
Abstract
Objectives:
There are ongoing uncertainties in the relationship between obsessive–compulsive disorder (OCD) and obsessive–compulsive personality disorder (OCPD). This study aimed to test the proposition that OCPD may be a marker of severity of OCD by comparing groups of OCD individuals with and without OCPD on a number of variables.
Method:
A total of 148 adults with a principal diagnosis of OCD were administered the Mini International Neuropsychiatric Interview, Yale–Brown Obsessive–Compulsive Scale, Sheehan Disability Scale, Vancouver Obsessional Compulsive Inventory and Symptom Checklist 90-Revised. Participants with a DSM-IV diagnosis of OCPD were compared with those without OCPD.
Results:
Some 70 (47.3%) participants were diagnosed with OCPD. The groups of participants with and without OCPD did not differ significantly with respect to any of the demographic variables, clinician-rated severity of OCD, levels of disability and mean age of onset of OCD. All self-rated OCD symptom dimensions except for contamination and checking were significantly more prominent in participants with OCPD, as were all self-rated dimensions of psychopathology. Participants with OCPD had significantly more frequent hoarding compulsions and obsessions involving a need to collect and keep objects. Of Axis I disorders, only panic disorder was significantly more frequent in participants with OCPD than in those without OCPD.
Conclusions:
A high frequency of OCPD among individuals with OCD suggests a strong, although not necessarily a unique, relationship between the two conditions. This finding may also be a consequence of the blurring of the boundary between OCD and OCPD by postulating that hoarding and hoarding-like behaviours characterise both disorders. Results of this study do not support the notion that OCD with OCPD is a marker of clinician-rated severity of OCD. However, individuals with OCPD had more prominent OCD symptoms, they were more distressed and exhibited various other psychopathological phenomena more intensely, which is likely to complicate their treatment.
Introduction
The relationship between obsessive–compulsive disorder (OCD) and obsessive–compulsive personality disorder (OCPD) has been a subject of interest and controversy for more than a hundred years. Although it may seem that a large part of the problem is about possible terminological confusion, not long ago OCPD was regarded as a precursor to or a characterological counterpart of OCD. Certainly, there are links and some overlap between OCD and OCPD, but how closely they are related remains uncertain. It has been suggested that the key difference between them is that the features of OCD are largely ego-dystonic, whereas those of OCPD are mostly ego-syntonic. This distinction does not always seem to be so clear-cut, but its implications are important conceptually and with regards to treatment. For example, ego-syntonic features are often regarded as more treatment resistant because the person does not experience them as ‘alien’ and may be less motivated to change them.
One way of gaining more insight into the relationship between OCD and OCPD has been to systematically compare OCD individuals with and without OCPD. These comparisons have yielded somewhat conflicting results. For example, most studies did not find a significant difference in OCD severity (based on the total Yale–Brown Obsessive–Compulsive Scale scores) between OCD individuals with and without OCPD (Albert et al., 2004; Coles et al., 2008; Diaferia et al., 1997; Garyfallos et al., 2010; Pinto et al., 2011). In contrast, one recent study reported that people with OCPD had a more severe OCD than those without OCPD (Lochner et al., 2011). Complicating matters further, some studies have reported a significantly greater severity of compulsions in individuals with OCPD, although they did not have a more severe overall OCD (Albert et al., 2004; Coles et al., 2008).
Some inconsistency was found in terms of the functional impairment and course of OCD, although different measures were used, making it difficult to directly compare the studies. Three studies reported significantly more disability or impaired functioning in people with OCPD than in those without OCPD (Coles et al., 2008; Garyfallos et al., 2010; Lochner et al., 2011); in two of these studies, however, there was apparently no correspondence between the level of impairment and severity of OCD, as individuals with OCPD showed significantly more impairment without having a significantly more severe OCD (Coles et al., 2008; Garyfallos et al., 2010). This suggests that impairment in individuals with OCPD might not have been related to OCD. One study found no difference in terms of the course of OCD between individuals with and without OCPD (Albert et al., 2004).
Data on the age of onset of OCD and the age of onset of OCD symptoms also differed between studies. While some studies found no significant difference in the age of onset of OCD and/or the age of onset of OCD symptoms between individuals with and without OCPD (Albert et al., 2004; Diaferia et al., 1997; Lochner et al., 2011), two studies reported that individuals with OCPD had a significantly earlier age of onset of OCD and OCD symptoms than those without OCPD (Coles et al., 2008; Garyfallos et al., 2010). A study comparing early- and late-onset OCD found that OCPD was significantly more frequent in patients with an early-onset OCD (Maina et al., 2008).
Three studies (Coles et al., 2008; Garyfallos et al., 2010; Lochner et al., 2011) have compared OCD individuals with and without OCPD in terms of their obsessions and compulsions, and in doing so they all relied on the Y-BOCS Symptom Checklist categories. While the findings were consistent across the studies in that almost all categories of compulsions were significantly more common in individuals with OCPD, one study reported only symmetry and hoarding/saving obsessions to be significantly more frequent in individuals with OCPD (Coles et al., 2008) and the other two found that in addition to symmetry and hoarding/saving obsessions, individuals with OCPD had significantly more frequent doubting obsessions (Garyfallos et al., 2010) and contamination and religious obsessions (Lochner et al., 2011).
Results of the studies examining the patterns of co-occurrence with other Axis I mental disorders in OCD individuals with and without OCPD were also discordant. One study reported that any mood disorder was significantly more frequent among people with OCPD (Coles et al., 2008), unlike the results of two other studies (Garyfallos et al., 2010; Lochner et al., 2011). Likewise, any anxiety disorder was significantly more frequent among people with OCPD in one study (Coles et al., 2008), contrary to the findings by Garyfallos et al. (2010). Lochner et al. (2011) found that of all the anxiety disorders, only posttraumatic stress disorder was significantly more common among people with OCPD, with a co-occurring generalised anxiety disorder actually being significantly more frequent among people without OCPD. There was no agreement between the three studies (Coles et al., 2008; Garyfallos et al., 2010; Lochner et al., 2011) in terms of the frequency of co-occurring tics or tic disorders, eating disorders and hypochondriasis or somatoform disorders in OCD individuals with and without OCPD. One of the studies reported a significantly higher frequency of intermittent explosive disorder and trichotillomania in OCD individuals with OCPD (Lochner et al., 2011).
These dissonant research findings are largely a consequence of the use of different assessment tools and issues pertaining to sample size and recruitment. Several interpretations of the relationship between OCD and OCPD have been made. First, some authors have suggested that OCD occurring together with OCPD may represent a subtype of OCD (Coles et al., 2008; Garyfallos et al., 2010). The second view has been that the presence of OCPD may be a marker of severity of OCD (Lochner et al., 2011). Finally, it has been proposed that no specific relationship exists between OCD and OCPD (Albert et al., 2004; Black and Noyes, 1997; Wu et al., 2006). Thus, the uncertainty about the nature of the relationship between OCD and OCPD continues.
In view of these findings, the main aim of the present study was to compare large groups of OCD individuals with and without OCPD in terms of the aforementioned variables: severity of OCD, levels of disability, age of onset of OCD, intensity of OCD symptoms and types and frequencies of co-occurring Axis I conditions. Our specific goal was to test the proposition that OCPD may be a marker of severity of OCD. In addition to the categorical and interviewer-based instruments used in previous studies, we also compared individuals with and without OCPD using dimensional and self-report measures of OCD symptoms, general distress and psychopathology, as this might shed more light on the relationship between OCD and OCPD. There are potential treatment implications of the results of this study in that one would expect OCD with OCPD to be associated with poorer prognosis and response to treatment of OCD if it is a more severe and disabling condition than OCD without OCPD.
We did not have specific hypotheses regarding these comparisons due to the conflicting results of the research conducted so far. However, our clinical experience suggests that at least a number of OCD individuals with OCPD are more difficult to treat because of the need to address both OCD symptoms and OCPD traits, and because these symptoms and traits are sometimes so entangled that it is very hard to ascertain whether or not they are ego-dystonic. We deduced from this observation that OCD individuals with OCPD might show indicators of more distress, psychopathology and disability than those without OCPD.
Methods
In total, 148 adults with a principal diagnosis of OCD participated in the Nepean OCD Study, which was described elsewhere (Starcevic et al., 2011). Participants were recruited from several sources: attendees of local anxiety disorders clinic and support groups, patients referred by general practitioners and mental health professionals and respondents to newspaper advertisements. The principal diagnosis of OCD meant that help was sought for it, or that OCD was deemed mostly responsible for distress or impairment in functioning. Persons with a co-occurring psychosis, bipolar disorder or other conditions considered to be more severe or disabling than their OCD were not eligible to participate. The Nepean OCD Study was approved by the local ethics committee, with all participants providing informed signed consent.
Assessments
The assessment encompassed administration of several instruments, as follows: the Mini International Neuropsychiatric Interview (MINI; Sheehan et al., 1999), Yale–Brown Obsessive–Compulsive Scale (Y-BOCS; Goodman et al., 1989), Sheehan Disability Scale (SDS; Sheehan, 1983), Vancouver Obsessional Compulsive Inventory (VOCI; Thordarson et al., 2004) and Symptom Checklist 90-Revised (SCL-90R; Derogatis, 1994).
The MINI is a semi-structured, clinician-administered interview that was used to ascertain that OCD was the principal diagnosis and establish the presence of co-occurring DSM-IV disorders and age of onset of all the diagnosed disorders. It was modified to include the DSM-IV diagnostic criteria for OCPD. The MINI has been validated against other diagnostic interviews, demonstrating solid psychometric properties (Lecrubier et al., 1997; Sheehan et al., 1997).
The Y-BOCS is the most widely used instrument for assessing OCD and it has very good psychometric properties (Deacon and Abramowitz, 2005; Woody et al., 1995). The Y-BOCS is also a semi-structured interview, but its primary purpose is to measure the severity of obsessions and compulsions. It consists of a checklist of obsessions and compulsions and a 10-item severity scale. Up to three most prominent obsessions and compulsions are rated on the severity scale. There are five criteria for rating severity: time spent, interference with functioning, distress, efforts to resist and perceived degree of control. Each criterion is rated on a 5-point Likert scale, with ratings summed to provide scores for the severity of obsessions, severity of compulsions and overall severity of OCD (total Y-BOCS score).
The SDS is a simple clinician-administered instrument that assesses levels of illness-related disability. It provides a total score and disability scores in three domains, represented by the corresponding subscales: Work, Social Life, and Family Life/Home Responsibilities.
The VOCI is a self-report measure of OCD symptoms. Unlike the Y-BOCS, it was not designed to measure the severity of OCD, but rather, it comprises an inventory of 55 OCD symptoms that are each rated on a 5-point Likert scale. Ratings are summed to yield scores on six subscales: Contamination, Checking, Obsessions, Hoarding, Just Right Experiences and Indecisiveness. The VOCI has been shown to have good to excellent psychometric properties (Thordarson et al., 2004).
The SCL-90R is a self-report 90-item measure of symptom distress and psychopathology. It provides a total score (Global Severity Index) and scores on nine subscales: Somatisation, Obsessive–Compulsive, Interpersonal Sensitivity, Depression, Anxiety, Hostility, Phobic Anxiety, Paranoid Ideation and Psychoticism. The SCL-90R has been demonstrated to be psychometrically sound (Peveler and Fairburn, 1990).
Procedure
Participants completed questionnaires (the VOCI and SCL-90R) and were interviewed by a psychiatrist or clinical psychologist trained in the use of the MINI and Y-BOCS. For the MINI-derived DSM-IV diagnoses of OCD and OCPD, inter-rater reliability based on 46 interviews, was excellent – with 97.8% and 95.7% agreement, respectively. The main rater and co-rater were present at the same interviews and made the MINI diagnoses independently from each other; co-raters recorded their agreement or disagreement with the main rater’s diagnoses, with disagreements at any stage of the diagnostic process being recorded as a disagreement for that diagnosis. Obsessions and compulsions recorded for each participant represent the most prominent obsessions and compulsions derived from the Y-BOCS.
Data analysis
Independent samples t-tests were conducted to determine whether there were significant differences in the mean current age, mean age of onset of OCD and mean scores on the severity of OCD, symptom dimensions of OCD, disability and dimensions of distress and psychopathology between participants with and without OCPD. Chi-square tests were calculated to determine whether there were significant differences in the frequencies of various demographic variables, obsessions and compulsions and co-occurring disorders between participants with and without OCPD. Where multiple statistical tests were performed, the familywise error rate was controlled using the False Discovery Rate method of Benjamini and Hochberg (1995).
Results
Of 148 participants, 92 (62.2%) were women. Their age ranged from 18–71 years, with the mean age of 45.42 (SD = 15.62). Some 59 (41.5%) participants were married or in a de facto relationship, whereas 48 (33.8%) were never married; 65 (46.1%) had post-high school qualifications. There were 54 (38.0%) participants who were employed full-time or part-time and 34 (23.9%) who were unable to work due to illness or disability.
In total, 70 (47.3%) participants were diagnosed with OCPD on the basis of the DSM-IV criteria. The groups of participants with and without OCPD did not differ significantly with respect to any of the demographic variables (Table 1). Although participants with OCPD had an earlier mean age of onset of OCD (mean = 17.21 years, SD = 11.16) than those without OCPD (mean = 19.85 years, SD = 11.25), this difference was not statistically significant (t = -1.430; df = 146; p = 0.155).
Demographic characteristics of OCD participants with and without OCPD
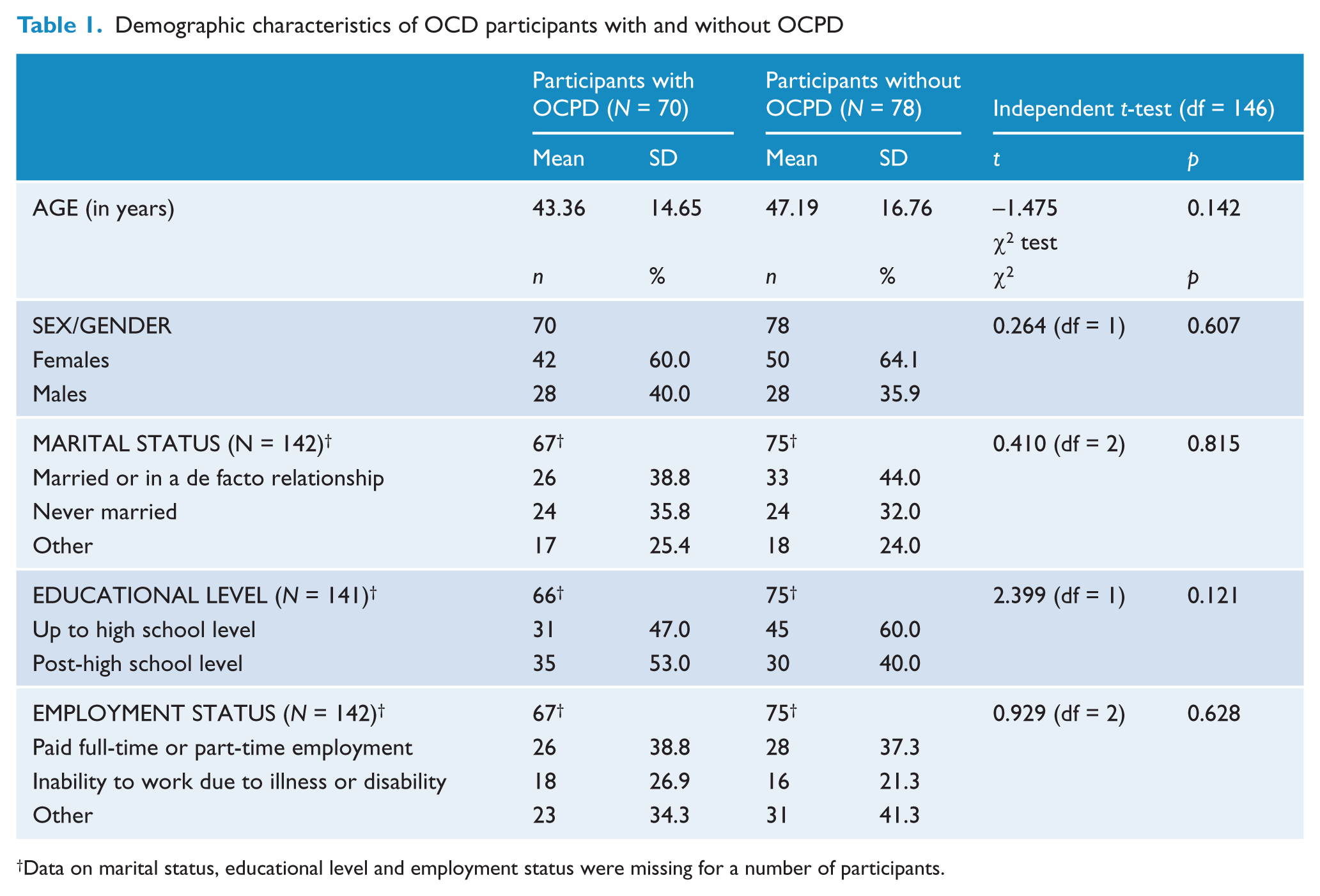
Data on marital status, educational level and employment status were missing for a number of participants.
Table 2 compares participants with and without OCPD in terms of their scores on the Y-BOCS, VOCI, SDS and SCL-90R. The two groups did not differ significantly in terms of the clinician-rated severity of obsessions, compulsions, overall OCD and disability levels. In contrast, results on the self-report VOCI showed that all OCD symptom dimensions except for contamination and checking were significantly more prominent in participants with OCPD. These participants also scored significantly higher on all dimensions of psychopathology, as assessed by the SCL-90R.
Comparisons between OCD participants with and without OCPD in terms of their scores on the Y-BOCS, VOCI, SDS and SCL-90R
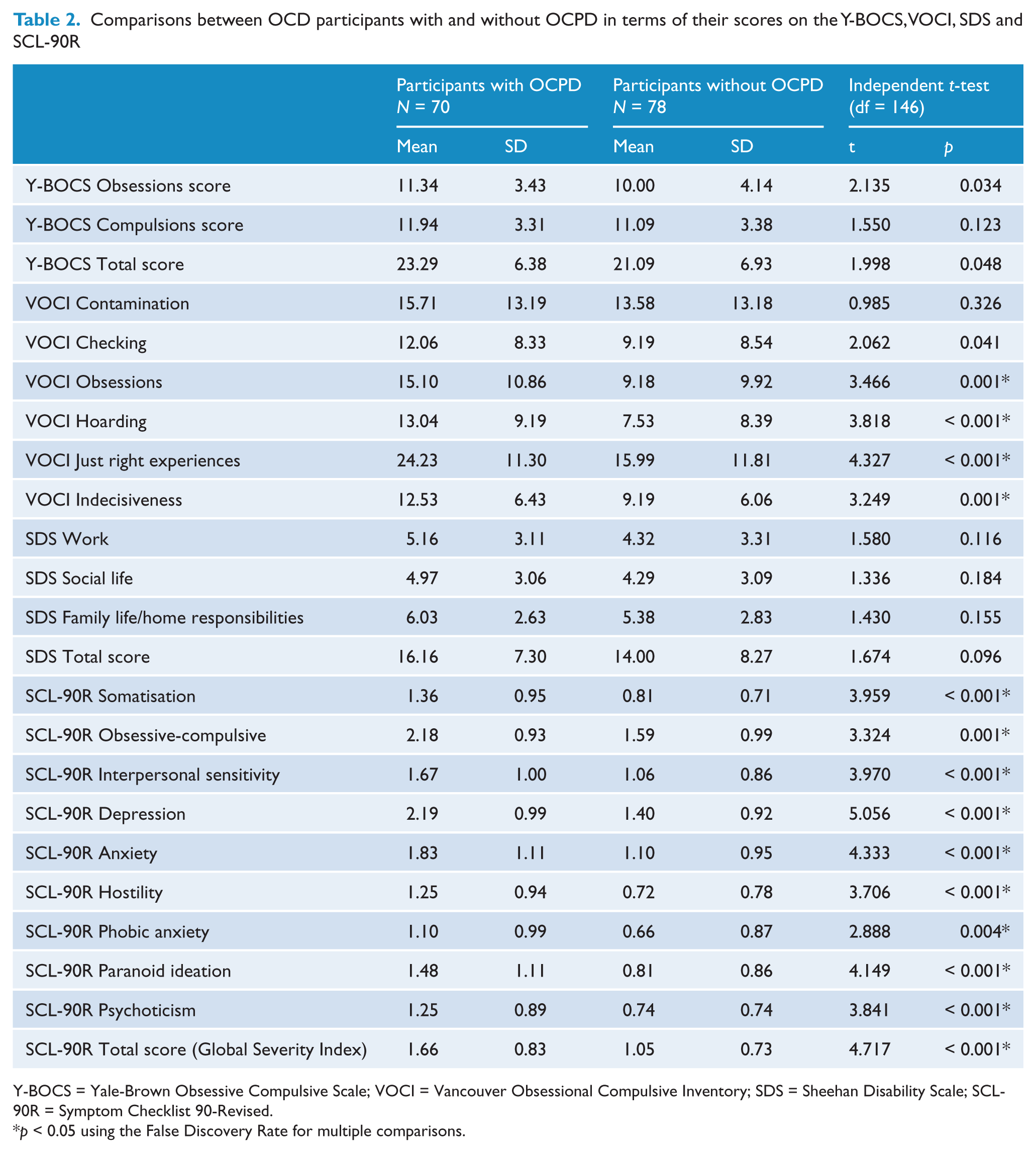
Y-BOCS = Yale-Brown Obsessive Compulsive Scale; VOCI = Vancouver Obsessional Compulsive Inventory; SDS = Sheehan Disability Scale; SCL-90R = Symptom Checklist 90-Revised.
p < 0.05 using the False Discovery Rate for multiple comparisons.
Table 3 shows that there were no significant differences in the frequency of the most prominent obsessions and compulsions between participants with and without OCPD, except for the obsessions involving a need to collect and keep objects and hoarding compulsions, which were significantly more frequent in participants with OCPD.
The frequency of the most prominent obsessions and compulsions in OCD participants with and without OCPD
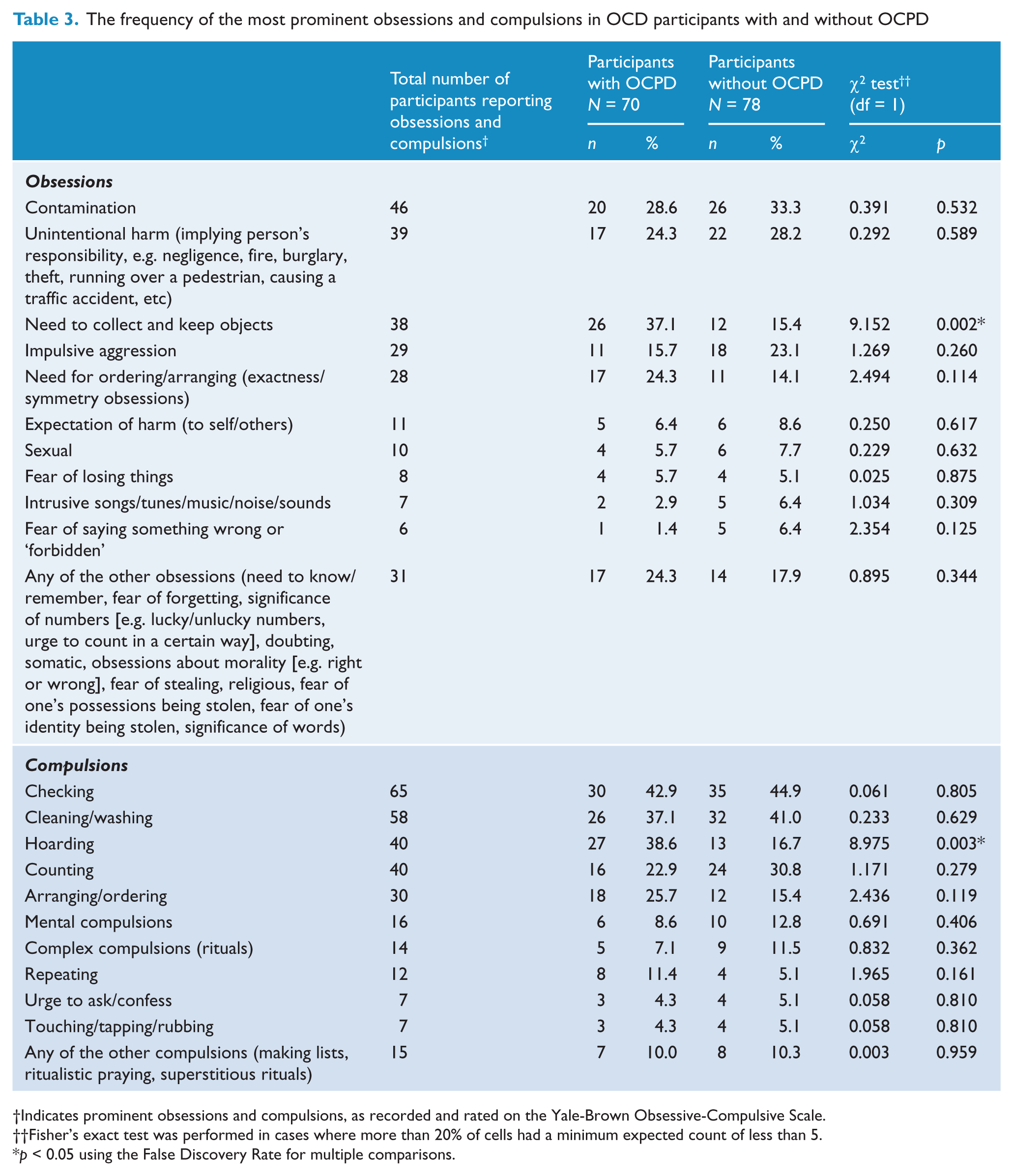
Indicates prominent obsessions and compulsions, as recorded and rated on the Yale-Brown Obsessive-Compulsive Scale.
Fisher’s exact test was performed in cases where more than 20% of cells had a minimum expected count of less than 5.
p < 0.05 using the False Discovery Rate for multiple comparisons.
Table 4 presents the frequencies of current co-occurring disorders in participants with and without OCPD. Only panic disorder was significantly more frequent in participants with OCPD than in those without OCPD.
The frequency of current co-occurring disorders in OCD participants with and without OCPD
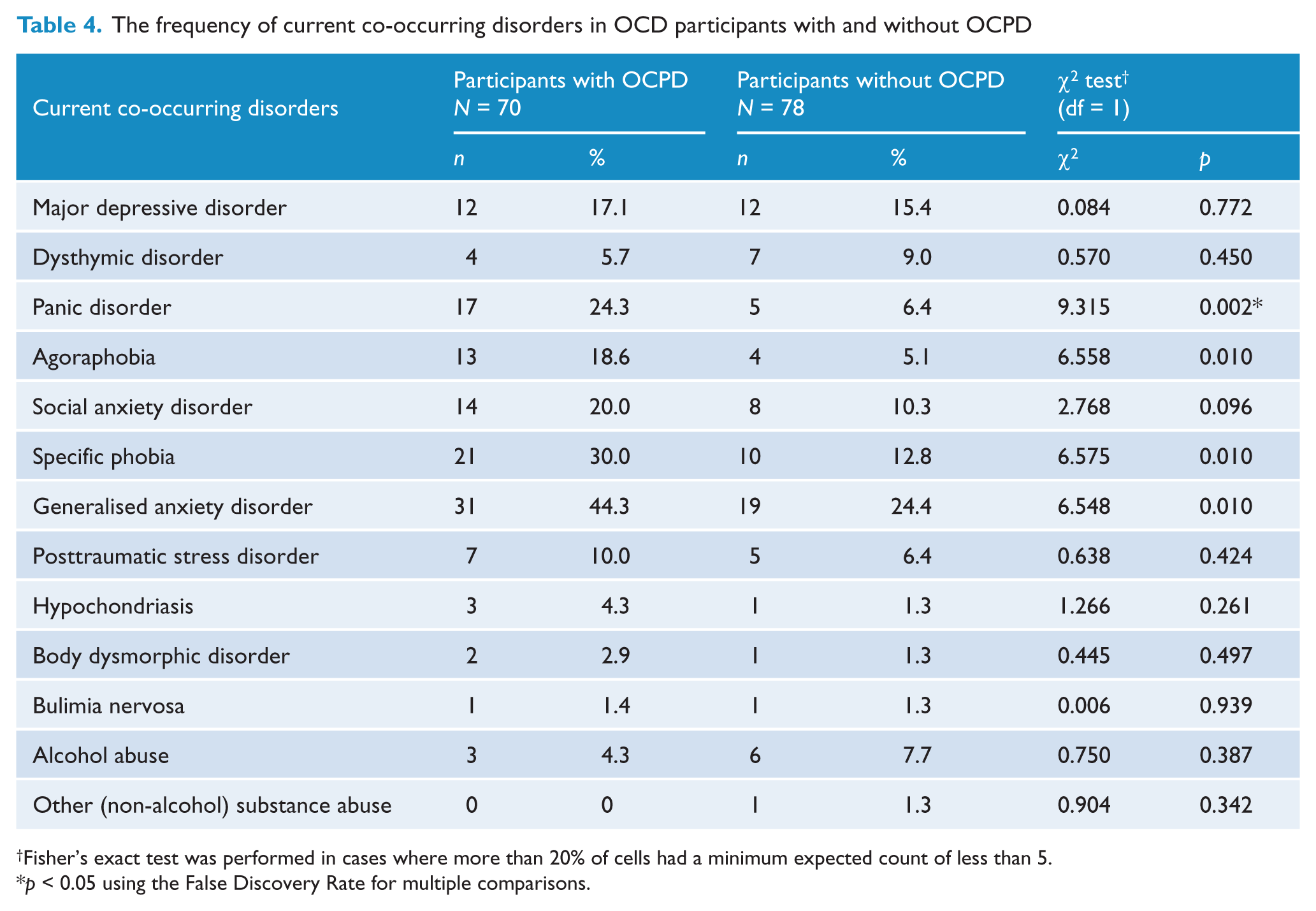
Fisher’s exact test was performed in cases where more than 20% of cells had a minimum expected count of less than 5.
p < 0.05 using the False Discovery Rate for multiple comparisons.
The DSM-IV criteria for OCPD have been criticised as being based on an arbitrary diagnostic threshold (e.g., Pinto et al., 2008); also, compared with the DSM-III and DSM-III-R criteria, the DSM-IV criteria provide a lower diagnostic threshold for OCPD. Therefore, we repeated the same analyses using more stringent criteria for the diagnosis of OCPD by requiring the presence of five out of eight DSM-IV criteria instead of only four. With these criteria, there were 50 (33.8%) participants with OCPD. For 56 of 64 compared variables, comparisons between participants with and without more stringently diagnosed OCPD yielded very similar results to comparisons between participants with and without DSM-IV OCPD. The differences were in terms of the participants with more stringently diagnosed OCPD having a significantly earlier mean age of onset of OCD (15.95 vs. 19.95 years, p = 0.04), significantly greater overall impairment (17.00 vs. 14.01, p = 0.028) and impairment in the domain of family life/home responsibilities (6.36 vs. 5.35, p = 0.033), significantly more prominent checking compulsions (13.18 vs. 9.20, p = 0.007) and a significantly greater frequency of co-occurring agoraphobia (24.0% vs. 5.1%, p = 0.001), generalised anxiety disorder (52.0% vs. 24.5%, p = 0.001), specific phobia (34.0% vs. 14.3%, p = 0.005) and social anxiety disorder (26.0% vs. 9.2%, p = 0.007).
Considering that there were relatively few differences between the results of comparisons using different criteria to diagnose OCPD, further discussion is based mainly on the results derived from the DSM-IV criteria.
Discussion
In our sample of people with OCD, 47.3% met the DSM-IV criteria for OCPD. This percentage was higher than in other studies, where the frequency of the DSM-IV OCPD in individuals with OCD ranged from 22.9–34.7% (Albert et al., 2004; Coles et al., 2008; Garyfallos et al., 2010; Lochner et al., 2011; Pinto et al., 2006, 2011; Samuels et al., 2000). The differences in the rates of OCPD might have been caused by a range of factors, such as different instruments used and different thresholds at which diagnostic criteria are thought to have been met. With the more stringent criteria, about one-third of our sample (33.8%) was diagnosed with OCPD. Relatively small differences between findings of the analyses using DSM-IV criteria and those based on the more stringent criteria suggest that a high percentage of individuals with the DSM-IV OCPD did not reflect a tendency to overdiagnose OCPD.
Several findings of this study need to be noted. First, our OCD participants with and without OCPD did not differ significantly in terms of the clinician-rated severity of OCD and levels of disability. The finding about the severity of OCD is in agreement with most studies (Albert et al., 2004; Coles et al., 2008; Diaferia et al., 1997; Garyfallos et al., 2010; Pinto et al., 2011). In contrast, some studies have reported OCD with OCPD to be a more disabling condition (Coles et al., 2008; Garyfallos et al., 2010; Lochner et al., 2011), and our findings using the more stringent criteria also point in this direction. However, the overall pattern of our results suggests a link between the severity of OCD and levels of disability and fails to support the notion that OCD with OCPD is a more severe condition than OCD without OCPD as far as the clinician-rated severity of OCD is concerned.
Other results of this study indicate that there are differences between OCD individuals with and without OCPD, although they may not be of such proportions to affect the clinician-rated severity of OCD. For example, we found on the VOCI that except for the two most common OCD symptoms, namely contamination/washing symptom dimension and checking compulsions, participants with OCPD had more prominent OCD symptoms. This is broadly in agreement with studies that reported a significantly greater frequency of nearly all compulsions and some obsessions in individuals with OCPD (Coles et al., 2008; Garyfallos et al., 2010; Lochner et al., 2011).
When it comes to the frequency of various obsessions and compulsions, we found that unlike in some previous studies (Coles et al., 2008; Garyfallos et al., 2010; Lochner et al., 2011), only hoarding compulsions and obsessions about a need to collect and keep objects were significantly more common in our participants with OCPD. This difference is likely due to the fact that other studies used the Y-BOCS Symptom Checklist categories, whereas we relied on the three most prominent Y-BOCS obsessions and compulsions.
Results of current and previous research converge to suggest that higher frequencies of hoarding compulsions and obsessions about a need to collect and keep objects among people with OCPD are probably a consequence of an inclusion of hoarding-like tendencies in the DSM-IV criteria for OCPD. This seems to artificially increase an overlap between OCPD and OCD with hoarding symptoms, and contributes to the blurring of a boundary between OCPD and OCD. A ‘redundancy’ between OCPD and OCD regarding symptoms such as hoarding has been noted by others (Pinto et al., 2008), further questioning the optimal way of positioning hoarding vis-à-vis OCPD and OCD.
In comparison with participants without OCPD, those with OCPD reported significantly more distress and more manifestations of all measured types of self-rated psychopathology, including that related to OCD. Likewise, panic disorder was diagnosed more frequently in participants with OCPD, and so were several other anxiety disorders when using the more stringent criteria for OCPD. All this may make the overall clinical presentation of people with OCPD more complex, with possibly adverse effects on treatment. In other words, a possible negative effect of OCPD on the treatment of OCD may be a consequence of more co-occurring symptoms, distress, psychopathology and disorders. This is an issue that requires further study, also in light of the conflicting research findings so far. While some studies reported a poorer response to both pharmacological and behavioural treatment for OCD in the presence of OCPD (Cavedini et al., 1997; Pinto et al., 2011), others did not find OCPD to be a predictor of poorer response to treatment of OCD (Baer et al., 1992; Fricke et al., 2006).
Although our participants with and without OCPD did not differ with respect to the mean age of onset of their OCD, the mean age of onset of OCD was significantly earlier in the group of participants with OCPD when using the more stringent criteria for OCPD. As already noted, previous research has produced conflicting results in this domain (Albert et al., 2004; Coles et al., 2008; Diaferia et al., 1997; Garyfallos et al., 2010; Lochner et al., 2011; Maina et al., 2008), and our findings do not provide a conclusive contribution to the issue. An important methodological problem here is the retrospective, unreliable determination of the age of onset of OCD.
This report should be viewed in light of its limitations and strengths. It is based on cross-sectional assessment, which precluded investigation of temporal relationships between OCD and OCPD and any direct effects of OCPD on treatment of OCD. Although the comparisons between the groups with and without OCPD yield only descriptive findings, these still provide important insights as to how the groups differ and in which domains they are more alike. Another limitation is that interview-based assessments were made by the same clinician. Although we did not have specific hypotheses regarding the findings of the study, clinicians’ expectations might have influenced the results to some extent. We did not assess OCPD dimensionally and did not perform analyses at the level of the OCPD criteria. At the same time, our results, obtained from a large sample by means of a categorical assessment, could be more easily compared with those of other studies that used the same diagnostic approach. Also, unlike other studies, we used self-report, dimensional measures of OCD symptoms and general distress and psychopathology. However, findings obtained from these self-report measures and clinician-administered instruments were somewhat discrepant. This could be due to distortions on self-report measures caused by prominent psychopathology in participants with OCPD, or it could result from clinician bias on clinician-rated measures. Clearly, this calls for further research and examination of the sources of inconsistencies between various types of measures.
In conclusion, the findings of this study suggest that there are no significant differences in the clinician-rated severity of OCD and levels of disability between OCD individuals with and without OCPD. This does not support the notion that OCD with OCPD is a marker of clinician-rated severity of OCD. A high frequency of OCPD among individuals with OCD suggests a strong, although not necessarily a unique, relationship between the two conditions; this might have also been a consequence of the blurring of their boundary by postulating that hoarding and hoarding-like behaviours characterise both disorders. Finally, people with OCPD seem to have more prominent OCD symptoms, they are more distressed and exhibit various other psychopathological phenomena more intensely, which is likely to complicate their treatment.
Footnotes
Acknowledgements
The authors are grateful to Colin Slocombe (ACEDA Adelaide), Michelle Graeber (ARCVIC Melbourne), Dr Scott Blair-West (Melbourne Clinic), the Blacktown OCD Support Group, Julie Leitch (Kogarah OCD Support Group), Linda Junee (Mental Health Association of New South Wales) and the Penrith Mental Health Practitioners Network.
Funding
The Nepean OCD Study was supported by the Nepean Medical Research Foundation and by a grant from the Pfizer Neuroscience Research Grants Program.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.