
Abstract
Depression is a common mental disorder. In Australia the 12-month prevalence for depression is 4.1% of the adult population [1] and accounts for a sizable proportion of disease burden. The most recent Australian burden of disease study suggests that depression and anxiety account for 55% of the total DALYs for mental disorders [2]. International estimates paint a similar picture. The World Health Organization burden of disease study reports that unipolar depression is the third leading cause of burden worldwide [3]. The cost of depression is substantial with recent estimates suggesting that AU$935 million dollars of national health expenditure is spent on depression treatment per annum. A recent meta-analysis [4] of internationally published depression cost-of-illness studies found that despite methodological differences across studies, depression is associated with high annual health sector costs as well as productivity costs. Current treatment of depression in Australia averts 13–16% of the disease burden and even if all depression was treated using evidence-based treatments only 24–52% of the disease burden would be averted [5,6].
It is unsurprising that the prevention of depression is of growing interest to researchers and policy makers. There is a growing literature investigating the prevention of depression in adults and children [7–9]. Much of this literature focuses on the identification of sub-threshold depression (the existence of some depressive symptoms but insufficient to warrant a full major depressive disorder (MDD) diagnosis), known as indicated prevention [10], and the subsequent provision of psychotherapy (usually cognitive–behavioural) to prevent the onset of a full MDD. Existing reviews of these interventions find that they can be effective in reducing the onset of MDD [8]. However, the question of whether such interventions provide good value for finite health resources remains. Few studies have investigated this question [11,12], and these have expressed outcomes in clinical terms rendering comparisons with preventive interventions outside depression impossible.
The current study was undertaken within the context of a larger study, called Assessing Cost-Effectiveness in Prevention (ACE-Prevention). ACE-Prevention aims to assess the cost-effectiveness of 100 preventive and 50 ‘benchmark’ interventions to provide value for money advice to health policy makers. The project avoids methodological confounding since all economic evaluations are undertaken using a standardized framework [13]. The current paper describes the economic evaluation of two types of psychological interventions for the prevention of adult depression following opportunistic screening for sub-syndromal depression in general practice. The first intervention is based on individual self-help with minimal support [14] and the second is based on a cognitive-behavioural group intervention. The paper aims to answer the question of whether the provision of brief psychological therapy or more comprehensive psychological therapy after screening is a good use of health care resources compared to current practice within the Australian context.
Material and methods
General ACE-Prevention methods
The economic evaluations are undertaken within the context of a protocol written for ACE-Prevention minimizing methodological confounding [15]. Evaluated interventions are sourced from the published literature ensuring available evidence of effectiveness. A health-sector economic perspective is adopted with costs divided into government and private. The economic framework is cost-utility analysis. Costs and cost-offsets of interventions are measured in Australian dollars and expressed in the base year of 2003. Unit cost prices not available for the 2003 reference year are adjusted using published health price deflators [16]. Outcomes are evaluated using disability-adjusted-life-years (DALYs). This outcome metric is used across all disease areas evaluated within ACE-Prevention and allows broader across-disease comparisons. The DALY is conceptually similar to a quality-adjusted-life-year (where all years of life lived in a health state are weighted for the quality of life). The striking feature of such measures is that both mortality and morbidity effects of interventions can be measured by the one metric making across-disease comparisons possible. The weights used to value the health states within the DALYs come from the Australian burden of disease studies [2]. Time and travel costs are included, though these are reported separately to the primary health-sector results. We do not include productivity costs, but rather the time it takes users of the intervention to undertake the intervention. As there is no established methodology of valuing time a simple approach based on age/sex adjusted wage-rates is used as a proxy [17]. A 3% annual discount rate is applied to all costs and outcomes, as is commonly used in many Australian studies [18].
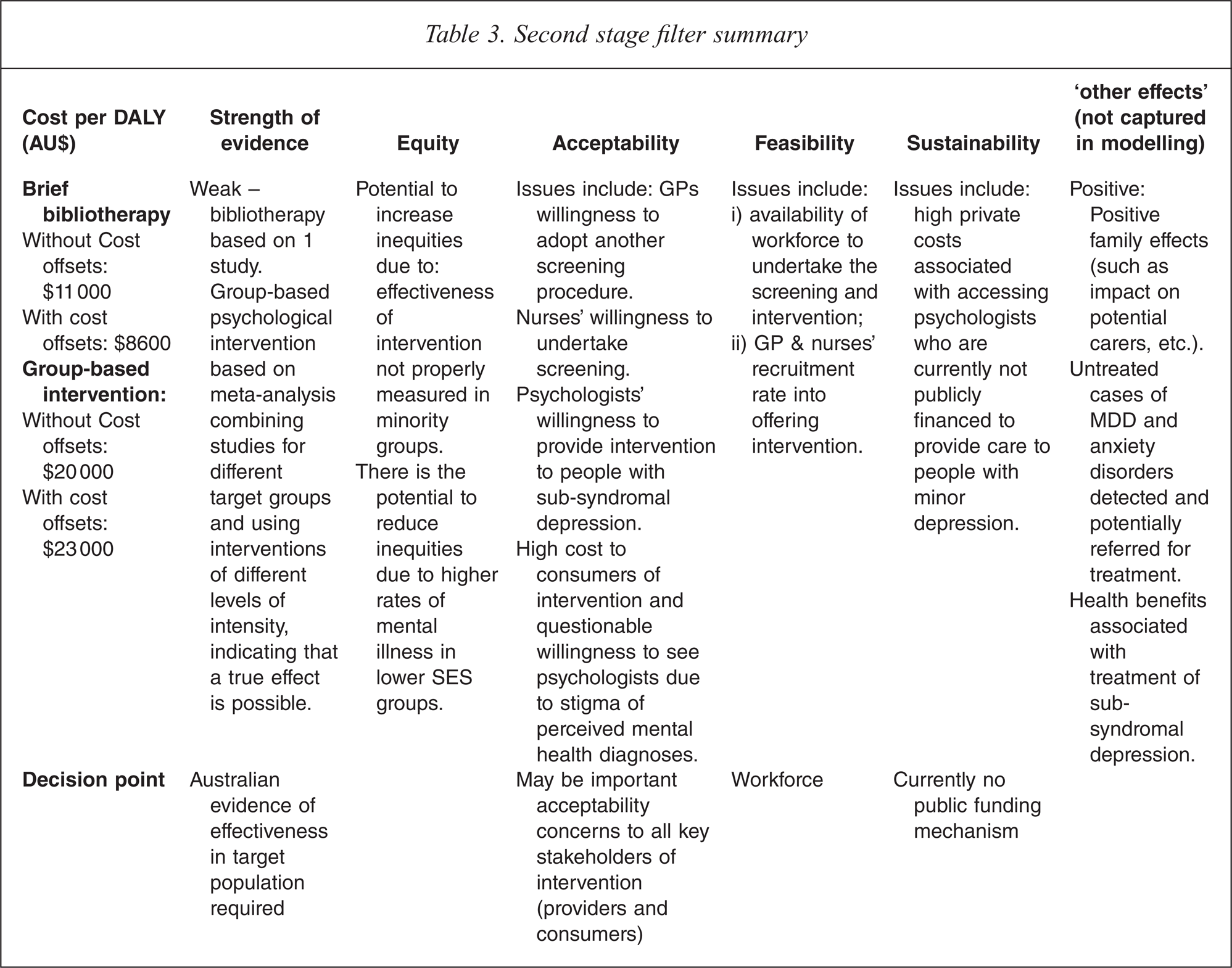
ACE-Prevention uses a $50,000/DALY ‘value for money’ threshold. Interventions whose incremental cost-effectiveness ratios (ICERs) fall below this threshold are considered ‘good’ value for money and interventions whose ICERs fall above this threshold are considered ‘poor’ value for money. This threshold has been used in previous Australian economic evaluation studies and is a ‘rule of thumb’ within the Australian context [13]. It must be appreciated that such threshold cut-offs are somewhat arbitrary since interventions which fall above such thresholds may still be funded. Other principles, such as the rule-of-rescue or equity are important in setting health care priorities over and above efficiency considerations [13]. Hence all results are subjected to a second-stage filter analysis. This analysis tries to capture other non-efficiency (i.e. non-ICER) criteria important to health policy makers. The second-stage filter criteria include:
The strength of the evidence base;
Effects on equity;
‘Feasibility’ and ‘sustainability’ in terms of work force considerations, financing mechanisms and health system structure;
‘Acceptability’ of the intervention to key stakeholders including clinicians, patients and policy makers;
Other important beneficial or harmful effects associated with the intervention not identified in the analyses.
All technical ICERS are discussed in terms of their performance on these second-stage filter considerations.
Specification of interventions evaluated
There are numerous published reviews of interventions designed to prevent depression [8, 9,19–21], the largest of these [9], includes 69 interventions, though the entry criteria for this review was broad and included many studies which reduced depressive symptoms rather than depression. Three reviews focus on studies which objectively measure the incidence of MDD as an outcome [8,19,20]. The most recent of these focuses on psychological interventions for the prevention of MDD and includes interventions aimed at adults and children. The studies included within all reviews were cross-referenced and all studies which objectively measured the incidence of MDD as an outcome from all three reviews are considered relevant for the current evaluation. As such we are confident that Cuijpers et al. [8] includes all relevant studies. As a final check, a primary literature search was conducted in October 2007 using the search terms ‘depress∗’ AND ‘prevent∗’ in Web of Science. This search produced 606 titles and found one more relevant study [22] published after the Cuijpers et al. [8] cut-off date.
Consideration of all studies constituting the Cuijpers et al. [8] review, with the addition of Seligman [22], as a whole is problematic, as a standardized intervention that can be easily costed has to be specified for the ACE-Prevention evaluation context and the population and intervention parameters of the different studies were heterogeneous. It was decided to model the cost-effectiveness of the Willemse et al. [14] intervention as it is suited to the Australian context since it is set in general practice. A second ‘average’ intervention was also defined based on four studies which were conducted in adult populations either within primary care or community settings [22–26]. The interventions evaluated in these studies were more comprehensive in nature compared to Willemse et al. [14] and could be more easily characterized, compared to the entire body of interventions comprising the Cuijpers et al. [8] review.
The first intervention based on Willemse et al. [14] opportunistically screens the general adult population who attend general practitioners (GPs), for sub-syndromal depression (defined as at least one core symptom of depression and three or fewer of the minor symptoms), using a commonly used depression screening instrument (such as the Centre for Epidemiological Studies Depression Scale (CES-D) or the Instel Screening Instrument used in the trial). A trained general practice nurse undertakes the initial screening. People who screen positive are then referred by the GP to a psychologist for the second stage screening, consisting of a formal diagnostic interview (the trial used the Composite International Diagnostic Instrument (CIDI)) to exclude people meeting the diagnostic criteria for a full-blown depressive disorder. Once it is established that the person is eligible for the intervention then a brief psychological intervention is offered consisting of another visit to a psychologist, a self-help cognitive-behavioural therapy manual and six short follow-up telephone calls (we call this intervention ‘brief bibliotherapy’).
The second intervention consists of eight visits to a psychologist, and one booster session all in group therapy format (called the ‘group-based intervention’). The content of the intervention is largely cognitive-behavioural in nature. The intervention parameters are based on four screening studies undertaken in general adult populations [22,23,25,26].
Both interventions are aimed at the Australian 2003 population who attend a GP and meet the criteria: no current or past (in last 12 months) diagnosis of MDD, dysthymia, bipolar disorder, social phobia, agoraphobia or panic disorder; not receiving psychotherapeutic treatment in the last year; not suffering from any psychotic disorder; at least one core symptom of depression (sadness or loss of interest); and 1, 2 or 3 of the other minor symptoms of depression. The proportions of the Australian adult population who meet the criteria for the intervention were all derived from the 1997 National Survey of Mental Health and Well-Being (NSMHWB).
The ‘current practice’ comparator for both interventions is ‘do-nothing’ as they are aimed at people who meet the above criteria and are not receiving any psychological treatment.
Efficacy/effectiveness of interventions
The study by Willemse et al. [14] used a randomized design and followed participants for one year using the incidence of depression as the key outcome. The proportion of the population screened (72%) and the proportions of people participating in the intervention were sourced from this study. Willemse et al. [14] were interested in the added value of bibliotherapy over care as usual, and the corresponding unidirectional hypothesis was tested in a 1-tailed test, accordingly powered. The study found that 12% of the intervention and 18% of the control group became depressed at follow-up (p = 0.049, 1-tailed). Nevertheless, this small trial provides only weak evidence on the intervention's effectiveness. Even though the study does not have strong effectiveness credentials, we modelled the effectiveness as reported in the trial expecting some of the uncertainty iterations to show no benefit associated with the intervention.
The meta-analysis by Cuijpers et al. [8] was used as the primary measure of effectiveness for the group therapy intervention (the inclusion of Seligman et al. [22] did not dramatically alter the results, hence we opted to use the published results). This meta-analysis found that the relative risk of developing depression in the intervention group was 0.78 (95% CI 0.65–0.93). It combined studies undertaken in various settings with different target populations and is therefore not ideal. Given that no heterogeneity attributable to study sample type (i.e. children, adults, etc.) was found by Cuijpers et al. [8] we decided to use the results from this meta-analysis (rather than the less robust estimate based on the four smaller studies alone). It should be noted that the proportions of the population screened and the proportions participating in the evaluations in the four general adult studies (when reported) were very similar to the Willemse et al. [14] trial and hence were not altered in the two evaluations (proportions are listed in Table 1).
Uncertainty parameters used in the simulation analysis
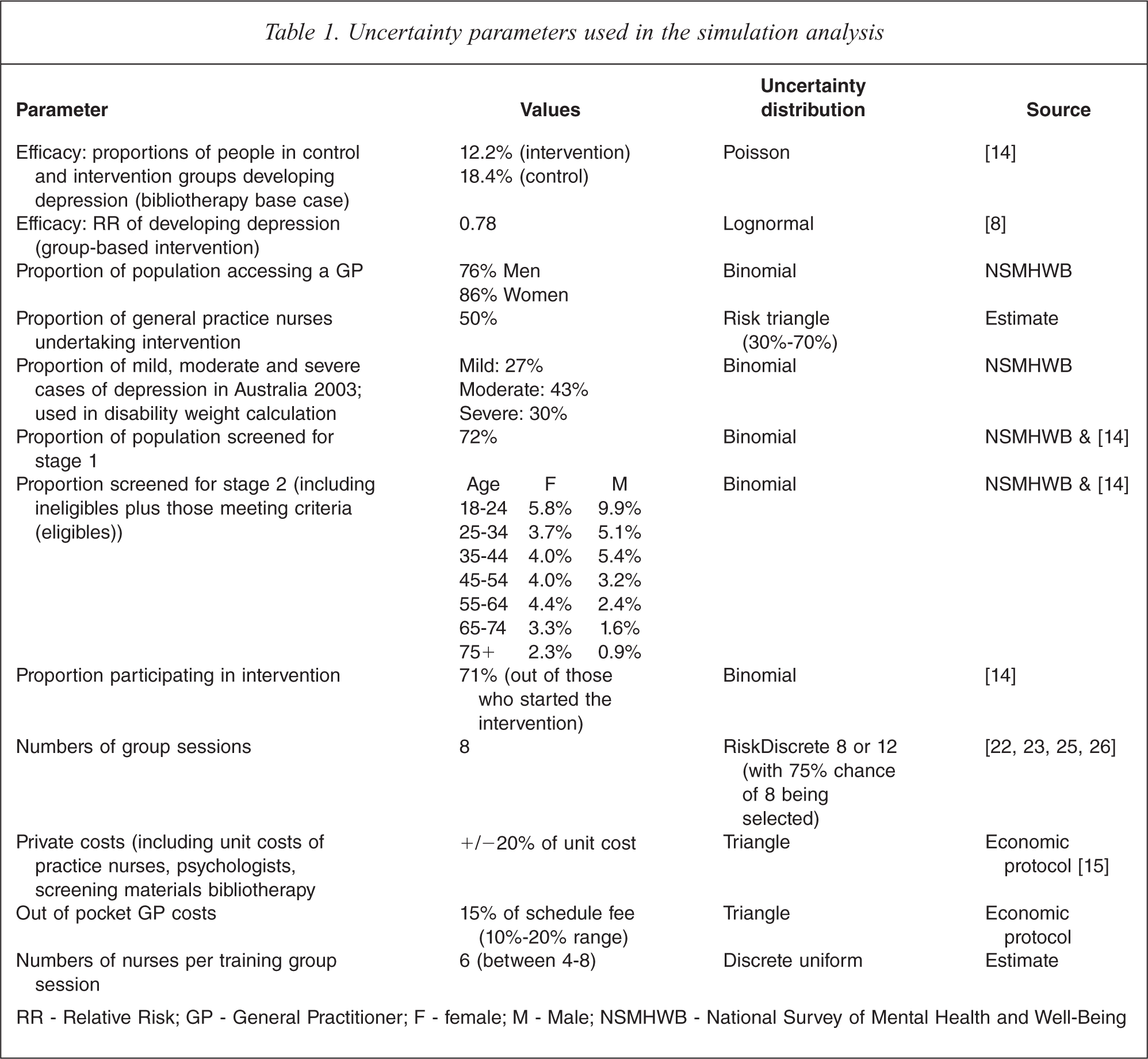
RR – Relative Risk; GP – General Practitioner; F – female; M – Male; NSMHWB – National Survey of Mental Health and Well-Being
Modelling to health outcomes
The numbers of people meeting the specification criteria for both interventions were modelled through a Markov chain with one-year cycles for a period of five years. A 5-year time horizon is chosen since the longer term epidemiology of depression is not well investigated and only limited data are available to accurately model the life-time course of the disorder [5]. This time horizon is also consistent with other Australian economic evaluation studies in depression [5,27]. Secondly, the intervention studies all had short follow-up durations (usually 1–2 years) and the long-term effectiveness of such interventions is unknown.
The health states in the chain are ‘non-depressed’, ‘depressed’ (meeting the criteria for MDD) and ‘dead’. We have not modelled sub-syndromal depression as a separate health state as the focus of this intervention is the prevention of MDD. The model incorporates mortality risks from suicide and all other causes modelled separately. The probabilities of converting to depression come from the trial data, with an adjustment made to the probabilities associated with conversion to MDD to account for age/sex differences in the incidence and prevalence of MDD in Australia. This was necessary because the proportions of young males meeting the criteria for the intervention were high (e.g. 10% of males aged 18–24), though the incidence of depression in this group is low. Conversely, the proportions of women aged between 45–54 meeting the criteria for intervention eligibility was 4%, though the incidence of depression in this group is higher.
The non-fatal and fatal health benefits associated with reduction in the progress to MDD in the intervention case are modelled using epidemiological estimates of disease duration, severity and risk of suicide from a model for depression developed for a prior economic evaluation of the treatment for depression [5]. Disease duration was determined from a microsimulation model using published estimates of time to recurrence and duration of episode [5]. The disease disability weight for MDD is a weighted average determined from the proportions of mild, moderate and severe cases of depression in Australia (estimated from the NSMHWB) along with the associated Dutch disability weights [28] (0.14, 0.35 and 0.76 respectively). A 50% decay rate of benefit is modelled for years 2–5 for both interventions (by year 5 the intervention effect is almost non-existent). This decay effect is consistent with Cuijpers et al. [8] who found that intervention effects are reduced over time.
Costs of interventions and offsets
The costs of the brief bibliotherapy intervention include the costs of: i) training practice nurses in opportunistically screening people for sub-syndromal depression; ii) practice nurse time in undertaking the opportunistic screening (assumed to be 15 minutes); iii) the screening instrument; iv) a GP in referring the person to a psychologist for further assessment; v) a private psychologist for two full face-to-face consults (one for assessment and one for the intervention) and six short telephone calls; and vi) the CBT manual. The latter two of these cost items and a patient contribution element of the GP visit are borne by patients. The unit costs of resource use were based on published prices or costs, i.e. GPs costs were sourced from the Medicare Benefits Schedule (Medicare is the publicly financed universal health insurance scheme available in Australia); practice nurse costs were sourced from the Australian Practice Nurse Association (APNA); the cost of psychology services was sourced from the Manual of Resource Items and their Associated Costs [29]; and, manual and screening instrument costs were based on trial estimates.
The costs of the group therapy intervention included the same items i) to iv) above; v) the cost of a private psychologist (one full face-to-face consult for assessment and nine group sessions lasting two hours (with an average of 10 participants) for the intervention (eight for the initial therapy and one booster session); and vi) the cost of non-adherers (that is people who did not complete the intervention where non-completion is assumed to be a maximum of three 2-hour group sessions with a psychologist). The unit cost associated with group therapy sessions was derived from the Medicare Benefits Schedule.
The cost-offsets of the interventions were defined as the costs associated with the treatment of MDD. These costs were estimated from the Australian Institute of Health and Welfare's (AIHW) Disease Costs and Impact Study [16] based on standardized national health expenditure records.
Time and travel costs for patients were assessed for the brief bibliotherapy intervention using the following assumptions: stage 1 screening 0.5 h (15 min screening, 15 min waiting, no travel time as the screening is opportunistic); stage 2 screening 1.6 h (includes time with GP, travel time to the psychologist and time with the psychologist; 9 h intervention time (average time it takes to work through the manual sourced from [12]); and 3 trips (1 to GP and 2 to psychologist).
For the group-based intervention the same time assumptions have been used for stage 1 and stage 2 screening. The following assumptions have been specifically used for this intervention: 18 h intervention time (accounting for nine 2-h group therapy sessions); 11 trips (1 to GP and 10 to psychologist).
Key assumptions
Some of the key assumptions of the current analysis include:
practice nurses are able to appropriately administer the screening tool and identify intervention candidates;
the epidemiology of MDD (both the non-fatal and fatal components) after sub-syndromal depression is similar to ‘general’ MDD (determined from existing overseas cohort studies);
there is no dose effect of the brief bibliotherapy intervention (unlike face-to-face CBT for a full MDD, where at least six sessions must be completed for a benefit to be observed);
all participants are given the group therapy intervention in group format (all studies were in group format);
one therapist provides the group therapy sessions;
adherence and participation rates of bibliotherapy are similar to those observed in Willemse et al. [14];
between 85% and 50% of people in the group therapy intervention will not adhere to the intervention (adherence defined as at least four sessions); and
there is a 50% decay rate of effect after the first year for both interventions.
Uncertainty and sensitivity analysis
To incorporate the uncertainty associated with all costs and outcomes we use Monte Carlo simulation modelling and present uncertainty ranges as well as point estimates for benefits, costs, cost offsets and cost-effectiveness ratios. Details of the parameters varied in the uncertainty analysis are presented in Table 1. The results from these analyses are presented as scatterplots on a cost-effectiveness plane and acceptability curves.
Sensitivity analysis is a useful addition to probabilistic uncertainty analysis, as it allows the impact of individual assumptions of key design features of an intervention to be examined. We explored in univariate analysis the following scenarios:
Decay rate (conducted in both interventions)
Alteration of Markov model time horizon (only conducted in brief bibliotherapy intervention)
Medicare Benefits Schedule financing of psychologists for brief bibliotherapy intervention
Best Case Analysis
Results
The ICERS and costs of the both interventions are detailed in Table 2.
Results of reference case analysis for brief bibliotherapy and group-based psychological interventions
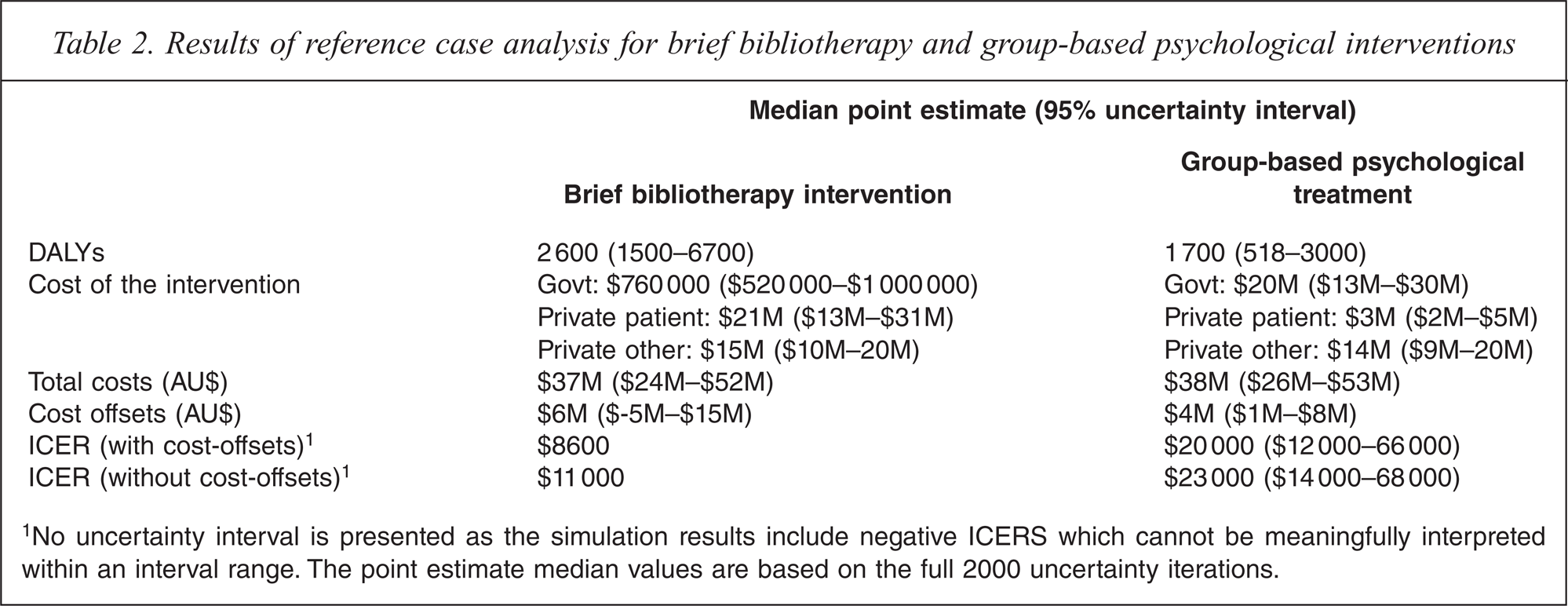
1No uncertainty interval is presented as the simulation results include negative ICERS which cannot be meaningfully interpreted within an interval range. The point estimate median values are based on the full 2000 uncertainty iterations.
The brief bibliotherapy intervention was found to be cost-effective, though in 11.5% of the simulations a negative health benefit was modelled (i.e. there were more cases of depression in the intervention group compared to the control), refer to Figure 1, black scatter plot. This finding can be attributed to the weak measure of effectiveness used in the analysis (the confidence interval around the relative risk of progression to MDD reduction spans 1.0) and is more appropriately interpreted as no benefit rather than a negative benefit since there are no compelling arguments to believe that the intervention is harmful. The acceptability curve (Figure 2, black curve) and the scatter plot show that in 18% of the simulations the intervention is not cost-effective (there is either no health benefit or the ICER falls above the AU$50 000/DALY threshold).
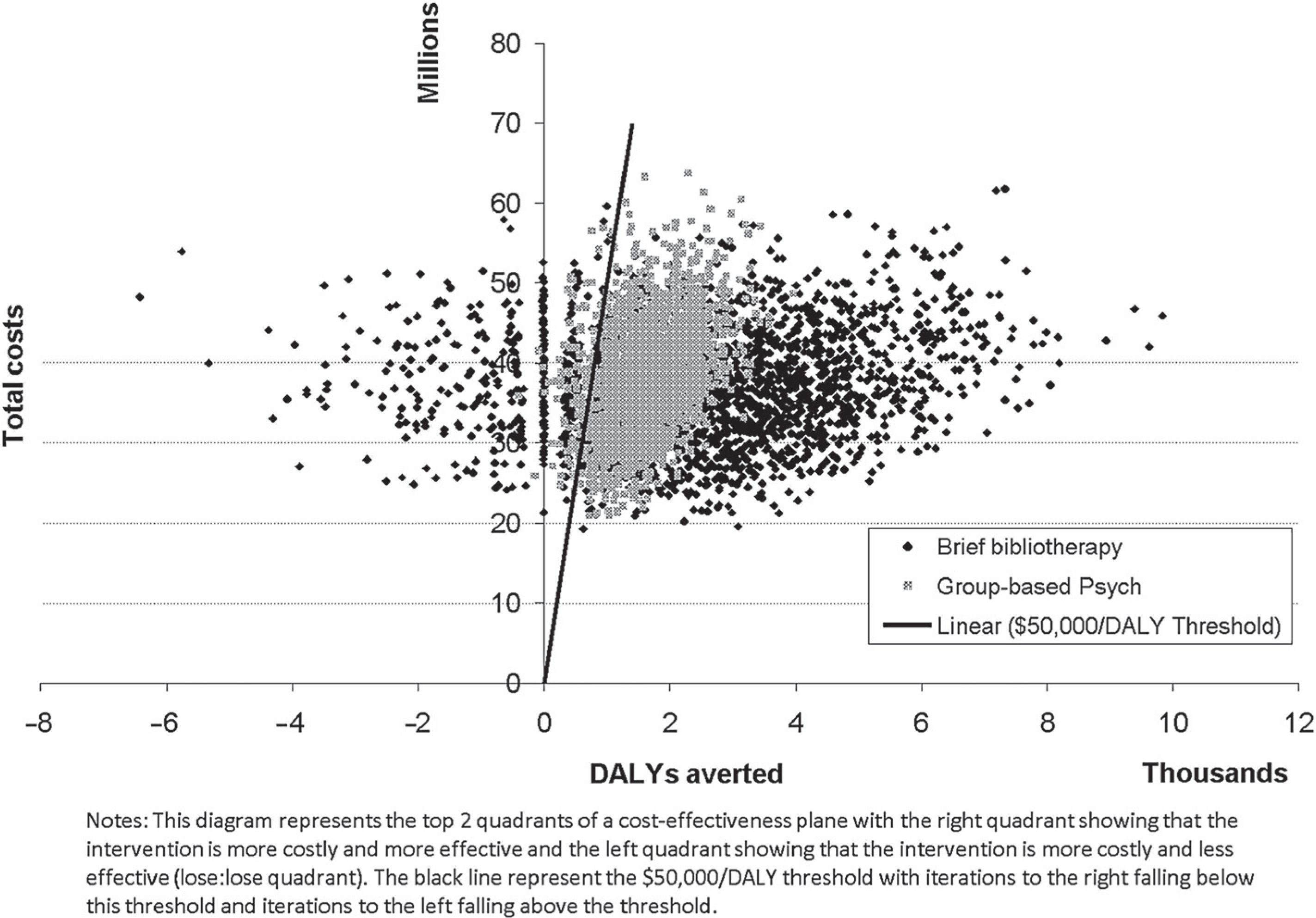
Scatter plot of 2000 uncertainty iterations with $50,000 per DALY threshold cut-off.
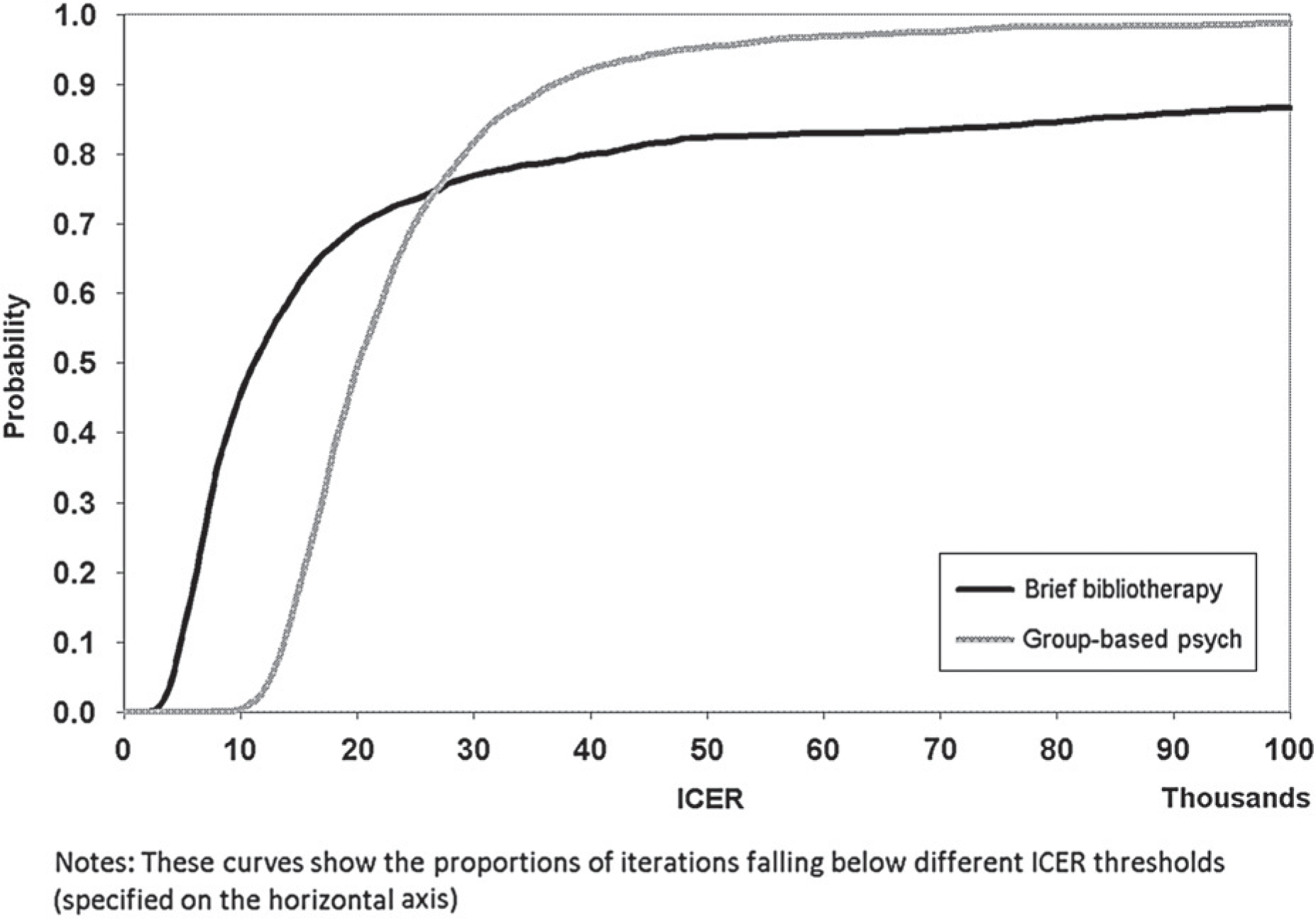
Acceptability curve (including cost offsets).
Most health gain in DALYs is from depression improvement (89%), with a smaller contribution from averted suicide. The difference in the DALYs averted between the two interventions is due to the way benefit was modelled. The group-based psychological intervention was based on a smaller RR of MDD reduction.
The group-based psychological treatment intervention was also found to be cost-effective with only 4% of the iterations falling above AU$50 000/DALY (Figure 1 grey scatter plot and Figure 2 grey acceptability curve). In contrast to brief bibliotherapy, very few iterations showed no health benefit because the measure of effectiveness is based on a large meta-analysis with significant differences observed.
The inclusion of time and travel costs increase the ICER with cost-offsets for brief bibliotherapy to AU$21 000 per DALY and for the group-based psychological intervention to AU$44 000 per DALY.
A discussion of second-stage filter considerations relevant to these interventions is provided in Table 3.
Second stage filter summary
Sensitivity analyses
Decay rate
Alteration of Markov model time horizon (bibliotherapy intervention only)
Medicare Benefits Schedule financing of psychologists for bibliotherapy intervention
Best case
Discussion
Both of these interventions represent potential good value for money. Extensive sensitivity analyses support this conclusion. However, the indices of effectiveness upon which each of the analyses are based are somewhat weak. The effectiveness of the brief intervention is based on a single trial and that of group therapy is based on a meta-analysis which includes a variety of studies with limited generalizability. When bibliotherapy is assessed using the current financing of psychologists, along with the measure of effectiveness from Cuijpers et al. [8], the median ICER is AU$16 000/DALY, which is below the median ICER of AU$21 000/DALY for the group therapy intervention. Furthermore, under the best case scenario sensitivity testing up to 20% of the disease burden attributable to depression in Australia can be averted. Since the majority of iterations fall below AU$50 000/DALY and there are few preventive interventions for mental disorders available within Australia, piloting and evaluation, particularly of brief bibliotherapy, is warranted.
There are issues with respect to acceptability of the intervention to GPs and psychologists as well as the end-users of the intervention (people with sub-syndromal depression). There are also substantial work-force issues, since these interventions are ideally delivered by psychologists who are already stretched within the current health care system (particularly in Australia since the introduction of Medicare rebates for depression treatment).
The only other published economic evaluation of preventive interventions in adult populations is based on the randomized trial of brief bibliotherapy and used a broader costing perspective compared to the current study [12]. The study framework was cost-effectiveness where results were reported in costs per depression-free day. Our current analyses are in keeping with those reported in Smit et al. [12], though are more conservative with respect to cost-offsets as only savings associated with depression averted are included. Smit et al. [12] found that the medical costs of the intervention group were lower than the control group. However, the control group received care by GPs who were asked to base treatments on the Dutch primary care guidelines for depression. It is unlikely that in standard practice this would occur, therefore the increased costs associated with the control group are a result of the trial requirements and unlikely to be realized in standard practice. Furthermore, the current results compare favourably with economic evaluations of the treatment of depression [5,27].
It is important to note that the interventions may not be true ‘primary’ prevention as it is possible that people who had prior episodes of depression (>more than 12 months ago) may be offered the intervention. Therefore the target population is likely to be a mix of people with no history of depression as well as people with a prior history (over 12 months). Since most adult mental disorders are preceded by mental disorders in childhood/adolescence (though not necessarily the same ones) [30] this is probable. From a public health perspective this distinction is less important as treatment would not be withheld in either case. Secondly, studies of primary prevention (that is first-ever incidence) are very difficult in mental health since there is no psychometrically validated diagnostic tool which reliably assesses lifetime incidence.
Economic modelling methods allow a more complete analysis of the economic credentials of health interventions to be gained over and above the information offered by clinical trials alone (e.g. the evaluation can include longer time horizons and population-wide intervention dissemination). However, modelling techniques have limitations. Many assumptions are required, particularly pertaining to the generalizability of information used from international studies, regardless of whether these are clinical trials or epidemiological studies. While every effort is made to ensure such assumptions are based on high quality empirical estimates, this is not always possible. Therefore, while the current evaluation is explicit in its assumptions, it cannot be guaranteed that each assumption is accurate. Of note are the epidemiological parameters for depression. While we have used the best available estimate for parameters such as duration of depression episodes or relapse rates, sufficient information is not available to know with certainty the lifetime epidemiology of depression. It is reassuring that sensitivity testing around the 5-year time horizon of the model shows that the results are robust to this parameter.
Finally, this analysis presents a ‘partial’ picture of the benefit associated with screening for sub-syndromal depression. Untreated cases of full MDD and possibly anxiety will also be detected and referred for treatment. Furthermore, there may also be health benefits associated with the treatment of sub-syndromal depression. Therefore the current analysis is conservative in the benefits attributable to the intervention. So in answer to the question of whether the prevention of depression by the two modelled interventions represent good value for money, the answer is yes, particularly brief bibliotherapy, though further evaluation is required to confirm that the interventions truly are effective and the parameters used in the modelling framework are generalizable to the Australian context.
Footnotes
Acknowledgements
The authors would like to thank Pim Cuijpers for advice regarding the effectiveness measures used in this study.