
Abstract
Major depression is the commonest mental disorder in Australia [1] and causes more disability than any other disease [2]. Effective treatment options with antidepressant drugs and/or a specific, effective psychotherapy exist and are recommended by treatment guidelines [3], [4]. Among the psychotherapeutic approaches cognitive–behavioural therapy (CBT) and interpersonal therapy have the best-documented efficacy. In addition, there are self-help variants of CBT using books (‘bibliotherapy’) and/or the Internet. However, a significant proportion of people identified with depression in a community survey reported not to have sought any care and those seeking care often did not get adequate treatment [1]. In a previous analysis, we have indicated that a meaningful reduction of the burden of depression in Australia would only take place if depression was treated as a chronic episodic condition requiring maintenance rather than episodic treatment [5]. In this paper, we present the cost-effectiveness of different treatment options for depression.
There is little comparable information on the cost-effectiveness of the different treatment options in the literature which consists predominantly of drug-comparison studies of tricyclic antidepressants (TCAs) and newer antidepressants such as the selective serotonin re-uptake inhibitors (SSRIs). There are a number of methodological problems with most of these studies and none are directly transferable to the Australian health-care system because of differences in costs of these treatments.
To overcome these shortcomings, as part of the Assessing Cost-effectiveness – Mental Health (ACE-MH) project and using a common economic protocol [6], we decided to evaluate the available evidence on costs and benefits of CBT and antidepressant drugs in the treatment of episodes of major depressive disorder and as maintenance treatment in the prevention of recurrence of depressive episodes.
Method
The general methods of ACE-MH are reported in detail elsewhere [6]. In brief, interventions are chosen as options for change compared to current practice in the year 2000. Costs accruing in the Australian health sector, that is, including all health service costs and patient outof-pocket costs, are estimated and discounted at 3% back to year 2000 values.
A Steering Committee of mental health experts, policy makers and representatives of community organizations selected the interventions for analysis, scrutinized the assumptions made in modelling cost-effectiveness and assisted in defining and applying a set of ‘second filter’ criteria (quality of evidence, equity, feasibility and acceptability to stakeholders), which can potentially influence conclusions drawn based only on cost-effectiveness considerations.
The selected interventions for adult depression include:
We model the impact of the acute episode interventions (options 1–4) in Australians experiencing at least one episode of major depression in the year 2000 (513 000) who sought care (302 000) but did not receive an evidence-based treatment (122 000). These estimates are based on the 1997 Survey of Mental Health and Wellbeing (SMHWB) [1]. The criterion for seeking care was consulting for a mental health problem with a psychologist, psychiatrist, general practitioner (GP), surgeon, social worker, mental health team worker or an admission to hospital. We defined evidence-based treatment as a minimum of three such consultations and having received medication and/or CBT. We assume that only 15% of patients are likely to take up bibliotherapy. We model the impact of maintenance interventions (options 5–7) in all people seeking care for depression in the year 2000 assuming maintenance treatment is not part of current practice.
Health benefit
The health benefit of each intervention is measured in disability adjusted life years (DALYs) including a non-fatal component, years lived with disability (YLD), determined by the severity-weighted time lived with depression and a smaller fatal component, years of life lost (YLL), calculated as the discounted stream of life lost because of suicide.
Modelling health benefits requires data on the epidemiology of depression (duration of episodes, time to next episode and severity) and the impact of interventions (on severity and duration of episodes, on the risk of recurrent episodes and the risk of suicide while depressed). A companion paper focusing on the impact of treatment options on the size of the depression burden in Australia [5] provides details of the methods of estimating health benefits (Table 1).
Model input parameter values and sources of information
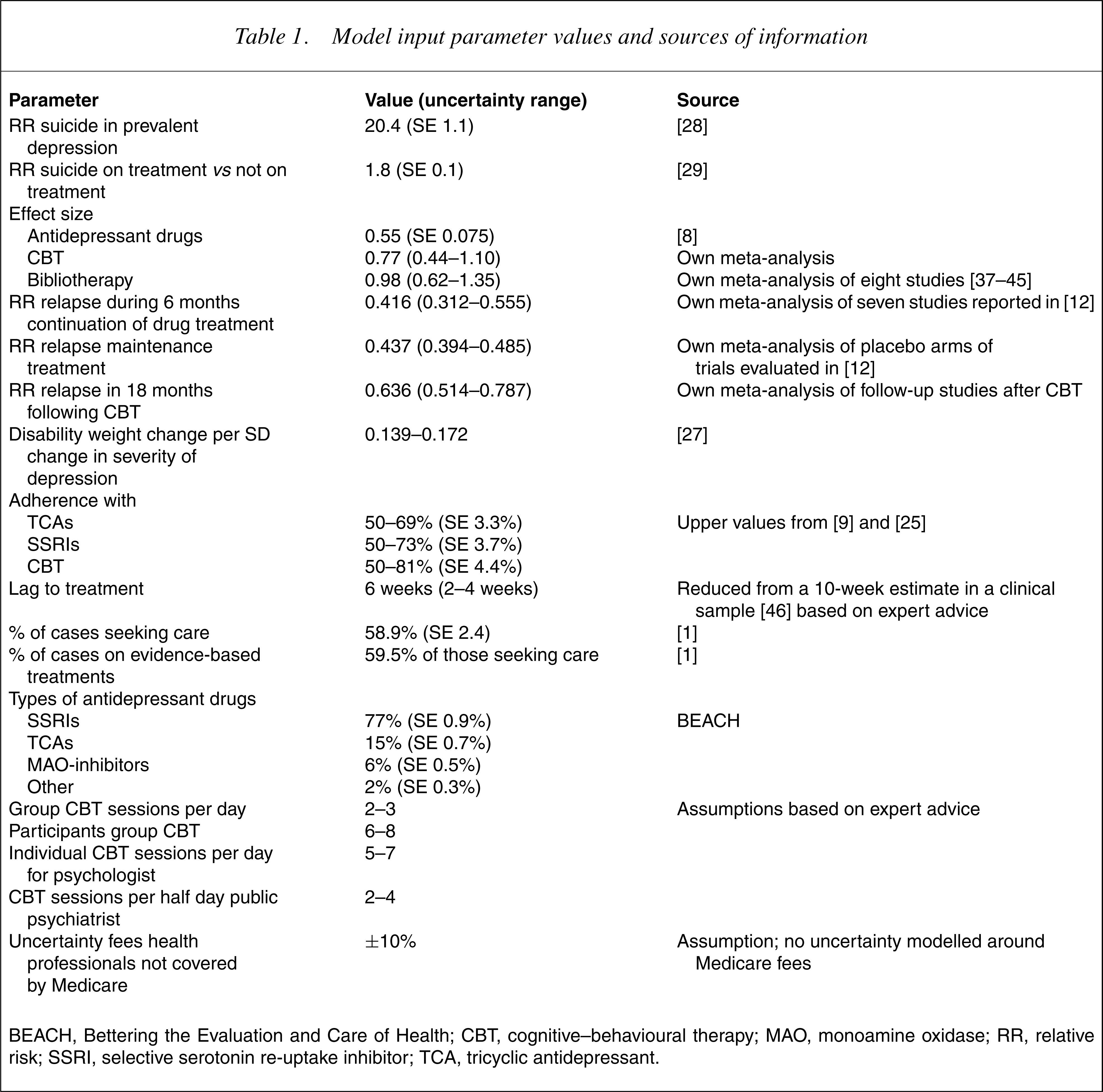
BEACH, Bettering the Evaluation and Care of Health; CBT, cognitive–behavioural therapy; MAO, monoamine oxidase; RR, relative risk; SSRI, selective serotonin re-uptake inhibitor; TCA, tricyclic antidepressant.
We estimate the average duration of episodes and the proportion of time spent in depression following an episode from data published on community follow-up studies. We grade the severity of prevalent cases of depression from the SMHWB by the number of standard deviations (SDs) from the mean Mental Component Score (MCS) of the SF-12 into normal (<45) mild (35.1–45), moderate (25–34.9) and severe (<25) and apply disability weights (DW) for mild (0.14), moderate (0.35) and severe (0.76) depression [7] thatwere also used in the Australian Burden of Disease Study [2]. From the international literature on randomized controlled trials, we derive impact measures that alter the severity of depression during an episode or alter the duration of the next episode. The pooled effect size for SSRIs over placebo is 0.55 (95% CI=0.40–0.70) and no difference is reported between four different SSRI drugs [8]. Meta-analyses also consistently show no difference in efficacy between SSRIs and TCAs [9–11]. From the published figures of a recent meta-analysis [12], we derive a pooled reduction in the risk of relapse for continuation and maintenance of antidepressant drug treatment (Table 1).
From our own update of the Gloaguen meta-analysis of cognitive therapy [13] we estimate a pooled-effect size of 0.77 (95% CI=0.44–1.10). Two outlier studies by the same author determine much of the heterogeneity between results. Excluding these studies reduces the effect size to 0.54 (95% CI=0.29–0.79) We base our main results on the first estimate but test the sensitivity of results if using the lower estimate. Our review of the naturalistic long-term follow-up studies following trials comparing CBT with antidepressant drugs in acute episodes [14–18] indicates a prolonged effect for 18 months after the treatment period. Two small trials of maintenance CBT suggest a similar impact of maintenance strategies with antidepressant drugs or CBT [17], [19].
Adherence
Several recent meta-analyses with a large overlap in the studies included report 3–6% lower discontinuation rates for SSRIs in comparison to TCAs [8–10],[20]. As most trials are of short duration representing what is possible with motivated patients and doctors, adherence rates for SSRIs and TCAs may be more divergent than what has been found in the controlled-trial literature. Four studies of primary care report patient adherence ranging from 50% to 66% but do not make mention of the type of antidepressant [21–24]. Although trials of CBT on average report 81% adherence [25], a community study recruiting volunteers via the local media for a 12-week course of CBT reported 47%, dropping out mostly in the first 3weeks [26]. Consistent with other analyses in the ACE-MH project, we model adherence to range between the recorded adherence level in trials and an estimated lower level of 50% adherence in community settings.
Calculation of benefits
As described elsewhere [6], we use two methods to translate the effect size into a health benefit. Briefly, the first method relies on an Australian valuation study which quantified a mean DW change for each SD change in severity of depression [27]. As the effect size quantifies the impact of an intervention in SD units, the product of the effect size and the mean DW change per SD represents the health gain. The second method applies the effect size to the MCS of the SF-12 across eligible respondents in the mental health survey after which the difference in average DW with and without treatment is calculated. Both methods are incorporated in our uncertainty analyses. This results in a broadening of the uncertainty ranges around the cost-effectiveness ratios, reflecting the absence of an established method for translating effect sizes into a change in DALY DWs.
Reductions in the DW are only applied to the time from the commencement of the intervention taking into account a lag to treatment-seeking. We model that those not adhering to treatment gain no health benefit although they can incur some costs.
During the continuation and maintenance treatment periods following an acute episode, we assume that the reduction in risk of recurrence or relapse can be applied to the average time spent in depression. The comparator in the analysis for each intervention is continuation of current treatment-seeking patterns including a lag to treatment-seeking for each new episode. For bibliotherapy we model health gain during the acute episode only. This may well be an underestimate as it is not unlikely that this self-help variant of CBT also has benefits beyond the acute episode. We make this decision because we have no direct evidence for a sustained benefit and because the cost-effectiveness ratio is very favourable because of the very low cost of the intervention.
From the point prevalence of depression in the SMHWB, an estimate of the relative risk for suicide of 22.4 from a meta-analysis [28] and observed suicide deaths in Australia in 2000, we derive suicide deaths attributable to depression by age and sex. We assume an RR of 1.8 from Swedish routine data collection systems [29] applies to those who are not on effective treatment. No information is available that suggests that TCAs or SSRIs differ in their ability to prevent suicide and therefore we use the same estimate for both drug classes. In the absence of long-term studies, we also assume that suicide rates are similar in patients on CBT as in those on antidepressant drugs. As in the Australian Burden of Disease Study, the YLL associated with a death are calculated as the cohort life expectancy for each age and sex category. We then divide the total YLL for suicide in treated and untreated depression by the person-years of depression in 2000.
Health service costs
In our cost estimates we assume the same mix of providers as reported in the SMHWB, prescribing and supervising drug treatment (56% GP) only, 10% psychiatrist only and 33% GP plus psychiatrist). We take into account weekly visits in the first month, monthly visits for 2 months and then every 3 months for review. For those seeing both a GP and a psychiatrist we include one initial GP visit for referral, weekly sessions with a psychiatrist for 1 month and then fortnightly sessions for another month before being referred back to the GP for further monitoring and management once every 1–2 months. We assume that cases not adherent with drug treatment accrue similar costs as those on non-evidence based treatments.
Drug costs are derived from the Health Insurance Commission for scripts filled under the Pharmaceutical Benefits Scheme (PBS) for the 1999/2000 financial year. The average dosage modelled for TCAs is 150 mg and for the group of SSRIs and related drugs 40 mg (fluoxetine, paroxetine or citalopram, mianserin), 150 mg (sertraline, venlafaxine), 200 mg (fluvoxamine) or 400 mg (nefazodone). The cost to the patient is averaged over general and concession patients and safety net and non-safety net patients. A summary of the monthly drug cost for SSRIs is calculated by weighting the cost for each drug by the proportion of prescriptions for each SSRI or TCA derived from the Bettering the Evaluation and Care of Health (BEACH) GP data collection system for the year 2000 [30].
For CBT, we cost 12 one-hour sessions for five scenarios: individual therapy sessions by a clinical psychologist or psychiatrist in public service or private practice as well as group therapy by a publicly funded psychologist. A GP visit for referral is included in all scenarios. Bibliotherapy is modelled as one long and two short visits to a GP and the purchase of a book (Table 2).
Summary of unit cost information, data sources and assumptions
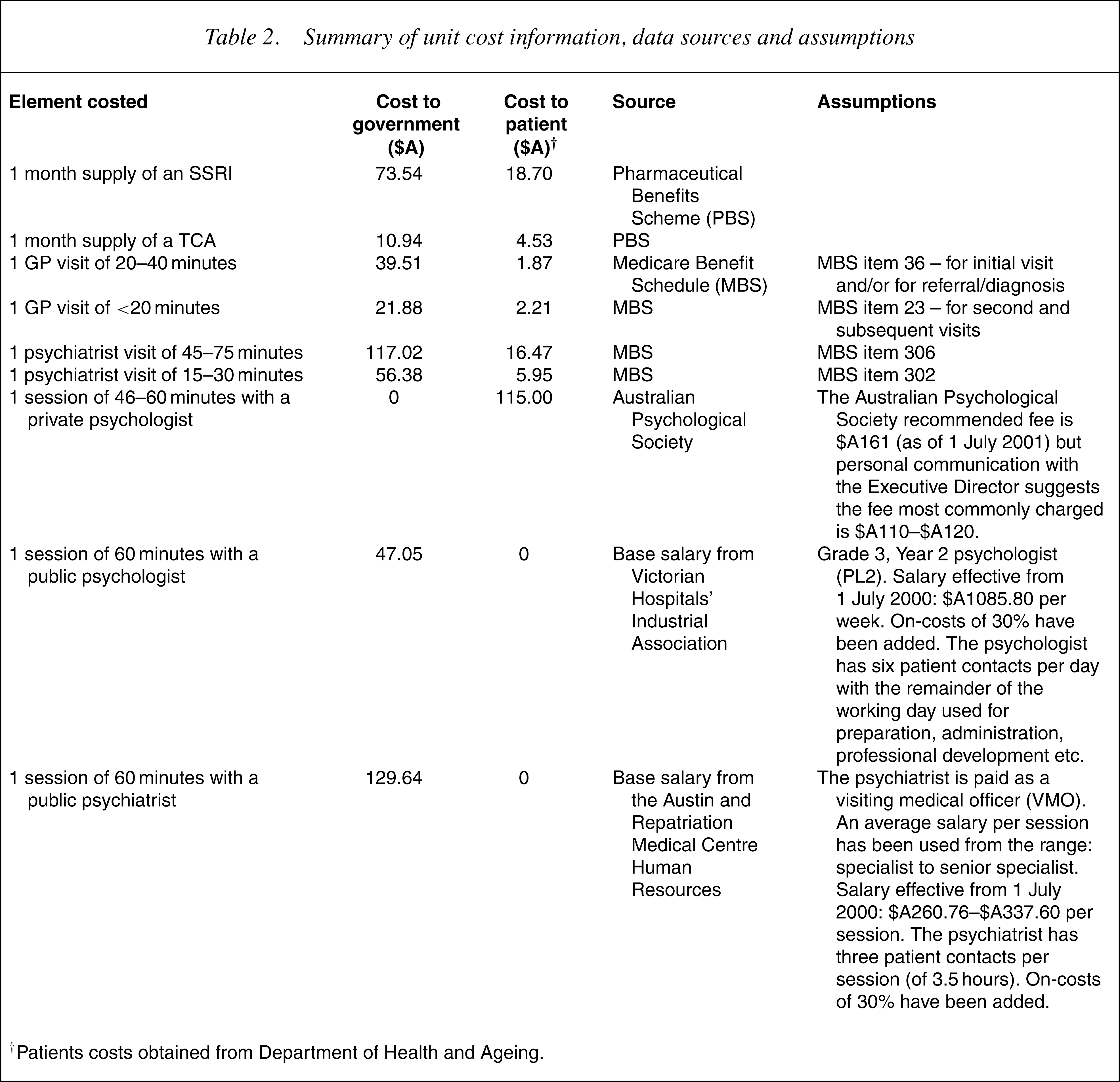
†Patients costs obtained from Department of Health and Ageing.
Depressed patients who receive non-evidence based treatment under current practice are costed for the mean number of visits to a GP (4.2), psychiatrist (0.3) and psychologist (2.2) as observed in SMHWB.
Uncertainty
In determining the benefits and costs associated with each intervention, we have assembled the best evidence available. However, there is uncertainty associated with all cost and outcome estimates. We use Monte Carlo simulation modelling and present uncertainty ranges as well as point estimates for benefits, costs and cost-effectiveness ratios that reflect all the main sources of uncertainty in the calculations.
Details of the parameters and distributions for the uncertainty assumptions used are shown in Table 1. The probability distributions around the input variables are based on: (i) standard errors quoted in, or calculated from, the literature; (ii) a range of parameter values quoted in, or calculated from, the literature; or (iii) expert advice. We use the @RISK software which is basically a macro allowing multiple recalculations on an Microsoft-Excel spreadsheet each time choosing a value from uncertainty distributions defined for input variables. We calculate 95% uncertainty ranges for our output variables (bounded by the 2.5th and 97.5th percentiles of the 4000 values generated). Results are presented to two significant digits only.
Results
All interventions for major depression examined have a favourable incremental cost-effectiveness ratio (ICER) under Australian health service conditions. Bibliotherapy, group CBT, individual CBT by a psychologist on a public salary and TCAs are very cost-effective treatment options falling below $A10 000 per DALY even when taking the upper limit of the uncertainty interval into account (Table 3).
Summary of point estimates and 95% uncertainty ranges of benefits, costs and incremental cost-effectiveness ratios (ICER) of interventions for major depression
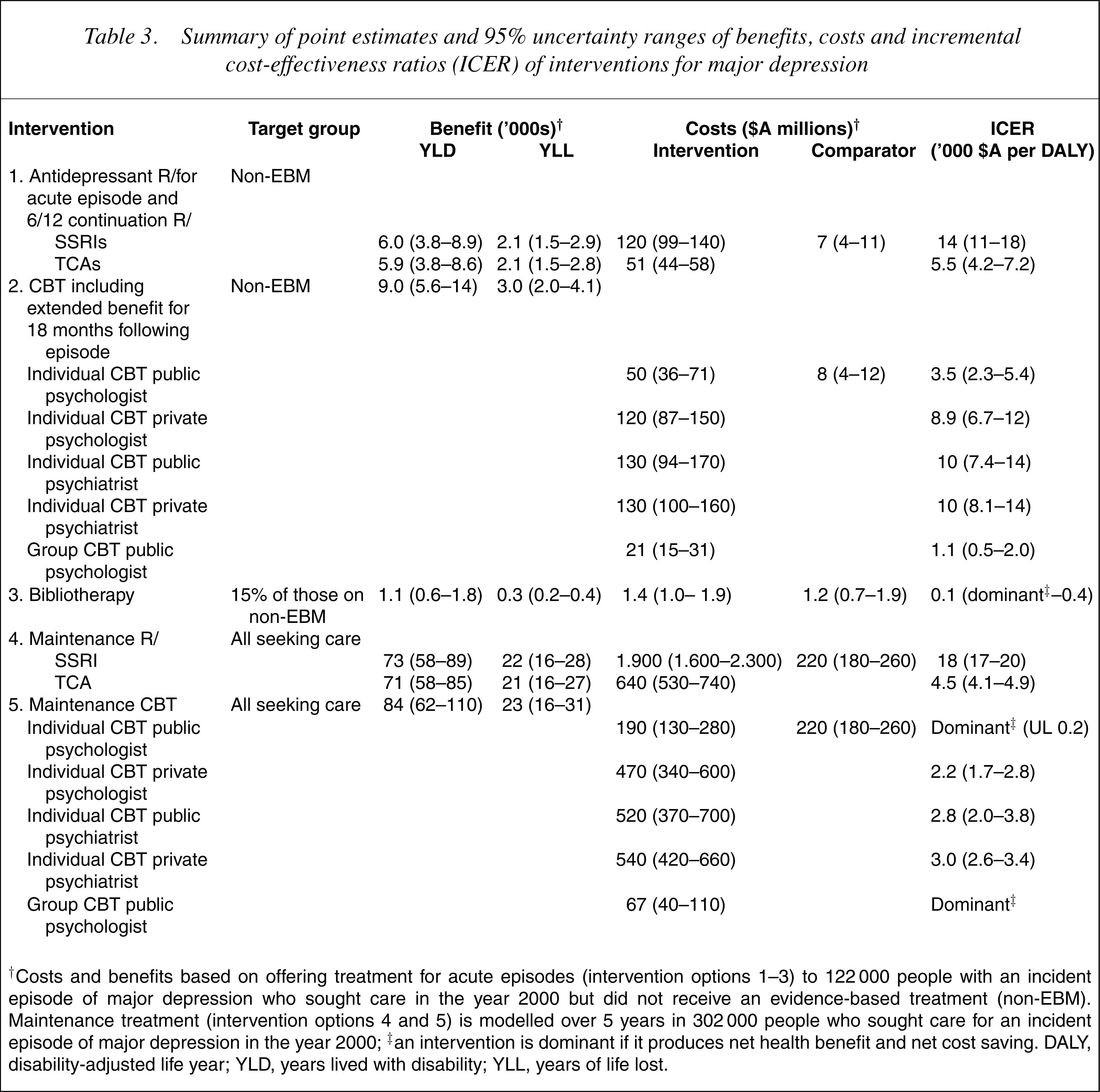
†Costs and benefits based on offering treatment for acute episodes (intervention options 1–3) to 122 000 people with an incident episode of major depression who sought care in the year 2000 but did not receive an evidence-based treatment (non-EBM). Maintenance treatment (intervention options 4 and 5) is modelled over 5 years in 302 000 people who sought care for an incident episode of major depression in the year 2000; ‡an intervention is dominant if it produces net health benefit and net cost saving. DALY, disability-adjusted life year; YLD, years lived with disability; YLL, years of life lost.
The ICER of maintenance treatment with CBT is very favourable as the costs per individual are relatively low in relation to considerable benefits. Maintenance and episodic treatment with TCAs have similar ICERs while maintenance treatment with SSRIs is less favourable (ranging from $A17 000 to $A20 000 per DALY) but still well belowthe threshold of $A50 000 we use in the ACE-MH studies as ‘affordable’.
Maintenance treatment strategies are associated with the largest amount of overall health gain. The total cost of treating all people with depression who present for care (taking an average 62% adherence into account) with 5 years of maintenance treatment with SSRIs is considerable: close to 2 billion $A. The costs are less than one-third of that if TCAs are used and CBT is again a cheaper option than drug interventions.
In a sensitivity analysis, we examine using a lower effect size for CBT (0.56 instead of 0.82), the pooled estimate of the impact of CBT trials for depression after exclusion of two outlier studies with very high effect sizes. This increases the ICER of CBT for acute episodes by 35% and by 6% for maintenance CBT. However, the overall conclusions remain the same: CBT is more cost-effective than drugs if provided by a publicly funded psychologist and particularly if done in groups; maintenance CBT is a very cost-effective option; CBT by private providers has a similar ICER as TCAs; and SSRIs are less cost-effective, but still affordable.
Second filter considerations are presented in Table 4. The evidence-base for both CBT and antidepressant drugs is sufficient although there are some concerns that almost all the evidence on CBT is in Anglo-Saxon populations and is delivered by psychologists. There are moderate concerns about equity, particularly if it would be largely available on a ‘user pays’ basis by private providers. Expanding access to CBT is challenging in terms of workforce and funding arrangements. The main issue with antidepressant drugs is that it is not very likely that many clinicians will go back to prescribing TCAs despite the fact that SSRIs give only marginal added benefits at much higher cost, and hence the less favourable ICERs.
Second-stage filter considerations for cognitive–behavioural therapy (CBT) and antidepressants
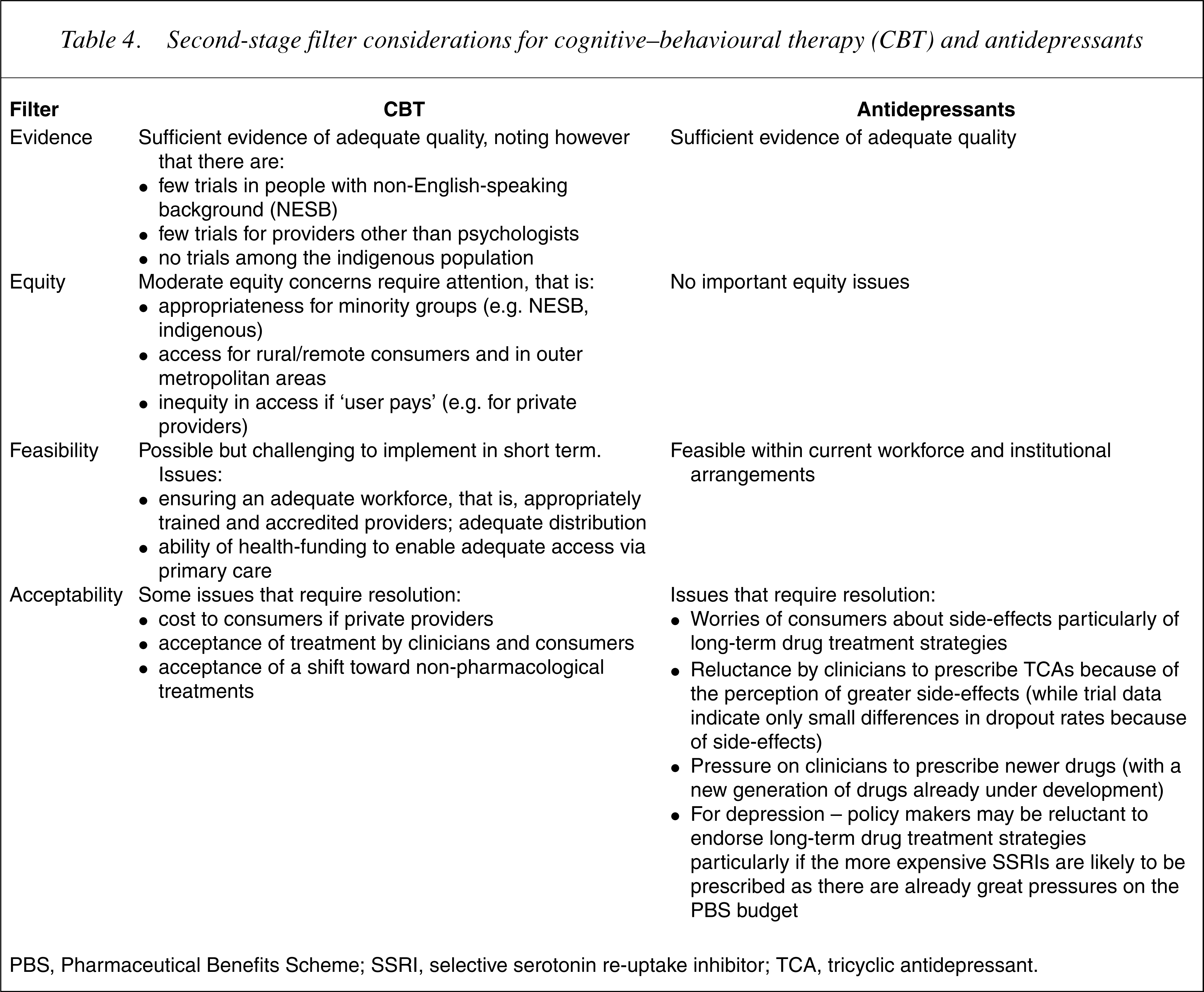
PBS, Pharmaceutical Benefits Scheme; SSRI, selective serotonin re-uptake inhibitor; TCA, tricyclic antidepressant.
Discussion
A range of cost-effective interventions for episodes of major depression exists. Bibliotherapy is the cheapest option with net cost savings if offered instead of ineffective treatment options. However, bibliotherapy may be a treatment option for only a small proportion of people with depression. Cognitive–behavioural therapy when delivered by psychologists on a ‘public’ salary is the next best option, followed by TCAs, CBT by private providers and SSRIs.
Maintenance treatment with CBT is a very favourable option but maintenance treatment with TCAs is also very cost-effective. However, the total cost for CBT would be much less than that for drugs. With a ICER costing approximately $A18 000, maintenance treatment with SSRIs is still a cost-effective option, but the overall cost over 5 years is considerable if maintenance treatment is offered to all cases of major depression currently seeking care. The annual cost of maintenance treatment would be higher still as we have not included incident cases in the years following our baseline year of 2000.
Our results strongly favour long-term treatment strategies for depression. As the vast majority of people with depression experience multiple episodes over a lifetime and are particularly prone to relapses shortly after an index episode, there are strong arguments to treat all depression as a chronic episodic disorder and not just those with three or more episodes as recommended in current treatment guidelines [3]. Unlike drugs, CBT conveys a longer-lasting impact beyond the time of treatment. It therefore seems advisable to make CBT available to all people experiencing depression rather than to resort to large numbers of people taking psychotropic drugs as first-line care over long periods. Cognitive–behavioural therapy using books should be strongly advocated for those willing and able to use it.
Key policy issues with regard to CBT concern the availability of suitably trained providers and the funding thereof. The bulk of the evidence on CBT is for psychologists as providers. Although there may be capacity to increase provision of CBT services above current levels, it is unlikely that there are enough trained psychologists to extend services to all those with major depression, let alone including those with anxiety disorders who would benefit from CBT as well [31]. There is no explicit evidence that other providers such as nurses and social workers can deliver CBT with similar effectiveness. However, the fact that bibliotherapy has similar effectiveness indicates that the type of provider may not be the most critical element of CBT. Alternative modes of delivery of computer-administered CBT (e.g. via the Internet or at GP practices) are currently being explored. Such methods would, in particular, facilitate access to CBT in rural and outer metropolitan areas where there are few therapists.
Funding is the other main policy issue. Current mental health services concentrate on treating the more severe and complex mental disorders. Large-scale provision of CBT for depression would mean a major change in the focus of these services. Expanding services in primary care in collaboration with GPs and community health centres is a more feasible option. However, the main challenge is how to fund it. A recent initiative by the Australian government to improve access to psychologists through GPs (as being piloted in the ‘Better outcomes in mental health care’ initiative) shows that funding mechanisms outside of Medicare are feasible.
More widespread implementation of CBT could potentially lead to cost offsets: (i) for the PBS because of a reduction in prescription of antidepressant drugs and (ii) for the health system in general because of a decrease in resource usage resulting from a reduction in relapse and severity of depression. These have not been considered in the analyses, but would only have made the findings more favourable toward CBT.
The cost-effectiveness analyses assume steady state operation, that is, assuming interventions are fully implemented and operate in accordance with its efficacy potential. In practice, resources will need to be allocated to implementation of the intervention, for example, in administering a new delivery system and in ensuring adequate training and accreditation of providers.
Based on cost-effectiveness, TCAs should be the drug of choice for depression unless not well tolerated. There is some worry about the toxicity of TCAs when taken in overdose, but there is insufficient evidence that prescribing TCAs leads to higher suicide rates [32]. Although the ICERs for giving SSRIs to those currently not treated are still within range of what is considered ‘affordable’ in Australia, a comparison of changing from TCAs to SSRIs has very high ICERs (exceeding $A250 000 per DALY). Reverting to widespread use of TCAs is unlikely to find favour with clinicians and patients despite these findings. However, the cost mainly to government through the PBS is very high because of the large number of people with depression who are eligible for treatment.
Although directly observed economic data on the cost-effectiveness of psychotherapies is limited and based on short-term follow-up [33], modelling the available evidence provides very strong support for CBT under Australian health service conditions. The generalizability of this finding to other industrialized countries is largely dependent on the cost of delivering the interventions, as there are similarities in the epidemiology of depression between countries.
Our finding that TCAs are more cost-effective than SSRIs is contrary to the conclusions of published drug-comparison studies. There are three reasons for this difference. First, we model no difference in impact between the drugs. In contrast, a study conducted by the non-profit Canadian Organisation for Health Technology Assessment [34] ‘borrowed’ utility weights from another study [35], giving greater utility while depressed on SSRIs than while depressed on TCAs, despite acknowledging the equivalence between the two drugs in reducing symptoms of depression. Second, we use modest differentials in adherence rates as consistently reported from meta-analyses. Finally, most drug-comparison studies estimate cost offsets from reduced health service use that compensate for the higher cost of SSRIs. We decided not to include a change in hospital costs for depression in our analyses. For the analyses of intervention strategies for acute episodes and a continuation phase this would make little difference as we model the changes in the group currently not receiving evidence-based care when consulting a health professional. In the 1997 survey, they reported an average number of 0.05 days in hospital which is so small that omission of these costs could not have a sizeable effect on the results. The average number of hospital days reported by all cases seeking any health care for their depression in the SMHWB is 1.9 days. This is our target group for maintenance treatments. However, we have no trial data to determine what proportion of hospital costs can be saved. Moreover, evidence from elsewhere may not apply to the health-care system we have in Australia. Therefore, we decide to ignore any impact on hospital costs. This may have led to some underestimation of the true cost savings associated with maintenance treatment.
Elsewhere, we discuss that translating trial findings into a health benefit in DALY terms is problematic [6]. Further developmental work is recommended such as the use of general quality of life outcome measures in trials and more sensitive disability weights in DALYs. Nevertheless, we argue that comparisons within depression are valid as the same imperfect methods are used to translate trial findings derived by similar means and the health benefit is largely driven by the effect size. Comparisons of these results with those for other mental or physical disorders are more affected by these methodological limitations.
Our estimates of the 20% average time with major depression over 5 years of follow-up is somewhat higher than reported from a clinical study in the US which found that 15% of time was spent with depressive symptoms at the level of major depression over 9 years of follow-up [36]. Using the lower estimate would increase the cost-effectiveness ratios for maintenance treatment options by 38% without altering the ranking order of interventions by their cost-effectiveness ratios.
Our ability to model depression as a chronic episodic disorder rather than episode by episode allows the evaluation of long-term treatment strategies. This is an important new development as we find such strategies to be cost-effective and potentially much more effective in curbing the burden of depression [5] even if we take ‘realistic’ adherence rates into account.
Caveat
The ACE-MH project was jointly funded by the Australian Department of Health and Ageing, Mental Health and Suicide Prevention Branch and the Department of Human Services, Mental Health Branch, Victoria in recognition of the importance of research into the cost-effectiveness of interventions in mental health treatment and care. This work draws upon, but is also limited by the available research and the assumptions necessary to complete the work.
The results of the analyses provide valuable material, likely to contribute to future policy deliberations by all service providers. Conclusions drawn from the economic evaluations should be considered within the context of the second-stage filter process, which qualifies the results taking into account issues of equity, feasibility, strength of evidence and acceptability to stakeholders. This second-stage filter process addresses some of the practical considerations required for changes in actual service practice.
Footnotes
Acknowledgements
The principal Investigators for the project are: Theo Vos, Rob Carter and Gavin Andrews. We thank members of the ACE –Mental Health Steering Committee for their input into the project: David Barton, Graham Burrows (Chair), Sue Caleo, Vaughan Carr, Dermot Casey, Joy Easton, William Hart, Helen Herrman, Barbara Hocking, Assen Jablensky, Anthony Jorm, Lyn Littlefield, Patrick McGorry, John McGrath, Paul Morgan, Lorna Payne, Deb Podbury, Kristy Sanderson, Suzy Saw, Bruce Singh, Bruce Tonge, Ruth Vine and Harvey Whiteford. The unit record data for the Survey of Mental Health and Wellbeing were obtained from Australian Bureau of Statistics (ABS) and a revised scoring algorithm to determine ICD-10 and DSM-IV diagnoses was provided by Gavin Andrews. Data on current prescribing behaviour by GPs was obtained from the Bettering the Evaluation and Care of Health data collection system run by the Australian Institute of Health and Welfare and the General Practice Statistics and Classification Unit of the University of Sydney. The average cost of various types of medical attendances and the various forms of SSRI and TCA were obtained from Medicare Benefits Schedule and Pharmaceutical Benefits Scheme data from the Department of Health and Ageing.