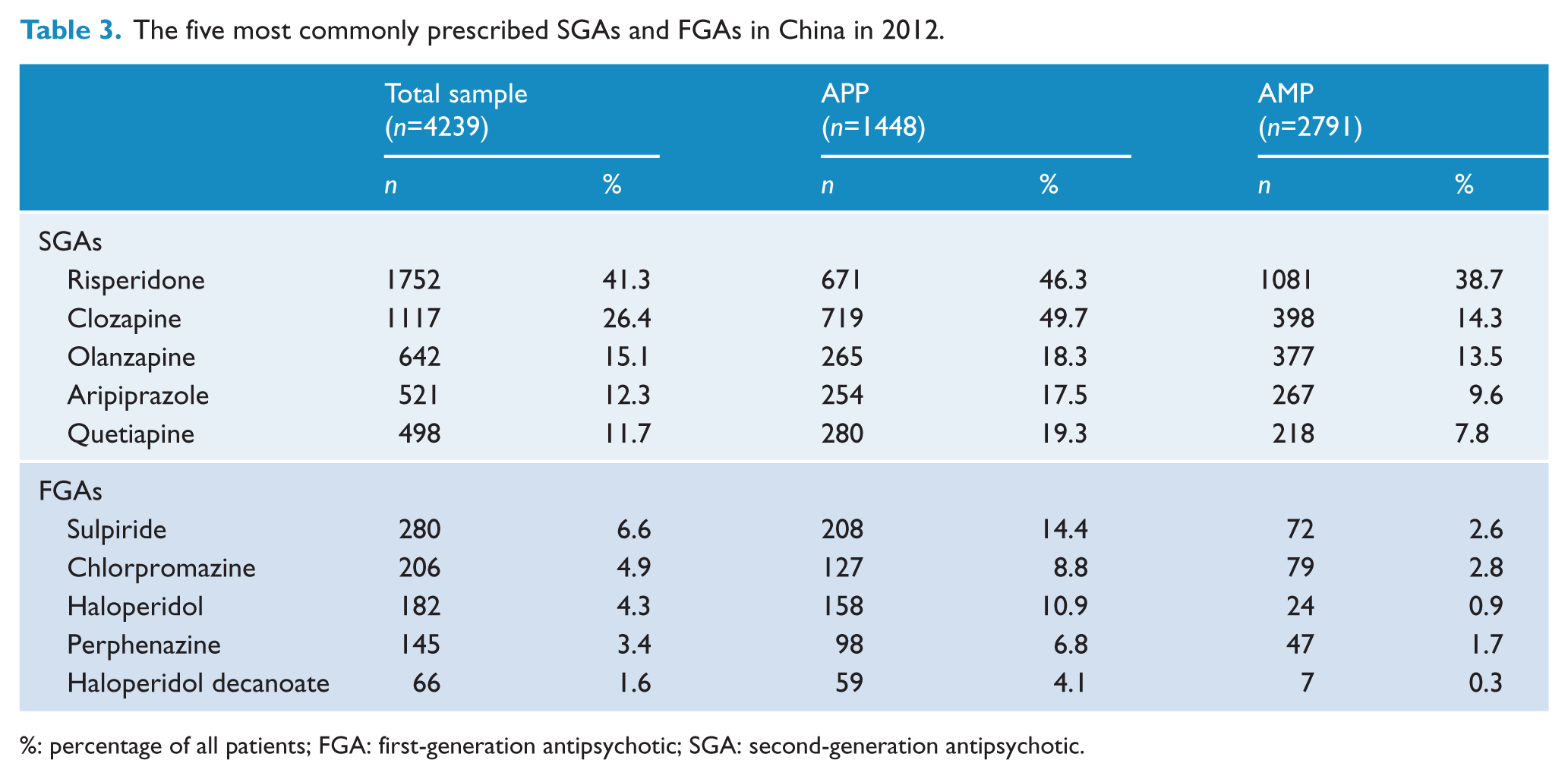
%: percentage of all patients; FGA: first-generation antipsychotic; SGA: second-generation antipsychotic.
Factors associated with antipsychotic polypharmacy (n=4239). Multiple logistic regression analysis with antipsychotic monotherapy as the reference group. a
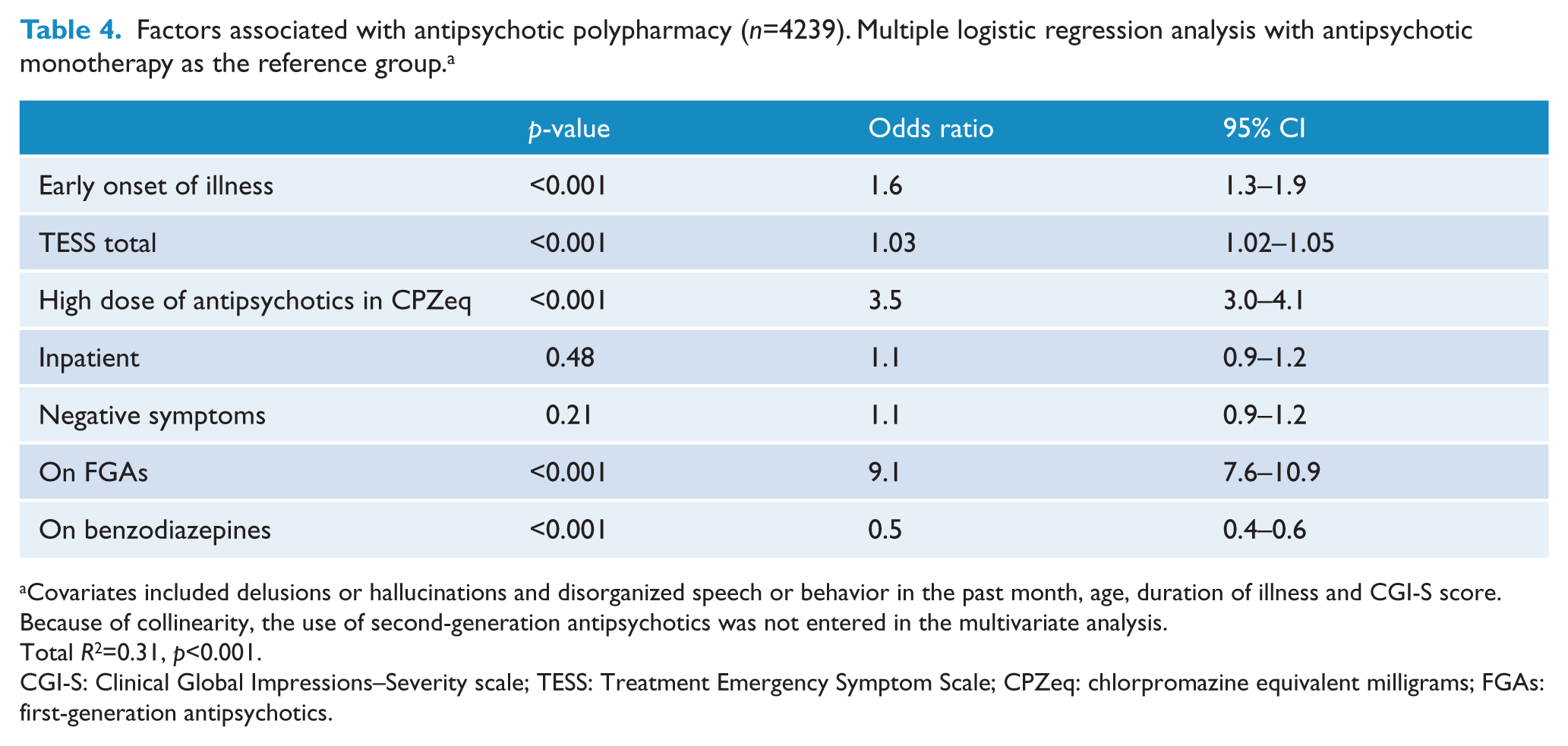
Covariates included delusions or hallucinations and disorganized speech or behavior in the past month, age, duration of illness and CGI-S score. Because of collinearity, the use of second-generation antipsychotics was not entered in the multivariate analysis.
Total R2=0.31, p<0.001.
CGI-S: Clinical Global Impressions–Severity scale; TESS: Treatment Emergency Symptom Scale; CPZeq: chlorpromazine equivalent milligrams; FGAs: first-generation antipsychotics.
Discussion
Approximately one-third of Chinese schizophrenia patients received APP in 2012 according to this study. This frequency was significantly higher than the findings in 2002 and 2006 when about one-quarter of Chinese schizophrenia patients received APP. The frequency of APP of 34.2% found in China in 2012 is higher than the frequencies found pooling data from 147 studies in North America (16.0%) and Europe (23.0%), but similar to the pooled frequencies across four decades in Asia (32.0%) (Gallego et al., 2012a). However, the frequency of APP decreased over time, particularly in Asia, with frequencies from 55.5% in 1980 to 19.2% in 2000 (Gallego et al., 2012a). These results, together with the lower APP frequencies in 2002 and 2006 from the same survey in the same regions, suggest that APP may be increasing again in China.
By comparison, in the REAP project that surveyed the prescription trends for psychotropic drugs in schizophrenia inpatients in Asia, the proportion of APP was 46.8% in 2001, 38.3% in 2004 and 43.4% in 2009, while the corresponding figures in China were 25.2%, 23.8% and 35.9% (Sim et al., 2004b; Xiang et al., 2012). However, only four major psychiatric hospitals in China were involved in the REAP surveys, limiting the generalizability of the findings.
APP figures in Asian patients reported in earlier surveys, including ours, were considerably higher than what has been reported for Western patients (Chong et al., 2000; Gallego et al., 2012a; Roh et al., 2014; Xiang et al., 2007a). The common use of APP in Asia may be partly due to the traditional belief that a mixture of different pharmacological compounds is superior to a single one (Chong et al., 2000). APP is mainly prescribed in the treatment of schizophrenia as a last option after other strategies have failed (Suppes et al., 2005). However, data also indicate that APP is used instead of the much more evidence-based switch to clozapine monotherapy (Nielsen et al., 2012). Moreover, as mentioned before, there is only weak evidence supporting the improved efficacy with APP (Barbui et al., 2009; Correll et al., 2009). At the same time, APP can increase adverse effects and cost of treatment and reduce treatment adherence (Gallego et al., 2012b; Mojtabai and Olfson, 2010; Zink et al., 2010). Therefore, treatment guidelines consistently discourage APP (Goff and Dixon, 2011).
Another finding of this study is that APP increased in the same regions in China from 26.1% in 2002 and 26.4% in 2006 to 34.2% by 2012. The frequency of combination FGA+SGA decreased statistically significantly, but not to a clinically relevant extent over the three surveys (16.8% in 2002, 16.2% in 2006 and 14.0% in 2012). In contrast, combinations of FGA+FGA were used only in a minority of patients in 2012 compared to 2002. The frequency of SGA+SGA combinations increased by a clinically relevant level from 3.2% in 2002 to 19.2% in 2012. Thus, the introduction and widespread use of SGAs seems responsible for the increased APP over the past decade. The possible reasons for this trend include the presumably enhanced therapeutic effects of SGAs due to targeting a variety of receptors (Sim et al., 2004b), although this justification lacks robust evidence (Leucht et al., 2013). In addition, SGAs, except for clozapine and risperidone, were not covered by basic health insurance in China until 2005–2006. The wider coverage of health insurance introduced in 2006 may partly explain the higher rate of SGA prescriptions, both in monotherapy and as part of APP.
APP was associated with a number of clinical variables. Similar to the results of the REAP project (Sim et al., 2004a; Xiang et al., 2012) and multiple prior studies (Correll and Gallego, 2012; Roh et al., 2014), APP was associated with higher antipsychotic doses in this study, which may be one reason for the increasing likelihood of more frequent and more severe side effects (Carnahan et al., 2006). As also reported in prior studies (Correll and Gallego, 2012), APP was more often used with FGAs probably because of the assumption that the use of several different antipsychotics may optimize the dopamine-2 receptor occupancy and target various receptors beyond the dopamine-2 receptor (Sim et al., 2004b), although this practice is not borne out by robust research data (Barbui et al., 2009; Cipriani et al., 2009). To the best of our knowledge, higher negative symptomatology in APP patients has only been reported once before (Morrato et al., 2007); this association may either be due to the greater illness severity and functional disability found with negative symptoms that may prompt APP, or could be the result of higher doses in APP subjects resulting in secondary negative symptoms. Since negative symptoms have strong functional implications (Austin et al., 2013), patients on APP with clinically relevant negative symptoms may need to undergo dose reduction in order to distinguish enduring primary from secondary negative symptoms.
BZDs are commonly used adjunctive drugs in schizophrenia administered primarily for anxiety, insomnia and in rapid tranquillization to control psychotic symptoms and agitation (Tor et al., 2011; Xiang et al., 2007b). The sedative effects of APP (Correll et al., 2007) may be responsible for its association with less use of BZDs. Younger age at onset has been associated with APP in one prior study (Millier et al., 2011). This association may be explained by the fact that earlier illness onset is usually correlated with poorer treatment response (Lieberman et al., 1994), which may lead to more use of APP.
Both uni- and multivariate analyses revealed that compared to AMP, APP was associated with poorer patients’ and their families’ satisfaction with treatment, which may be attributed to greater adverse effects, cost of treatment and reduced treatment adherence caused by APP (Gallego et al., 2012b; Mojtabai and Olfson, 2010; Zink et al., 2010). However, the relationship could also be related to the higher illness severity and psychopathology despite APP, resulting in dissatisfaction with the efficacy of the treatment for more resistant illness expressions. According to the distress/protection model of QOL (Voruganti et al., 1998), QOL results from an interaction between protective (e.g. self-esteem and social support) and distressing factors (e.g. severe drug-induced side effects). Owing to the side effects related to APP and its association with greater illness severity and treatment resistance, we hypothesized that patients on APP would have lower QOL than those on AMP. Contrary to expectations, we found that APP was associated with higher QOL in the mental domain and no decreased QOL in the physical domain, despite decreased treatment satisfaction. One possible explanation for this finding is that the majority of patients (90.0% in the APP group and 88.9% in the AMP group) lived with their families. We speculate that social support from family members may explain the better mental health QOL in the APP group. In addition, the possibility cannot be excluded that the SF-12 could not truly reflect QOL. The SF-12 consists of only 12 items, which may limit its validity, although it has been tested in both Chinese and Western populations. These unexpected findings need to be examined in future studies using different measures on QOL.
There are a number of limitations to this study. First, APP was assessed cross-sectionally, which could have inflated the frequencies by counting both long-term and intended APP as well as patients undergoing antipsychotic switching. In a cross-sectional survey the causality of APP use and other variables could not be examined. Second, the reasons for prescribing particular antipsychotics were not explored. There are differences in healthcare schemes, prescribing traditions and treatment guidelines between institutions even within one province or municipality. The confounding effects of these differences could not be addressed. Third, patients who could not understand the contents of the survey were excluded, which might bias the findings to an uncertain extent. Fourth, the conversion of antipsychotic doses into CPZeq is not unequivocally accepted as accurate, particularly for SGAs (Taylor et al., 2003). Fifth, the majority of Chinese schizophrenia patients live in the community (Xiang et al., 2008). In this study, 58.2% of patients were in hospital where they were more likely to have received APP (Correll and Gallego, 2012). Nevertheless, these limitations are partly offset by the study’s strengths, which include its large, homogeneous and representative sample, as well as to earlier study time points for comparison where data were collected with the same design.
In conclusion, about one in three schizophrenia patients received APP in this study. The frequency of APP seems to be increasing recently. Considering the increased likelihood of drug-induced side effects related to APP and patients’ and their families’ dissatisfaction with psychiatric treatment in general – and antipsychotics in particular, further examination of the rationale and appropriateness of APP and its alternatives is warranted.
Footnotes
Acknowledgements
The authors thank clinicians who helped to organize the study in each study site.
Funding
The study was supported in part by grants from the 12th Five-Year Plan of the National Key Technologies R&D Program of China (grant number: 2011ZX09302-004).
Declaration of interest
Dr Correll has been a consultant and/or advisor to or has received honoraria from: Actelion, Alexza, American Academy of Child and Adolescent Psychiatry, Bristol-Myers Squibb, Cephalon, Eli Lilly, Genentech, Gerson Lehrman Group, IntraCellular Therapies, Lundbeck, Medavante, Medscape, Merck, National Institute of Mental Health, Janssen/J&J, Otsuka, Pfizer, ProPhase, Roche, Sunovion, Takeda, Teva, and Vanda. He has received grant support from BMS, Feinstein Institute for Medical Research, Janssen/J&J, National Institute of Mental Health (NIMH), National Alliance for Research in Schizophrenia and Depression (NARSAD), and Otsuka. He has been a Data Safety Monitoring Board member for Cephalon, Eli Lilly, Janssen, Lundbeck, Pfizer, Takeda, and Teva. The remaining authors had no conflicts of interest in conducting this study or preparing the manuscript.