
Abstract
High-functioning autism spectrum disorder (ASD) refers to children who have autistic disorder or pervasive developmental disorders not otherwise specified (PDDNOS) without intellectual delay, together with children with Asperger's syndrome [1]. According to the DSM-IV criteria, social impairments and circumscribed patterns of behaviours and interests are two core features of high-functioning ASD, which contribute to poor social competence and the manifestation of behaviours such as circumscribed interests, rigidity involving non-functional routines and/or repetitive motor movements [1–2]. In addition to the core symptoms of high-functioning ASD, these children have been found to exhibit a variety of behavioural and emotional problems, which sometimes result in multiple psychiatric diagnoses [3–8]. For example, Mattilla et al. [6] found that 74% of children with high-functioning ASD, had multiple comorbid psychiatric disorders such as behavioural disorders and anxiety disorders [8]. White et al. [7] conducted a systematic review on the prevalence of anxiety in children and adolescents with high-functioning ASD and found that between 11% and 84% of these children with high-functioning ASD had an impairing degree of anxiety, with simple phobias, generalized anxiety disorder, separation anxiety disorder, obsessive–compulsive disorder, and social phobia being commonly reported.
With increasing studies documenting high prevalence of various behavioural and emotional problems among children with high-functioning ASD, the issue of comorbidity in the assessment of this population, which was infrequently addressed in the past, is gaining its attention. Because children with high-functioning ASD have strengths in cognitive and language abilities, many referrals to child psychiatric clinics are initially based on associated, rather than their core features [9]. As a result, clinicians and researchers are now also focusing on not just the core symptoms of high-functioning ASD but also on associated behavioural and emotional difficulties experienced by these children with high-functioning ASD when assessing and treating them [7]. The occurrence of these behavioural and emotional problems may cause further significant clinical impairment and burden to themselves and families. As such, the assessment of a full range of comorbid symptoms associated with high-functioning ASD is of outmost importance [10].
The Child Behaviour Checklist (CBCL) has been used in several studies to identify the diverse behavioural and emotional problems among children with autism [11]. Collectively, findings from studies that utilized the CBCL indicated that children with autism scored significantly higher on problems related to anxiety, depression, and attention problems than typically developing children [12–18]. However, in most of these studies, the author used the CBCL syndromes and few have used both the CBCL syndromes and the DSM-oriented scales in identifying the comorbid problems among children with autism. In addition, in some of these studies the authors included children with varied cognitive abilities and not just those with high-functioning ASD. Finally, the literature on behavioural and emotional problems among children with high-functioning ASD is still very limited especially in non-western samples.
To address these limitations in the literature, the present study was conducted in Singapore, allowing us to determine the prevalence of behavioural and emotional problems using the CBCL syndromes and the DSM-oriented scales in a clinical sample of children diagnosed with high-functioning ASD.
Method
Participants
The medical records of 85 children referred to the Autism Clinic at the Child Guidance Clinic (CGC) for intervention between August 2009 and February 2010 were screened. These children were diagnosed by their clinicians to have high-functioning ASD using the ICD-9 and DSM-IV criteria [19–20]. Of these, 14 were excluded because they were below 6 years of age, not studying in local mainstream schools and/or had incomplete CBCL responses. The final sample included 71 children between 6 and 18 years of age (M = 10.24, SD = 2.91). Ethnicity based on parent reports were 86.1% Chinese, 9.7% Malay, and 4.2% others.
Measures
The CBCL/6-18, a parent-rated form that includes 118 items that describe the child's behavioural, emotional, and social problems over the past 6 months, was used [11]. These items are rated on a 3-point scale (0 = not true (as far as you know), 1 = sometimes or somewhat true, or 2 = very true or often true). Items on the CBCL/6-18 can be summed up to provide eight ‘narrow-band’ syndromes (anxious/depressed, withdrawn/depressed, somatic complaints, social problems, thought problems, attention problems, rule-breaking behaviour, and aggressive behaviour), two ‘broad-band’ syndromes (internalizing and externalizing problems), and a total problems scale. In addition, six DSM-oriented scales can also be obtained: affective problems, anxiety problems, somatic problems, attention deficit/hyperactivity problems, oppositional defiant problems, and conduct problems.
Raw CBCL scores can be converted into T scores. For all scales, T scores ranging from 65 to 69 are in the borderline clinical range, whereas T scores of 70 and above are in the clinical range. T scores of below 65 are considered as non-clinical. For the purposes of this study, a T score of 65 and above for the CBCL syndromes and DSM-oriented scales indicated the problem to be of clinical concerns. Because English is one of the official languages in Singapore, most adults are fluent in English. Thus, the English version of the CBCL was completed by about 93% of the parents, with the remaining parents completing the version in Chinese (7%). Both the English and Chinese versions of the CBCL have been validated in a clinical sample in Singapore [21].
Procedure
Data for the present study were obtained from an ongoing clinical database amassed at the Child Guidance Clinic (Singapore) that has been approved for research use. All personal identifiers were removed and data were kept confidential in accordance with IRB research guidelines. The raw scores of CBCL were entered into the Assessment for Data Manager program (ADM) (ASEBA, Burlington, VT) to generate T scores of the CBCL syndromes and the DSM-oriented scales before being entered into the Statistical Package for Social Sciences (SPSS, Chicago, IL.) version 15.0 for data analysis. T scores were used in this study because they provide descriptions regarding the severity of the behavioural and/or emotional problems. Mean T score profiles were generated, providing a graphic representation of each group's pattern of scores on the CBCL syndromes and DSM-oriented scales (see Figure 1).
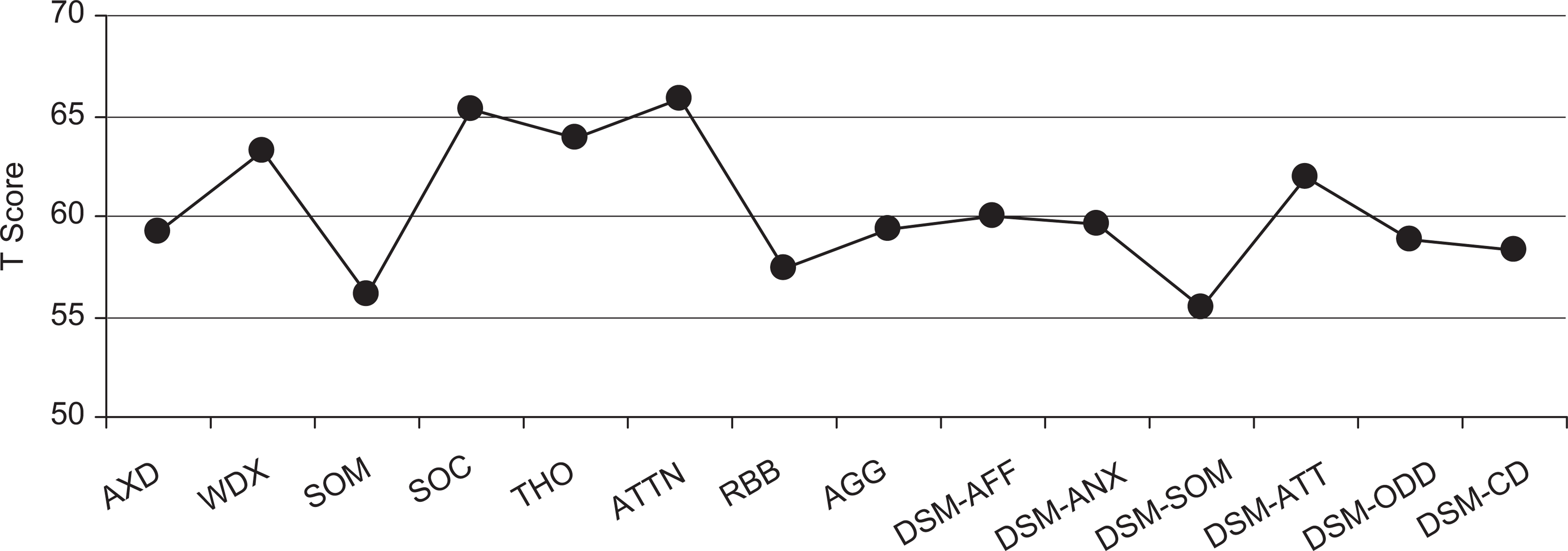
Profiles of the CBCL syndromes and the DSM-oriented scales for the total sample. CBCL, Child Behaviour Checklist; DSM, Diagnostic and Statistical Manual, AXD, anxious/depressed; WDX, withdrawn/depressed, SOM, somatic; SOC, social; THO, thought; ATTN, attention; RBB, rule-breaking behaviour; AGG, aggressive behaviour; DSM-AFF, affective problems; DSM-ANX, anxiety problems; DSM-SOM, somatic problems; DSM-ATT, attention problems; DSM-ODD, oppositional defiant problems; and DSM-CD, conduct problems.
Results
Of the 71 children included, 56 were male and 15 were female (≈4:1 male:female ratio). Figure 1 presents the profiles of the T scores for the CBCL syndromes and the DSM-oriented scales for the total sample.
Child Behavioural Checklist syndromes
As can be seen from Figure 2, 86% of children with high-functioning ASD had at least one CBCL syndrome which parents reported to be of clinical concerns. For these children, 24% of them (which forms the largest group) had 2 CBCL syndromes of clinical concerns. Among the eight CBCL syndromes scales, social problems (60.6%), thought problems (50.7%), attention problems (49.3%), and withdrawn/depressed (40.8%) were most commonly reported. The least commonly reported was rule-breaking (12.7%). Table 1 presents the prevalence of the CBCL syndromes of clinical concerns.
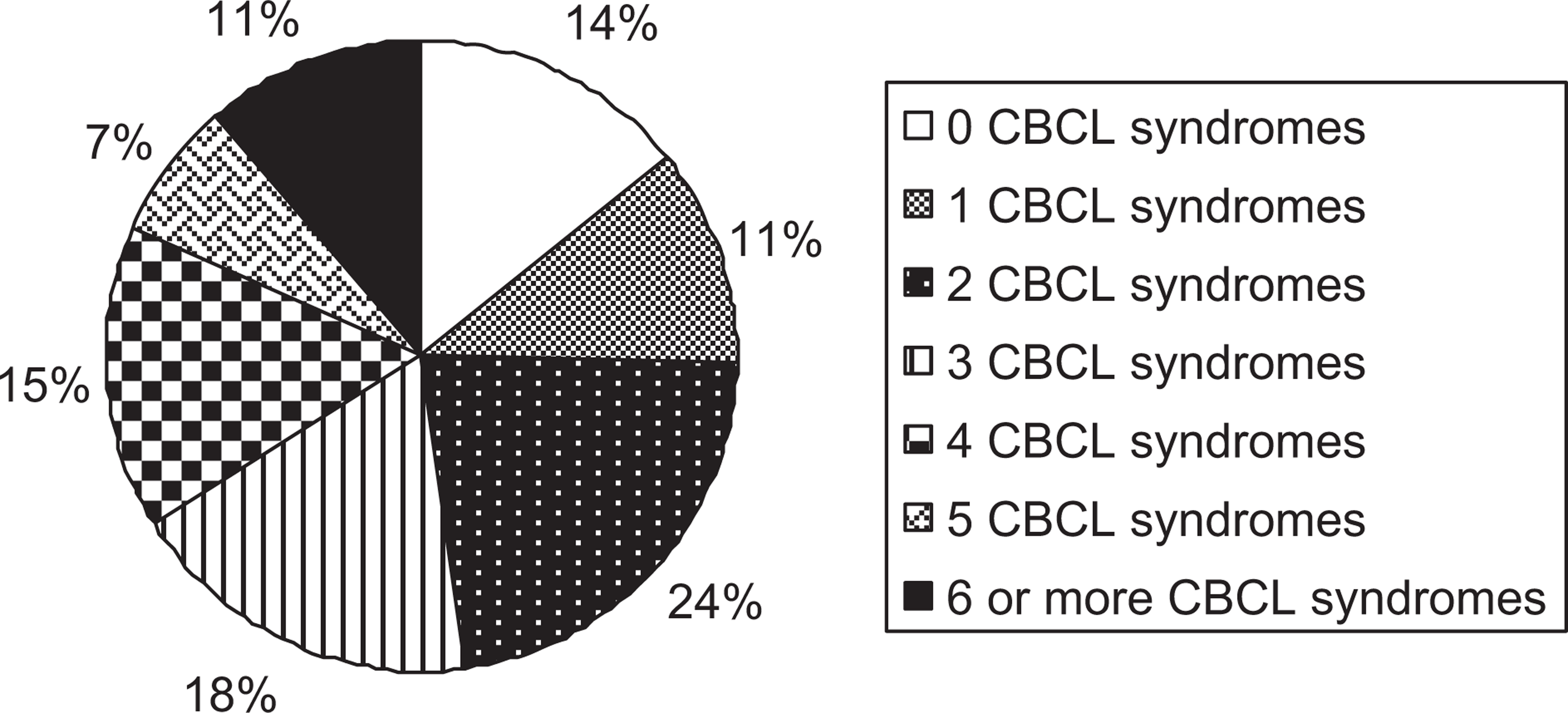
Percentage of children with CBCL syndromes of clinical concerns. CBCL, Child Behaviour Checklist.
Prevalence of CBCL syndromes and DSM-oriented scales of clinical concerns
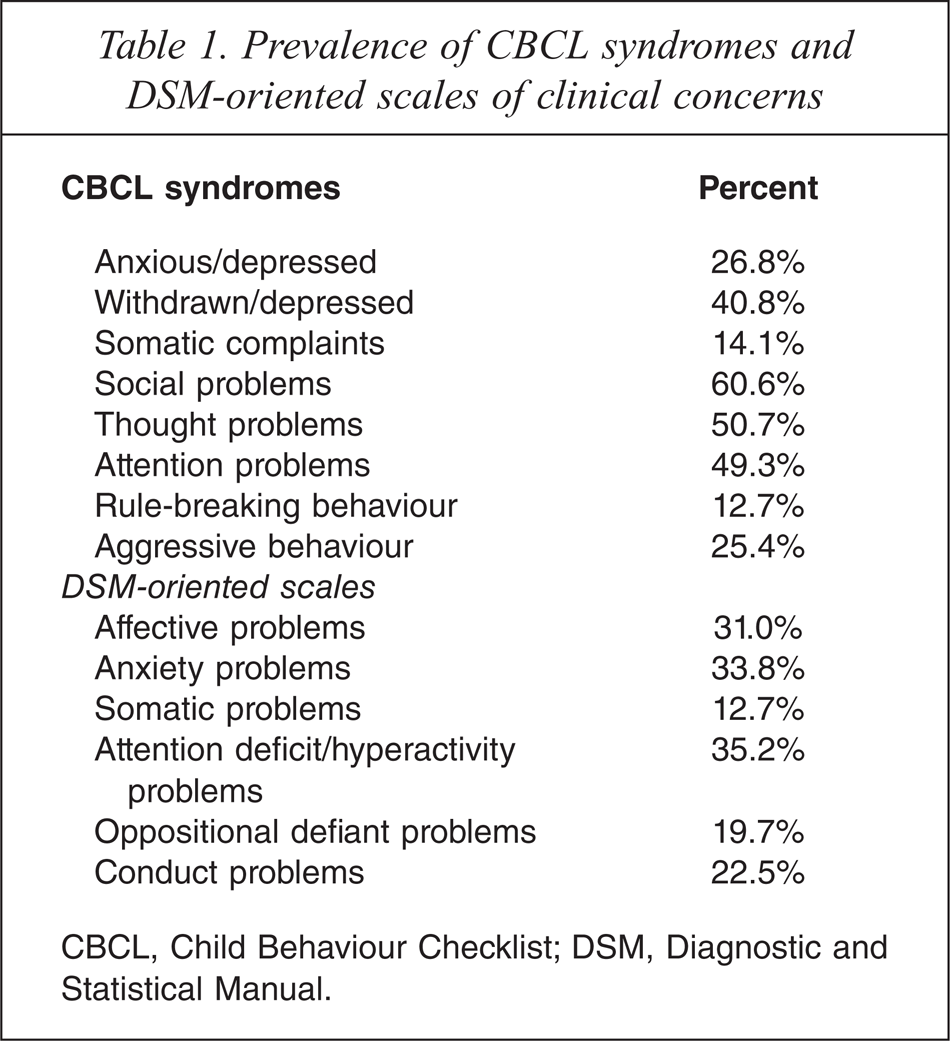
CBCL, Child Behaviour Checklist; DSM, Diagnostic and Statistical Manual.
DSM-oriented scales
As can be seen from Figure 3, 72% of children with high-functioning ASD had at least one DSM-oriented scale which parents reported to be of clinical concerns. For these children, 27% (which forms the largest group) of them had 1 DSM-oriented scale to be of clinical concern. Among the six DSM-oriented scales, attention deficit/hyperactivity problems (35.2%), followed by and anxiety problems (33.8%) and affective problems (31%) were most commonly reported (see Table 1).
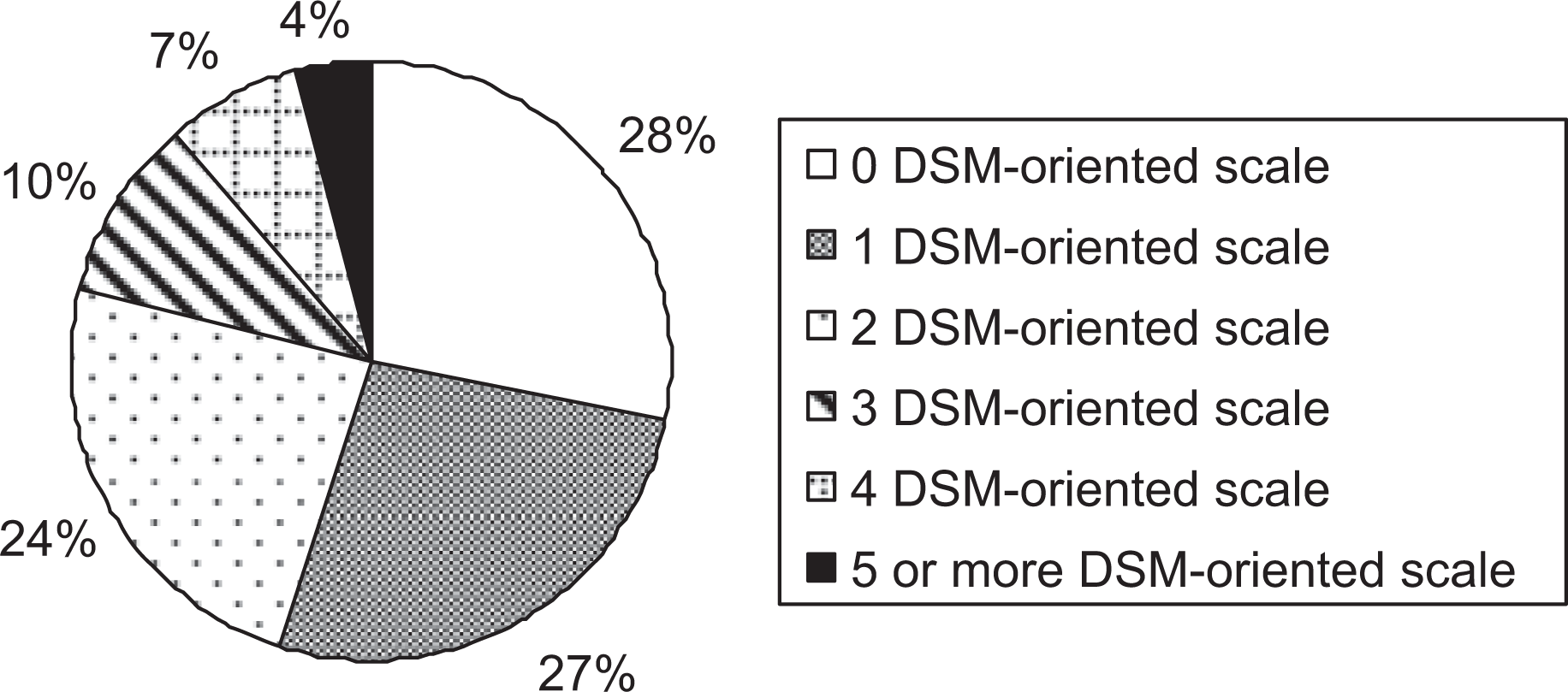
Percentage of children with DSM-oriented scales of clinical concerns. DSM, Diagnostic and Statistical Manual.
Mean item ratings
We identified the 10 items that had the highest mean ratings for the total sample, as shown in Table 2. The percentage of children whose parents gave ratings of 1 (somewhat or sometimes true) or 2 (very true or often true) to the 10 highest scoring items are also found listed in Table 2. Interestingly, the top two items were: 8, can't concentrate, and 78, inattentive or easily distracted. For all items >60% of the children received either a rating of 1 or 2, with item 8, can't concentrate and item 9, can't get his/her mind off certain thoughts; obsessions being commonly reported.
The ten highest scoring CBCL items
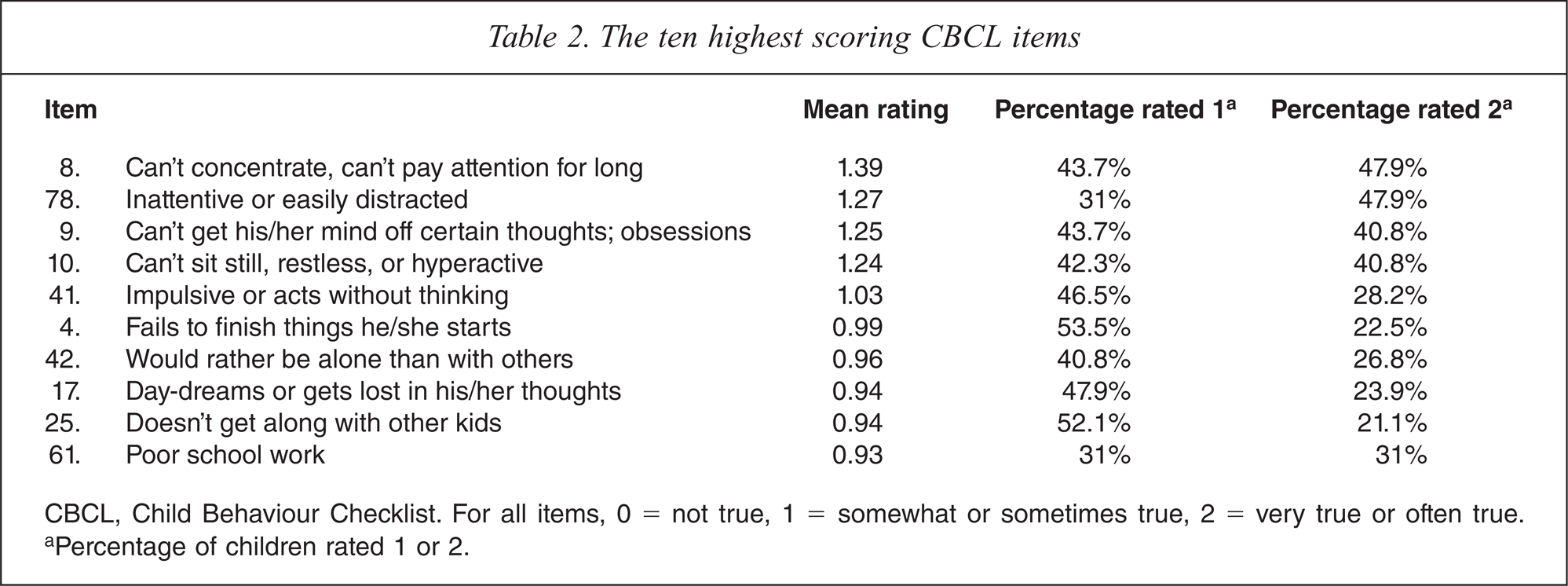
CBCL, Child Behaviour Checklist. For all items, 0 = not true, 1 = somewhat or sometimes true, 2 = very true or often true.
aPercentage of children rated 1 or 2.
Discussion
The goal of the study was to examine the prevalence of behavioural and emotional problems among children with high-functioning ASD. Previous studies have indicated that children with high-functioning ASD are often associated with significant behavioural and emotional problems [7,13,15,18]. Using the CBCL syndromes, findings from our present study provide further evidence to confirm high prevalence of behavioural and emotional problems among children with high-functioning ASD. Specifically, we found that children with high-functioning ASD are characterized by elevated scores on withdrawn/depressed, social problems, thought problems, and attention problems. This suggests that withdrawn/depressed, social, thought, and attention problems represent the clinical picture of children with high-functioning ASD [13,15]. The fact that these children had significantly elevated scores on four CBCL syndromes (withdrawn/depressed, social problems, thought problems, and attention problems) suggests a profile of behavioural and emotional problems that might result in multiple psychiatric diagnoses, thus reflecting the comorbidity commonly reported for children with high-functioning high-functioning ASD.
Using the DSM-oriented scales, we found that 72% of our sample had at least one or more behavioural and/or emotional problems consistent with the DSM-IV criteria. Specifically, we found that attention deficit/hyperactivity problems (35.2%), anxiety problems (33.8%) and affective problems (31%) were the most prevalent among children with high-functioning ASD. In addition, analyses of the top ten scoring CBCL items also provided similar conclusions. Item 8, can't concentrate, which characterizes many children with ADHD, had the highest mean rating and was also the most commonly reported item of concern (91.2%). Although the DSM-IV criteria exclude the diagnosis of ADHD in the presence of the course of any pervasive developmental disorders, ADHD symptoms may be present in children with high-functioning ASD. This has been established in many studies indicating the diagnostic overlap between high-functioning ASD and ADHD [3,6,8,15].
The anxiety problems scale corresponds with the DSM-IV criteria for generalized anxiety disorder, separation anxiety disorder, and specific phobia while the affective problems scale corresponds with the DSM-IV criteria for dysthymia and major depressive disorder [20,22]. Hence, in line with current literature, findings from our present study indicate that anxiety and depression are common psychiatric comorbidities among children with high-functioning ASD with prevalence ranging from 11% to 84% [4,7]. Kanner [23] suggested that many of the core features of autism, particularly the insistence on sameness and the repertoire of fixed behaviours, routines and obsessions, were anxiety driven. Even minor changes in the environment may induce confusion and distress for the child with autism [24], while the fear of possible change can be a further source of anxiety. Schopler and Mesibov [25] further suggested that resistance to change in autism is due to difficulty in understanding what is happening in the environment and a feeling of constant uncertainty. Hence, the presence of anxiety and depression could result from these children's self-awareness of their own difficulties when facing situations in which they are expected to display age-appropriate social judgement and social behaviour [26–27]. On the other hand, the prevalence rates of depression among children with high-functioning ASD range from 5% to 82% [4,28]. Some studies have indicated that depression is more common in individuals with high-functioning ASD and Asperger's syndrome because they may be more aware of their social deficiencies [4,26].
Oppositional defiant problems (22.2%) and conduct problems (19.7%) were also found in our sample of children with high-functioning ASD. A possible explanation is that children with high-functioning ASD are presented with cognitive deficits, such as difficulties with theory of mind and executive functioning [29–30]. Because of these cognitive deficits, they may have difficulty understanding social norms and understanding the perspectives of other people. In addition, because of their rigid behaviours, they may also have difficulties in following directions and may insist on doing things on their own terms. Underlying anxiety may also present as resistance in compliance, thereby appearing as oppositional behaviour. As such, their cognitive deficits, rigid behaviours and anxiety may present as disruptive and oppositional behaviours.
The present study is not without any limitations. Firstly, the sample size of 71 is relatively small. Secondly, we did not include those with any form of cognitive impairment, and therefore our findings can only be generalized to children with high-functioning ASD. Thirdly, our high-functioning ASD sample was recruited from a clinical setting and not from a community setting, which made it not representative of the high-functioning ASD population. Future studies with larger and more diverse samples should be considered. Fourthly, there is a need to validate findings obtained from the CBCL by comparing them with diagnoses obtained from structured interviews such as the Computerised Diagnostic Interview Schedule for children [31]. Finally, information regarding the child's behavioural and emotional problems was only obtained from parents. A multi-informant approach to assessment and diagnosis (i.e. from parents, child, and teachers) is recommended [32].
Despite these limitations, findings from the present study have important implications. The findings can help clinicians to be more aware of associated behavioural and emotional problems when assessing or treating children with high-functioning ASD. In addition, findings on the prevalence of comorbid symptoms associated with high-functioning ASD are an important consideration in the planning of clinical services for children with high-functioning ASD in Singapore.
Footnotes
Acknowledgements