
Abstract
Participants were classified into smokers and non-smokers (which included former and never smokers). We used the Kessler 10 (K10) symptom score to classify smokers into three levels of psychological distress (low, medium or high) and socioeconomic disadvantage was measured using an area-based index of relative disadvantage converted into quintiles.
We used logistic regressions to: (i) examine associations between smoking status (smoker/non-smoker) and psychological distress and socioeconomic disadvantage in 1997 and 2007 surveys; and (ii) to test whether the prevalence of psychological distress and social disadvantage among smokers increased between 1997 and 2007.
The ‘hardening hypothesis’ of smoking suggests that those who continue to smoke cigarettes in the face of strong societal discouragement are more dependent and less likely to quit because the people who find it easy to quit have already done so [1]. This hypothesis predicts that as smoking prevalence decreases, lighter smokers will quit first, leaving a higher proportion of ‘hardcore’ smokers in the population. If the proportion of hardcore smokers is increasing over time, a potential consequence is that more intensive individual level tobacco cessation interventions will be needed to be able to reduce the smoking prevalence in this population [2].
One category of hardcore smoker is those who have a comorbid mental disorder that may make it more difficult for them to quit. High levels of comorbidity between smoking, substance use, anxiety and affective disorders and psychosis have been found in surveys of clinical populations [3] and epidemiological studies, in Australia and internationally [4,5]. Longitudinal studies [6,7] suggest that individuals who are anxious and depressed are more likely to smoke and smokers with mental disorders experience more difficulty quitting [8,9] (for an exception see El-Guebaly et al. [10]). The higher rates and heavier levels of smoking among people with mental illness [3] places them at an increased risk of developing tobacco-related diseases [9].
Some studies have reported a slower decline in smoking prevalence in the economically disadvantaged compared to the advantaged, because the advantaged are less likely to start smoking and more likely to quit if they do smoke [11]. This has been referred to as the social gradient of smoking. Socially disadvantaged smokers may be considered ‘harder’ because they tend to have higher levels of exposure to smoking (e.g. passive smoking) [12], and may be more resistant to public health interventions discouraging smoking [13].
The prevalence of smoking in the Australian population declined by about 2% between 1997 to 2007 in the two National Surveys of Mental Health and Well-Being (NSMHWB). The impact of this decline on the prevalence of mental disorders in smokers has not been examined. If the ‘hardening hypothesis’ is correct, those who still smoke cigarettes in 2007 will be more nicotine dependent and more likely to have a mental disorder that makes them less able to quit [14]. This hypothesis predicts that symptoms of depressive and anxiety disorders will be more prevalent in current (and continuing) smokers [15] in 2007 than in 1997.
In Australia, it is unclear whether the social gradient in smoking has increased over the last decade. One recent analysis of the social gradient in smoking in the 1989/1990 and 2001 Australian National Health Surveys [16] found an increasing social gradient of smoking only in males. Among males, the rate of decline in smoking prevalence was higher in the most socioeconomically advantaged quintile than in the least advantaged quintile. Similarly, analyses of Australian National Drug Strategy Household data from 1998, 2001 and 2004 showed larger declines in the prevalence of smoking in the most socioeconomically advantaged quintile than in the least disadvantaged quintile, although formal statistical testing of the changes in social gradient were not undertaken (cited in Scollo and Siahpush [12]). No further analyses of changes in the social gradient of smoking in Australia have been undertaken.
This paper examines whether psychological distress and socioeconomic disadvantage are more prevalent in Australian smokers compared to non-smokers in 2007 than in 1997. We used data from the 1997 and 2007 NSMHWB to address these questions. These surveys examined the prevalence of common substance abuse and mental disorders and risk factors such as smoking in a representative sample of the Australian population. Specifically, we compared the characteristics of current smokers in the 1997 and 2007 NSMHWB on: psychological distress and measures of social disadvantage. Ideally we would have compared the prevalence of DSM-IV mental disorders among smokers but major changes in the way these disorders were assessed between 1997 and 2007 precluded such comparisons (these included, differences in the time frame for reporting symptoms (past 12 months versus lifetime) and a larger number of anxiety disorders were assessed in 2007 than in 1997).
Method
Sample
Both the 1997 and 2007 NSMHWB interviewed multistage probability samples of English-speaking Australians living in private dwellings. The 1997 sample comprised 10 373 persons aged 20 to 85 years and the 2007 sample comprised 8135 20 to 85 year olds. The response rate was lower in 2007 (60%) than in 1997 (78%). A non-response follow-up study conducted of participants in the 2007 survey concluded it may have underestimated the prevalence of mental disorders in men, youths and the Perth population, but the difference in prevalence was likely to be small [17]. Information on the sampling design and methods for the 1997 and 2007 NSMHWB are published elsewhere [17–19].
Measures
Smoking status
Participants were asked whether they never, formerly or currently smoked tobacco. Current smokers included those who smoked daily, weekly, or less than weekly. Former and never smokers were coded as non-smokers (0) and current smokers were coded as smokers (1).
Psychological distress
Psychological distress was measured using the Kessler 10 (K10), a 10-item scale which assesses symptoms of nervousness, restlessness and depressed affect in the last 4 weeks (1997)/30 days (2007). Higher scores indicate higher levels of psychological distress [20]. Respondents who scored 10 to 15 were coded as having low distress, those between 16 and 29 had medium distress, and those between 30 and 50 had high distress [21].
Socioeconomic disadvantage
Socioeconomic disadvantage was measured using an index of relative socioeconomic disadvantage converted into quintiles. This is an area-based measure of disadvantage. For more details on this index refer to the Australian Bureau of Statistics [22].
Data analysis
Prevalence estimates of psychological distress and socioeconomic disadvantage (quintile) according to smoking status (current versus non-smoker) were calculated for all respondents after application of replicate weights which adjusted for demographic strata and clusters in the representative samples.
Logistic regressions were used to compare differences in the odds of smoking according to psychological distress and index of relative disadvantage quintile for each survey year (1997 and 2007). For regressions using the index of relative disadvantage as predictor, the lowest quintile was the reference group. For regressions using psychological distress as a predictor, low distress was used as the reference group. Given psychological distress tends to be more prevalent in the economically disadvantaged [23], we ran sensitivity analyses adjusting for socioeconomic disadvantage.
To examine differences between 1997 and 2007 in the prevalence of smoking according to psychological distress and socioeconomic disadvantage, we combined the 1997 and 2007 data sets and tested whether the addition of interaction products between each of the independent variables and survey year (1997 versus 2007) (i.e. psychological distress by survey year and index of relative disadvantage quintile by survey year) improved the fit of our models. All analyses used unweighted data and adjusted for age and sex as both these factors are correlated with smoking and psychological distress [24].
Results
Psychological distress among smokers
The prevalence of psychological distress according to smoking status (smokers versus non-smokers) in 1997 and 2007 surveys are presented in Table 1. The associations between smoking status and psychological distress after adjusting for age and sex are presented in Table 2.
Prevalence of smoking according to level of psychological distress: 1997 and 2007
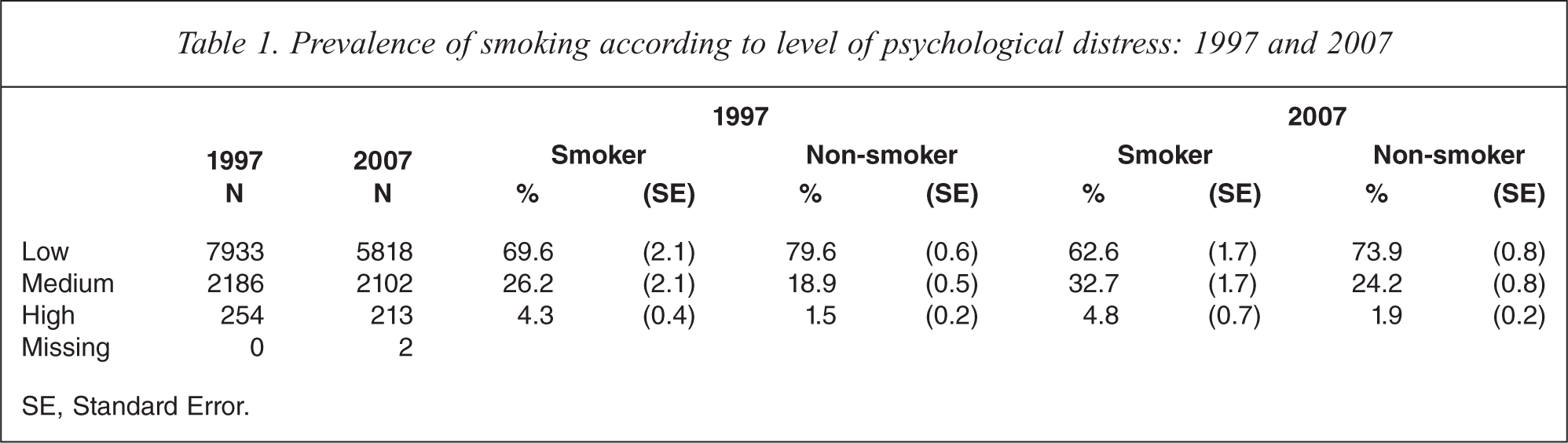
SE, Standard Error.
Odds ratios of smoking according to psychological distress: 1997 and 2007
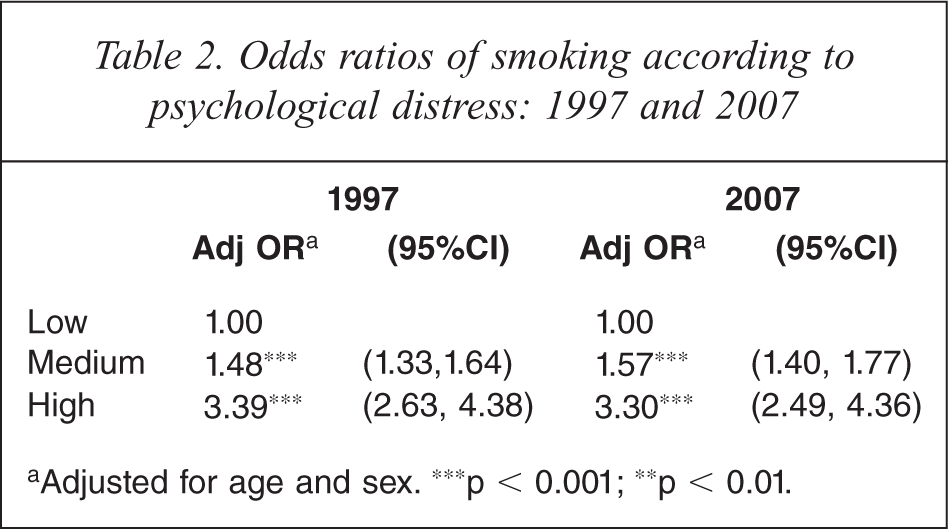
aAdjusted for age and sex. ∗∗∗p < 0.001; ∗∗p < 0.01.
Medium and high psychological distress were more common among smokers than non-smokers in both survey years, while low psychological distress was more prevalent among non-smokers.
Individuals with high levels of psychological distress had around three times higher odds of being a smoker than those with low psychological distress in both 1997 and 2007. Persons with medium psychological distress had about 1.5 times higher odds of being a smoker compared to those with low psychological distress in both years. These associations were maintained after adjusting for socioeconomic disadvantage.
There was no significant interaction between survey year and psychological distress in predicting smoking status. This indicates that there was no difference between survey years in the prevalence of psychological distress among smokers.
Socioeconomic disadvantage among smokers
The prevalence of socioeconomic disadvantage according to smoking status (smokers versus non-smokers) in 1997 and 2007 surveys is presented in Table 3. The association between smoking status and socioeconomic disadvantage after adjusting for age and sex is presented in Table 4.
Prevalence of smoking according to level of disadvantage (quintile): 1997 and 2007
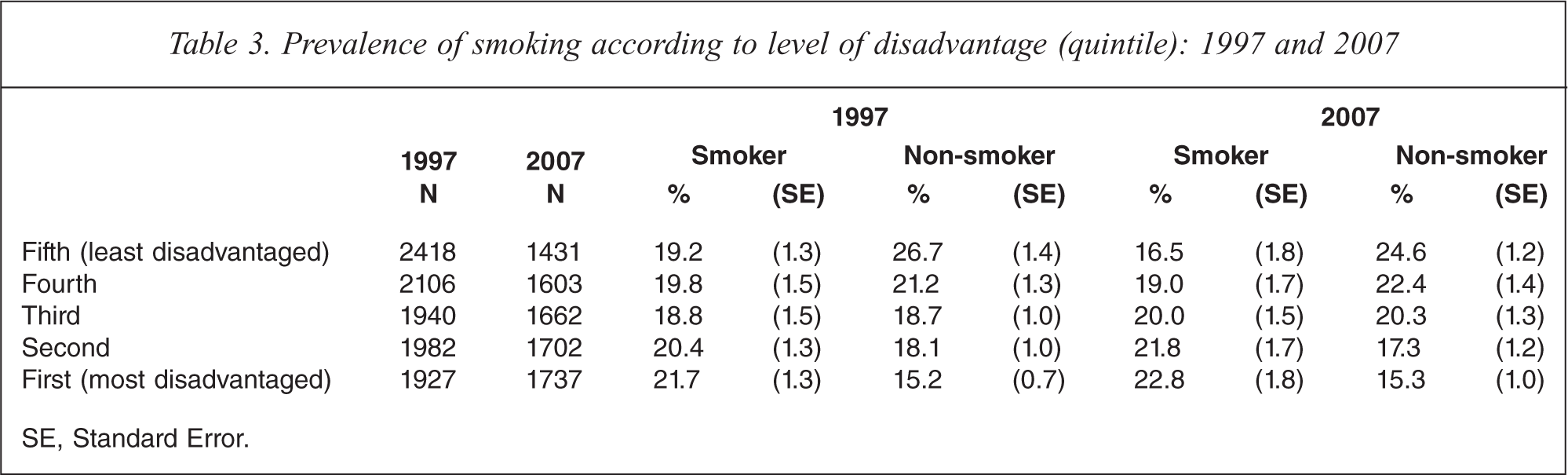
SE, Standard Error.
Odds ratios of smoking according to index of relative disadvantage (quintile): 1997 and 2007
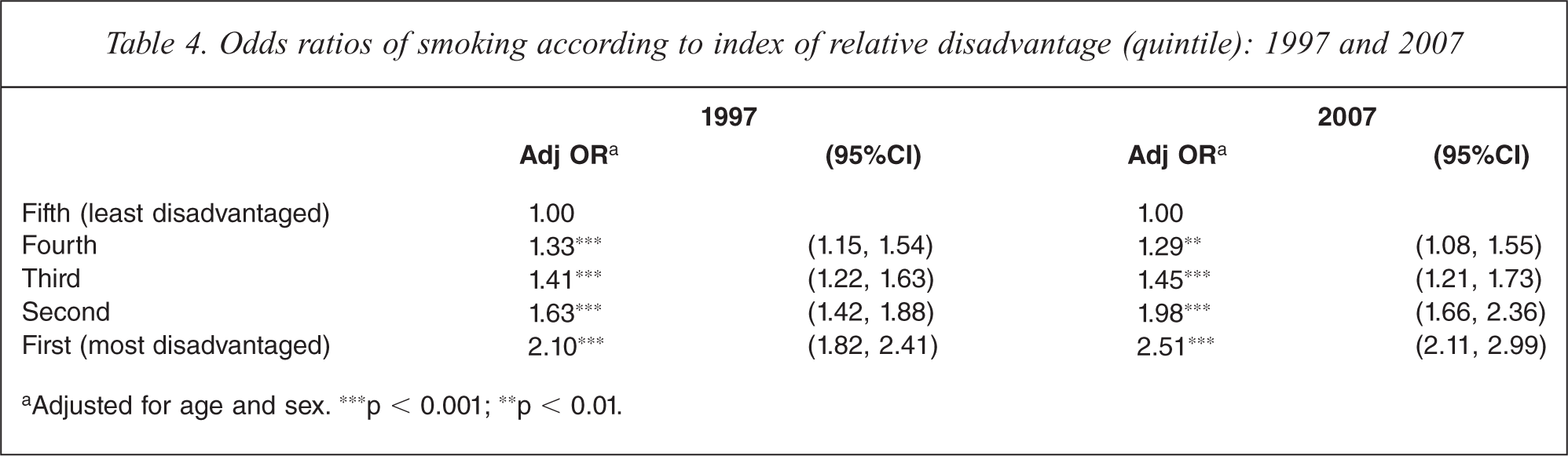
aAdjusted for age and sex. ∗∗∗p < 0.001; ∗∗p < 0.01.
In both years, smoking was most common in persons from the most disadvantaged quintile (21.7% in 1997 and 22.8% in 2007). In contrast, non-smokers were most common among persons in the least disadvantaged quintile (26.7% in 1997 and 24.6% in 2007) in both years.
Logistic regressions showed a significant socioeconomic gradient of smoking in both survey years. Individuals from the most disadvantaged (first) quintile were twice as likely to smoke than those in the least disadvantaged (fifth) quintile in 1997, and two and half times more likely in 2007.
Individuals from the second most disadvantaged (second) quintiles were about 1.6 times more likely to smoke than those in the least disadvantaged (fifth) quintile in 1997 and almost twice as likely in 2007.
Individuals from the third quintile were about 1.4 times more likely than those in the fifth quintile in both years. There was only a marginal difference in smoking prevalence between the fourth and fifth quintiles in both years, with those from the fourth quintile about 1.3 times more likely to smoke than those in the least disadvantaged quintile.
There was a significant interaction between survey year and disadvantage in predicting smoking status p < .05. In the two most disadvantaged quintiles, the association between disadvantage and smoking was larger in 2007 than in 1997. There were no other significant interactions.
Discussion
We found, as have others, that smoking was more common among those with medium and high psychological distress than those with low psychological distress. These patterns were observed in both surveys. We also found a socioeconomic gradient in smoking in both surveys which was consistent with previous research [25]. This confirms that socially disadvantaged persons with mental disorders continue to be over-represented among smokers and reinforces the need for smoking cessation and public health interventions to better target these smokers.
However, we found no evidence of an increase between the surveys in the prevalence of psychological distress among smokers. This suggests smokers in 2007 do not appear to be any ‘harder’ in terms of comorbid mental distress than in 1997. There was, however, some evidence to suggest the prevalence of smoking decreased from 1997 to 2007 in the two least disadvantaged quintiles, but it did not appear to significantly change in the more disadvantaged quintiles over this period.
Limitations
In addition to psychological distress and economic disadvantage, there are a number of other potential indicators of hardening that we were unable to examine. These include: number of cigarettes smoked per day, time to first cigarette in the morning, number of attempts to quit smoking in the past year, and intentions to quit smoking [26]. These variables were not included in the National Surveys of Mental Health and Well-Being so it was not possible to explore them in our study. Due to major changes in the way that DSM-IV mental disorders were assessed between the 1997 and 2007 surveys, we were also unable to compare the prevalence of these disorders and other substance abuse among smokers and non-smokers between surveys.
Cross-sectional survey data do not permit us to determine whether smoking is a cause or consequence of psychological distress or socioeconomic disadvantage. Longitudinal studies would provide stronger evidence of the relationships between smoking, common mental disorders and lower socioeconomic status.
Conclusion
We find no evidence that the decline in the prevalence of smoking in Australia between 1997 and 2007 has been accompanied by any ‘hardening’ of continuing smokers as assessed by rates of psychological distress and socioeconomic disadvantage.
We did find that smokers do continue to be disproportionately affected by mental disorders and socioeconomic disadvantage. From a public policy perspective, this finding highlights that smokers with a mental disorder or socioeconomic disadvantage are important targets for tobacco control interventions.
Footnotes
Acknowledgements