
Abstract
Objective:
Tourette syndrome is often associated with attention deficit hyperactivity disorder, obsessive compulsive disorder and other co-morbidities, the presence of which can reduce health-related quality of life. The relationship between the number and type of co-morbidities and tic severity upon health-related quality of life has been insufficiently examined in Tourette syndrome populations and not at all in the Australian context. We hypothesised that an increased number of co-morbid diagnoses would be inversely related to health-related quality of life and that the presence of attention deficit hyperactivity disorder and obsessive compulsive disorder in particular would negatively impact health-related quality of life.
Method:
In all, 83 people with a previously established diagnosis of Tourette syndrome, who responded to a letter of invitation sent to the Tourette Syndrome Association of Australia past-member database, formed the study sample. Participants completed the Gilles de la Tourette Syndrome-Quality of Life Scale and a short form of the National Hospital Interview Schedule to assess tics and related behaviours.
Results:
Participants with pure-Tourette syndrome had significantly better health-related quality of life than those with Tourette syndrome and three or more co-morbid diagnoses. Few differences were observed between the pure-Tourette syndrome and Tourette syndrome and one or two co-morbid diagnoses groups. Analysis of the impact of individual co-morbid disorders and Tourette syndrome symptoms on health-related quality of life indicated that attention deficit hyperactivity disorder exerted a significant negative effect, as did the presence of complex tics, especially coprolalia and copropraxia. When these variables were examined in multiple regression analysis, number of co-morbidities and the presence of coprophenomena emerged as significant predictors of health-related quality of life.
Conclusion:
While tics are the defining feature of Tourette syndrome, it appears to be the presence of co-morbidities, attention deficit hyperactivity disorder, in particular, and coprophenomena that have the greater impact on health-related quality of life. This has implications for symptom-targeting in the treatment of Tourette syndrome since all available treatments are symptomatic and not disease modifying.
Keywords
Introduction
Gilles de la Tourette syndrome (TS) is a neurodevelopmental disorder characterised by multiple motor tics and at least one vocal tic that have been present for over a year (Robertson and Eapen, 2014). Tics can be classified as simple (e.g. blinking, coughing) or complex (e.g. forced touching of self, others or objects; linguistically meaningful phrases or utterances), with the latter involving either a cluster of simple tics or a more coordinated sequence. Prevalence rates of TS of between 0.4% and 3.8% for children aged 5–18 years have been reported and around 0.05% for adults (Knight et al., 2012; Robertson and Eapen, 2014).
TS is commonly associated with other psychiatric disorders, with around 90% of people with TS experiencing co-morbid psychopathology (TS-plus) and the remainder showing motor and vocal tics only (pure-TS; Eapen and Robertson, 2015; Freeman et al., 2000). A recent study reported that the lifetime prevalence of any psychiatric co-morbidity among people with TS is 86% and that 58% have two or more psychiatric disorders (Hirschtritt et al., 2015). Up to 36% of individuals with TS have been reported to have three or more co-morbid diagnoses in community samples (Robertson, 2015). The most commonly reported co-morbidity is attention deficit hyperactivity disorder (ADHD), with reported prevalence rates in TS cohorts of 35–90% (Roessner et al., 2007), followed by obsessive compulsive disorder (OCD) with a prevalence of 30–50% (Storch et al., 2007) and, to a lesser extent, autism spectrum disorders (ASD; Eapen et al., 2013).
While there do not appear to be phenomenological differences between ADHD symptoms in individuals with primary ADHD and those with TS + ADHD, the latter group have poorer outcomes and reduced functioning in perceptual and motor competence, sustained attention and impulsivity, as well as higher rates of learning disabilities, behavioural problems and social/emotional difficulties (Carter et al., 2000; Robertson et al., 2015).
The majority of studies investigating the differences between symptoms of co-morbid TS + OCD and primary OCD suggest that differences in symptom distribution and severity exist between individuals with tic and non-tic-related OCD (Cath et al., 2000, 2001; George et al., 1993; Jaisoorya et al., 2008; Leckman et al., 1994). Specifically, OCD symptoms in people with tics typically present as inappropriate, sexual and violent themes in obsessions, as well as compulsions concerning symmetry/‘evening-up’ behaviours, saying/doing things ‘just right’, counting, repeating, ordering, arranging and forced touching (Leckman et al., 1994).
The psychosocial consequences of TS have been observed to include poor peer relationships and teasing, aggressive and withdrawn behaviour, depression, anxiety and low self-esteem (Muller-Vahl et al., 2010). A number of studies have reported that the presence of psychiatric co-morbidity has an additional negative impact on psychosocial and educational functioning (Bernard et al., 2009; Debes et al., 2010; Eapen et al., 2013; Elstner et al., 2001; Storch et al., 2007). Taken together, it would appear that the presence of co-morbidities and/or the presence of notable subclinical features of these, rather than the severity of tics per se, may typically be related to the psychosocial and psychological impairment associated with TS (Eapen and Črnčec, 2009). Furthermore, these sequelae suggest that quality of life (QoL) may also be affected by co-morbidity, as well as provide an avenue by which to study these relationships.
Relationship between QOL, TS and co-morbid disorders
QoL is a multidimensional construct and includes health- and non-health-related domains of functioning. Health-related QoL (HR-QoL) is a specific subset of overall QoL that refers to the perceived physical, mental and social effects of an illness and associated therapies upon an individual over time (World Health Organization, 2006). Thus, HR-QoL is generally appropriate to the study of psychiatric illness.
The impact of TS and its associated co-morbidities on HR-QoL and QoL has been increasingly evaluated in the literature during the past decade (Cavanna et al., 2013a). Cavanna et al. (2013a) reviewed 13 studies that investigated HR-QoL in adults and/or young people with TS. While noting some variability in the literature, the authors concluded that ‘the severity of tics and presence of co-morbidities, particularly OCD and ADHD, are associated with a poorer HR-QoL in children’ (Cavanna et al., 2013a: 91). The impact of co-morbidities on HR-QoL in adults with TS was noted to be more complex, and in particular the negative contribution that anxiety and depression can make to HR-QoL in adults with TS was highlighted (Cavanna et al., 2013a). The review also summarised methodological limitations in the literature, including the use of different HR-QoL measures – including generic QoL instruments, variability in diagnosing co-morbidities, referral bias and small samples sizes (Cavanna et al., 2013a). This research group has also developed and validated a HR-QoL measure specifically for TS cohorts, the Gilles de la Tourette Syndrome-Quality of Life Scale (GTS-QoL; Cavanna et al., 2008).
A recent study by Cavanna et al. (2013b) assessed the utility of the GTS-QoL in 75 children with TS, finding that individuals with co-morbid OCD and/or ADHD demonstrated lower HR-QoL on the instrument’s obsessional subscale than individuals with pure-TS. However, no other significant differences were found between these two groups (Cavanna et al., 2013b). In a second study using the same cohort, Cavanna et al. (2013c) compared HR-QoL reporting between children and their parents using the GTS-QoL for Children and Adolescents and the Child Tourette’s Syndrome Impairment Scale (CTIM-P), respectively. HR-QoL scores were compared across four groups constructed from the sample of 75 children, which included pure-TS, TS + OCD, TS + ADHD and TS + OCD + ADHD (Cavanna et al., 2013c). No significant differences between the four groups were noted using the GTS-QoL, but significant differences were found between the groups for the total school activity and social activity scores on the CTIM-P.
The current study used the GTS-QoL to investigate the impact of cumulative co-morbidities on the HR-QoL of people with TS. The study also aimed to assess the specific impact of co-morbid diagnoses including ADHD and OCD and to explore these questions with cognisance to the presence of complex tics including coprophenomena and tic severity. The methodology thus provides a wider assessment of factors potentially impinging on HR-QoL than is available in much of the extant literature and increases the research and clinical applicability of the findings. We understand this to be the first study of its type within the Australian context.
Materials and methods
The study had the approval of the Human Research Ethics Committees of the Sydney Local Health and Sydney South West Local Health Districts. Informed consent was provided by, or on behalf of, all participants.
Participants
Participants included 83 people with an established diagnosis of TS made by a medical professional (61 males; mean age = 26 years). The sample comprised 43 children (<18 years) ranging in age from 4 to 17 years (median age = 12 years) and 40 adults aged 19–69 years (median age = 41 years). Of the sample, 97% reported a Caucasian cultural background. Participants were contacted via the Tourette Syndrome Association of Australia (TSAA) past-member patient database and invited to participate in the research. A total of 767 surveys were initially sent out, with 115 of these returned as ‘no longer at this address’, reflecting a 13% response rate.
Measures
Participants were sent a survey package containing a number of measures including a short form of the National Hospital Interview Schedule for the assessment of tics and related behaviours (Robertson and Eapen, 1996). This measure provided an overview of demographic information as well as an assessment of TS symptoms, co-morbid symptoms and diagnoses, medication history and family history information. The psychometric properties of this instrument have been previously established with good inter-rater reliability and concurrent validity against the Yale Global Tic Severity Scale and Diagnostic and Statistical Manual of Mental Disorders (DSM) criteria (Robertson and Eapen, 1996).
Participants were also administered the GTS-QoL (Cavanna et al., 2008), with parents completing the measure on behalf of children aged 17 years or less. The GTS-QoL consists of 27 items across four subscales (psychological, physical, obsessional and cognitive), and a total score can be calculated. Items are scored on a 5-point scale with response options ranging from ‘no problem’ to ‘extreme problem’, and where higher scores denote a lower level of HR-QoL. A ‘satisfaction with life’ scale ranging between 0 ‘extremely dissatisfied with my life’ and 100 ‘extremely satisfied with my life’ is also included at the end of the GTS-QoL. An initial validation study of 136 patients with TS revealed acceptable psychometric properties – with the internal consistency, reliability and test–retest reliability of the instrument being high (Cronbach’s alpha ⩾ 0.8 and intraclass correlation coefficient ⩾ 0.8); and validity supported by interscale correlations (range 0.5–0.7), confirmatory factor analysis and acceptable correlations with other rating scales and clinical variables (Cavanna et al., 2008). The scale has been used widely in the assessment of HR-QoL since its development across a number of contexts and by different research teams, including follow-up from deep brain stimulation (Cannon et al., 2012).
Data analysis
Data were analysed using SPSS, version 22 (IBM Corp., 2013). One-way analyses of variance (ANOVAs) were used to assess the impact of (1) the number of previously established co-morbid diagnoses reported by participants and (2) the presence of ADHD and/or OCD and other combinations of co-morbidities on HR-QoL. One-way ANOVA was also performed to analyse the impact of endorsement of specific TS symptoms on GTS-QoL subscales, with post hoc Tukey’s HSD (honestly significant difference) comparisons used to evaluate group differences. Finally, a standard multiple regression analysis was utilised to explore the relative contribution of a range of variables on GTS-QoL total score. Alpha was set at 0.05 for all comparisons, following recommendations by Saville (1990) who argues for this per-comparison level rather than a family-wise approach when conducting research in novel areas. To help the reader evaluate the size of observed effects independently of statistical significance, Cohen’s d effect sizes were also reported. It is widely accepted that Cohen’s d values of 0.2–0.49 denote small-sized effects, 0.5–0.79 denote medium-sized effects and >0.8 denote large effect sizes. With respect to interpreting the effect size of correlation coefficients, values of 0.1, 0.3 and 0.5 are thought to denote small, medium and large effect sizes, respectively.
Results
Number of co-morbid diagnoses, HR-QoL and satisfaction with life scores
Participants reported a range of previously established co-morbid diagnoses. These are presented below in the format of percentage of cases in young people aged 17 years or less, percentage in adults and overall percentage: ADHD (26%, 15%, 21%), OCD (39%, 33%, 35%), specific learning disorders (24%, 25%, 24%), ASD (21%, 8%, 15%), other anxiety disorders (41%, 50%, 45%), depressive disorders (17%, 50%, 33%), oppositional defiant disorder/conduct disorder (CD; 2.3%, 7.5%, 4.8%), schizophrenia (2.3%, 7.5%, 4.8%) and posttraumatic stress disorder (PTSD; 0%, 2.5%, 1.2%).
Correlations between the satisfaction with life scores and the HR-QoL subscales indicated a significant negative correlation between satisfaction with life and all four HR-QoL subscales: psychological HR-QoL (r = −0.65, p < 0.001), physical HR-QoL (r = −0.44, p < 0.01), cognitive HR-QoL (r = −0.42, p < 0.01) and obsessional HR-QoL (r = −0.51, p < 0.01). Given the directionality of the satisfaction with life scores (where higher scores indicate higher satisfaction) and the HR-QoL subscales (where higher scores indicate lower HR-QoL), these correlations all suggest a positive relationship between the various aspects of HR-QoL and satisfaction with life.
Participants were categorised into three groups based on the number of co-morbid diagnoses reported. The first group consisted of individuals with no co-morbidities and a diagnosis of pure-TS (n = 23). The second group was made up of participants who endorsed one or two co-morbid disorders, ‘TS + 1/2 additional diagnoses’ (n = 38), with the final group consisting of individuals with three or more co-morbid conditions in addition to their TS, ‘TS + 3 + additional diagnoses’ (n = 22). No statistically significant differences were observed between the groups with respect to age of participants or gender distribution (ps < 0.05). Moreover, no statistically significant or clinically meaningful association was observed between age and any HR-QoL scores or satisfaction with life score (all ps > 0.05, all rs < 0.20), with groups therefore analysed as a whole.
Results indicated that the overall ANOVA was statistically significant with respect to the psychological F(2, 71) = 4.15, p = 0.02; physical F(2, 71) = 5.02, p = 0.009; and obsessional F(2, 71) = 10.89, p < 0.001 subscales of the GTS-QoL, as well as for the overall satisfaction with life score F(2, 69) = 3.77, p = 0.03, and this approached significance in the case of the cognitive subscale (p = 0.06). Note that were a Bonferroni correction applied (0.05/4 = 0.0125), the physical and obsessional results would have remained significant. Post hoc analyses revealed a significant difference between individuals in the TS + 3 + additional diagnoses group and both the pure-TS group and the TS + 1/2 additional diagnoses groups on the psychological and obsessional HR-QoL subscales (ps < 0.05). There was also a significant difference between the pure-TS and TS + 3 + additional diagnoses groups in cognitive HR-QoL scores and between the TS + 1/2 additional diagnoses and TS + 3 + additional diagnoses groups on physical HR-QoL scores and overall satisfaction with life (p < 0.05). The difference between the pure-TS and TS + 1/2 additional diagnoses groups was not statistically significant for any of the GTS-QoL subscales. Descriptive statistics and statistical information are provided in Table 1 and depicted in Figure 1.
Descriptive statistics of quality of life subscales by number of diagnoses.
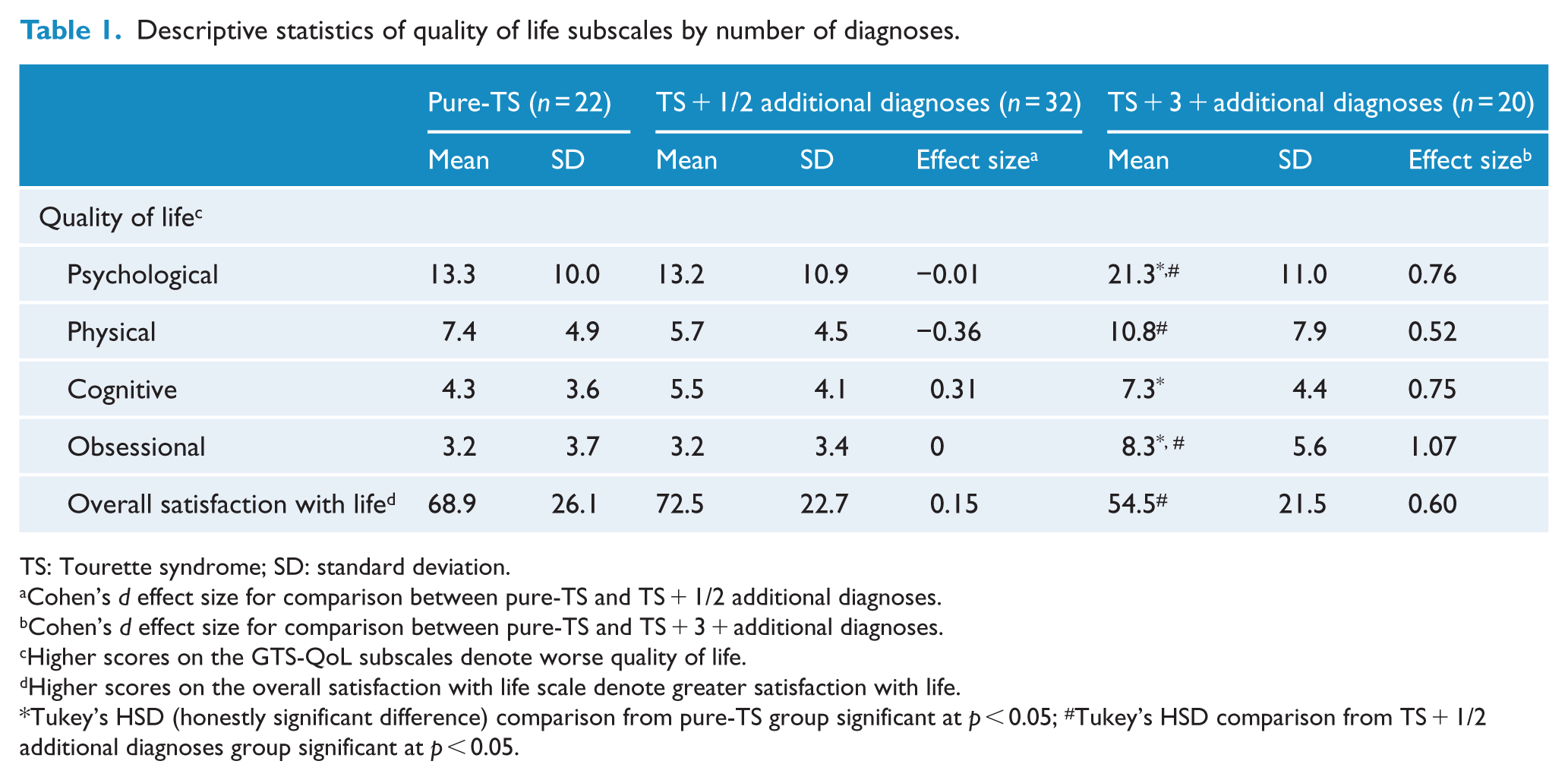
TS: Tourette syndrome; SD: standard deviation.
Cohen’s d effect size for comparison between pure-TS and TS + 1/2 additional diagnoses.
Cohen’s d effect size for comparison between pure-TS and TS + 3 + additional diagnoses.
Higher scores on the GTS-QoL subscales denote worse quality of life.
Higher scores on the overall satisfaction with life scale denote greater satisfaction with life.
Tukey’s HSD (honestly significant difference) comparison from pure-TS group significant at p < 0.05; #Tukey’s HSD comparison from TS + 1/2 additional diagnoses group significant at p < 0.05.
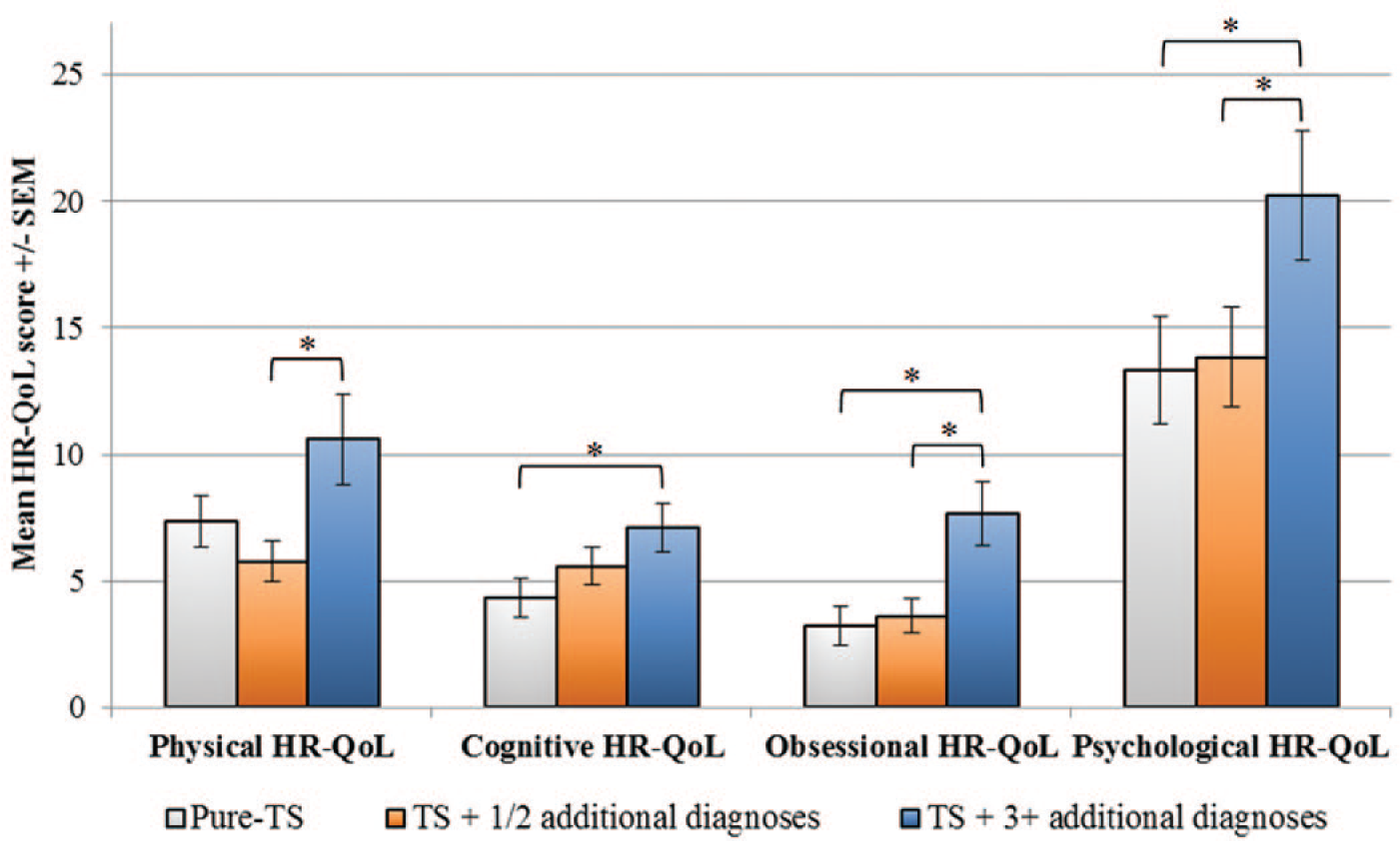
GTS-QoL subscale scores by number of co-morbidities.
Type of co-morbid diagnoses, HR-QOL and satisfaction with life scores
Participants were next categorised into groups according to the type of co-morbid diagnoses present (pure-TS n = 23, TS + ADHD n = 10, TS + OCD n = 21, TS + ADHD + OCD n = 7, TS + other disorders [not including ADHD or OCD] n = 22). The HR-QoL scores for the five groups were analysed for each of the HR-QoL subscales with post hoc Tukey’s HSD tests performed to explore pairwise comparisons (see Table 2 for descriptive statistics). Two of the four overall ANOVA results for the HR-QoL subgroups reached statistical significance (cognitive HR-QOL: F(4, 69) = 4.84, p = 0.002, and obsessional HR-QOL: F(4, 69) = 5.32, p = 0.001). As above, these would also have been significant at a Bonferroni-adjusted 0.0125 level. The overall satisfaction with life score was also non-significant (p > 0.05).
Descriptive statistics of quality of life and satisfaction scores by type of co-morbid diagnosis.
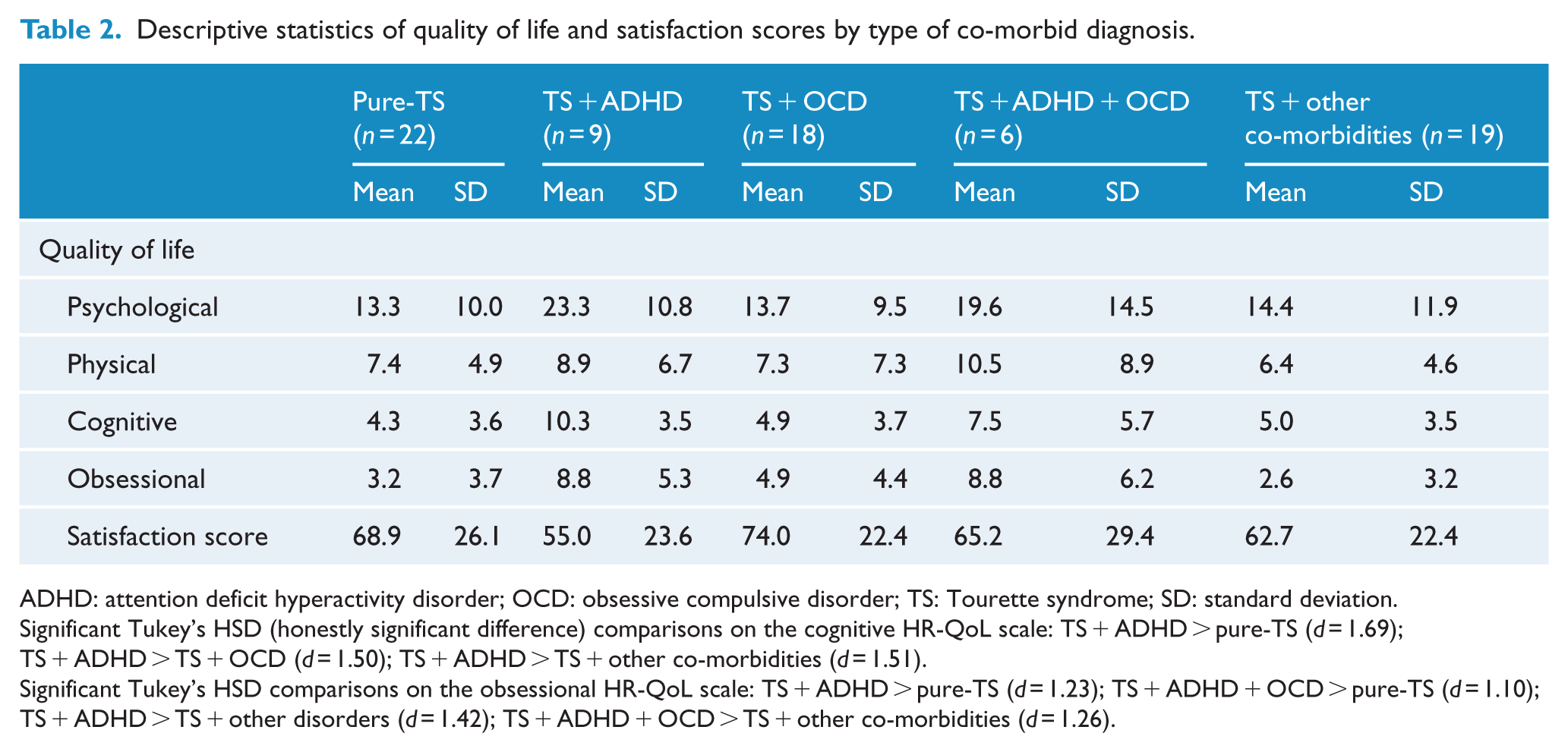
ADHD: attention deficit hyperactivity disorder; OCD: obsessive compulsive disorder; TS: Tourette syndrome; SD: standard deviation.
Significant Tukey’s HSD (honestly significant difference) comparisons on the cognitive HR-QoL scale: TS + ADHD > pure-TS (d = 1.69); TS + ADHD > TS + OCD (d = 1.50); TS + ADHD > TS + other co-morbidities (d = 1.51).
Significant Tukey’s HSD comparisons on the obsessional HR-QoL scale: TS + ADHD > pure-TS (d = 1.23); TS + ADHD + OCD > pure-TS (d = 1.10); TS + ADHD > TS + other disorders (d = 1.42); TS + ADHD + OCD > TS + other co-morbidities (d = 1.26).
With respect to the cognitive HR-QoL scale, Tukey’s post hoc comparisons revealed a significant difference between pure-TS and TS + ADHD (p < 0.01), TS + ADHD and TS + OCD (p < 0.01), and TS + ADHD and TS + other disorders (p < 0.05). In all cases, the TS + ADHD group had scores denoting lower HR-QoL. Within the obsessional HR-QoL subscale, there was a significant difference between pure-TS and TS + ADHD, pure-TS and TS + ADHD + OCD, TS + ADHD and TS + other disorders, and TS + ADHD + OCD and TS + other disorders (ps < 0.05). In all cases, the group containing participants with ADHD had HR-QoL scores denoting lower HR-QoL (see Table 2 and Figure 2). Inspection of Figure 2 also suggests that a similar pattern, whereby the subgroups with participants who had ADHD were showing poorer HR-QoL scores, was also in evidence for the psychological and physical HR-QoL subscales.
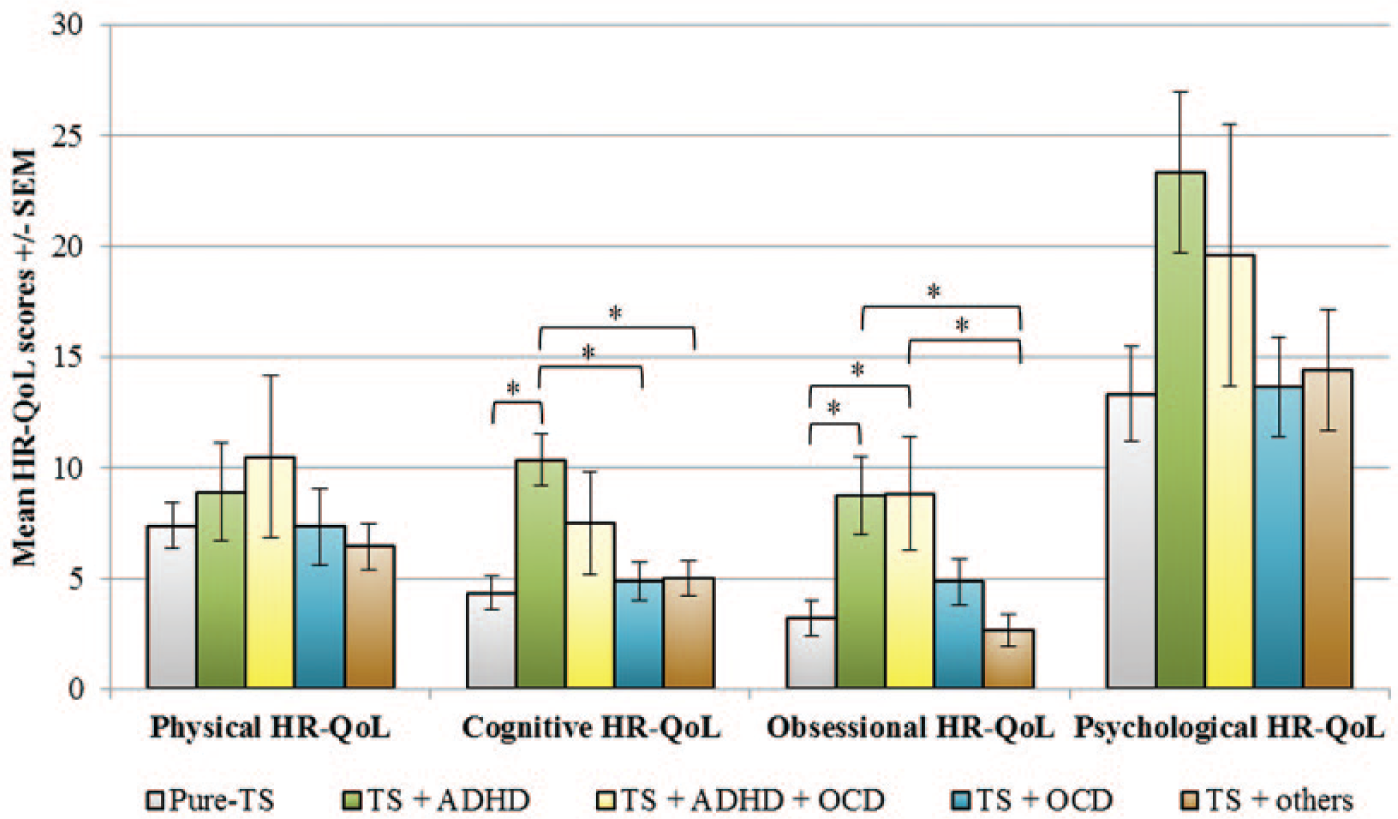
GTS-QoL subscale scores by pattern of co-morbidities.
TS symptoms, presentation severity and HR-QOL
To further explore the impact of TS symptomatology on HR-QoL, a series of one-way ANOVAs were conducted comparing the presence of a range of complex tic phenomena on HR-QoL. The specific complex tics investigated were echolalia (repeating words, phrases or sounds of others), echopraxia (imitating gestures or movements of others), palilalia (repeating one’s own words, phrases or sounds), coprolalia (uttering obscenities), copropraxia (making rude gestures) and self-injurious behaviour (see Table 3). A significant difference was found for all four HR-QoL subscales with the presence of coprolalia and copropraxia (ps < 0.05). Echolalia and echopraxia showed a significant difference in all HR-QoL subscales except for cognitive HR-QoL and physical HR-QoL, respectively (p < 0.05). For palilalia, a statistically significant result was only found for the obsessional HR-QoL subscale (p < 0.01). No significant differences were obtained for self-injurious behaviour.
GTS-QoL subscale scores for specific TS symptoms.
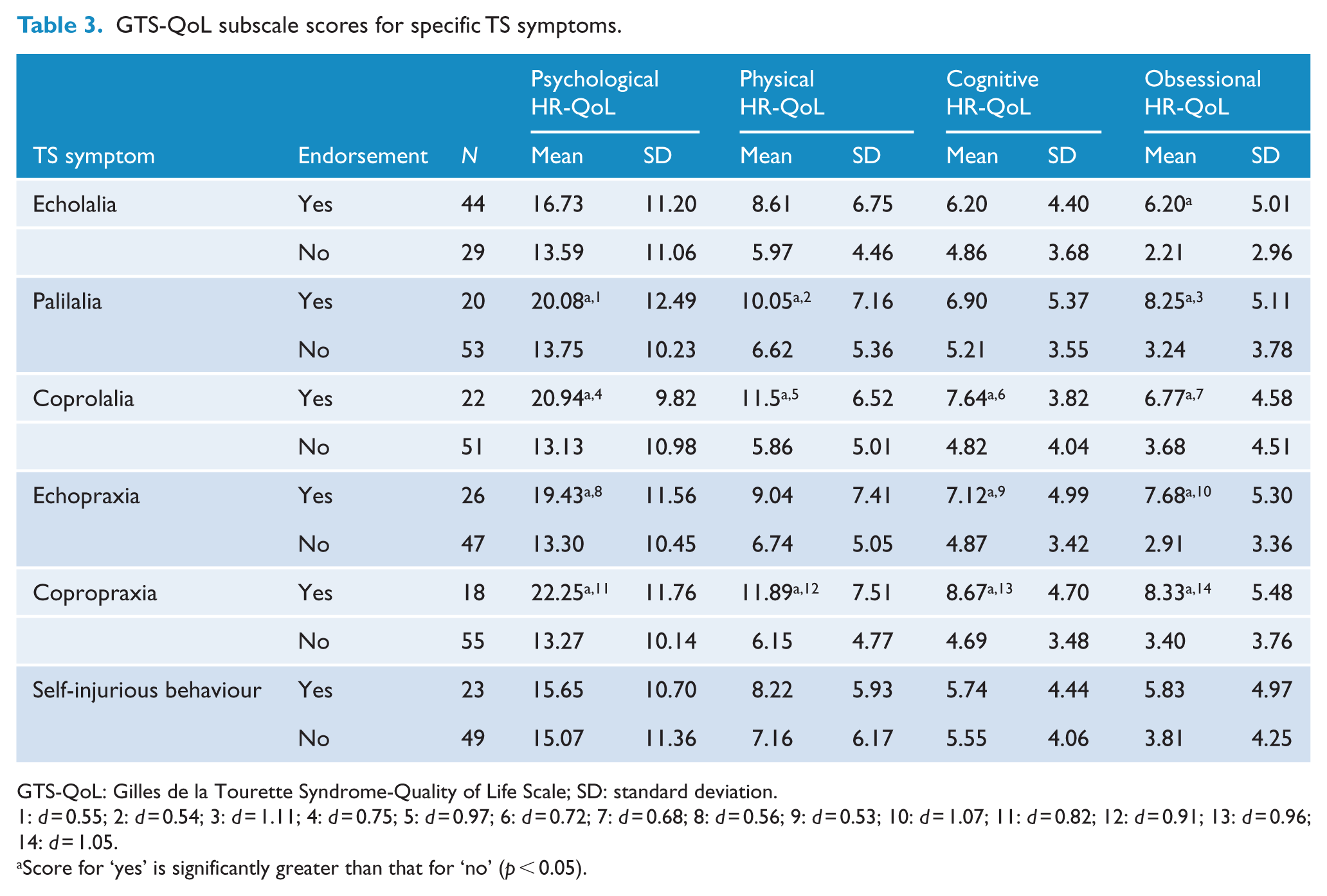
GTS-QoL: Gilles de la Tourette Syndrome-Quality of Life Scale; SD: standard deviation.
1: d = 0.55; 2: d = 0.54; 3: d = 1.11; 4: d = 0.75; 5: d = 0.97; 6: d = 0.72; 7: d = 0.68; 8: d = 0.56; 9: d = 0.53; 10: d = 1.07; 11: d = 0.82; 12: d = 0.91; 13: d = 0.96; 14: d = 1.05.
Score for ‘yes’ is significantly greater than that for ‘no’ (p < 0.05).
While a direct measure of TS symptom severity was unavailable for analysis, it was possible for the authors to construct a simple metric of TS symptom severity based upon the addition of several of the symptom variables noted above (coprolalia, copropraxia, echolalia, echopraxia, palilalia and self-injurious behaviour). To this was added the age of onset, with <5 years taken to denote greater severity. In this regard, a TS severity score ranging from 0 to 7 was derived.
One-way ANOVA with co-morbidity status as the grouping variable revealed an overall significant finding, F (2, 76) = 4.37, p = 0.016, with the pure-TS group having a mean TS severity score of 2.09 (standard deviation [SD] = 1.60), the TS + 1/2 co-morbidity groups a mean score of 2.08 (SD = 1.71) and the TS + 3 + co-morbidity groups a mean score of 3.43 (SD = 2.06). Post hoc Tukey’s HSD analyses suggested that the TS + 3 + co-morbidity group were scoring significantly higher than the pure-TS and TS + 1/2 co-morbidity groups on TS severity (ps < 0.05).
Pearson’s r correlations between the TS severity score and GTS-QoL subscales were significant for psychological HR-QoL (r = 0.37, p = 0.001), physical HR-QoL (r = 0.42, p < 0.001), cognitive HR-QoL (r = 0.38, p = 0.001) and obsessional HR-QoL (r = 0.60, p < 0.001) subscales – indicating that on these subscales higher TS severity scores were associated with lower levels of HR-QoL. No significant relationship was evident for overall satisfaction with life (r = −0.17, p = 0.16).
Regression analysis
Given there appeared to be independent and notable effects upon HR-QoL of the number of co-morbidities, the presence of ADHD, the presence of coprophenomena and tic severity as defined above, the authors resolved to conduct a final analysis pooling these factors into a standard multiple regression analysis. For ease of interpretation, GTS-QoL total score was used as the dependent variable, which was calculated by adding the four subscale scores, as suggested by the scale authors (Cavanna et al., 2008). Subscale to total score correlations on the GTS-QoL were high, ranging from 0.74 for cognitive HR-QoL to 0.93 for psychological HR-QoL. Results of evaluation of assumptions were satisfactory with no outliers noted.
Table 4 shows descriptive statistics and variable intercorrelations, unstandardised regression coefficients (B), standardised regression coefficients (β) and p values. With all four predictors in the equation, R = 0.58, R2 = 0.34, adjusted R2 = 0.30, F(4, 64) = 8.23, p < 0.001. Two of the independent variables contributed significantly to prediction of GTS-QoL total score, presence of coprophenomena (sr2 = 0.06) and number of co-morbidities (sr2 = 0.04). The four independent variables in combination contributed another 0.20 in shared variability. Altogether, 30% (adjusted) of the variability in GTS-QoL total score was predicted by knowing scores on these four independent variables. While the presence of ADHD and tic severity were significantly correlated with GTS-QoL total score (0.35 and 0.46, respectively), these variables did not contribute significantly to regression.
Standard multiple regression of co-morbidity and Tourette syndrome–related variables on GTS-QoL total score.
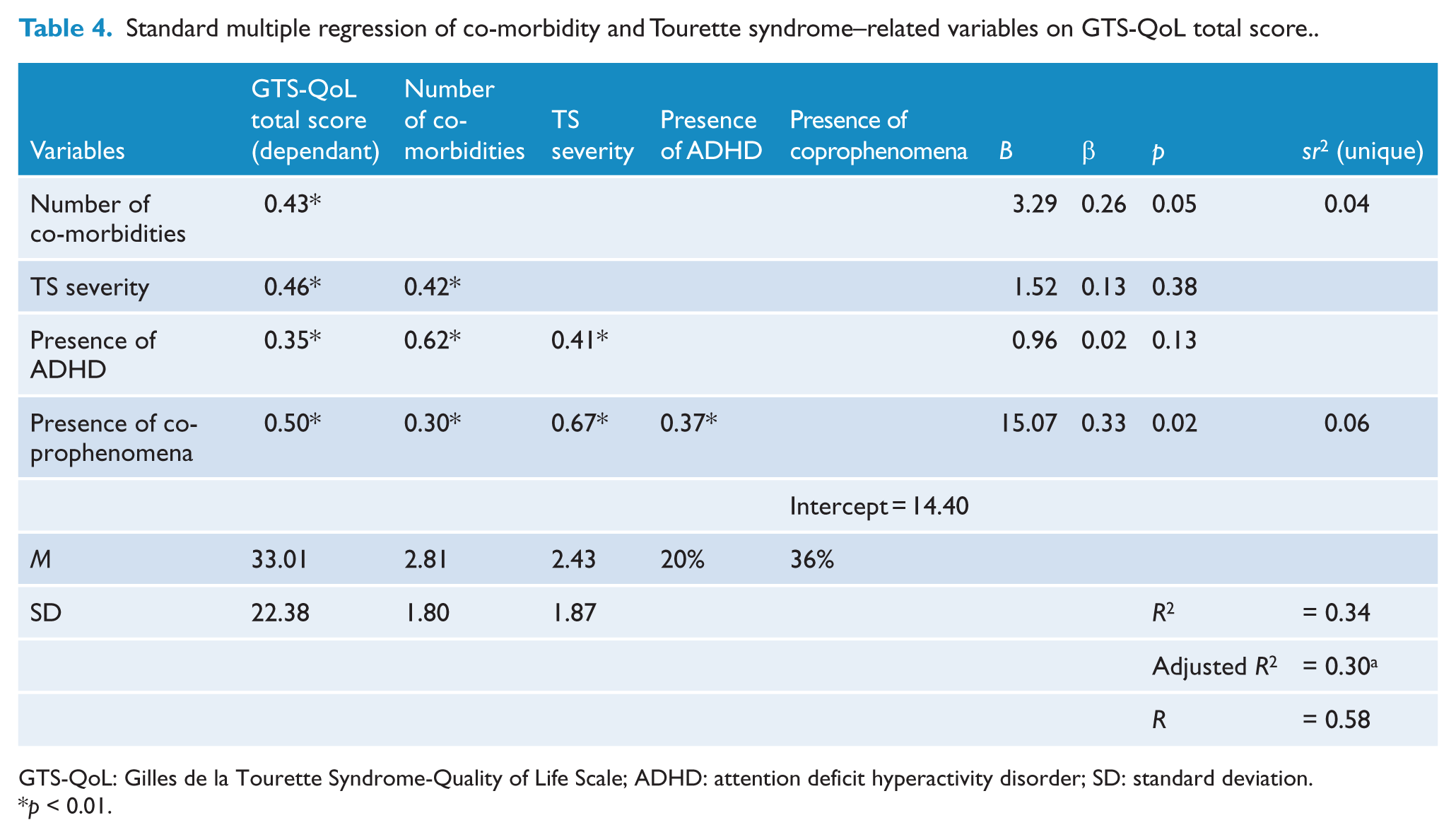
GTS-QoL: Gilles de la Tourette Syndrome-Quality of Life Scale; ADHD: attention deficit hyperactivity disorder; SD: standard deviation.
p < 0.01.
Discussion
This study assessed the relationship between HR-QoL and psychiatric co-morbidity in individuals with TS. Individuals with TS + 3 or more additional diagnoses had the highest HR-QoL scores (denoting lower levels of HR-QoL) across psychological, physical, cognitive and obsessional subscales of the GTS-QoL. This group also scored significantly higher than both the pure-TS group and the TS + 1/2 additional diagnoses groups on psychological and obsessional HR-QoL subscales, higher than the pure-TS group on the cognitive subscale and higher than the TS + 1/2 additional diagnoses group on physical HR-QoL, with medium-to-large effect sizes observed. This suggests that having three or more additional disorders has a significant impact on HR-QoL in TS. It is conceivable, however, that the impact on the different subscales may be a function of the type of the associated co-morbidity rather than the number of co-morbidities.
A second set of analyses in the current study assessed the impact of particular disorder combinations on HR-QoL. These analyses revealed a number of differences between individuals with pure-TS, TS + ADHD, TS + OCD and TS + ADHD + OCD. For example, the TS + ADHD group scored significantly higher on the cognitive HR-QoL subscale than those with pure-TS and those in the TS + OCD and TS + other disorder groups. The TS + ADHD and the TS + ADHD + OCD groups also achieved the highest scores on the obsessional subscale of the GTS-QoL measure, which were significantly higher than all other groups. In all instances, effect sizes were large. This is consistent with previous research indicating that ADHD and OCD significantly affect the behavioural and psychosocial functioning of people with TS (Eapen et al., 2013) which in turn can negatively impact different aspects of HR-QoL (Bernard et al., 2009). However, the results of the current study also indicate that ADHD may have the most significant additive effect in determining HR-QoL in TS, given that it was the addition of this disorder that was associated with higher scores on both the cognitive and obsessional HR-QoL subscales. This is supportive of previous research outlining an association between TS, ADHD and inattention and learning difficulties, and delinquent behaviours and functional impairment (Sukhodolsky et al., 2003).
However, this aspect of the findings is inconsistent with a recent study by Cavanna et al. (2013c) that found no differences in child-reported GTS-QoL scores between groups categorised according to co-morbid diagnoses (pure-TS, TS + ADHD, TS + ADHD + OCD, TS + OCD). While there were a similar proportion of participants with co-morbid ADHD in both studies, it is possible that a difference in the severity of symptoms experienced by participants, a variable not measured in either study, could have accounted for the discrepant findings. This is reminiscent of a study by Pringsheim et al. (2009), which demonstrated that ADHD severity was a predictor of psychosocial QoL in children with TS (as measured by a generic instrument, the Child Health Questionnaire, Parent Form 50). Other potentially relevant methodological differences between the Cavanna and present studies include the respondent (in this study, parents gave a HR-QoL rating on behalf of children) as well as the age range of participants.
An unexpected finding in this study was that ADHD rather than OCD had a significant impact on the GTS-QoL obsessional subscale, contrary to previous research and the intuitive argument that OCD would be associated with obsessionality (Eddy et al., 2011). This may be due to the variability in the severity of these co-morbid conditions or other unique variables in the different cohorts, as well as many studies having only a small number of participants in the different subgroups. Future research incorporating a larger sample and control participants is needed to fully understand these relationships, and it is suggested that replication studies are required with similar methods and with the TS participants subdivided into various diagnostic groups.
There were significant medium-to-large-sized correlations between satisfaction with life scores and the four HR-QoL subscales in the total sample. This indicates that, as one might anticipate, overall satisfaction with life is associated with all HR-QoL subscales. Furthermore, given the potentially stigmatising nature of coprophenomena, the finding that individuals who reported experiencing coprolalia and copropraxia displayed significantly higher scores on all HR-QoL subscales of medium-to-large effect size, indicating lower QoL, can be intuitively understood.
There was some evidence obtained in this study to suggest that participants in the TS + 3 + co-morbidity group may have had a higher level of TS severity, as determined through the TS severity score used in the study, compared with those who had pure-TS or TS + 1/2 co-morbidities. We note that our TS severity score was in many respects an index of the presence of complex tics. Medium-to-large-sized positive correlations were observed between the TS severity score and subscale scores on the GTS-QoL. Research on the relationship between tic severity, co-morbidities and QoL has been inconsistent within the literature (Cavanna et al., 2013c; Eddy et al., 2011; Hoekstra et al., 2004), which may be a reflection of the way people with TS are categorised. For example, there is a possibility that complex tics may beget other co-morbidities and that there is a relationship between complex tics and the presence of specific TS phenomenology and associated co-morbidities. In this regard, a recent study by Eapen and Robertson (2015) found that only 13.5% of people with TS had pure-TS while the remainder had associated co-morbidities and psychopathologies (TS-plus), and that 39% of the TS-plus group displayed coprolalia, compared to none (0%) of the pure-TS. Other relevant factors including the proportion with specific co-morbidities (e.g. proportion with ADHD vs proportion with OCD in each cohort) and the number of males versus females (especially in terms of the proportion in each cohort with OCD symptoms) could all contribute to the discrepancy in findings on the relationship between co-morbidities and HR-QoL (Eapen and Robertson, 2015). Research also suggests that people with TS who have complex tics may be more aware of their tics and the urge to tic, and hence are perhaps more affected in terms of HR-QoL (Crossley and Cavanna, 2013; Eapen and Robertson, 2015). Thus, it is plausible that HR-QoL may be related to complex tics and coprophenomena – which are affecting HR-QoL more so than, or in conjunction with, the differential impact of a particular co-morbidity. This study offers some nascent evidence in this regard. Bearing in mind the small numbers, the percentage of participants in this study reporting three or more complex tics was as follows – pure-TS, 14%; TS + ADHD, 50%; TS + OCD, 25%; TS + other disorders, 14%.
Furthermore, when number of co-morbidities, the presence of ADHD, the presence of coprophenomena and tic severity were regressed against GTS-QoL total score, only the number of co-morbidities and the presence of coprophenomena were significant in the regression model – despite all variables being initially correlated with GTS-QoL. The relationship between ADHD, tic severity and QoL may therefore be mediated by the relationship between number of co-morbidities, coprophenomena and QoL – and future studies will be tasked with further delineating the unique and combined influence of these variables and building upon these novel findings.
Data obtained in this study cannot speak to the pathogenetic link between TS and the commonly observed co-morbidities in TS, namely, ADHD and OCD, as pathogenesis and impact upon HR-QoL are not necessarily related constructs. In any event, it is interesting to observe that much contemporary research points to the genetic and phenotypic linkage between OCD and TS (Roessner et al., 2005), and yet the current results suggest OCD may impact less upon HR-QoL as compared to ADHD in the context of TS. This could at least be partly explained on the basis of the relationship between OCD and ADHD on the one hand and the presence of other co-morbidities in the context of TS. For example, Hirschtritt et al. (2015) showed that the genetic correlations between TS and mood (RhoG, 0.47), anxiety (RhoG, 0.35) and disruptive behaviour disorders (RhoG, 0.48) may be accounted for by ADHD. This study also noted such a relationship for mood disorders, by OCD. Thus, some co-morbidities may be more biologically related to ADHD or OCD and not specifically to TS, and in such a scenario the influence of these co-morbidities on HR-QoL may vary based on the proportion of participants in each cohort with TS and associated primary ADHD and OCD, which may be pathogenetically different to pure-TS cases.
We would also highlight to the reader in this context that TS is often associated with obsessive compulsive behaviours (OCB), such as ‘evening up’, doing things just right, and arranging and ordering (Robertson, 2012), and that such behaviours are perhaps not as distressing or cause as much dysfunction as primary OCD: Hence, the impact on HR-QoL may vary depending on those with TS-related OCB versus primary OCD and the method and criteria used to classify participants as having a co-morbidity. Moreover, parental history of ADHD has been found to be associated with a higher burden of non-OCD, non-ADHD co-morbid psychiatric disorders (odds ratio [OR] = 1.86; 95% confidence interval [CI] = [1.32, 2.61]), again suggesting that the genetic loading and the pathogenesis of the different phenotypic presentations seen in people with TS may vary from one individual to another, and this in turn may have an impact on the co-morbidities (Hirschtritt et al., 2015). A recent study by Robertson et al. (2015) found that conduct disorder (CD) in people with TS was not an integral part of the TS pathogenesis but rather that CD in the context of TS is related to the presence of ADHD, as well as a family history of aggressive and violent behaviour and forensic encounters.
Available research data on TS and related disorders such as ADHD and OCD suggest the role of specific, yet overlapping neuronal circuitry resulting in varied TS phenomenology ranging from simple to complex clinical presentations and associated co-morbidities. Thus, those with predominantly basal ganglia circuitry involvement may present with pure-TS characterised by motor and vocal tics only, while those with frontostriatal circuitry involvement may have more ADHD and disruptive behaviours, while those with limbic-basal ganglia circuitry involvement may show anxiety or OCD symptoms. These interconnected neural systems can be linked to functionally relevant anatomic areas and pathways that influence specific cognitive or behavioural domains, the programming of which are genetically modulated during development and mediated through a range of molecular pathways and interacting neurotransmitter systems with more severe and extensive neuronal circuitry involvement resulting in more co-morbidities (Eapen, 2012). The penetrance of the different co-morbidities may also be related to the specific genetic abnormality and the timing and dose effects of the dysregulation of the genes/ligands as well as gender and a number of perinatal events (‘second hits’) that can render varying pathogenetic consequences (Robertson and Eapen, 2013) and associated health burden and HR-QoL effects. Our finding that the presence of complex tics including coprophenomena and three or more co-morbidities have a significant impact on HR-QoL may be linked to the varied genetic loading and more extensive neurocircuitry involvement, resulting in more severe and complex clinical presentations and associated impact on functioning.
Limitations
The study comprised several methodological limitations which readers are encouraged to remain cognisant of in interpreting the study results. The use of self-reporting in gathering data may have resulted in bias in recording co-morbid diagnoses, either through over- or under-reporting. For example, it is conceivable in the current dataset that obsessional symptoms were sometimes reported as OCD, and the rates of schizophrenia obtained were also unusually high. Nonetheless, participants were asked specifically for established diagnoses in order to minimise errors in this regard, as is common practice in medical research. The use of categorical (yes/no) data for co-morbid diagnoses also meant that variations in co-morbid symptom severity could not be controlled for. Consequently, this may have skewed the perceived impact of particular co-morbid categories on HR-QoL and the comparative differences between subgroups. The use of symptom scales that assess ADHD and OCD symptoms could be used to quantify the severity of symptoms in future research, as could the use of a specific measure of TS severity. An ideal scenario would involve use of a structured clinical interview where the complex matter of multiple co-morbidities and subclinical symptoms could be carefully distinguished and recorded. The issue of potential differences between parent and self-report of HR-QoL in the context of TS has also been explored recently in the literature (Cavanna et al., 2013c; Gutierrez-Colina et al., 2015), and the use of youth self-report would have strengthened this study and enabled comment upon this aspect. The relatively low response rate observed in the study (13%) may have arisen in part due to the fact that surveys were sent to past-members of the TSAA, who may have had reduced interest in participating in research related to their TS; however, the mail-out methodology itself may also have affected the response rate and led to a degree of selection bias. The recruitment format may also have contributed to aspects of the somewhat unexpected pattern of co-morbidities in the study sample (i.e. relatively low percentage of participants with ADHD and relatively high percentage with pure-TS), although this pattern has also been observed in comparable studies (e.g. Cavanna et al., 2013b) – suggesting that nonresponse bias (Johnson and Wislar, 2012) may not have been a major factor in this sample. Finally, future studies might ideally incorporate stratification of participant age ranges, although no association was noted in the current sample with respect to age and QoL scores.
Conclusion
The current findings have the potential to further our understanding of the optimal management of people with TS in clinical practice, including to highlight the importance of incorporating HR-QoL measures in comprehensive symptom-targeting and to raise the awareness of clinicians that specific factors including multiple co-morbidity, ADHD and coprophenomena – factors in some respects considered not to be part of the core TS features and diagnosis – exert a significant influence on the HR-QoL and well-being of patients.
It is conceivable that the influence of co-morbidities is over and above that of tic severity in impacting HR-QoL, and early identification and assertive management of co-morbidities is indicated where these are causing distress and impairment. In addition to this, the presence of coprophenomena exerts an independent negative influence upon HR-QoL. This is understandable given the nature of these symptoms, but it is also likely that the presence of coprophenomena can, in some people, contribute to the long-term development of negative attributions by the person and those associated with them with respect to not only the tic disorder but also potentially themselves as individuals (e.g. being ‘different’ or ‘bad’): Attributions such as these can in turn have a cumulative effect, affecting multiple spheres of life, general QoL and indeed the manifestation of other psychiatric conditions. A history of coprophenomena is therefore important to assess not only with respect to clinical history but also for the possible sequelae of this for the individual.
In time, diagnostic classificatory systems may also need to take into account the varying clinical presentations that co-occur with tics under a ‘Tic Spectrum disorder’ including tics only, tics with OCB/OCD, tics with ADHD, tics with ASD and so on (Eapen and Črnčec, 2014), as these tend to have a distinct course, treatment response and outcomes. For example, in cases with tics and ADHD, the first-line pharmacological agent of choice may be clonidine; in the case of tics and OCB/OCD, augmentation with a dopamine-blocking agent may be needed in addition to selective serotonin reuptake inhibitor treatment, while in presentations where tics co-occur with ASD symptoms and behavioural problems, risperidone may be a preferred first-line agent.
With respect to further treatment implications, it is worth noting that at this juncture all available TS treatments are symptomatic and not disease modifying. It is also to be noted that, in addition to psychopharmacological approaches, there is growing evidence base for behavioural treatments built around principles of habit reversal such as Comprehensive Behavioural Intervention for Tics (Piacentini et al., 2010); however, outcomes may be constrained in individuals with co-morbid cognitive or learning difficulties or ASD symptoms.
The simple awareness of tic disorders when treating people with ADHD or OCD will also allow for mild co-morbid tics to be identified when these are present rather than be missed as frequently happens. This in turn can lead to appropriate management of the co-morbidities and assist in the anticipation and differentiation of possible associated features. For example, tics may be mistaken for fidgetiness in the context of ADHD, and coprolalia may be perceived as ‘naughty’ or ‘oppositional’ behaviour and may attract negative consequences. When such co-morbidities are identified early leading to appropriate management and understanding, this can have a significant positive impact on the HR-QoL of the individual and the overall course and outcome.
Footnotes
Acknowledgements
The authors would like to thank both the Tourette Syndrome Association Australia for their assistance and support in the conduct of this research and the study participants for generously providing their time. The study was completed as part of the Independent Learning Project of author Corina Snedden, with some assistance by Sarah McPherson and Laurie Nichols, within the medical degree curriculum through the School of Medicine, University of New South Wales.
Declaration of interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.