
Abstract
Objective:
This study aimed to identify factors associated with the high rates of smoking amongst people with psychosis living in a disadvantaged region in Adelaide, South Australia.
Methods:
Data were collected from 402 people with psychosis, aged 18–64 years, who lived in the northern suburbs of Adelaide. This area is disadvantaged on many measures of socioeconomic well-being and people living in this region have higher rates of smoking compared to the general Australian population. We hypothesised that whilst tobacco use by people with psychosis living in this region was primarily associated with mental illness, factors related to social disadvantage also contributed to the high rates of smoking.
Results:
Approximately 74% of men and 71% of women with psychotic disorders living in the northern suburbs of Adelaide were current smokers. Factors such as unemployment, lower levels of education and receiving government welfare, factors known to be associated with smoking in the general population, were more prevalent in the northern region. Smokers with psychosis were less likely to participate in recreational programs and physical activity, and more likely to use illicit substances and be a victim of crime. They had poorer health and financial outcomes than non-smokers. There were some gender differences: for men with psychosis, employment and having a post-school qualification decreased the risk of smoking while cannabis use increased the risk; for women with psychosis, a diagnosis of alcohol abuse/dependence, using cannabis and being sedentary were risk factors for smoking, while attending recreational programs reduced this risk.
Conclusion:
Smoking rates were strikingly high in both men and women, and particularly high in women when compared with previous research. Our study shows that the risk of smoking is increased by factors related to the social disadvantage of living in the northern Adelaide region. Smoking cessation interventions for people with mental illness should take into account the social context, and also address relevant comorbidities such as drug and alcohol disorders.
Introduction
Approximately 23% of men and 19% of women in Australia are current smokers (Australian Bureau of Statistics (ABS), 2012). Tobacco smoking in Australia is responsible for 23% of deaths and accounts for 8% of the total burden of disease and injury (Begg et al., 2007). To counter this, public health policies and interventions have attempted, with some success, to reduce tobacco use (Australian Institute of Health and Welfare (AIHW), 2011a). However, rates of smoking have remained relatively unchanged for people living with psychosis (de Leon and Diaz, 2005; Morgan et al., 2011).
Lower socioeconomic status is linked to smoking in Australia (Miller and Hickling, 2004) and throughout the world (Kaleta et al., 2012). In South Australia, 32% of people living in socially disadvantaged areas are current smokers, compared to 20% of people who live in more privileged areas (Kriven and Miller, 2000). In Australia, smoking is associated with unemployment, below high school education, living in lower income households (Scollo and Winstanley, 2008) and substance use (AIHW, 2011b).
Recent Australian studies reported that 77% of people with a first episode of psychosis (Wade et al., 2005) and 62% of people attending a psychiatric rehabilitation program (Moeller-Saxone, 2008) were current smokers. International studies have similarly demonstrated a higher prevalence of smoking in people with psychosis (de Leon and Diaz, 2005). Whilst smoking does appear to be closely linked to psychosis, perhaps via a shared genetic liability (Novak et al., 2009), most people with psychosis live in disadvantaged circumstances, and it is possible that social factors might also contribute to their very high rates of smoking.
Demographic factors including male gender (Salokangas et al., 2006), single marital status (Dodd et al., 2010), receiving government welfare and unemployment (Keizer et al., 2009) have all been associated with smoking in people with psychosis and are similar to determinants of smoking in the general population (Scollo and Winstanley, 2008). Other factors such as living in a residential facility or shelter (Johnson et al., 2010) and having a diagnosis of schizophrenia (de Leon and Diaz, 2005) have been linked to smoking in people with severe mental illness. Johnson et al. (2010) examined gender differences in people with serious mental illness and found that male smokers were likely to have an education level below year 12, be separated or divorced and be older (aged 50–59 years), while for women, living in supported accommodation and younger age (17–29 years) were associated with current smoking. People who have schizophrenia and smoke tobacco have even lower physical activity levels than non-smokers, along with a poorer diet, higher risk of developing cardiovascular disease (Bobes et al., 2010) and lower satisfaction with their health and social relationships (Dixon et al., 2007). In addition, the relationship between alcohol and substance abuse and smoking in people with mental illness is well known (Koola et al., 2012; Sara et al., 2012). Smokers endure financial hardship, often resulting in a lack of food and other necessities (Steinberg et al., 2004).
The northern suburbs of Adelaide
The outer northern suburbs of Adelaide are amongst the most disadvantaged regions in Australia (ABS, 2013) and therefore provided a suitable setting to examine the relationships between social and demographic factors and smoking in people with psychosis. In 2000, 32% of people living in this area were current smokers compared to western (22%), southern (21%) and eastern (20%) regions of Adelaide (Kriven and Miller, 2000). While northern smoking rates decreased to 24% in 2004–2006, this was still higher than both the national average rate (AIHW, 2011a) and the rates in other South Australian regions (Jury et al., 2007).
In the northern region, a higher proportion of residents live in housing trust accommodation compared to the rest of Adelaide (Jury et al., 2007; Spoehr et al., 2007). Twenty-two percent of northern residents earned only AU$20,000–40,000 per year compared to the whole of Adelaide (18%) (Jury et al., 2007). Northern unemployment rates (19% in some postcodes) are consistently amongst the highest in urban Australia (ABS, 2012). Although 66% of people in the northern region had completed secondary school, only 34% pursued tertiary education or obtained a Technical and Further Education (TAFE) or trade qualification compared to 43% for South Australia as a whole. There was a tendency towards women remaining unemployed and having lower high school completion rates compared to men.
People living in the northern area also have poorer health outcomes compared to other regions, illustrated by the higher rates of respiratory disease (7% in the north and 4% in central and eastern Adelaide) (Jury et al., 2007). People living with mental illness make up 15.2% of the northern population, which is higher than other metropolitan and rural regions in Adelaide (11.9–15.1%; Jury et al., 2007). Drug use (Spoehr et al., 2007) and criminal offences committed against residents are both more common in the north compared to other parts of Adelaide (Office of Crime Statistics and Research, 2011).
It has been suggested that within this context, smoking is a coping mechanism to manage the hardships of daily life (Cancer Council NSW, 2008). It can be hypothesised that in the northern suburbs of Adelaide, social deprivation increases the likelihood of smoking and, conversely, smoking reinforces disadvantage (Cancer Council NSW, 2008). Despite the social disadvantages described above, northern residents have frequent social interaction with friends and neighbours (Spoehr et al., 2007), which may partly mitigate poor physical and mental health. However, their low involvement in community programs (29%) (Spoehr et al., 2007) suggests that residents prefer informal interaction with their neighbours and friends to more structured events in the wider community.
The current study
This study was undertaken to explore the reasons for the high rates of smoking in people with psychosis living in the northern suburbs of Adelaide. We investigated this question by examining the social context in which these people lived. Indicators of social disadvantage were derived from two reports by the Department of Health that assessed the socio-demographic characteristics of the northern region (Jury et al., 2007; Spoehr et al., 2007). We identified factors associated with higher rates of smoking in the general population, looked at whether these factors were more prevalent in the northern suburbs of Adelaide, and then examined whether they were linked to smoking in people with psychosis living in this region. We also undertook separate regression analyses to determine whether these factors predicted smoking in men and women with psychosis.
Method
Participants and procedure
Data from 402 participants with psychotic disorders, living in the Northern Mental Health catchment region in South Australia, were collected during the second Australian national survey of people living with psychotic illness. A detailed description of the method has been published by Morgan et al. (2011). The study consisted of a two-phase sampling design. In phase 1, people aged 18–64 years in contact with public mental health services in the previous 12 months were screened for psychosis. In phase 2, all 1215 screen-positive participants were contacted (if possible) and invited to participate in the survey, resulting in 402 completed interviews (33%). The Queen Elizabeth Hospital research ethics committee approved the study and written informed consent was provided by all participants.
Measures
Smoking variables
Lifetime tobacco use was measured by asking participants if they had ever regularly smoked cigarettes, tobacco, cigars, or a pipe. Participants were classified as current smokers if they had smoked in the previous 4 weeks. Those answering no to this question were considered non-smokers (comprising never smokers and ex-smokers). Information regarding smoking history and quit attempts was also obtained. Nicotine dependence was measured using the Fagerstrom Test for Nicotine Dependence (Fagerstrom et al., 1990).
Demographic data
Information was collected relating to gender, age, marital status, accommodation, level of education, and age at leaving school. Formal study in the past year included any enrolment in school, TAFE, university and colleges/institutes of advanced education. Current employment was recorded for the last 7 days and included both part-time and full-time paid work. Fortnightly income was recorded as: (1) AU$499 or less; (2) between AU$500 and AU$799; and (3) AU$800 or more; and participants were asked whether they received government benefits as their main source of income. Independent living included residing in public/private rental or owning own home and non-independent living included living with family and supported accommodation / institution / hospital. The Diagnostic Interview for Psychoses (DIP) was used to make diagnoses according to International Classification of Diseases (ICD)-10 criteria (Castle et al., 2006).
Physical health
Physical activity was assessed using the International Physical Activity Questionnaire (IPAQ; Craig et al., 2003). Physical health variables including weight, height, self-reported respiratory or cardiovascular problems, blood pressure, cholesterol levels and criteria for the presence of metabolic syndrome were collected. The methods for the assessment of obesity and metabolic syndrome have been reported elsewhere (Galletly et al., 2012).
Social participation
Attendance at social and recreational programs in the past year included any participation in community events or organised sport.
Financial difficulties and physical health
Financial difficulty was measured from questions drawn from the 2007 National Survey of Mental Health and Wellbeing (Slade et al., 2009) and included items about being able to heat or cool home/room, going without meals, or having pawned or sold something in the past year due to shortage of money.
Substance use and criminal activity
Respondents were asked how often they had used alcohol, cannabis, amphetamines and other drugs in the past year and were classified into (1) not used; (2) monthly or less than monthly; and (3) weekly/daily (Castle et al., 2006). Alcohol dependence and risk categories were measured using the Alcohol Use Disorders Identification Test (AUDIT; Saunders et al., 1993). Lifetime diagnoses of alcohol abuse / dependence, cannabis abuse /dependence and other substance abuse / dependence were assessed using the DIP (Castle et al., 2006). Caffeine consumption was measured as the quantity of caffeinated drinks consumed per day on average in the past 4 weeks. Respondents were asked if they had been a victim of actual or threatened assault in the past year (Australian National Health Survey; ABS, 2001).
Statistical analyses
Bivariate analyses were performed using SPSS (version 19; IBM Corp., 2010). A significance level of p < 0.05 was used for all analyses. To explore the differences between smokers and non-smokers, independent t-tests were used for continuous variables and chi-squared tests or Fisher exact tests were used for categorical variables.
A binary logistic regression was performed to explore gender differences in predictors of smoking. The data were stratified by gender and variables with cell counts of less than 5 were excluded from the regression. The variables chosen for the regression analysis were variables that were significant from previous analyses in the current study and variables that were appropriate or significant from past research. These variables were added simultaneously into the regression analysis.
Results
Table 1 presents the demographic and diagnostic characteristics of the sample. Table 2 shows 290 (73%) of the total sample smoked − 171 (74%) of men and 119 (71%) of women. Smokers were more likely to have less education, be unemployed and have a lower income. Men smoked more cigarettes daily, but reported more quit attempts.
Demographic and diagnostic characteristics of current smokers and current non-smokers with psychosis living in northern Adelaide.
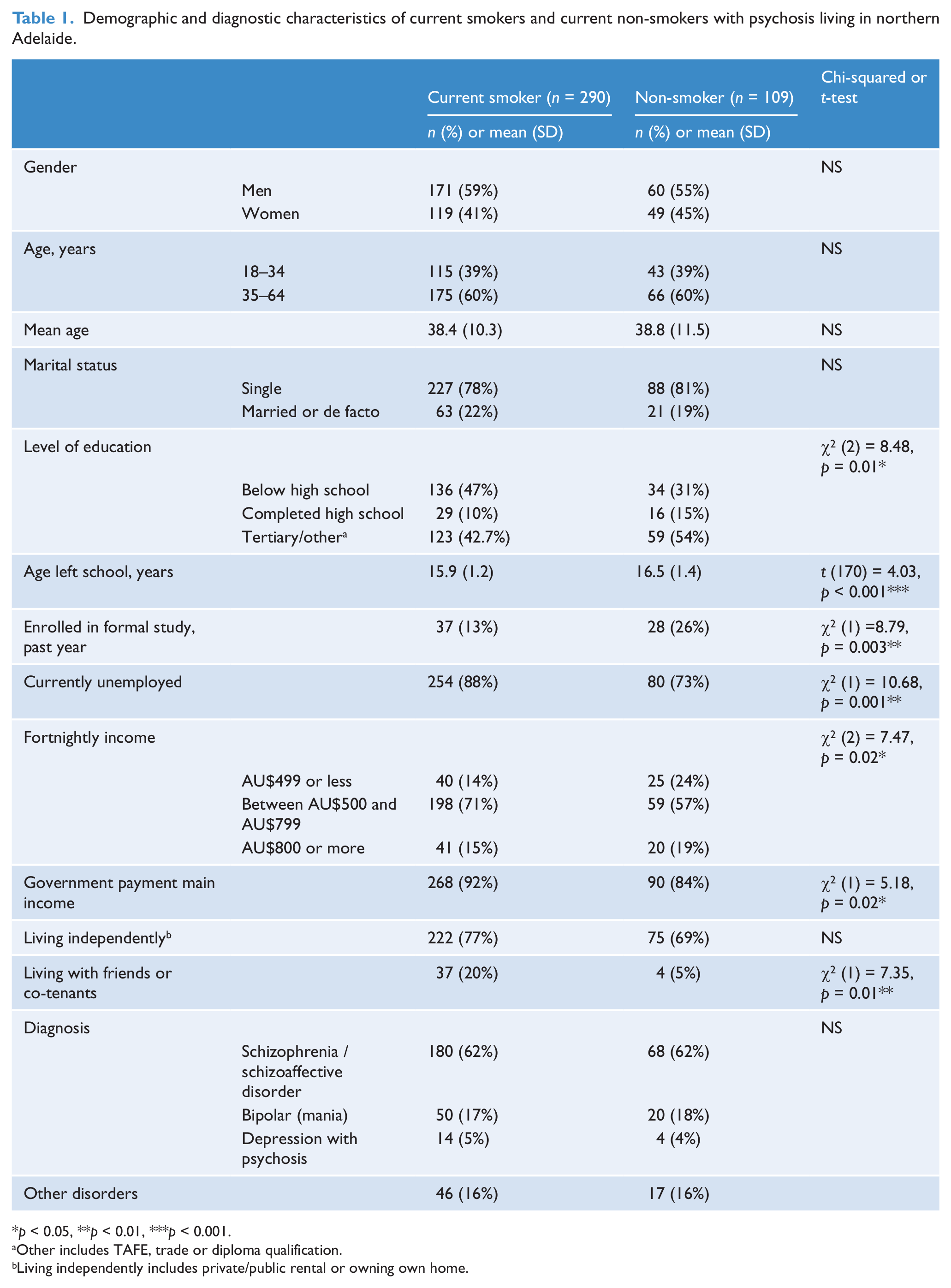
p < 0.05, **p < 0.01, ***p < 0.001.
Other includes TAFE, trade or diploma qualification.
Living independently includes private/public rental or owning own home.
Smoking history for men and women with psychosis living in northern Adelaide.
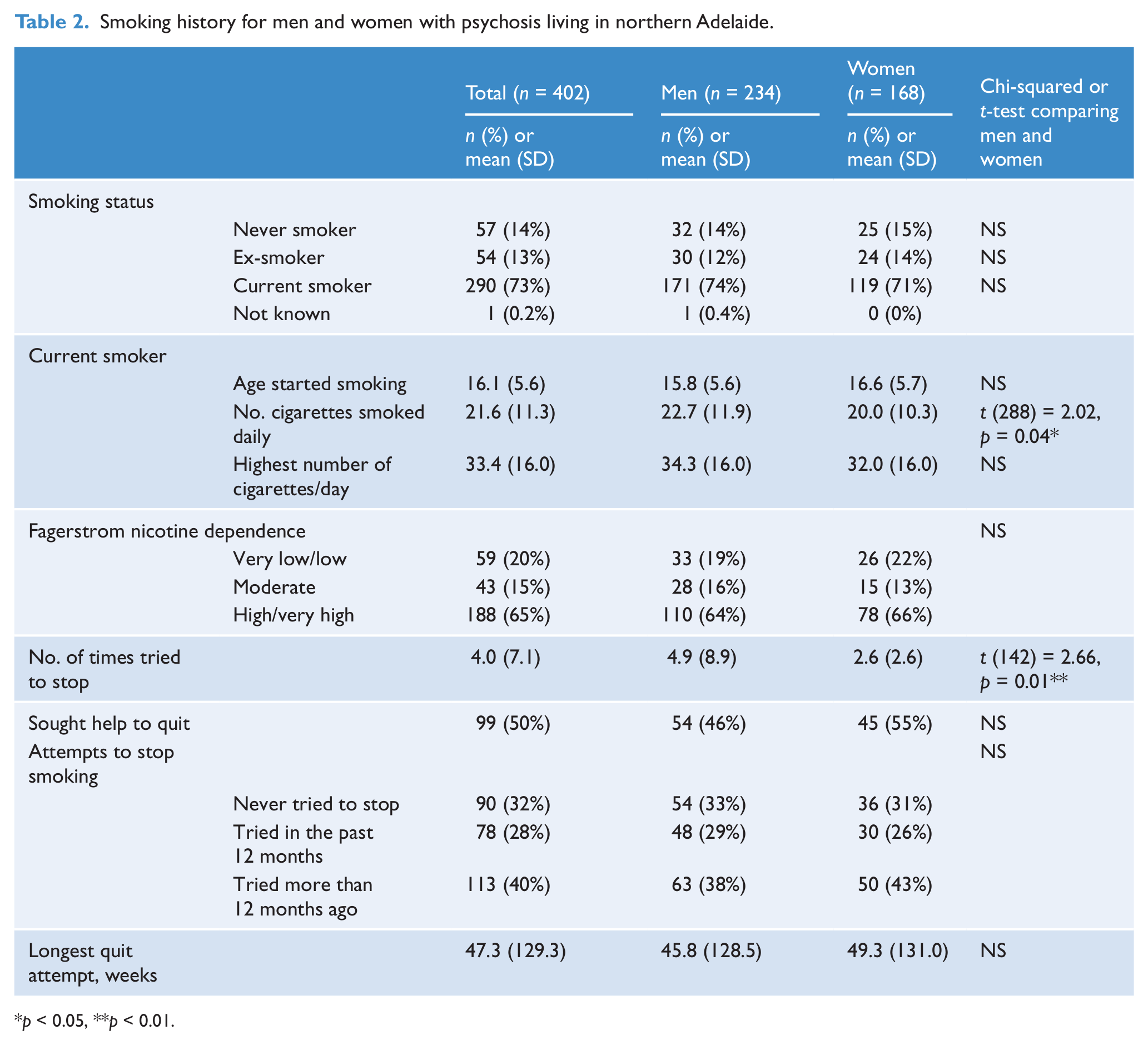
p < 0.05, **p < 0.01.
Smokers were significantly less likely to attend social and recreational programs or to undertake moderate or vigorous activity (Table 3).
Social participation and physical activity for current smokers and current non-smokers with psychosis.
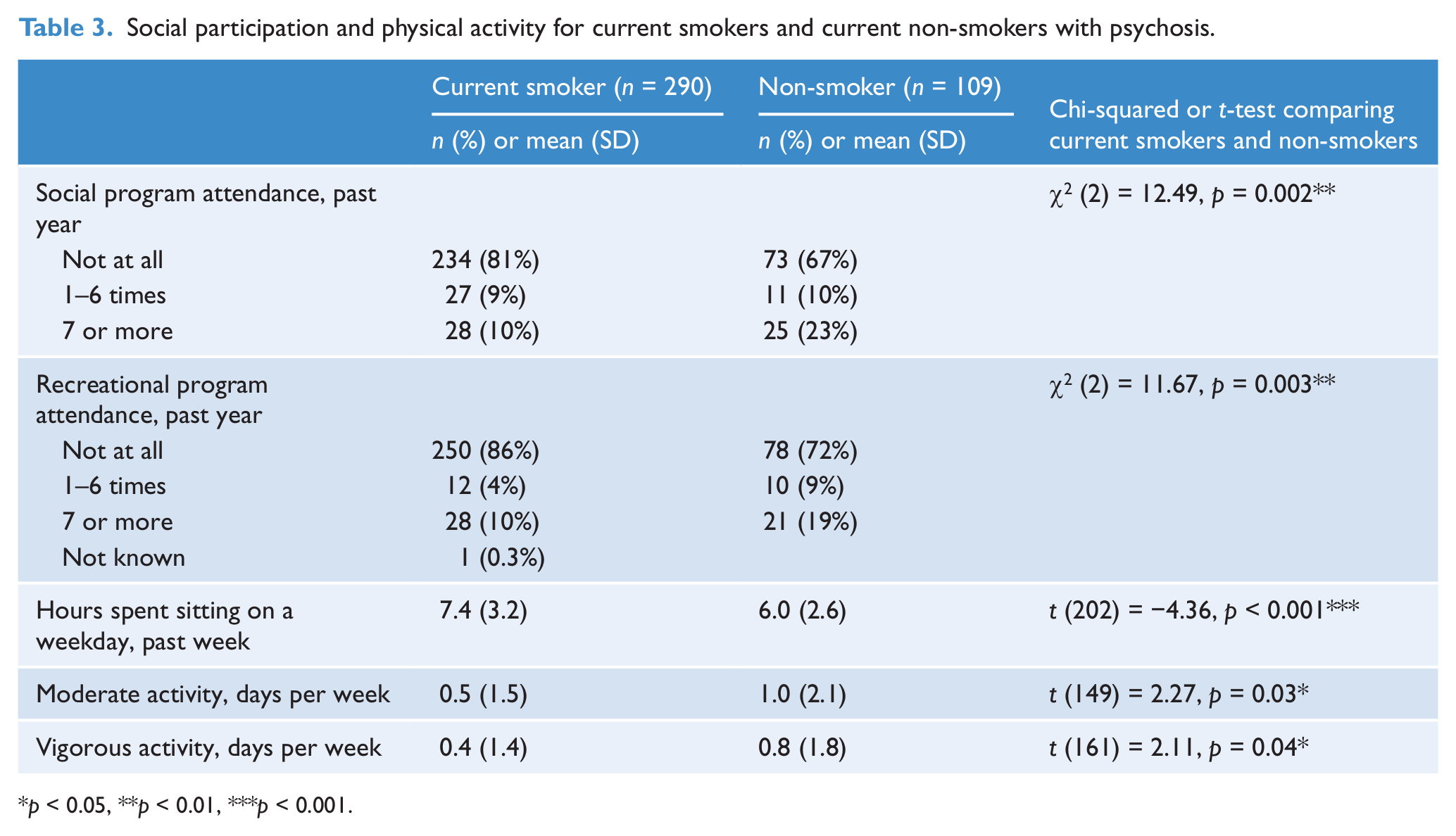
p < 0.05, **p < 0.01, ***p < 0.001.
They were also significantly more likely to experience poor financial and health outcomes than non-smokers (Table 4). Smokers had higher rates of alcohol and cannabis abuse and were more likely to have been assaulted in the previous year (Table 5).
Financial and health consequences for current smokers and current non-smokers with psychosis.
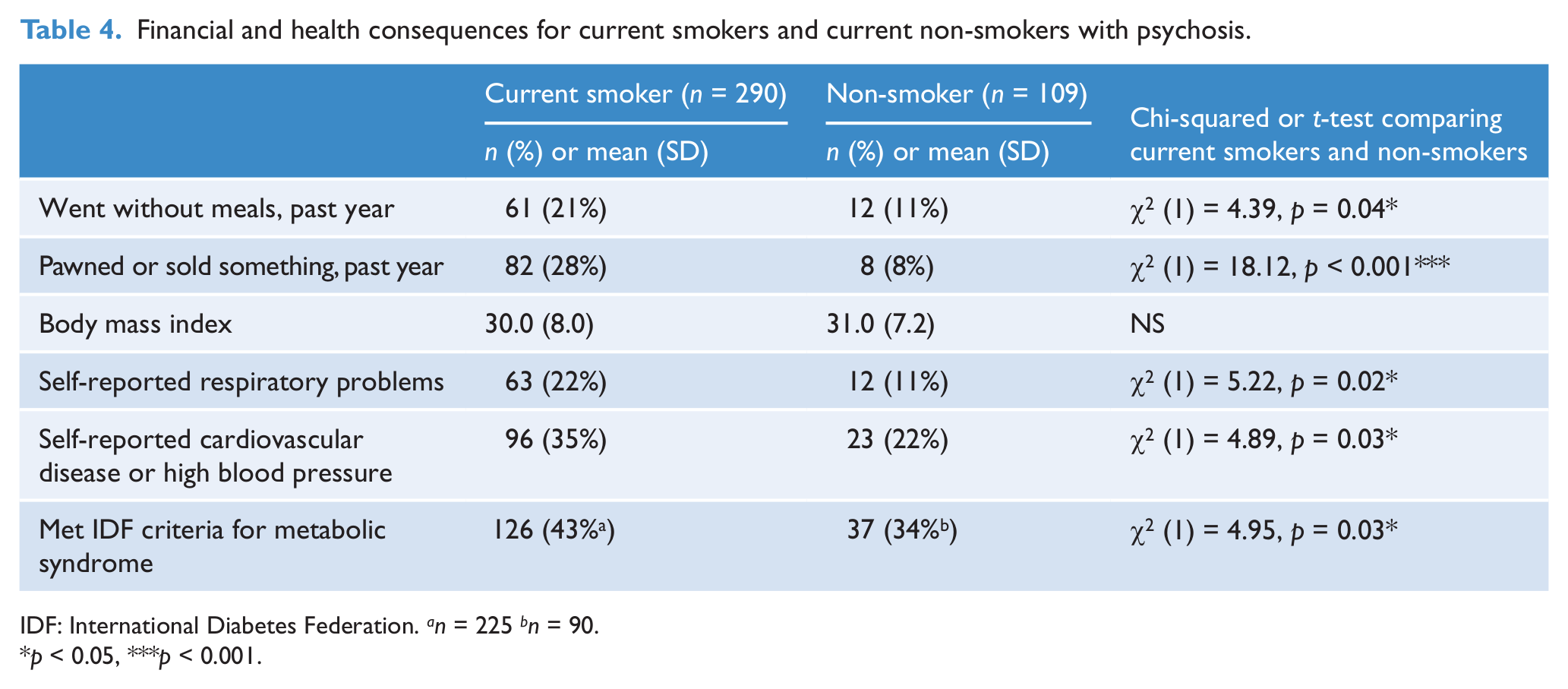
IDF: International Diabetes Federation. an = 225 bn = 90
p < 0.05, ***p < 0.001.
Substance use and criminal activity for current smokers and current non-smokers.
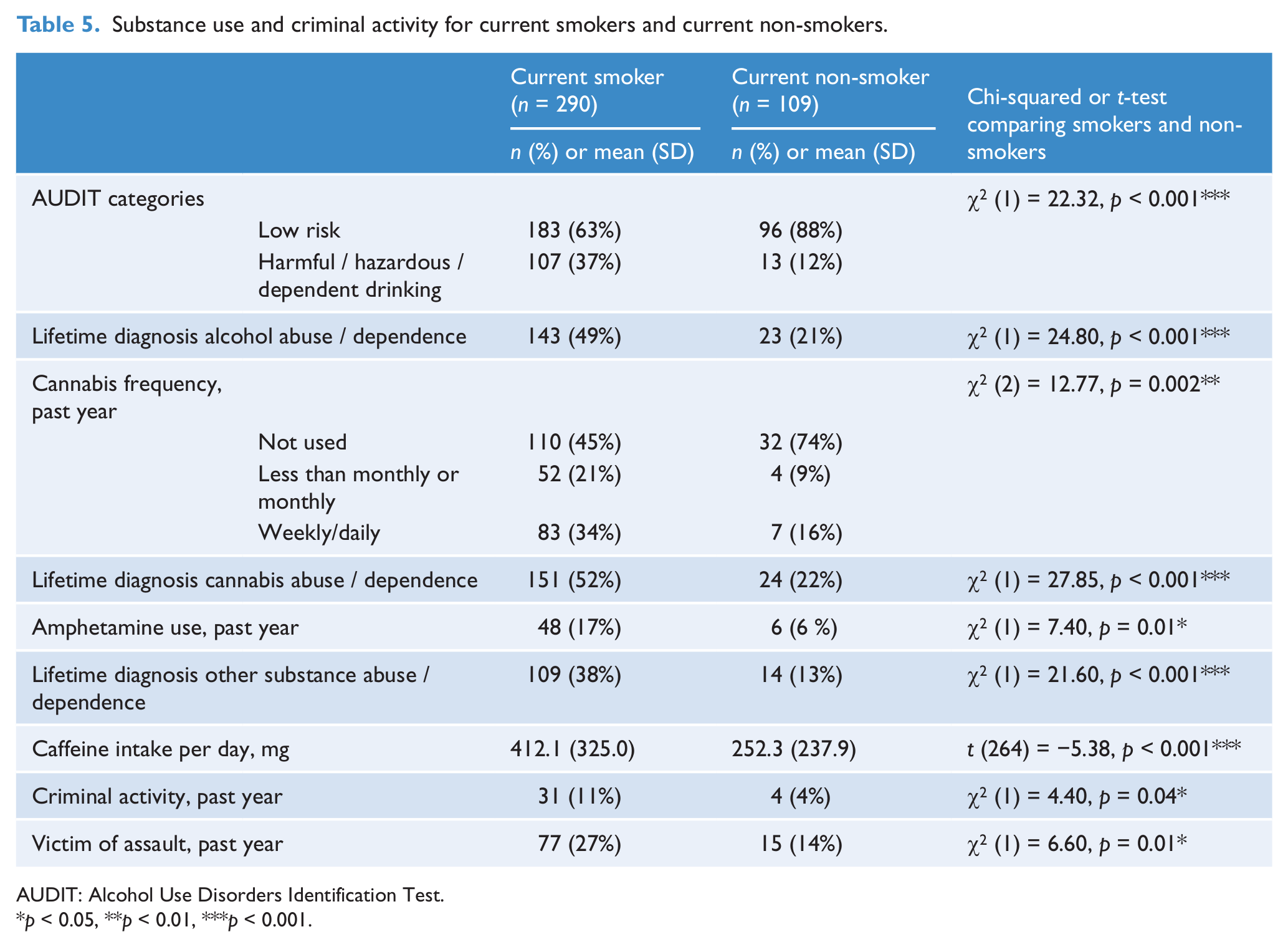
AUDIT: Alcohol Use Disorders Identification Test.
p < 0.05, **p < 0.01, ***p < 0.001.
Gender differences in the associations between alcohol and cannabis use, and smoking are presented in Table 6. Table 7 reports the results of the regression analyses.
Alcohol and cannabis use among men and women with psychosis who are smokers and non-smokers.
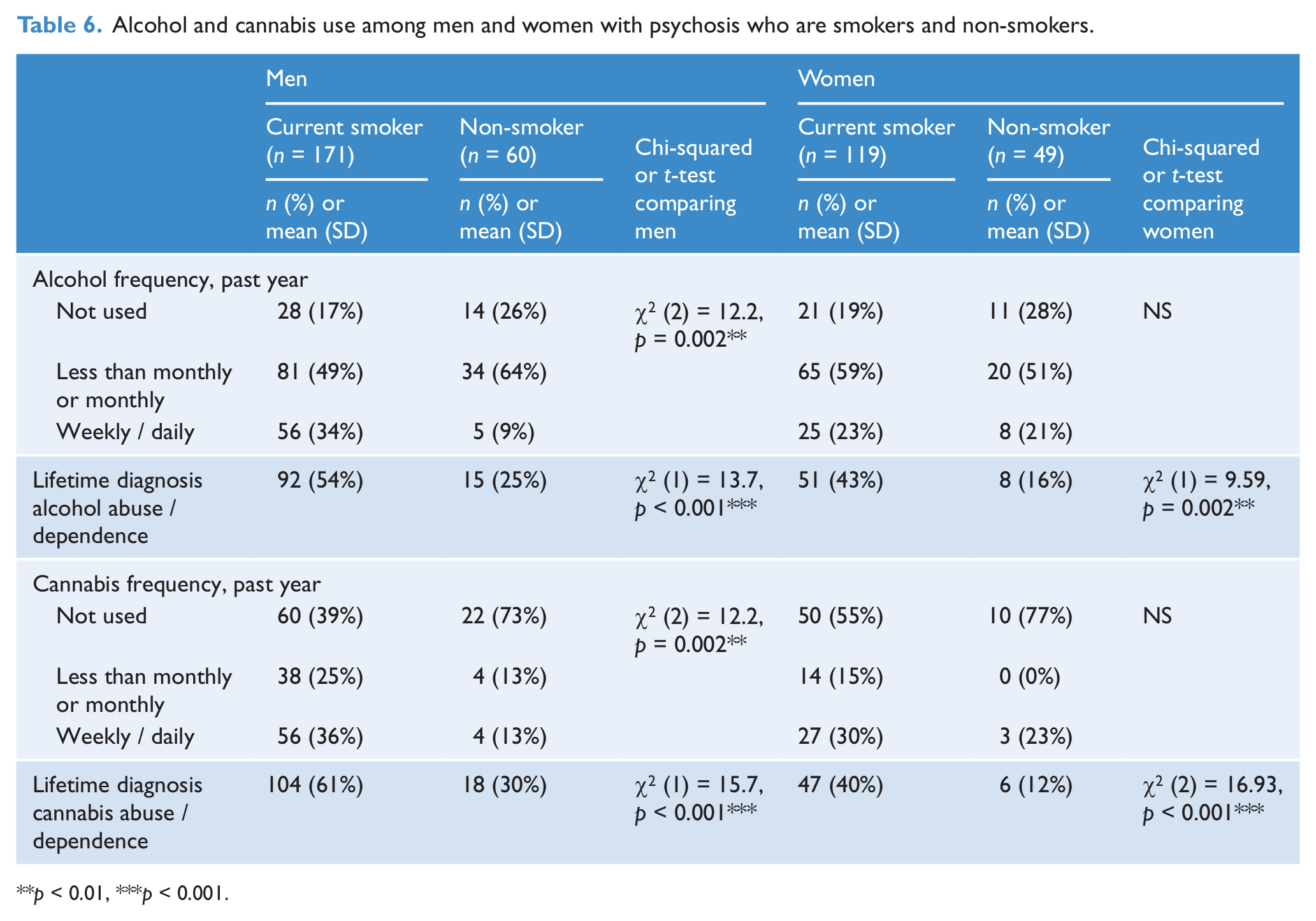
p < 0.01, ***p < 0.001.
Odds ratios and confidence intervals of current smoking in males and females with psychosis.
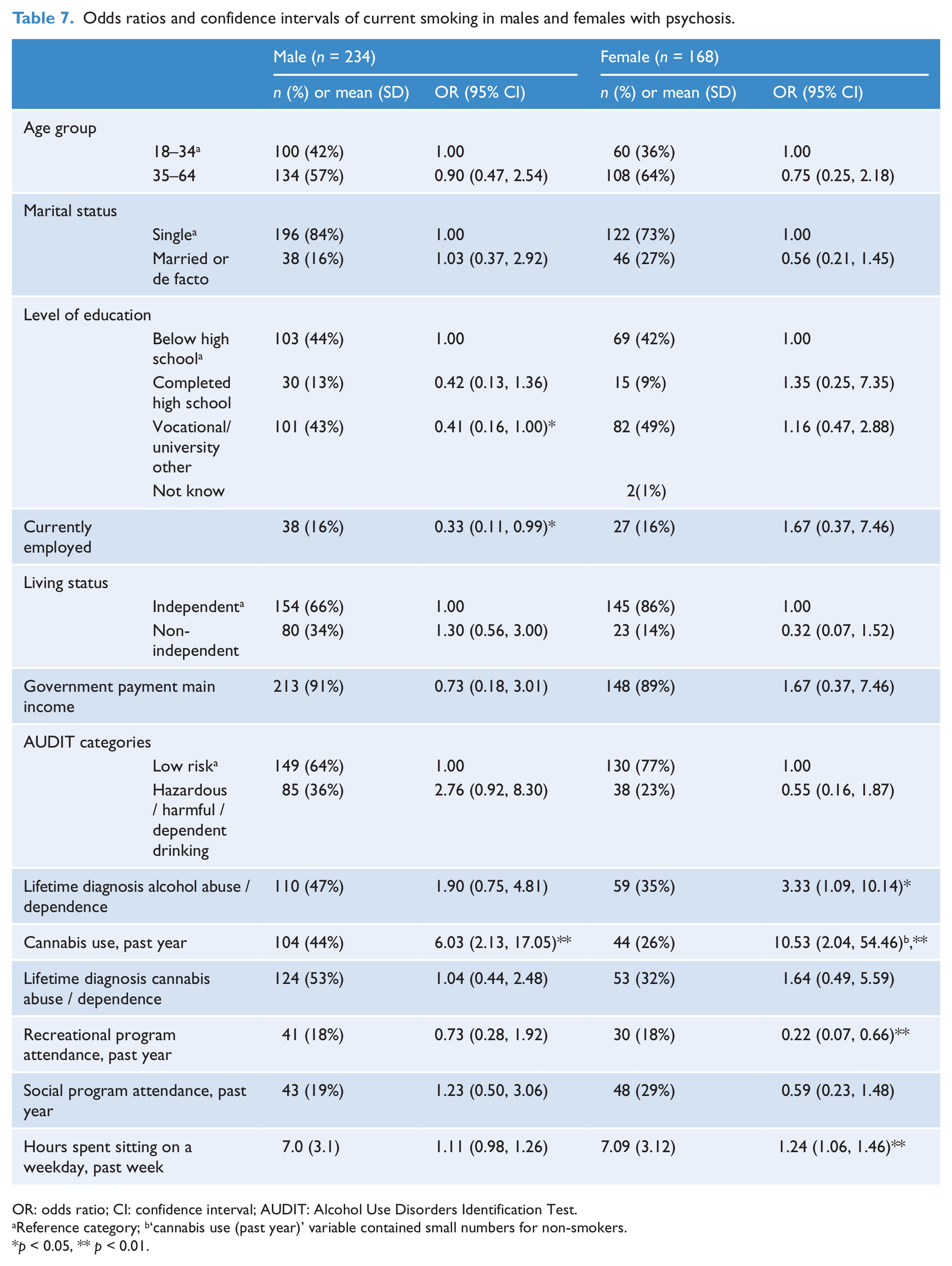
OR: odds ratio; CI: confidence interval; AUDIT: Alcohol Use Disorders Identification Test.
Reference category; b‘cannabis use (past year)’ variable contained small numbers for non-smokers.
p < 0.05, ** p < 0.01.
For males, the full model containing all predictors was significant, χ2 (14, n = 216) = 65.69, p < 0.001, and explained between 26% and 39% of the variance in smoking status. Lack of post-school qualifications, unemployment and cannabis abuse were significant predictors of smoking. For females, the full model including all predictors was significant, χ2 (14, n = 157) = 49.13, p < 0.001, and accounted for between 27% and 38% of the variance in smoking status. A lifetime diagnosis of alcohol abuse / dependence, cannabis abuse, non-attendance at recreational programs and more sedentary behaviour were all significant predictors of smoking.
Discussion
This study showed that the prevalence of smoking was very high in people with psychotic disorders living in the northern suburbs of Adelaide. Smoking rates are higher in areas of social disadvantage and in people with severe mental illness; our data suggests that our sample had very high rates of smoking because of these combined factors. Unlike prior studies, this present study found no significant differences between current smokers and non-smokers with psychosis in terms of gender, marital status, living situation or diagnosis (de Leon and Diaz, 2005; Dodd et al., 2010; Johnson et al., 2010). The gender finding was surprising as in both the general population and in psychosis samples, a greater proportion of men are smokers. However, unemployment, below year 12 education and receiving government welfare were significantly more common in smokers in the current study, which is consistent with prior research (Keizer et al., 2009; Salokangas et al., 2006) and general population data (Scollo and Winstanley, 2008). These factors are all more common in the northern suburbs, so the people with psychosis were doubly disadvantaged – they lived in a deprived area, then they had lower rates of education and employment than the general population of the region. Unemployment rates in the current study 88% were higher than in previous studies of people with mental illness in Australia (77%; Baker et al., 2007), indicating the impact of the high unemployment levels characteristic of the northern area.
Daily cigarette consumption was slightly below findings in previous literature (29 vs 32; Baker et al., 2007) but the number of quit attempts by men in this current study was two times higher than previous studies (Baker et al., 2007). This supports previous South Australian research showing that people with severe mental illness are motivated and interested in quitting smoking (Ashton et al., 2010).
We found a higher proportion of current smokers did not attend social or recreational programs compared to non-smokers, even given the low participation rates in community events that already exist among the general population in the northern region (Spoehr et al., 2007). The introduction of smoke-free policies may act as a deterrent to attending community events for the habitual smoker. The level of physical activity was low for all participants, but smokers had a significantly lower level of physical activity and spent only half a day per week on moderate activity, and an average of 7 hours on a weekday being sedentary. Taken together, these findings suggest that people with psychosis who smoke are inactive and disengaged; so interventions that include time scheduling, involvement in a range of activities and vocational rehabilitation might be helpful.
Poorer physical health and financial outcomes were observed in smokers in this study, supporting previous findings (Bobes et al., 2010; Steinberg et al., 2004). Smokers were more likely to go without basic necessities, including meals, illustrating the financial burden of supporting nicotine addiction. Smokers were also more likely to live with friends or be co-tenants; the financial consequences of smoking may make living alone unaffordable.
We found that there were different predictors of smoking in men and women. For men, having a post-school qualification and being in paid work decreased the likelihood of smoking, which suggests that non-smoking may also assist with getting employment and non-smoking workplaces may support the maintenance of a non-smoking status, or that people with a higher level of functioning are less likely to smoke. This is supported by previous literature which found that having a below high school education predicted smoking in men (Johnson et al., 2010). Cannabis use was a risk factor for both men and women. Contrary to previous findings, having a diagnosis of alcohol abuse dependence in women also predicted smoking (Johnson et al., 2010) and this could possibly be related to the higher rates of drug and alcohol use in the northern area (Spoehr et al., 2007).
Limitations
This study utilises a cross-sectional design which does not allow for causal inferences to be made. Our findings are derived from a disadvantaged community, and may not be generalisable to more socially advantaged communities.
After finding that the rates of smoking were higher than expected for women, being similar to the rates for men in our sample, a regression analysis stratified by gender was employed to explore this finding. This method allowed us to determine predictors of smoking status for males and females, but stratifying the sample did result in a loss of power.
We relied on self-reports so there may have been under-reporting of socially undesirable behaviours such as substance use and criminal activity. Patients attending mental health services through the private sector and people in prisons were not surveyed so this study is only representative of patients accessing public mental health services.
Conclusion
Smoking rates were strikingly high in both men and women in our sample compared to prior research. The relationship between psychotic illness and tobacco smoking is complex and our study shows that the risk of smoking is increased by factors related to the social disadvantage of living in the northern Adelaide region. The key message from this study is smoking cannot be addressed in isolation from the socio-demographic context, especially for people with severe mental illness.
It has been previously suggested that smoking must be addressed by changing the social conditions that cause inequalities (O’Brien et al., 2012). Similarly, our findings suggest that interventions should not focus only on smoking cessation, but also address factors that are associated with social disadvantage, including promoting employment, education, social and community participation, physical activity, health and well-being, and a safer community. The high levels of smoking in women with psychotic illness in the north is an important finding which is contrary to our understanding of the association between gender and smoking status in the general community. While there were different risk factors for smoking in men and women, interventions need to focus on engaging in activities, particularly employment, recreational activity and substance use across both genders to reduce smoking behaviours. Smoking reduction and cessation programs have shown promising results (Ashton et al., 2010) and need to be located in the northern region where they can be easily accessed. Further research in this area is warranted to develop and evaluate interventions informed by these findings.
Footnotes
Acknowledgements
This paper is based on data collected in the framework of the 2010 Australian National Survey of High Impact Psychosis. Members of the Survey of High Impact Psychosis Study Group are: V Morgan (National Project Director), A Jablensky (Chief Scientific Advisor), A Waterreus (National Project Coordinator), R Bush, V Carr, D Castle, M Cohen, C Galletly, C Harvey, B Hocking, A Mackinnon, P McGorry, J McGrath, A Neil, S Saw and H Stain. Ethics approvals for the study were obtained from relevant institutional human research ethics committees. The authors acknowledge, with thanks, the hundreds of mental health professionals who participated in the preparation and conduct of the survey and the many Australians with psychotic disorders who gave their time and whose responses form the basis of this publication.
Funding
This study was funded by the Australian Government Department of Health and Ageing.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.