
Abstract
During the past 40 years, international migration has become increasingly prevalent [1]. To give only two examples, the Australian immigration programme for 2003–2004 offered 100 000–110 000 places for migrants, plus a parent contingency reserve of 6500 places for a full year; while Canada has welcomed, on average, 220 778 immigrants and refugees per year for the past 10 years [2].
Immigration is a major stressful life-event capable of putting mental health at risk and generating maladjustment [3–5]. The acculturation stress hypothesis has been proposed as an explanation of the effects of immigration on mental health [6, 7]. This hypothesis proposes that the stresses of living in a foreign culture promote mental disorder in vulnerable individuals [8–13]. It also assumes that the higher emotional distress accompanying migration is a result of the disruption to family, friendship and other social support networks [14, 15], and of the migrant's exposure to an unfamiliar cultural–physical environment [16], to prejudice and discrimination [3, 17], and to low socioeconomic status [18]. Tests of this hypothesis, however, have given conflicting results: some studies find levels of psychological distress in immigrants higher than in the indigenous general population [19–23], but others report lower levels [24–28]. The discrepancies between studies may be explained by considerable methodological differences in sampling procedures, age grouping, screening instruments, and time frame or by differences in national immigration policies.
Israel is a country built by Jewish immigrants from all over the world and has always been open to them. Over the 60 years of its history many waves of immigrants have reached its shores. The past two decades, for instance, have witnessed a huge wave of Jewish immigration from the former Soviet Union (FSU): 81% of the immigrants arriving between 1989 and 2004 (total n = 1 180 870) were Jewish immigrants from the FSU [29]. Such a mass migration offers a unique opportunity to test the acculturation stress hypothesis, as well as to study a variety of risk factors. Previous studies have shown higher levels of psychological distress among FSU immigrants compared to the veteran Israeli population [30–37]. Most of these studies, however, were carried out on groups of limited size and suffered from methodological shortcomings. Only one study has compared psychological distress among Jewish newcomers from different countries: it found that FSU immigrants were more distressed than their counterparts from Ethiopia [38].
The study reported here used data from the Israel National Health Survey (INHS), the first nationwide study of mental health in Israel, the aim of which, among other goals, was to estimate the prevalence rates of psychological distress in Israeli adults [39]. The INHS was carried out in conjunction with the World Mental Health (WMH) survey initiative and followed its established uniform procedures [40]. The INHS provides a unique opportunity (i) to evaluate and compare psychological distress in immigrants from the FSU and elsewhere, and in the veteran population; (ii) to establish sociodemographic correlates for psychological distress in the immigrant population; and (iii) to test the acculturation stress hypothesis.
Method
Sampling and procedure
A detailed description of the INHS sample and procedures has been published elsewhere [39]. Briefly, the sample was extracted from the National Population Register and consisted of non-institutionalized de jure residents aged ≥21. The sample was designed to represent the distribution of selected gender–age–population groups in the general population (Arab and Jewish; the Israel-born; immigrants from the FSU or other countries after 1989). The sample was weighted back to the total population to compensate for the unequal selection probabilities resulting from disproportionate stratification, clustering effects and non-response. The weights were adjusted to make weighted sample totals conform to population totals known from reliable Central Bureau of Statistics (CBS) sources.
Personal interviews were conducted with the respondents in their homes from May 2003 to April 2004, in Arabic, Hebrew or Russian. The survey was administered, using a laptop computer-assisted personal interview, by interviewers trained and supervised by the CBS. Informed consent was received from all participants to the study, as required by the Israel Ministry of Health's Experimentation on Human Subjects Committee. The overall response rate was 73%. A total of 4858 completed interviews were collected, consisting of 3906 interviews with veteran Israelis, 845 interviews with immigrants after 1989 from the FSU (‘FSU immigrants’) and 107 interviews with immigrants from other countries during the same period (‘Other immigrants’). The mean (SE) length of immigration was 9.28 years (0.13) for immigrants arriving from the FSU and 8.56 years (0.38) for those from elsewhere, no significant difference (t = 1.69, df = 952, p = 0.1).
Assessing psychological distress
Psychological distress was measured on the General Health Questionnaire (GHQ-12) [41]. The GHQ-12 has been used extensively worldwide as a valid and reliable measure of non-specific psychological distress [42]. The questionnaire asks whether the respondent has experienced a particular symptom or behaviour recently and responses are rated on a 4-point Likert frequency scale, ranging from ‘much less than usual’ (score 0) to ‘much more than usual’ (score 3). Total scores range from 0 to 36 and vary by study population: total scores of approximately 11–12 are typical, and a score >20 suggests severe problems and psychological distress [43, 44]. The survey time frame was set as the month preceding the survey.
Prior to administration, the GHQ was translated into Hebrew, Arabic and Russian taking into consideration cultural aspects of the questions, colloquialisms and slang. A bilingual research assistant then translated the scale back to English. Each back-translation was compared to the original instrument and the few discrepancies found were discussed, and a third bilingual staff member was consulted. After a tentative decision the items in question were presented as a pilot test to the first 10 subjects enrolled to the study; evaluation of the responses confirmed validity of the translation.
Statistical analysis
The SUDAAN statistical package version 8.0.2 (Research Triangle Institute, Research Triangle Park, NC, USA) and the Taylor series linearization method were used to estimate standard error due to sampling design and the need for weighting. GHQ-12 scores were computed separately for veteran Israeli respondents, for FSU immigrants and for Other immigrants. Group differences on GHQ-12 scores were assessed using analysis of variance (ANOVA). Post-hoc single comparisons were evaluated using paired t-tests. Group differences for categorical variables were assessed using the Rao–Scott likelihood ratio χ2 test, based on the ratios between observed and expected frequencies.
Results
Table 1 lists the subject sociodemographic characteristics. A comparison of FSU immigrant and veteran Israeli respondents clearly shows the disparities between the two. The immigrant group contains more female, older, unmarried, higher educated and secular persons. The Other immigrants differed from both the FSU immigrants and veteran Israelis by their younger age and much higher proportion of religious persons. There were no significant between-group differences in employment status.
Subject Characteristics
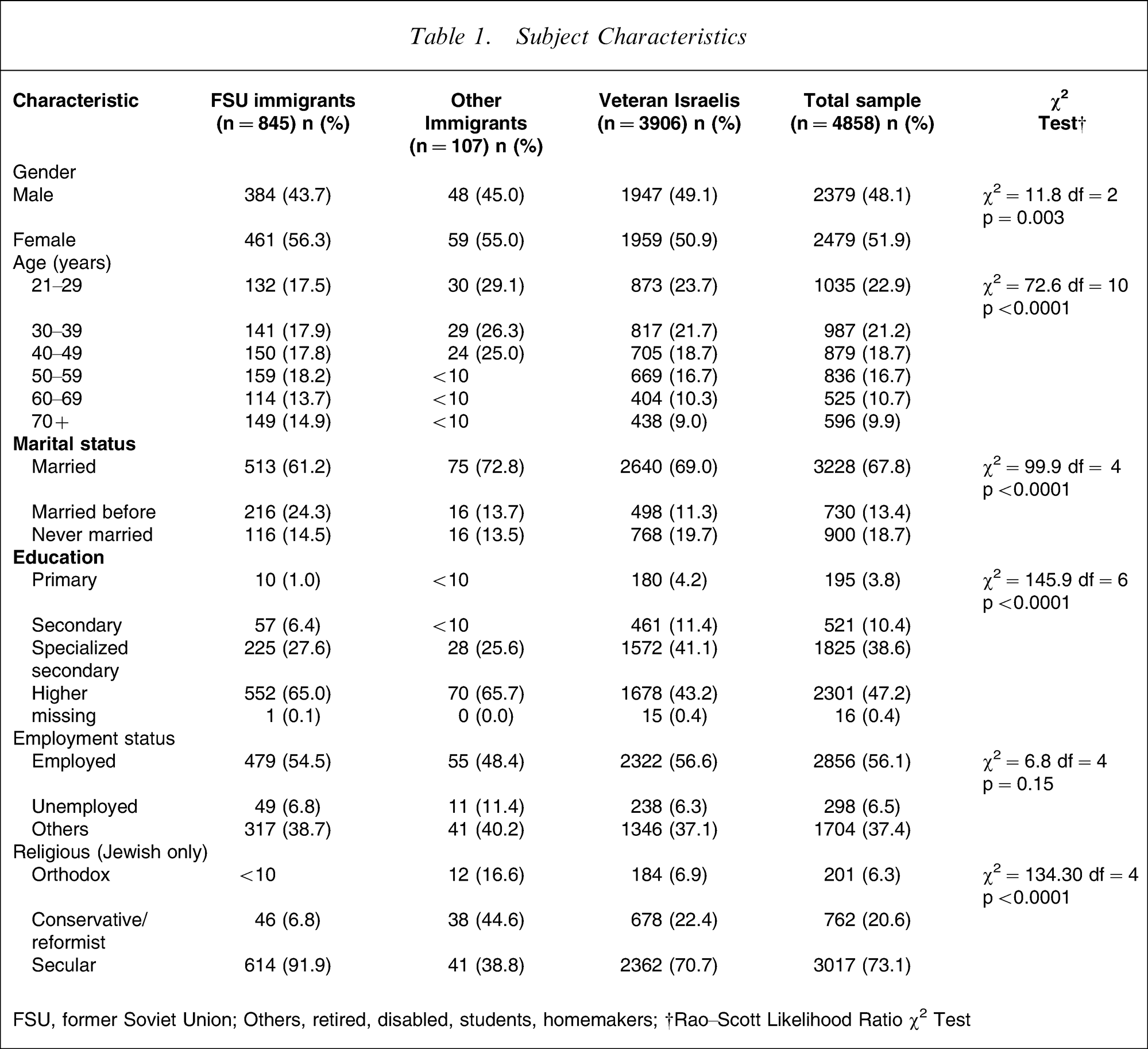
FSU, Former Soviet Union; Others, retired, disabled, students, homemakers; †Rao–Scott Likelihood Ratio χ2 Test
Table 2 compares GHQ-12 mean scores across the three study groups for each of the demographic categories. The results show consistently that psychological distress among FSU immigrants was significantly higher than among both veteran Israeli respondents and Other immigrants (21.5, SE = 0.25 vs 18.8, SE = 0.11 vs 18.4, SE = 0.53, respectively, F2,4858, p < 0.0001). As can be seen, the GHQ mean scores for all the groups exceed the normal level (11–12), while the distress score for the FSU immigrant population exceeded the ‘severe distress’ threshold (>20). At the level of the whole sample, this gap persists across most demographic subgroups (gender, age, marital status, education and employment status, and religious affiliation). In a number of subgroups, FSU immigrants’ psychological distress was even higher than among Other immigrants. This is the case for female respondents, for those aged 60–69, for married respondents, for those with a higher education qualification, for the secular and for respondents in the aggregate category of retired, disabled, students and homemakers. By contrast, no significant differences in GHQ-12 mean scores were found between Other immigrants and veteran Israelis.
General Health Questionnaire Mean Scores (SE)
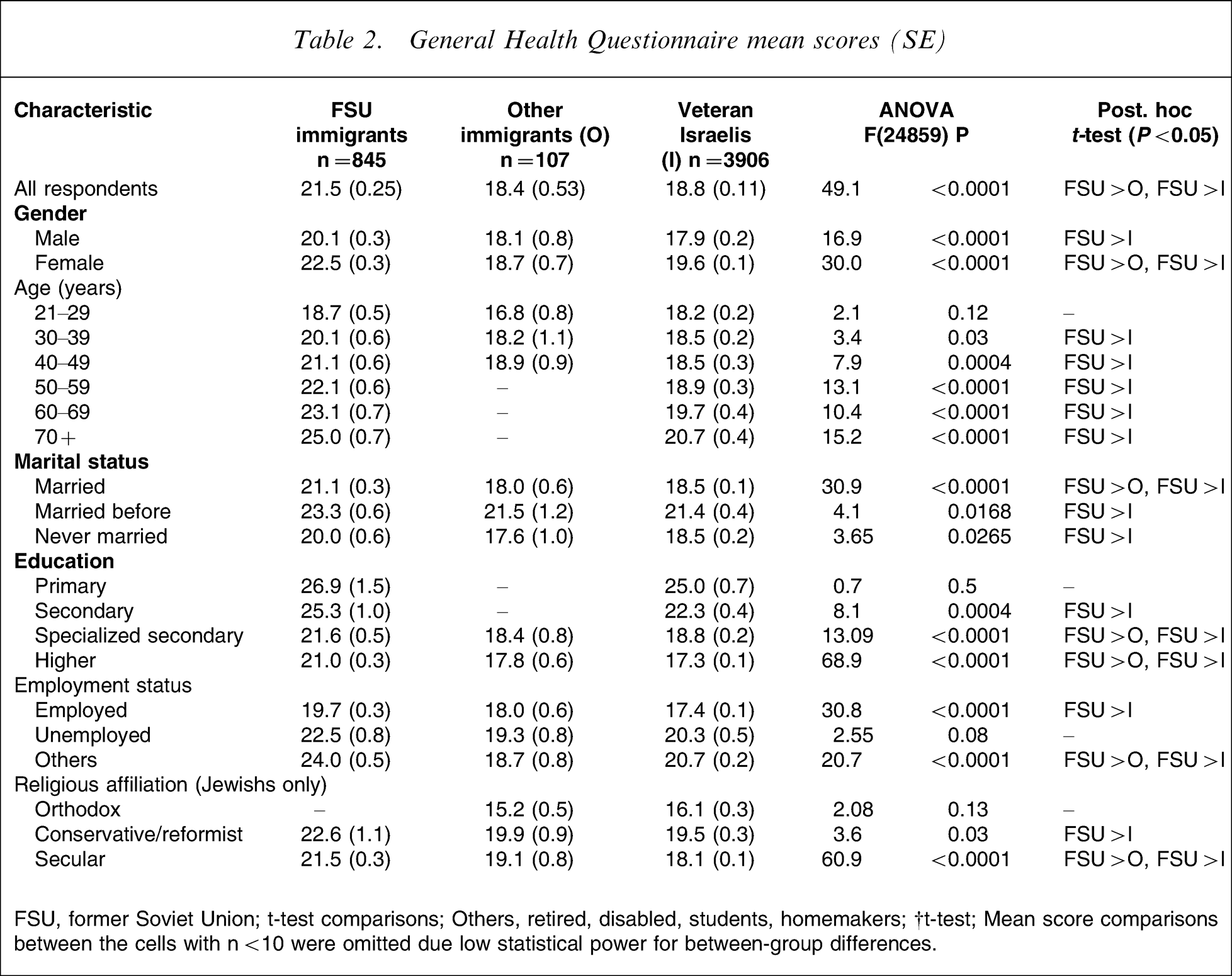
FSU, former Soviet Union; t-test comparisons; Others, retired, disabled, students, homemakers; †Mean score comparisons between the cells with n < 10 were omitted due the low statistical power for between-group differences.
Discussion
The present results show that the population of FSU immigrants in Israel has higher psychological distress than both the veteran Israeli population and immigrants from other countries. Although in all the groups GHQ-12 mean scores were higher than the normal score (11–12), only for the FSU immigrant respondents did the score exceed the GHQ-12 level suggesting severe distress (>20). Factors found associated with psychological distress were female gender, age above 50, being divorced or widowed, having higher education and being either unemployed or ‘not in workforce’. Thus, these findings support the acculturation stress hypothesis as an explanation for immigrants’ psychological distress only for immigrants from the FSU. Acculturation is conceptualized as a complex social–cultural–psychological process of adaptation to living conditions in the host country, and length of residence is one of its key indicators [6, 7]. Recent literature, however, on acculturation and adaptation has emphasized a distinction between two types of adaptive outcome, the psychological and the sociocultural [45, 46]. The former outcome implies good mental health, psychological well-being, and the achievement of personal satisfaction in the new cultural milieu, while the latter refers to the acquisition of the social skills and behavioural codes needed for successful everyday functioning. The present findings support this distinction. Socioculturally, the immigrants from the FSU can be considered well adapted, given that they have lived in Israel more than 9 years on average and do not differ from the host population by employment status. Yet their high levels of psychological distress show that they remain psychologically maladjusted.
It should be kept in mind that, in addition to the demands of acculturation, immigrants to Israel are subject to a wide range of acute and chronic stressors in a country where terrorist activity is permanent and increasing. Of course, all sectors of Israeli society are affected by terrorism [47–49], but immigrants’ acculturation problems may make them more exposed to it. For example, their lower socioeconomic status (SES) means that they more often frequent the public places and facilities subject to terrorist attack (buses, markets etc.). In other words, permanent awareness of their vulnerability to terrorism may cause anticipatory anxiety that in turn contributes to psychological distress. Regarding the lower SES among the immigrants compared with the veteran Israeli population, one should keep in mind that such evaluation may depend on the variables used to assess SES (e.g. education, income, and employment status). Although immigrants in the present study were as likely to be employed and more likely to be highly educated as veteran Israelis, their SES was relatively low because of the phenomenon of ‘underemployment’, where people are forced to work at a job inconsistent with their specialist training [50]. It seems that this phenomenon, a very common occurrence among higher educated immigrants, could explain the present finding that employed immigrants were more distressed than their employed hosts. Further, we found that the respondents from the ‘not in workforce’ category (students, homemakers, the retired, and the disabled) were more distressed than both employed and unemployed respondents and that ‘not in workforce’ immigrants were more distressed than ‘not in workforce’ veterans. A possible explanation is that this variable is confounded by gender, age and education, because female, older and higher educated respondents are overrepresented in the immigrant population.
The higher psychological distress associated with immigration status has been reported in many studies [50–52]. Research also suggests that the association between length of stay and psychological distress might be non-linear [19, 31], with two possible peak risk periods just after immigration and several years later [53, 54]. The first peak reflects distress at the drastic life changes caused by immigration, whereas the second peak reflects the later emergence or cumulative exacerbation of family difficulties. The present findings suggest that emotional distress may recur in the later stages of adjustment to migration [31] and that, in some cases, the distress may persist for many years [37].
One of the interesting findings was that FSU immigrants report significantly higher psychological distress scores than immigrants from other countries. This discrepancy cannot be attributed to length of time in the host country because both groups arrived over the same time period. The explanation could be demographic bias, unless the between-group differences in some demographics are balanced by between-group similarities in others. The groups were similar with regard to gender, education level, and employment status, that is, the characteristics commonly found associated with psychological distress [55–57]. In contrast, the immigrants from other countries were younger and more religious, that is, they have characteristics suggesting an enhanced ideological commitment to Israel, which in turn has been found to be positively associated with resilience from stressful events [58] and negatively associated with psychological distress [71]. Of course, there are other factors that, in part, may account for the differences in distress levels between the groups. For example, GHQ items, which tap a mixture of anxiety–depression symptoms, could well reflect the comorbid alcohol-related problems found more commonly in the FSU immigrant group than in other immigrant groups and the veteran Israeli population [60]. Testing this assumption warrants further investigation.
To see what demographic factors explained elevated psychological distress, we compared the scores of psychological distress across sociodemographic subgroups. This analysis indicated that certain groups were more vulnerable to high psychological distress: women, older people, the divorced/widowed, the secular, those who had less than college education, the unemployed and particularly those in the ‘not in workforce’ category. In all these groups, the scores for psychological distress were higher for immigrants than for their host counterparts. In the main, these results are consistent with the literature on immigrant mental health, which has reported psychological distress to be associated with female gender [61–64], older age at migration [65–70], marital status [59], employment [19, 53], and religious observance [72]. The present findings, however, differ from previous studies in three respects.
First, as expected, there was clear increase in GHQ mean scores with age, but the patterns of this change are different for immigrants and veteran Israelis: in the former, psychological distress increased gradually across the lifespan, while in latter, elevated levels of distress appeared after 50 years of age. We suggest that this difference in the patterns can be attributed to age-specific adjustment difficulties in immigrants but only to health-related distress in the older host population. This assumption relies on findings from our previous study that showed that age differences in the stress process of recent FSU immigrants in Israel were generally associated with age-specific perceived adjustment difficulties [66]. In contrast to increase in distress with age noted in the present study, no increase in the 12 month prevalence of mood and anxiety disorders with age was found in the INHS [73]. These seemingly contradictory results of the two studies could be explained by differences between the GHQ screening of distress symptoms and diagnosis of the specific mental disorders according to DSM-IV criteria with the Composite International Diagnostic Interview [74].
Second, respondents who were divorced and widowed (the ‘married before’ category) had higher levels of psychological distress than their married and single counterparts. Even among married respondents, however, married immigrants were more distressed than married veterans. A possible explanation for this difference is the emergence or exacerbation of family difficulties at later stages of acculturation [19, 31].
Third, among both secular and religious respondents, the levels of distress were higher for immigrants than for veteran Israelis. It is well-known that spirituality and religion as well as the practices and circumstances that go with them can strengthen the sense of a meaning to life, bolster emotional well-being and serve as a buffer to life's stresses. Hence, the present finding could mean that the supportive resources afforded by spirituality and religion are insufficient to compensate immigrants for disrupted family, friendship and other social support networks [14, 15].
Limitations and strengths
One limitation to be borne in mind when interpreting the findings is that we did not differentiate the veteran Israeli sample into locally born and pre-1989 immigrant subsamples. We made this choice in order to achieve sufficient statistical power. The heterogeneity of the Israeli population, which consists of the native-born and immigrants from 70 countries, provides an opportunity to check the direction of the association between migration and health indicators among different ethnic groups. Further research is needed to check how ethnic factors may affect the variables we studied. At present, extrapolation of the present findings to immigrant populations in other countries should be made with caution.
There are also considerable methodological strengths to this study. First, it is based on rigorous sampling procedures and a reliable representative sample of the country's population. Second, a relatively high response rate was achieved. Third, the interviews were conducted in the respondents’ mother tongue (Hebrew, Arabic or Russian) and scores were measured on a validated instrument, increasing the likelihood that the respondents understood the questions. Finally, the computerized interviews increased data quality by drastically reducing between-interviewer variation.
In conclusion, the present results support the acculturation stress hypothesis only for immigrants from the FSU. This should indicate to policymakers that they have to plan services and prevention programmes differentially for different immigrant groups.
Footnotes
Acknowledgements
This survey was carried out in conjunction with the World Health Organization/World Mental Health (WMH) Survey Initiative. We thank the staff of the WMH Data Collection and Data Analysis Coordination Centers for assistance with instrumentation, fieldwork, and consultation on data analysis. These activities were supported by the National Institute of Mental Health (R01 MH070884), the John D. and Catherine T. MacArthur Foundation, the Pfizer Foundation, the US Public Health Service (R13-MH066849, R01-MH069864, and R01 DA016558), the Fogarty International Center (FIRCA R03-TW006481), the Pan American Health Organization, Eli Lilly, Ortho-McNeil Pharmaceutical, GlaxoSmithKline, and Bristol-Myers Squibb. A complete list of WMH publications can be found at ![]() . Dr A.M. Ponizovsky was supported in part by the Ministry of Immigrant Absorption. We also wish to thank Nahum Steigman for his editing. The views and opinions expressed in this article are those of the authors and should not be construed to represent the views of the Israeli Government, nor of any of the sponsoring organizations.
. Dr A.M. Ponizovsky was supported in part by the Ministry of Immigrant Absorption. We also wish to thank Nahum Steigman for his editing. The views and opinions expressed in this article are those of the authors and should not be construed to represent the views of the Israeli Government, nor of any of the sponsoring organizations.