
Abstract
Keywords
Obsessive-compulsive disorder (OCD) is a disabling mental disorder characterized by recurrent intrusive thoughts, impulses or images (obsessions) and repetitive or stereotyped behaviours that the individual feels driven to perform (compulsions). It frequently begins in childhood or adolescence [1,2].
Paediatric OCD often co-occurs with other disorders such as Tourette's syndrome (TS) [3], a condition characterized by motor and phonic tics (see Leckman [4] for a review). Simple tics can usually be distinguished from compulsions by their relative brevity, lack of purpose, and typically involuntary nature although this can be less clear in the case of more complex tics such as repeating actions until it feels right [5]. It has been suggested that TS and OCD belong to an ‘obsessive-compulsive spectrum’ [6], sharing a similar neurobiological basis and a common genetic vulnerability [7].
Ritualized and repetitive behaviours are also commonly observed in children and young people with autism-spectrum disorders (ASD), and tics/TS are also over-represented in this group [8,9]. Clinically, TS and ASD share some features, including speech abnormalities (e.g. echolalia and palilalia), but there are also important differences: tics are predominant in TS and stereotypies in ASD [9].
Less is known about the relationship between OCD and ASD. There is evidence that young people with ASD experience more anxiety symptoms and anxiety disorders than normally developing children (see Chalfant, Rapee & Carroll [10] for a review), and epidemiological data suggest that the relationship between OCD and ASD is particularly strong. One study found that children with ASD were 14 times more likely to meet criteria for OCD than children without ASD [11]. Another recent study found a high rate of OCD among autistic children, OCD being the second most common disorder after specific phobia [12]. Conversely, recent clinical research in adults has shown that ASD can be a co-morbid problem in OCD [13,14] and that autistic traits are prevalent in children/adolescents with OCD with or without comorbid ASD [15].
A few studies have examined the presence of specific obsessive-compulsive (OC) symptoms in individuals with ASD. McDougle [16], for example, administered the Yale-Brown Obsessive compulsive Scale (Y-BOCS) [17] to a group of adults with autism and OCD and compared the frequency of the main OCD symptom categories. They found that adults with autism were less likely to report obsessional thoughts or cleaning, checking and counting symptoms, but were more likely to report repeating, hoarding, touching, tapping and self-damaging behaviours than adults with OCD. The main limitation of this study was that 50% of the ASD group had below-average intellectual abilities and/or were mute. It is therefore plausible that these patients were unable to report some OC symptoms, especially obsessions. More recently, Russell
To our knowledge, only one study has looked at specific obsessive-compulsive symptoms in children with ASD and OCD. Zandt, Prior, & Kyrios [19] compared children with ASD and OCD and found that OCD children had a higher frequency of obsessions and compulsions than children with ASD. Regarding the specific symptom content, children with OCD were more likely to endorse compulsions in all areas assessed by the Children's Yale-Brown Obsessive compulsive Scale [20], with the exception of ordering compulsions and compulsions involving another person. They also endorsed more obsessions than children with ASD for all obsession types except for religious and miscellaneous obsessions.
Findings in adults have highlighted the importance of carefully distinguishing OCD symptoms from other common repetitive behaviours and special interests in ASD [18]. Similarly in children, clinical experience and preliminary reports suggest that these symptoms can respond to traditional behavioural treatments adapted for this population [21,22].
It is currently unclear whether the OC symptom pattern or severity differs in children with OCD and ASD compared to typically developing children with OCD or with OCD and TS, and little is known about how the two conditions might interact to impact on course, or treatment response. Beginning to understand more fully the presentation of young people with OC symptoms in the context of ASD is crucial to ensuring that they receive early and effective treatment.
The main goal of the present study was to analyse the frequency and severity of OC symptoms in a group of children meeting criteria for OCD and ASD (OCD/ASD). We compared this group with two gender-matched groups of children meeting criteria for OCD only (OCD) or OCD and TS (OCD/TS). To our knowledge, this is the first report to systematically compare OC symptoms in children and young people with OCD and ASD in comparison with other individuals with OCD (with and without TS). Based on previous results in adults with ASD [18] and in children with TS [23], we expected similar types of OC symptoms and severity in the three groups. As additional goals, we examined whether there were any differences between these groups in treatment history, and in the child's broader emotional and behavioural difficulties. We predicted that children in the OCD/ASD group would have greater difficulties with peer relationships.
Materials and methods
Participants
Study participants were drawn retrospectively from patients referred to a specialist OCD service at the Maudsley Hospital in London between 1996 and 2006. A total of 469 patients were referred for assessment to this service during this period, of which 318 met ICD-10 [24] criteria for OCD as assessed by an experienced multidisciplinary team, including psychiatrists and psychologists. Informed consent for the participation in the study was obtained at the time of initial interview.
The index group consisted of children with OCD and ASD (OCD/ASD). Cases were selected where a diagnosis of an ASD had been made by the clinical team in accordance with ICD-10 criteria and with the consensus of at least one other experienced clinician, usually a senior child and adolescent psychiatrist. In two cases, the diagnosis was further verified by the results of a structured clinical interview (Autism Diagnostic Interview [25]). Fourteen cases were detected, of whom two were excluded because of a history of tics. This left a total of 12 cases (10 boys, 2 girls). The mean age of this group was 14.33 years (SD = 1.67, range: 1218). IQ data were available for five individuals in this group. Their mean IQ was 99 (SD = 23.55, range: 72–135).
The comparison groups consisted of 12 gender-matched subjects fulfilling ICD-10 criteria for OCD (OCD) (Mean age: 12.92, SD = 2.42, range 917) and 12 gender-matched patients fulfilling the criteria for OCD plus TS (OCD/TS) (Mean age: 13.92, SD = 2.67, range 9-17). IQ data were available for 3 individuals in each of these groups (OCD: IQ Mean = 98, SD = 8.14, range 96-111; OCD/TS: IQ Mean = 98, SD = 5.29, range 94–104). Children with other comorbidities, including any developmental disorder, or a history of possible or likely but undiagnosed ASD or TS, were excluded from the study.
Differentiation was made between compulsions and autistic rituals by experienced clinicians following an interview with the child, a mental state examination and a review of the child's developmental history. Behaviours were categorized as compulsions if they were distressing, unwanted and egodystonic, and were preceded by a thought or feeling of anxiety that they functioned to relieve. Autistic rituals were seen as more likely to be rewarding and pleasurable for the child, to be engaged in willingly and preferentially, and not to be closely linked with a specific thought or feeling.
Measures
Children's Yale-Brown Obsessive Compulsive Scale
The severity and types of OC symptoms were measured with the 10-item Children's Yale-Brown Obsessive Compulsive Scale and its ancillary Symptom Checklist (CY-BOCS-SC) [20]. The CY-BOCS-SC includes a list of more than 50 examples of obsessions and compulsions grouped thematically into seven main groups of obsessions and six of compulsions.
Children's Obsessive Compulsive Inventory
The Children's Obsessive Compulsive Inventory (ChOCI) is a self-report instrument developed to assess obsessive-compulsive symptoms in children and young people [26]. It consists of four subscales (obsessions, impairment associated with obsessions, compulsions, and impairment associated with compulsions). It has been shown to have good internal consistency and criterion validity and to be significantly correlated with the CY-BOCS [26,27].
Strengths and Difficulties Questionnaire
The child's broader emotional and behavioural difficulties were assessed using the Strengths and Difficulties Questionnaire (SDQ) [28], a brief behavioural screening questionnaire for 3-16 year olds. The SDQ has child, parent and teacher versions and includes 25 items across five psychological dimensions: emotional problems, conduct problems, hyperactivity/inattention, peer relationship problems and prosocial behaviour.
Those children who had psychometric evaluations were tested with the WISC III [29].
Procedure and statistics
We compared the clinical characteristics and symptom severity of the three groups of patients when they were first assessed. Fisher exact tests were used to compare the frequency of the different types of obsessions and compulsions endorsed on the CY-BOCS as well as the proportions of patients receiving psychopharmacological or psychological treatment. Continuous variables were compared with one-way ANOVAs followed by Bonferroni-corrected post-hoc comparisons. Given the small sample sizes, and as not all Teacher and Parent versions of the SDQ were returned, we report effect sizes for this measure when differences were significant. Effect sizes were calculated using Cohen's [30] criteria: ‘small’ effect size (ES) is 0.1, ‘medium’ is 0.25, and ‘large’ is 0.4 [30].
Results
Frequency of ASD in the clinic's sample
The 12 cases of OCD plus ASD represented 3.8 % of all patients with OCD (n = 318).
Age at assessment and previous treatment
The three groups did not differ in their age at the time of assessment, F (2,33) = 1.2, p > 0.05.
Participants had received a range of psychopharmacological treatments including SSRIs and antipsychotic medications as well as psychological treatments including cognitive behaviour therapy (CBT). Participants in the OCD/TS group were more likely to have received pharmacological treatment than the other participants, χ2 (6) = 13.57, p < 0.05. There were no significant differences in the proportion of patients who had received psychological treatment.
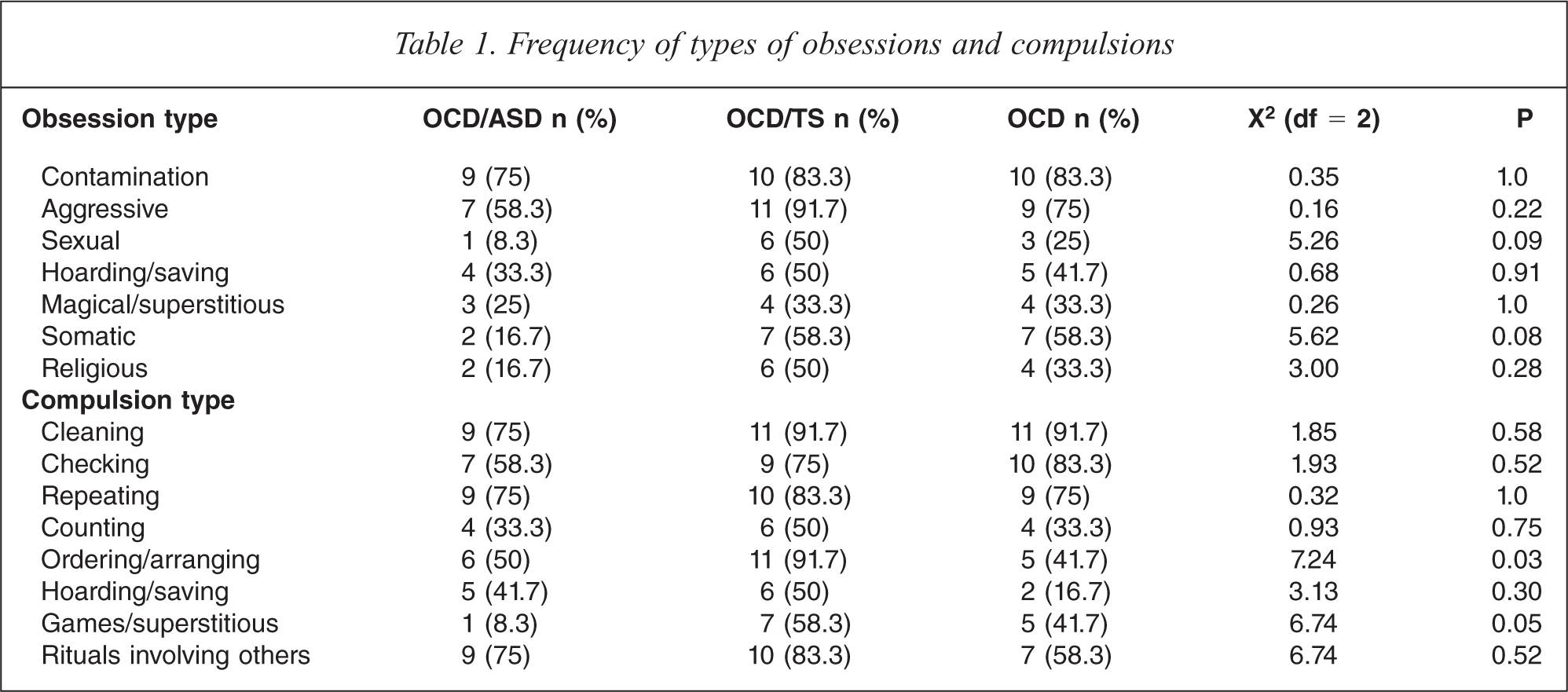
Types of obsessive-compulsive symptoms
As seen in Table 1, there were no differences between the three groups on the frequency of the different types of obsessions endorsed on the CYBOCS, although children from the OCD/ASD group showed a trend (p = 0.08) to have fewer somatic obsessions, and OCD/TS children showed a trend (p = 0.09) to report more sexual obsessions. Participants in the OCD/TS group were more likely to report ordering/arranging compulsions (p < 0.05) and a trend existed (p = 0.05) in participants of the OCD/ASD group to report fewer games/superstitious compulsions. All other compulsions were reported with equal regularity across the three groups.
Frequency of types of obsessions and compulsions
Symptom severity and impact
CYBOCS
There were no differences between the groups in terms of total severity (OCD/ASD, M = 25.17, SD = 7.01, range 16-40; OCD/TS, M = 24.67, SD = 5.15, range 16–31; OCD, M = 22.58, SD = 5.88, range 12–31), F (2,33) = 0.54, obsessions severity (OCD/ASD, M = 11.67, SD = 3.77, range 6–20; OCD/TS = 10.58, SD = 3.47, range 6–16; OCD, M = 10.92, SD = 3.2, range 5–15), F (2,33) = 0.3, or compulsions severity (OCD/ASD, M = 13.5, SD = 4.03, range 6–20; OCD/TS, M = 13.25, SD = 2.22, range 9–16; OCD, M = 11.67, SD = 3.20, range 6–16), F (2,33) =1.13 (all p > 0.3) (see Figure 1).
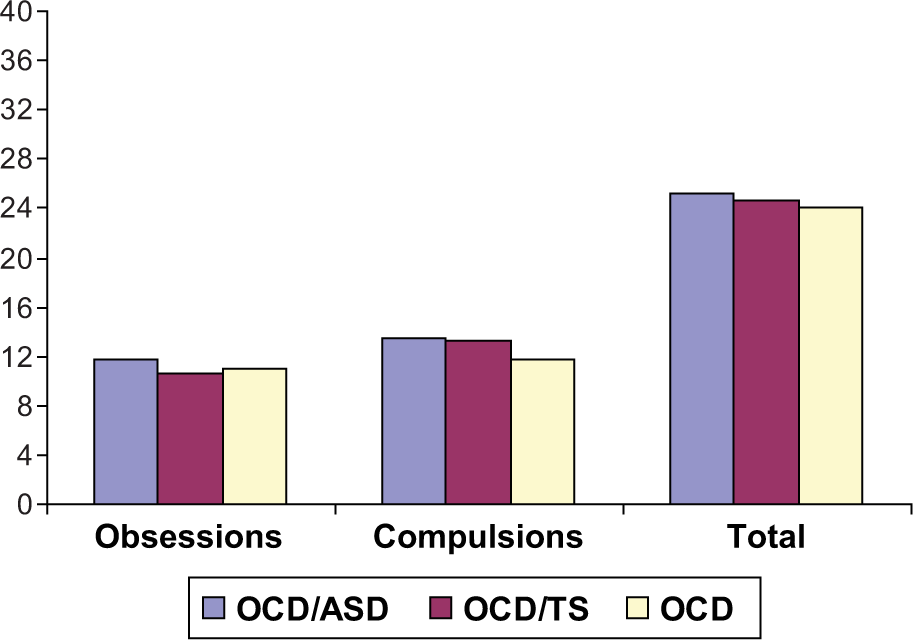
CY-BOCS severity scores for the three comparison groups.
There were no differences either in time occupied by obsessions, F (2,33) = 1.37, interference due to obsessions, F (2,33) = 0.61, distress associated with obsessions, F (2,33) = 0.378, resistance against obsessions, F (2,33) = 0.48 (all p > 0.5) or control over obsessions, F (2,33) = 2.549, p > 0.05.
Regarding compulsions, there were no significant differences between the groups in terms of time spent occupied by compulsions, F (2,33) = 0.12, interference due to compulsions, F (2,33) = 0.67, distress associated with compulsions, F (2,33) = 0.88 or resistance against compulsions, F (2,33) = 1.6 (all p > 0.2). However, there was a significant difference in control over compulsions, F (2,33) = 4.35, p > 0.05. A Bonferroni-corrected post-hoc test (equal variances assumed) showed no differences between children from the OCD/ASD group and the other groups but that children from the OCD/TS group scored higher (M = 3.25, SD = 0.62), i.e. reported less control than the children from the OCD group (M = 2.5, SD = 0.52), p < 0.05.
ChOCI
There were no significant differences between the three comparison groups on the ChOCI total (ChOCI-parents: OCD/ASD, M = 33.22, SD = 8.05; OCD/TS, M = 31.38, SD = 8.89; OCD, M = 31.45, SD = 9.92. CHOCI-self: OCD/ASD, M = 27.29, SD = 9.46; OCD/TS = 26.78, SD = 7.64; OCD = 28.3, SD = 8.46) nor on any of its subscales (data not shown but available upon request), all p > 0.4.
SDQ
There were no significant differences between the three comparison groups in terms of total difficulties scores on the Parent (OCD/ASD, M = 21.92, SD = 5.4; OCD/TS = 21.36, SD = 7.52, OCD = 19.55, SD = 6.71), Child (OCD/ASD, M = 22.91, SD = 5.71; OCD/TS, M = 18.25, SD = 10.56; OCD, M = 20.11, SD = 6.56), and Teacher (OCD/ASD = 16.43, SD = 3.91; OCD/TS = 18.42, SD = 7.70; OCD = 16.67, SD = 7.69) versions of the SDQ, all p > 0.4.
Regarding the SDQ subscales, there were no differences on any of the subscales for the Teacher version across the three groups. However, some differences emerged in the Parent and Child versions. On the Parent version, ANOVAs followed by post hoc tests for peer problems revealed higher scores for the OCD/ASD (M = 6.25, SD = 2) than for the OCD group (M = 2.73, SD = 2.28), p < 0.05, ES = 1.64. The scores for prosocial behaviour were significantly lower in the OCD/ASD group (M = 3.67, SD = 1.87) than in the OCD group (M = 6.27, SD = 1.9), p < 0.05, ES = 1.37, and marginally lower than in the OCD/TS group (M = 6.09, SD = 3.2), p = 0.06, ES = 0.06, indicating worse social functioning in children with ASD.
Finally, on the Child version, ANOVAs followed by post hoc comparisons showed that the score for peer problems was higher in the OCD/ASD group (M = 6.64, SD = 2.42) than for the OCD/TS (M = 3.75, SD = 2.60), p < 0.05, ES = 1.15 and the OCD (M = 2.78, SD = 1.71) groups, p < 0.05, ES = 1.84.
Discussion
We found that 3.8 % of a large clinic sample of children with OCD fulfilled criteria for ASD. To the best of our knowledge, there are no previous reports on the frequency of ASD in a clinic sample of children/adolescents with OCD. These results are consistent with recent work in adults with OCD [14] and indicate that individuals with ASD seem to be overrepresented in clinical OCD samples (see also Bejerot [31]).
The main goal of the present study was to compare the clinical characteristics and symptom severity of children with OCD plus ASD with those of children with OCD plus TS or OCD alone. As predicted, the three patient groups reported comparable levels of OC symptom severity and interference due to their OCD.
In terms of symptom content, children with OCD and TS reported more ordering and arranging compulsions and a trend towards more sexual obsessions compared to children with OCD and OCD/ASD. This is consistent with previous research showing that symmetry obsessions and ordering/repeating rituals as well as sexual obsessions are more common both in children and adults with comorbid TS [32,33]. This tic-related phenotype could constitute a subtype of OCD, with implications for the pharmacological management of the disorder [34–36].
In a previous adult ASD study [18] patients with ASD reported fewer somatic obsessions than patients with OCD. We found a similar trend in this study, although the differences did not reach statistical significance. Zandt
Patients in the OCD/ASD group also tended to report fewer games and superstitious behaviours on the CY-BOCS symptom checklist than the other two groups. Again, this is consistent with Zandt
Children in the three groups displayed similarly high levels of emotional and behavioural disturbance. There were no significant differences between the three comparison groups on the total difficulties scores of the SDQ (Parent, Child and Teacher versions). However, as predicted, children with ASD reported higher levels of problems with their peers than the OCD and OCD/TS groups. This is likely to reflect their difficulties in communication and reciprocity in social relationships.
Our study had several limitations. Firstly, small sample sizes may mean that some of our analyses were underpowered to detect differences between the groups. Secondly, although all patients were diagnosed by experienced clinicians, the study lacked structured diagnostic interviews for ASD. Therefore the rate of ASD in young people with OCD may be even higher than reported. Third, we did not have treatment outcome data for these patients and thus we cannot comment on any differences between the groups in this respect, although the team's clinical impression is that patients with OCD/ASD tend to have a poorer prognosis than OCD alone, or OCD with TS. It is also unclear how previous treatments could have affected the reporting of symptoms, and epidemiological or clinical studies on treatment-naïve patients would shed more light on this question. Finally, while none of the children in this study were deemed to be in the learning disability/mental retardation range, this was not formally measured in most children.
Keeping these limitations in mind, our findings have important implications for both clinical practice and research. The results suggest that children with ASD may experience a similar level of impairment from OC symptoms as children in the other diagnostic groups, although further research is required into how they may differ in terms of symptom type and severity. From an assessment perspective, clinicians need to be aware of the possible comorbidity between OCD and ASD. Care needs to be taken to differentiate symptoms of OCD from the other repetitive behaviours characteristic of ASD and it should be recognized that these symptoms are both distressing and impairing. In clinical practice, there is clearly a degree of overlap between the repetitive distressing compulsions of OCD, which phenomenologically are usually defined as being preceded by a specific obsession, and the repetitive behaviours of autism. However, it seems that if compulsions can be identified, even in the context of ASD, it can be therapeutic to help the young person understand the nature of obsessions and compulsions, and the role that anxiety plays in maintaining these symptoms. While more reliable means of differentiating compulsions from autistic rituals are needed, in our clinical practice we use the presence of egodystonia in relation to rituals, and anxiety in relation to reducing or eliminating rituals, to help decide whether OCD is present.
Contrary to Zandt
It is likely that individuals with OCD and comorbid ASD will benefit from standard treatments for OCD such as serotonin re-uptake inhibitors and cognitive behavioural therapies, but further work is needed to make adaptations to existing protocols to take into account the specific developmental characteristics of these patients.
Footnotes
Acknowledgements