
Abstract
There is a strong association between smoking and poor mental health. Previous epidemiological studies have reported that the prevalence of tobacco smoking in people with poor mental health is twice that in people with good mental health [1,2]. Compared to the general population, there is a higher prevalence of tobacco smoking in people with mental health disorders [3], including anxiety disorders [2,4], affective disorders [5], and psychotic disorders [6].
The prevalence of mental disorders appears to be much higher among smokers than non-smokers. Compared to people who had never smoked and ex-smokers, the prevalence of affective disorders and anxiety disorders were at least double for current smokers in the 1997 Australian National Survey of Mental Health and Well-Being (NSMHWB) [7,8]. Compared to those who never smoked, current smokers had 1.3 times higher odds of meeting criteria for an affective disorder and 1.5 times higher odds of having an anxiety disorder [7]. Higher levels of psychological distress were also observed in current smokers than in people who had never smoked or were ex-smokers. Patton et al. [9] found that symptoms of psychological distress made adolescents more likely to start smoking in a longitudinal study of 2032 Australian secondary school students. Similarly, other population-based longitudinal studies in the United States [10] and New Zealand [11] have reported an increased risk of becoming a daily smoker in depressed people compared to people without depression. Longitudinal studies in the Netherlands, Norway and the United States have reported a higher incidence of anxiety disorders [12] and depression [10,13] among smokers than non-smokers.
A number of hypotheses may explain the relationship between smoking and mental disorders. Firstly, smoking may be used by people with mental disorders, such as depression, as a form of self-medication for symptom relief [14]. Secondly, smoking does produce changes in neurotransmitters, such as monoamine oxidase [15], dopamine, serotonin, norepinephrine, acetylcholine, GABA, and glutamate [16]. These neurotransmitters are involved in the regulation of mood, pleasure, excitability, and attention, and so may make smokers more vulnerable to developing mental disorders. Finally, there could be shared risk factors for both tobacco smoking and poor mental health such as: genetic factors [17], low socio-economic status [18], neuroticism [19] and impulsivity [20].
The lower quit rates for people with mental disorders may reflect greater difficulties in quitting because of more severe withdrawal symptoms [20,21]. Quitting smoking may worsen the immediate mental health of people with mental disorders [22]. People suffering from mental disorders, including depression, are also less likely to use health care services [23], have less health knowledge, lower self-efficacy, and receive less support to quit smoking [24, 25].
Few studies have examined the relationship between mental health and smoking using a population sample, which is a limitation if we want to interpret the findings from a population health perspective. In the few studies that used a national sample, there was limited data on people's smoking and quitting behaviour, such as the length of time since ex-smokers have quit, what motivated people to quit smoking, smokers’ past attempts to quit, or the reasons why people smoke. The present study examined the relationships between detailed smoking and quitting behaviour and a measure of common mental health disorders (depression and anxiety) in the general Australian population.
Methods
Participants
The sample were from the 2004 (N = 26 017) and 2007 (N = 21 363) National Drug Strategy Household Surveys (NDSHS) conducted by the Australian Institute of Health and Welfare (AIHW) and the Australian Department of Health and Ageing [26,27] and accessed via the Australian Social Science Data Archive. The NDSHS is a series of cross-sectional national surveys that measure the prevalence, behaviour, knowledge, awareness, and attitudes towards alcohol, tobacco, and illicit drug use in representative samples of the Australian population. The surveys use multi-stage random sampling of households with the sample stratified by region and over-sampling in some states and territories. In each household the selected respondent was the person aged 12 and over who would have the next birthday. Two methods of data collection were used: drop and collect self-completed questionnaires (83% of sample) and computer assisted telephone interviewing. The overall response rate was 44% in 2004 and 52 % in 2007 [28,29].
Measures
Smoking status according to quitting activity
Participants were categorized as current smokers, ex-smokers (have smoked more than 100 cigarettes in their lifetime, but not currently smoking), or never smoked (have not smoked more than 100 cigarettes in their lifetime). Current smokers were further categorized according to whether they had made a quit attempt in the past 12 months, and if so, whether they succeeded or failed at short-term abstinence before relapsing (< 1 month = failed, ≥ 1 month = succeeded). Ex-smokers were categorized according to time since quitting (< 1 year, 1 or 2 years, 3 or 4 years, and ≥ 5 years).
Cigarettes per day
In current smokers, the number of cigarettes (both manufactured and roll-your-own) currently smoked per day (CPD) were categorized into: < 5 CPD, 5–14 CPD, 15–24 CPD, and ≥ 25 CPD.
Reasons for not quitting
Current smokers were asked whether they intended to quit smoking in the future. If they said no, they were asked to indicate the reasons. The list of responses included, ‘I enjoy smoking’, ‘Smoking relaxes me’, ‘Smoking helps me deal with stress’, ‘I am addicted to nicotine’, and ‘I tried to quit before, but failed’. Multiple responses were allowed.
Motivators for quitting
Current smokers were also asked ‘What motivated you to attempt to quit in the last 12 months’. The list of motivators included specific public health tobacco control strategies and policies, health and fitness, family and friends, and cost. Multiple responses were allowed.
Kessler 10 scale of psychological distress
The Kessler 10 (K10) measures the frequency of anxiety and depressive symptoms experienced by participants in the four weeks prior to the survey [30]. It has strong psychometric properties, and good correlation with DSM-IV criteria for affective and anxiety disorders [31]. Scores range from 10 to 50, with a lower score indicating a lower level of psychological distress (PD). Scores were classified into four categories to represent the level of PD: 10–15 = low, 16–21 = moderate, 22–29 = high, and 30–50 = very high [32].
Socio-demographic measures
To examine PD and smoking status by age groups, age was categorized into 10-year age groups (20–29, 30–39, 40–49, 50–59, 60–69, and ≥70), otherwise age was analysed as a continuous variable. The highest level of education completed was used as an indicator of socioeconomic status (SES) at the individual level, and the Index of Relative Advantage and Disadvantage (IRAD) as an indicator of SES based on participants’ area of residence. Highest level of education was categorized as: high school or below, certificate or diploma, and bachelor degree or above. The IRAD is a socio-economic index for areas compiled by the Australian Bureau of Statistics that takes into consideration income, education, employment, and occupations within census collection districts [33,34].
Data analysis
All statistical analyses were conducted using SPSS 17.0. Prevalence estimates of PD levels and smoking status were calculated with the data weighted to the Australian population according to area of residence, age and sex using weights supplied by AIHW. Chi-square tests of association were used to compare prevalence by socio-demographic groups using unweighted data.
Unweighted data were used in multinomial logistic regression models to examine association between smoking and PD. Smoking measures were the explanatory variables, and PD was the outcome variable (referent = low PD). Age, sex, IRAD, highest level of education, and year of survey were included as covariates to adjust for potential confounding.
Results
Overall, the prevalence of current smoking in 2004 and 2007 was 21.5% and 20.5% and ex-smoking was 29% and 27.7%. As expected, the majority of the sample had low PD (low = 69.1% in 2004 and 69.5% in 2007, moderate = 21.3% in 2004 and 20.9% in 2007; high = 7.5% in 2004 and 7.5% in 2007; and very high = 2.2% in 2004 and 2.1% in 2007). There was no significant difference in the relationship between smoking and psychological distress between the two surveys (2004 and 2007), hence the data were analysed together and survey year included as a covariate to adjust for potential confounding.
Socio-demographic characteristics
Table 1 shows the PD levels and smoking status by socio-demographic categories. Psychological distress was higher in females than males, in younger age groups, and in those of lower SES. Males were more likely to be current and ex-smokers, while females were more likely to have never smoked. Current smoking was most common in the younger age and lower SES groups, while ex-smoking was more common in the older age groups.
Distributions of psychological distress categories and smoking status categories within socio-demographic groups
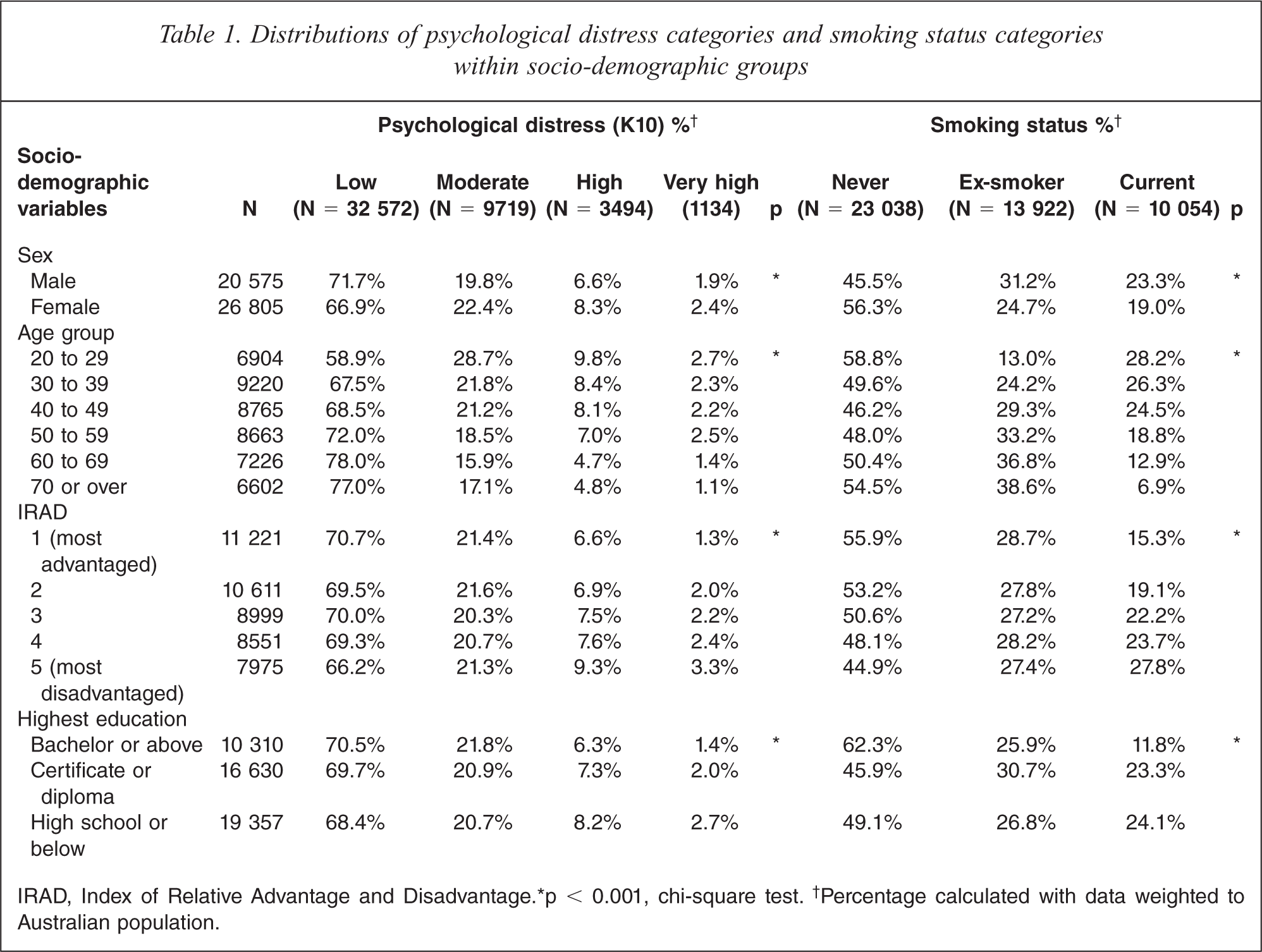
IRAD, Index of Relative Advantage and Disadvantage. ∗p < 0.001, chi-square test.† Percentage calculated with data weighted to Australian population.
Smoking status according to quitting activity
Both current smokers and ex-smokers had higher odds of having moderate, high or very high PD, compared to never smokers (see Table 2). The highest odds of PD were associated with being a current smoker who tried to quit in the previous 12 months, but had completely failed (< 1 month abstinent). Among successful quitters (i.e. ex-smokers), the longer the time (in years) that they had been abstinent for, the more similar their level of PD was to that of never smokers.
Odds ratios for moderate, high and very high psychological distress compared with low psychological distress associated with smoking status classified according to successful and unsuccessful quitting attempts†
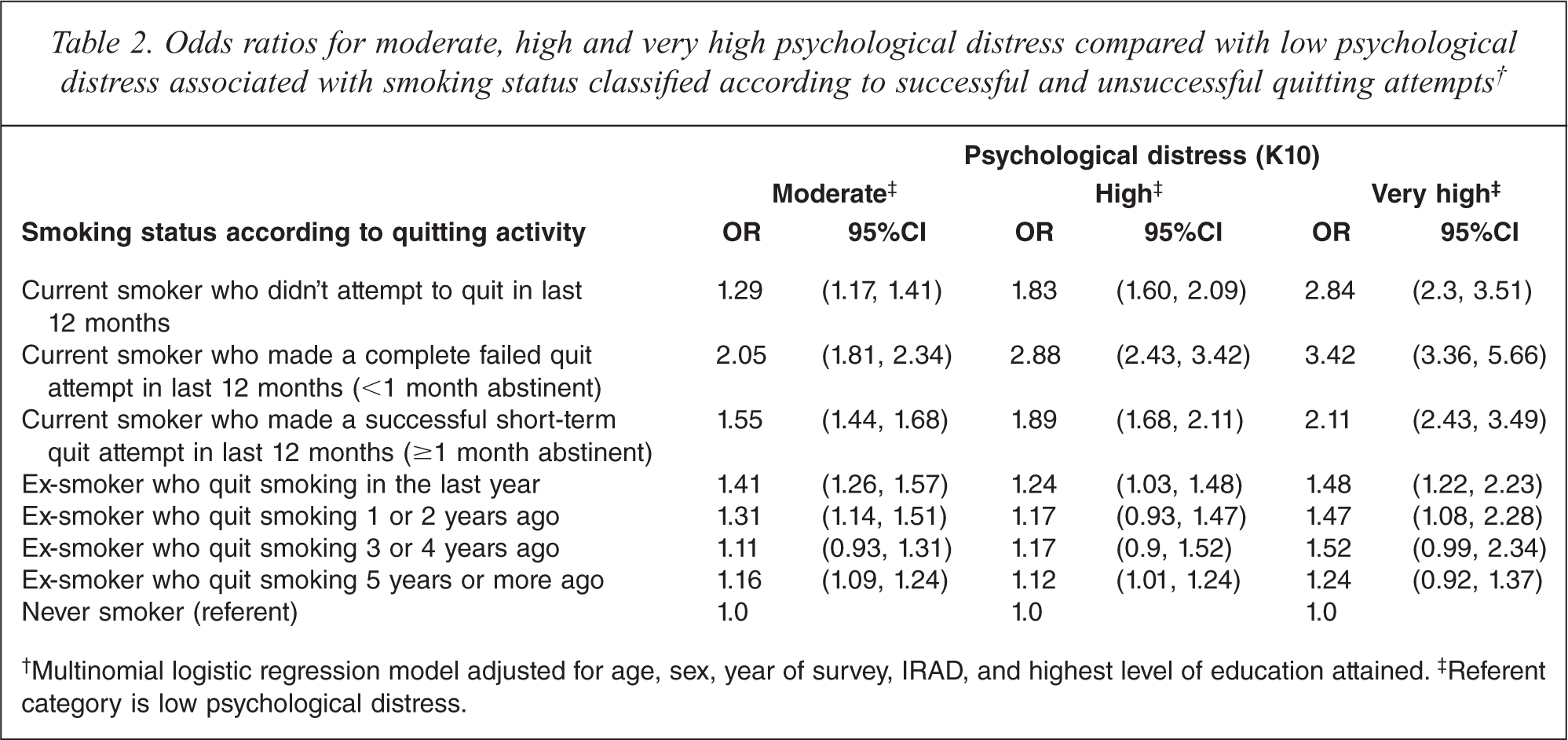
†Multinomial logistic regression model adjusted for age, sex, year of survey, IRAD, and highest level of education attained.‡ Referent category is low psychological distress.
Cigarettes smoked per day
For current smokers, a dose-response trend was apparent such that the level of PD increased with the number of cigarettes smoked per day (see Table 3).
Odds ratios for moderate, high and very high psychological distress compared with low psychological distress associated with number of cigarettes smoked per day in current smokers†
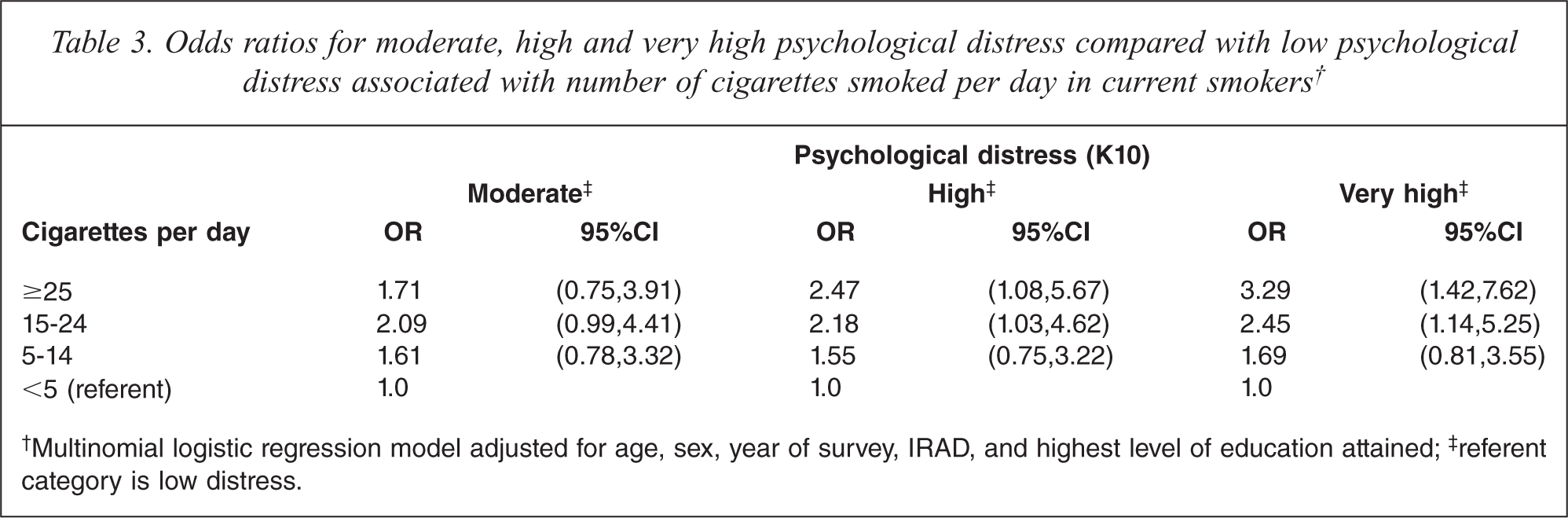
†Multinomial logistic regression model adjusted for age, sex, year of survey, IRAD, and highest level of education attained;‡ referent category is low distress.
Quitting intentions and reasons for smoking
In current smokers, multinomial logistic regression was used to examine the odds of higher levels of PD by whether or not the participant intended to quit smoking (yes or no, referent = no), and if not, what their reasons for not planning to quit were (list of reasons, yes or no, referent = no). Compared to those who did not plan to quit, smokers who planned to quit had higher odds of having moderate or high PD. Among smokers who did not plan to quit, those who reported enjoying smoking as a reason for not quitting had lower odds of moderate, or high or very high PD (see Table 4). Those who reported smoking for relaxation, smoking to deal with stress, addiction, and past failure at quitting as reasons for not planning to quit had greater odds of having higher PD, compared to the low PD group. Smoking due to enjoyment was associated with lower odds of moderate, high or very high PD.
Odds ratios for moderate, high and very high psychological distress compared with low psychological distress associated with intentions to quit, and reasons for not planning to quit in current smokers†

†Separate multinomial logistic regression models for each row, adjusted for age, sex, year of survey, IRAD, and highest level of education.‡ Referent category is low psychological distress;§ only available for year 2007
Motivators for quitting
Among current smokers who made a quit attempt in the last 12 months, there were no statistically significant differences in the odds of moderate, high or very high PD associated with ringing the QUIT line, asking a doctor for help, using nicotine replacement therapy, using a smoking cessation pill, reading ‘how to quit’ literature, or using the internet for quitting (see Table 5). Smokers who reported being motivated by wanting to get fit, smoking affecting their health or fitness, their doctor advising them to quit, family or friends asking them to quit, concern about their smoking affecting others and smoking costing too much had greater odds of moderate, high or very high PD. These results suggest that motivation to quit smoking by public health interventions was not associated with PD, and that being motivated to quit due to health, costs, and friends or family was associated with higher PD.
Odds ratios for moderate, high and very high psychological distress compared with low psychological distress associated with what motivated a quit attempt in current smokers who made an attempt in the last 12 months†
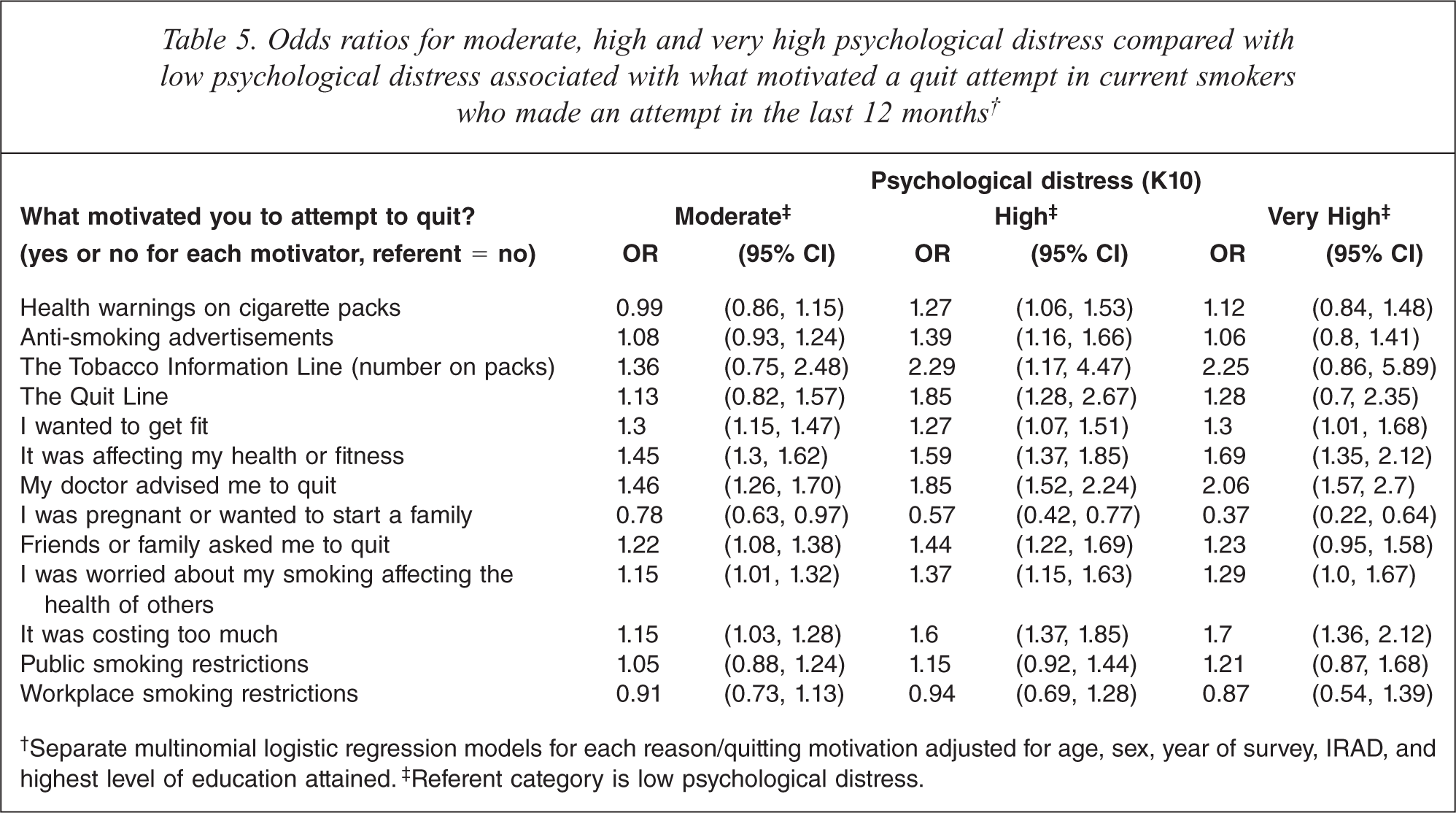
†Separate multinomial logistic regression models for each reason/quitting motivation adjusted for age, sex, year of survey, IRAD, and highest level of education attained.‡ Referent category is low psychological distress.
Discussion
Our analysis of the 2004 and 2007 NDSHSs showed a positive relationship between cigarette smoking and PD, as measured by the K10. Compared to low PD, risks of all levels of PD were greater for current smokers than non-smokers. Furthermore, among current smokers, risks of all levels of PD increased with greater CPD. These results are consistent with findings from the 1997 and 2007 NSMHWB [3,7,35].
Consistent with Glassman et al. [36], we found that quitting failures were associated with poorer mental health. Our results showed that PD was associated even with the ability to sustain short-term abstinence. These lower quit rates combined with an earlier age of smoking initiation [35], may contribute to the longer duration of smoking seen in smokers with poor mental health compared to mentally healthy smokers [2]. Reducing cigarette intake may be an important preliminary step to quitting as smoking more cigarettes per day has been related to lower quit rates in previous studies [37,38]. Smokers with PD may find cutting down the number of cigarettes a more achievable goal than complete cessation. The use of nicotine replacement therapy to ‘cut down to quit’ may be a useful aid to these smokers [39]. A possible explanation of the association between PD and lower quitting success is that distressed smokers may have greater nicotine addiction than mentally healthy smokers. Indeed, our results showed that higher CPD was associated with higher PD. Distressed smokers are at greater health risk from smoking than smokers with good mental health [40] due to their higher cigarette consumption and possible longer duration of smoking, which are strongly related with poorer physical health.
This study is the first to investigate the association between psychological health and the length of time since quitting in ex-smokers. The findings showed higher PD among ex-smokers than never smokers, and the association decreased with the time since quitting. The longer they were abstinent, the more their level of PD resembled that of people who never smoked. This suggests a reduction in risk of poor mental health with increasing time since quitting, analogous to the reductions seen for risk of cardiovascular disease [41] and lung cancer [42]. However, as these are cross-sectional data, it is also possible that this result reflects the cumulative effects of lower quitting success and greater smoking relapse among smokers with higher levels of PD. Smoking may increase the risk of developing depression, and being depressed may increase the risk of smoking [43].
Our findings on the relationship between PD and intentions to quit smoking are consistent with findings in clinical samples that the majority of mental health patients who smoke are interested in quitting [44]. Furthermore, among smokers who did not plan to quit, we found higher levels of PD among smokers who reported addiction, and lower levels of PD among those who report enjoying smoking as reasons for not quitting. This evidence contradicts the common belief that smoking is one of the few life pleasures for persons with mental disorders [45] that has led to reluctance to address smoking in those with mental health problems [46]. Our results suggest that people with poor mental health, including common symptoms such as depression and anxiety, could improve their physical health and quality of life through assistance to reduce smoking.
An explanation of the association between smoking and PD is that these smokers may ‘self-medicate’ their symptoms with cigarettes. This may explain the higher PD among smokers with a higher quitting failure rate. Our finding that PD was associated with smoking to reduce stress and for relaxation further provides evidence for the ‘self-medication’ theory. However, while depressed smokers may smoke to reduce their symptoms, it is an ineffectual strategy and counterproductive in the long-term [47].
Public health interventions
Common mental disorders, such as depression and anxiety, are typically of short duration but the risk of their recurrence is high. Some researchers have argued that depression should be treated as a chronic disorder with a recurring episodic course [48]. Indeed for a majority of people with anxiety disorders in NSMHWB, the first onset of symptoms was more than 10 years prior [2]. Consistent with Lawrence et al. [2] we found that even mild mental health symptoms were associated with smoking and with lower quitting success. Our finding that all levels of PD decrease with time since quitting, suggests that quitting smoking may also reduce PD in the long-term.
Our analyses found higher PD among smokers who reported financial expense as motivating them to make a quit attempt. The Australian government's recent increase in the tobacco tax rate may have a positive influence on quitting, especially among people with PD. Other public health strategies such as anti-smoking advertisements, the QUIT line and public smoking restrictions as motivations for making a quit attempt were not associated with smokers’ level of PD, implying that these strategies were equally effective at motivating a quitting attempt among all smokers, irrespective of their level of PD.
Clinical interventions
Our results showed that motivation to quit due to health concerns and advice from their doctor to quit were associated with higher levels of PD among smokers. General practitioners, who may be the medical profession most likely to encounter smokers with common mental health disorders, should recognize that these patients may be motivated to quit smoking to improve their physical and mental well-being. They can assist these patients by prescribing appropriate cessation aids (e.g. nicotine replacment therapy), discussing intermediate goals (e.g. cutting down) and referring them to allied health practitioners and self-help material to improve their self-efficacy, and to learn relaxation techniques and healthier ways to deal with stress, such as cognitive behavioural therapy. Community-based resources such as internet sites for depression and anxiety could also provide more material on the benefits of quitting smoking and links to quitting resources.
Strengths and limitations
Our study used a large population-based sample and measured mental health with a standard measure of psychological distress which has been shown to have good psychometric properties for measuring symptoms of common mental health disorders such as depression and anxiety [31]. The NDSHS also provided detailed data on smoking history and quitting behaviours.
Previous studies have shown that nicotine dependence may be an important factor in the relationship between mental health, physical health, and quitting smoking [49] but the NDSHS dataset did not measure nicotine dependence. We did, however, have data on the numbers of cigarettes smoked per day, which may be a proxy for nicotine dependence. Indeed we found that smoking more CPD was associated with higher PD, which is consistent with a relationship between nicotine dependence and PD.
Ex-smokers were classified as such if they were not currently smoking but 14% reported smoking in the past 12 months. Considering that around 46% of quitters can be expected to relapse in the first 12 months [50], many of these ex-smokers would be expected to relapse. However, in the analyses we have separated ex-smokers according to the years since quitting to account for differences in the ex-smoker population, including the risk of relapse. Our sample included participants aged 20 and over, thus in ex-smokers, the number of years since quitting differed across age groups, as older ex-smokers could have more years since quitting. Older people were less likely to be psychologically distressed; therefore, age could be an explanation of our finding that longer time since quitting was associated with lower PD. However, age was controlled for in the logistic regressions.
The response rates for these surveys were 44% (2004) and 52% (2007) and there is no information available on the characteristics of non-responders. However, the prevalence of daily smoking according to PD measured with K10 in the 2004 and 2007 NDSHSs was similar to that observed in the 2004 and 2007 National Health Surveys which had response rates of 89% and 91%. The prevalence of PD in the 2007 NDSHS was also similar to that reported in the 2007 NSMHWB (low = 71.1%, moderate = 19.5%; high = 6.9%; and very high = 2.6%) [51].
People with mental disorders are likely to be under-represented in population-based surveys. Smokers may also be less likely to participate in these studies, possibly leading to underestimation of smoking prevalence in the population. Certain populations that have a high prevalence of both mental health disorders and smoking, such as the homeless and institutionalized people, were excluded from the sample. Therefore, it is likely that we have underestimated the association between smoking and mental health. Furthermore, as with all self-reported data, there could be recall error or inaccuracies in reporting of smoking and quitting behaviour.
Our results suggest that smokers who are less successful in quitting attempts are likely to be more distressed than successful quitters. This association could be somewhat inflated if depressed smokers report past failures more accurately than mentally healthy smokers due to negative memory bias [52]. Similarly, the poorer mental health among smokers reporting addiction, but an inverse association with enjoyment of smoking as reasons for not quitting, may reflect depressive symptoms such as loss of agency and anhedonia. These are important findings nonetheless because they indicate that depressed smokers may not gain pleasure from smoking and may need more assistance to quit, particularly if they have previously tried and failed.
Conclusions
We found that symptoms of poor mental health are strongly related to current smoking and unsuccessful quit attempts. Smokers who smoke more cigarettes per day have poorer mental health. However, longitudinal research is needed to confirm whether tobacco reduction improves cessation and mental health outcomes, and which strategies are most effective.
Footnotes
Acknowledgements