
Abstract
Recent national estimates indicate that 34.9% of Australians who have met the diagnostic criteria for an affective, anxiety, or substance-use disorder in the past 12 months had consulted a health professional for their mental health [1,2]. The remaining proportion of people in this population are typically considered ‘untreated prevalent cases’ [3]. There are many reasons why people with mental disorders may not use formal health services. These include system-related factors such as the unavailability of mental health services due to cost or geographic location [4–8], factors relating to service providers such as the identification and knowledge of psychological symptoms in primary care [9,10], and personal beliefs about mental illness and its treatment. This last category incorporates individuals’ perceived need for a service or treatment [3,11,12], self-recognition of psychological symptoms, and beliefs about the availability of treatments and their effectiveness [10,11,13,14]. Still, a substantial proportion of people identified as having mental health problems report no need for services or prefer to ‘manage themselves’ [15].
Self-management may be a viable option for many individuals with mental health problems, as either an alternative or accompaniment to formal health services [16]. Readily accessible and accurate information about mental health problems and their treatment is now available to the public in multiple media. For example, e-mental health programmes offer self-driven, Internet-based information and treatment for depression and anxiety, often at no cost to the individual. Randomized control trials of established e-mental health programmes have demonstrated immediate and long-term reductions in depressive and anxiety symptoms amongst consumers [17,18]. Similarly, involvement in support groups (on-line or in person) and telephone counselling services are perceived positively by the public [19,20] and are associated with improved mental health [21–24]. Mixed evidence exists for less structured forms of self-management for mental health problems, such as bibliotherapy [25] and increased physical exercise [26,27], however, these activities are more likely to be helpful than not. The act of self-managing mental health problems may also provide benefits to the individual through an enhanced sense of self-efficacy [16]. Finally, the anonymity, flexibility, and geographic accessibility offered by most self-management strategies [16,19,28,29] may increase their appeal to those with typically low levels of formal service use, such as young people [1,30], men [31], and people in rural or remote locations [32–34].
Two national surveys by Jorm and colleagues have shown that the majority of Australian adults consider telephone counselling and self-management strategies (including physical activity and talking to family) to be helpful for depression [10,14,35]. A survey of rural communities by Jorm and colleagues [19] found that a substantial proportion of individuals with mental health problems reported using self-management strategies. However, the level of use of self-management strategies for mental health problems in the general Australian population remains unknown. Given the effectiveness of some self-management strategies [36,37] and their potential appeal to people who do not use professional services [16], epidemiological information is needed to describe the proportion, number, and characteristics of people who use support services and self-management strategies. This information may also help to understand the lack of formal service use amongst many people with diagnosable mental disorders.
Australia's 2007 National Survey of Mental Health and Wellbeing (NSMHWB) is the first population-based survey to gather information about non-practitioner led support service use and self-management for mental health problems amongst Australian adults, together with the measurement of formal health service use. The present study provides estimates of the extent to which Australians use self-management strategies for their mental health over a 12-month period. We report on people with anxiety and affective disorders who use:
self-management strategies exclusive of formal health services,
formal health services exclusive of self-management strategies,
formal services and self-management strategies,
either formal services or self-management strategies, and thus,
the remaining proportion of people who receive no services, and do not use self-management strategies.
Finally, we examine whether support service use and self-management strategies are equally or disproportionately used by those groups who are known to receive few formal services including men, young adults, and people living in non-urban locations.
Materials and methods
Sampling and procedure
Details of the survey design and sample have been provided elsewhere [2,38]. Briefly, the 2007 NSMHWB survey methodology identified a stratified random sample of Australian households, and selected one person from each household using an algorithm developed by the Australian Bureau of Statistics to best approximate a representative sample of the Australian population. Following a response rate of 60%, 8841 individuals completed the survey. Interviews were conducted by highly trained interviewers in respondents’ homes, and took an average of 90 min to complete.
Survey instrument
The survey included the World Mental Health Composite International Diagnostic Instrument (WMH-CIDI), version 3.0. The WMH-CIDI collects detailed information about current and past mental health symptoms and related functioning to assess whether the respondent met criteria for an affective, anxiety, and/or substance use disorder in the past 30 days, 12 months, or at any point during their lifetime. Diagnoses according to DSM-IV-TR and ICD-10 criteria can be derived. Socio-demographic information was collected, as well as measures of suicidal behaviour, cognitive status, functioning and disability, physical health, quality of life, general psychological distress, social networks, caring for others, perceived need for mental health care, and a screening measure for psychosis. The 2007 NSMHWB included a module for health service use in Australia, focusing on respondents’ use of formal health services for mental health problems over the last twelve months. This module inquired about hospital admissions and consultations with general practitioners, psychiatrists, psychologists, mental health nurses and other specialist mental health providers, other health professionals, and complementary/alternative therapists.
The 2007 NSMHWB also sought information about a range of self-management strategies for mental health problems. Respondents were asked whether they had used Internet support groups or chat rooms, self-help groups (not online), or telephone counselling services for their mental health in the last twelve months. These non-practitioner led services are called ‘support services’ in the present study. Respondents were also asked whether they had used the following strategies to ‘help deal with your mental health problems’: increased their level of exercise or physical activity; done more of the things they enjoyed; sought support from family or friends; cut out alcohol or drugs, or used alcohol or drugs. These activities are referred to as ‘self-management strategies’ in the present study. With the exception of the last activity [25], these strategies have been shown to be potentially helpful for the management of mental health problems [21,22,24,36,37,39,40], or have no adverse effects (see alcohol avoidance [25]). Accordingly, ‘using alcohol or drugs’ to deal with mental health problems was not considered in composite measures of self-management strategies in the current study. Instead we considered potentially beneficial strategies only.
Data analysis
This study focused on 12-month rates of support service use and self-management strategies for mental health amongst respondents who met the 12-month ICD-10 criteria for affective (including: depression, dysthymia, bipolar affective disorder) and/or anxiety disorders (agoraphobia, social phobia, panic disorder, generalized anxiety disorder, obsessive–compulsive disorder, post-traumatic stress disorder). Collectively, these disorders are referred to as ‘common mental disorders’. Substance use disorders were not included because there is currently little evidence available for the effectiveness of support services and self-management strategies for these disorders. Analyses also examined support service use and self-management amongst respondents without a diagnosis. For comparative purposes, rates of support service use and self-management strategies are contrasted with figures for formal service use. Simple logistic regressions were performed to compare the odds of respondents in different age groups, genders, and geographic regions using support services and self-management strategies for their mental health. Data was weighted to reflect the Australian population by accounting for the probability of respondents’ selection into the survey. All standard errors were derived using the jackknife method of replication, utilizing the replicate weights provided in the 2007 NSMHWB dataset. Weighted estimates of population size were rounded to the nearest 100 (e.g., 1 884 891 is reported as 1 884 900).
Results
Use of support services and self-management strategies
Table 1 presents 12-month rates for respondents’ use of support services and self-management strategies, relative to formal support services. These rates are shown for members of the Australian population who did (column 2) and did not (column 3) meet the diagnostic criteria for a common mental disorder in the last 12 months. Of people with common mental disorders, 39%, or an estimated 1 059 800 Australian adults, used formal services for their mental health in a 12-month period. By comparison, a greater 52.9% of people with common mental disorders used support services and/or self-management strategies for their mental health problems in the same period. For support services, telephone counselling and (non-online) support groups were more commonly used than online support/chat groups. Of those self-management strategies that were considered in the 2007 NSMHWB, doing ‘more of the things you enjoy’ and seeking ‘support from family or friends’ were most common; approximately one third of people with a common mental disorder used these strategies to deal with their mental health problems in the last 12 months. As expected, rates of formal health service use, support services, and self-management strategies for mental health were consistently and substantially lower amongst people without a common mental disorder. People without common mental disorders used self-management strategies for their mental health at higher rates than formal health services. When all services and strategies were considered together, we found that 62.6% of people with a 12-month affective and/or anxiety disorder used some (potentially beneficial) formal service, support service, or self-management strategy for their mental health. This equates to 1 700 700 Australian adults. Whilst this rate was lower amongst people without a common mental disorder, one in five (or 2 726 800 adults) still reported that they had used at least one formal service, support service, or self-management strategy for their mental health in the past 12 months.
12-month prevalence rates (95%CIs) of formal service use, support services, and self-management techniques for mental health amongst people with and without 12-month affective and/or anxiety disorders
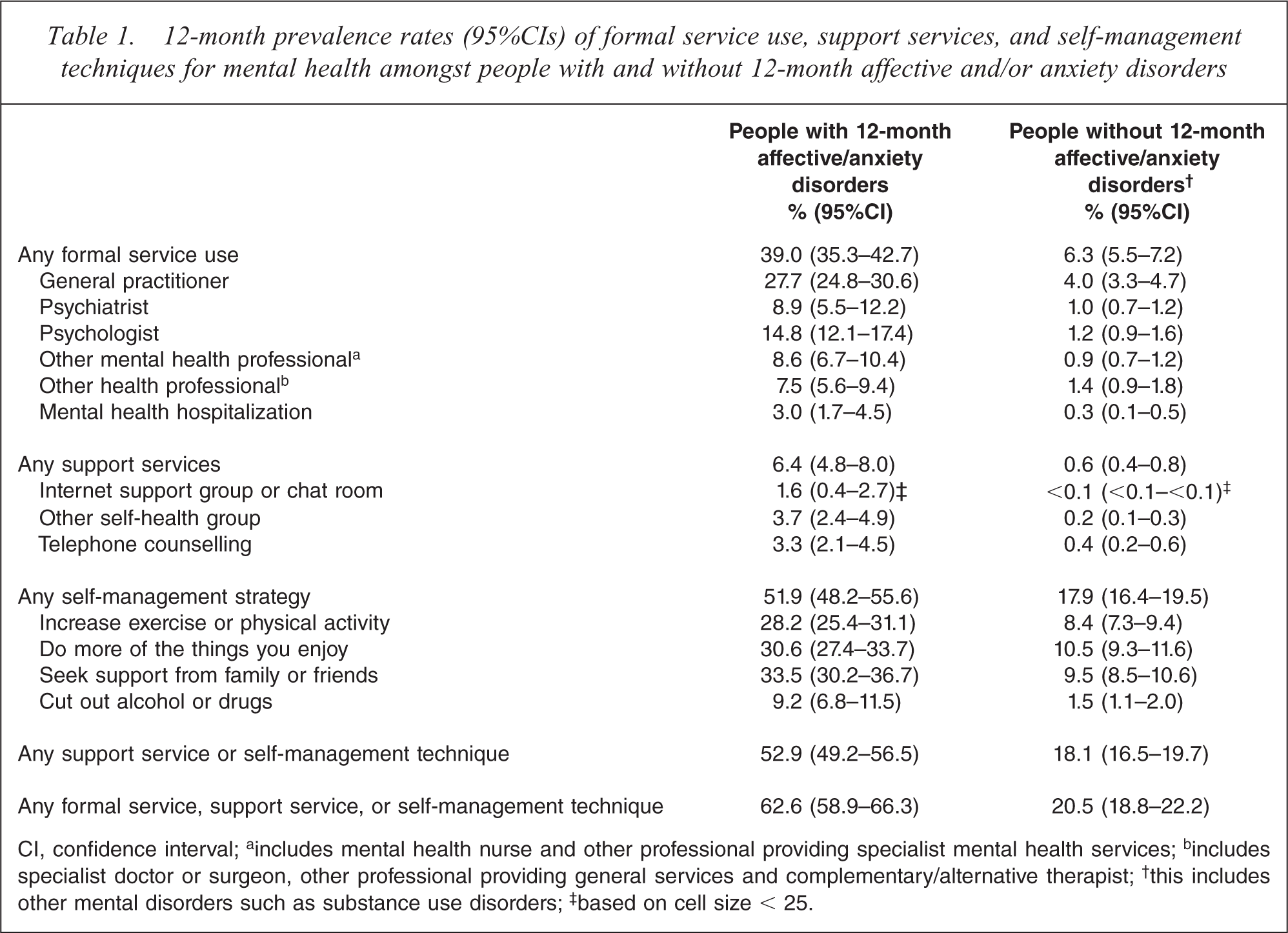
CI, confidence interval; a includes mental health nurse and other professional providing specialist mental health services; b includes specialist doctor or surgeon, other professional providing general services and complementary/alternative therapist; † this includes other mental disorders such as substance use disorders; ‡ based on cell size < 25.
Burgess et al. [1] have previously presented rates of formal service use in the total Australian population (i.e. including people with and without diagnoses for mental disorders), and consequently these are not presented here. In the total Australian population, 1.6% (95%CI: 1.2–1.9) of people used a support service for their mental health in the last 12 months; 31.3% (95%CI: 22.6–40.1) of these people did not meet the diagnostic criteria for a 12-month affective or anxiety disorder. Almost one quarter (23.7%; 95%CI: 22.2–25.2) of the total population used a self-management strategy for their mental health problems in the last year; 62.8% (95%CI: 59.9–65.8) did not have a common mental disorder. Finally, 27.6% (95%CI: 26.0–29.2) of the total population used any formal service, support service, or self-management strategy in the last 12 months; 61.6% (95%CI: 58.9–64.3) of whom were not identified with a common mental disorder.
We next considered whether people with common mental disorders who used support services and/or self-management strategies for their mental health did so in isolation or in conjunction with formal services. Of people with a 12-month common mental disorder, 24% (23.6%; 95%CI: 21.1–26.1) reported that they had used support services and/or self-management strategies without formal services for their mental health in the last year. A lower 9.7% (95%CI: 7.6–11.8) used formal services without support services and/or self-management strategies, and 29.3% (95%CI: 25.7–32.9) reported that they had used a formal health service plus support services or self-management strategies for their mental health in the last year. Thus, 37.4% (95%CI: 33.7–41.1) of people with a common mental disorder reported no use of formal services, support services or self-management strategies for their mental health problems. Considered another way, the current results showed that 55.4% (95%CI: 50.7–60.0) of people with a 12-month common mental disorder who used support services or self-management strategies also used formal health services in the same period, and thus, 44.6% did not. The most commonly used health service amongst people with a common mental disorder who also undertook support services or self-management strategies were GPs (41.1%; 95%CI: 36.5–45.7), followed by psychologists (22.3%; 95%CI: 17.8–26.9). These rates of formal service use were higher than those amongst people with common mental disorders who did not use support services or self-management strategies (GP use: 12.7%, 95%CI: 9.9–15.6; psychologist use: 6.3%, 95%CI: 4.3–8.2).
Table 2 presents 12-month rates of formal service use, support services, and self-management strategies for mental health amongst people with 12-month common mental disorders according to the key demographic factors of age, gender, and urbanicity. These analyses were performed to investigate whether support services and self-management strategies are disproportionately used by subpopulations known to use few formal services (e.g. men, young adults, and people living in non-urban locations). People with 12-month common mental disorders aged 44–64 years (OR: 1.5; 95%CI: 1.0–2.2) were more likely to use formal health services than young adults aged 16–24 years. This difference was not apparent for support services and/or self-management strategies. People in the oldest age group were less likely to use these non-practitioner led activities than the youngest group (OR: 0.36; 95%CI: 0.2–0.6). Women were more likely to use all services and self-management strategies than men with the exception of support services, though this non-significant result may reflect the small numbers of respondents in these categories. People with common mental disorders who lived in non-urban locations used fewer formal services, support services, and self-management strategies than those in urban areas, however, the odds of using these services or strategies did not differ significantly across these categories.
12-month rates (95%CIs) of formal service use, support services, and self-management strategies for mental health amongst people with 12-month affective and/or anxiety disorders, as function age, gender and urbanicity
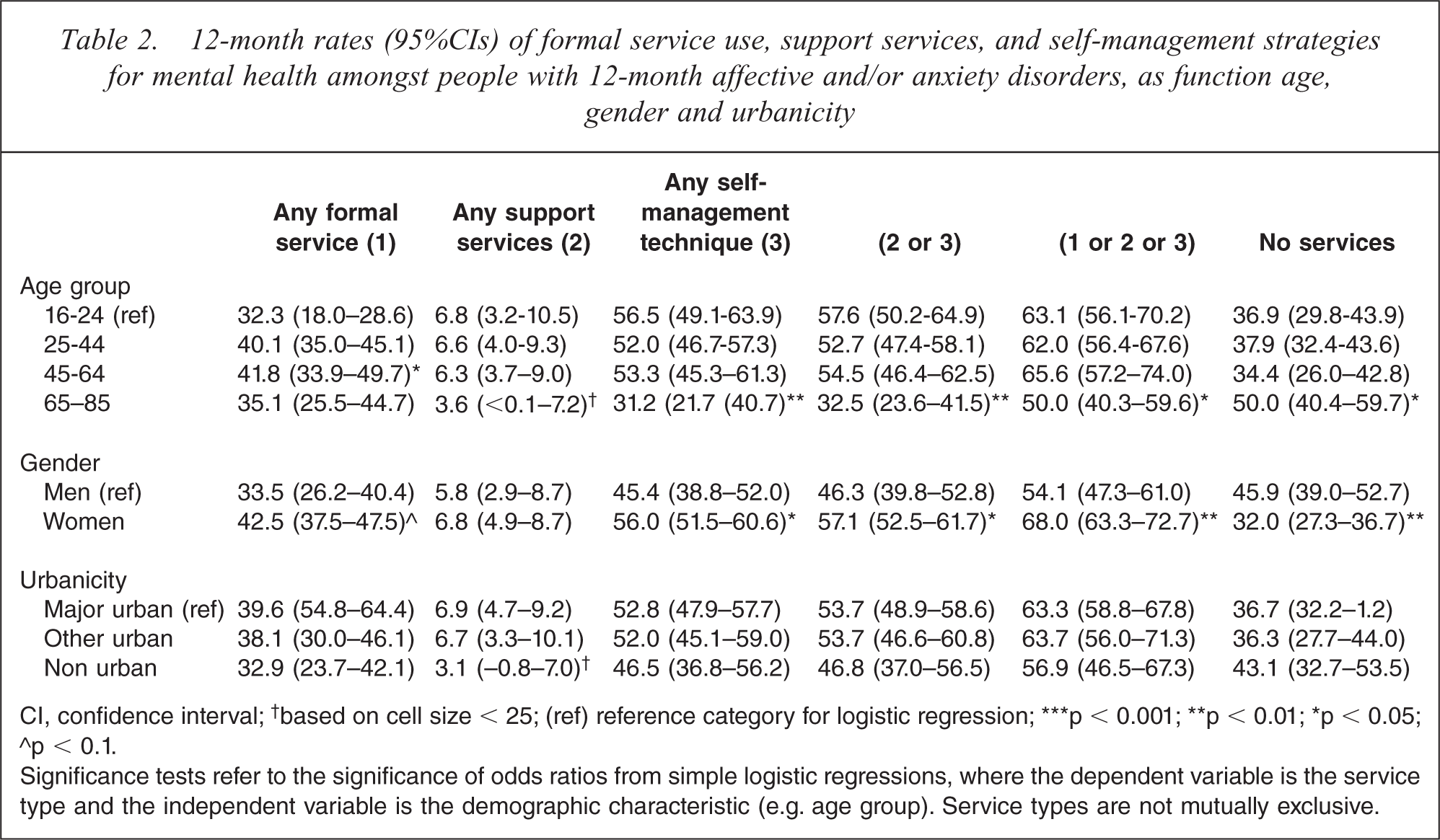
CI, confidence interval; † based on cell size < 25; (ref) reference category for logistic regression; ∗∗∗p < 0.001; ∗∗p < 0.01; ∗p < 0.05; ∘p < 0.1.
Significance tests refer to the significance of odds ratios from simple logistic regressions, where the dependent variable is the service type and the independent variable is the demographic characteristic (e.g. age group). Service types are not mutually exclusive.
Discussion
Summary of findings
Self-management strategies for mental health are widely used amongst Australian adults; more so than formal health services. Over half of the population with a current or recent common mental disorder reported using support services and/or self-management strategies for their mental health problems in the past year. This exceeds the 39% of people with 12-month common mental disorders who used formal health services, such as GPs, psychologists, and psychiatrists. Overall, we found that 62.6% of Australian adults who met the criteria for an affective and/or anxiety disorder in the last 12 months had sought to address their mental health problems via professional services, support, or lifestyle changes.
Preliminary investigations indicated that the demographic profile of people who used self-management strategies for mental health problems differed somewhat from that of formal service users. Whilst 49% of young adults aged 16–25 years with a 12-month diagnosis for mental disorder had used support services or self-management strategies for their mental health in the past year, less than half this percentage (23.3%) used formal services. The analogous gap between use of support services or self-management strategies and formal services amongst people aged 45–64 years was smaller (53.6% versus 40.5%). Further, whilst women used all services and strategies at higher rates than men, this gender-related discrepancy was smaller for forms of self-management (56.3% of women versus 42.2% of men) compared to formal service use (40.6% of women versus 27.6% of men).
Comparisons with other studies
In national surveys of mental health literacy, Jorm and colleagues [14,35] presented participants with vignettes of a person with depression and asked them to rate the helpfulness and harmfulness of several health professionals, treatments, services, and activities. Over half of Australian adults considered telephone counselling to be helpful for depression. Even more rated self-management strategies, including physical activity and talking to family or friends, as helpful. In a community sample of rural Australians who themselves had screened positive for a common mental disorder, Jorm and colleagues [19] found that 55% of participants reported that they had become more physically active in the last six months to ‘to cope with stress, anxiety, depression or other emotional problem’. Also, 50% and 46% reported that they had sought help from close friends or family, respectively, 12% had cut out alcohol, and 3% had sought telephone counselling. Thus, there is widespread support in the community for responses to mental health problems which involve lifestyle change, support and self-management. Further, as was evident in the present study, Jorm and colleagues found that self-management strategies were used more frequently than formal health services such as psychologists and psychiatrists. Rates for alcohol reduction and telephone counselling in Jorm et al.'s latter study are comparable to the present national results for people with 12-month common mental disorders. While the rate of help-seeking from friends and family was higher in Jorm et al. [19] than the current study, this may reflect methodological and demographic differences between the studies. Jorm et al.'s data were drawn from a follow-up study which had initially assessed respondent's views of services and strategies that may be helpful for mental health problems. Participation in this initial survey may have educated respondents about possible self-management strategies and increased their propensity to subsequently use these strategies [41].
To the authors’ knowledge, national rates of support service use and self-management for mental health problems have not been available for the Australian population prior to the inclusion of these questions in the 2007 NSMHWB. There are, however, a small number of relevant international results. Using cross-national data from the World Mental Health Surveys project, Wang et al. [42] found that people's use of ‘complementary and alternative’ treatments for mental health over a 12-month period ranged from 0.1% (Italy) to 2.8% (USA). In these surveys, ‘complementary and alternative’ therapies incorporated consultations with alternative therapists (e.g. chiropractors) and participation in Internet and non-online support groups. Data from Te Rau Hinengaro (The New Zealand Mental Health Survey), showed that 6.9% of New Zealand adults with a mental disorder used this category of services [43]. The definition of ‘complementary and alternative’ therapies used in these studies differs from the focus of our study. However, we are able to construct a similar grouping using data from the 2007 NSMHWB and find that 6.4% (95%CI: 5.1–7.8) of Australians with any 12-month ICD-10 mental disorder, or 1.9% (95%CI: 1.5–2.2) of the total population, have used ‘complementary and alternative’ therapies. The current Australian findings are, therefore, consistent with available international research.
Self-management of mental health problems: an alternative for some?
The present study found that over half of those people with a 12-month common mental disorder who used support services or self-management strategies for their mental health also used formal services. For these individuals, involvement in support groups, on-line or otherwise, and the use of self-management strategies may be at the suggestion of a health professional, to supplement practitioner-led treatment, or maintain the effects of such treatment following its conclusion. This is supported by the higher rates of formal service use amongst people who participate in support services and self-management strategies, relative to those who do not. This still leaves a substantial proportion of people using self-management strategies for common mental disorders without professional guidance, an estimated 796 000 people in a 12-month period. Are these individuals receiving appropriate care for their mental health problems? Several of the support services and self-management strategies assessed in the 2007 NSMHWB have demonstrated some level of effectiveness for the amelioration of psychological symptoms [21,22,24,36,37,39]. This is particularly true for people with milder disorders [16]. It may be predominantly people in these circumstances who are using self-management strategies. We found, for example, that the majority of people (62.8%) who reported undertaking self-management strategies for their mental health problems did not meet criteria for an affective or anxiety disorder in the last 12 months. This group will, however, include people with subclinical symptoms as well as people with previous diagnoses who may now be managing remitting symptoms or the recurrence of symptoms [3]. Thus, it is possible that the use of these support services and self-management strategies without formal services may adequately meet the needs of some who have a level of mental health literacy (i.e. knowledge of the strategies may be helpful and adequate for mild disorders).
It is also possible that self-management alone does not represent adequate treatment for many people. For these people, the absence of formal service use may reflect the presence of a barrier to appropriate treatment. This may include system-related factors or personal barriers, such as stigma and perceptions of the effectiveness or availability of formal mental health services [16,19,29]. Our preliminary exploration of formal service use compared to self-management in demographic groups that traditionally receive few formal services (e.g. young adults and men) suggests that the former may play a role. For example, while formal service use was lower among young adults than middle-aged adults, the use of self-management strategies was approximately equal across these two groups. Low formal service use amongst young adults has been attributed to a lack of specialized services for young people [44–46]. This system-related barrier is not evident for self-management strategies. Established gender differences in formal service use were, however, evident for support services and self-management strategies.
Implications and future research
A better understanding of the reasons that individuals use support services and self-management strategies for their mental health in addition, or at the exclusion, of formal services is required. This will help to determine whether these activities are a viable alternative to formal treatment for some people, and/or reflect current service inadequacies. Such information could inform mental health policy, including service delivery and funding, and the promotion of support services and self-management amongst people who may prefer and benefit from these alternatives. Further epidemiological research is required to identify the sociodemographic and diagnostic characteristics of people who use support services and self-management strategies. This will begin to answer questions about whether self-management is preferred by certain members of the population. The association between self-management of mental health problems and perceived need for formal services is also worthy of further investigation. Meadows and colleagues [3,11,12] have shown that a substantial proportion of people with mental disorders who do not use formal services do not perceive that they have any need for such services or prefer to ‘manage themselves’ [see also 15]. It may be that the lack of perceived need for formal services reflects (in part) current self-management.
Study limitations
The shortcomings of the 2007 NSMHWB survey design and sample have previously been discussed in detail [1,2]. With respect to the current study, it is likely that we have underestimated the proportion of people in the Australian population who used self-management strategies. This is because the list of support services and self-management strategies provided to respondents was not exhaustive and questions were not open-ended. For example, structured Internet-based programmes for mental health which have demonstrated popularity and efficacy [17] were not assessed. Secondly, methodological limitations may have influenced our analysis of urban- and non-urban effects. While formal service use is known to be lower in rural and remote communities [32–34], the measure of urbanicity available in the survey is not an adequate measure of geographic remoteness, which is the level at which the largest discrepancies in formal service use are observed [47]. Thirdly, we acknowledge that any discussion about the prevalence of service use, and lack of use, amongst people who have met criteria for a mental disorder is dependent upon the validity of the instruments used to measure these constructs [48]. Jorm [49] points out that diagnostic instruments administered by lay interviewers in epidemiological surveys have shown less-than-optimal agreement with clinical judgements and have the potential to misdiagnose non-cases of mental disorder. Individuals’ recollection of service use may also be inaccurate [50]. Accordingly, the proportion of ‘unmet need’ in population surveys (typically defined as people with mental disorders who are not receiving treatment), and use of support services and self-management strategies amongst those without disorders may be overestimated.
Summary and conclusions
This study is the first to provide national estimates of the use of non-practitioner led support services and self-management strategies for mental health problems in Australia. Although only 39% of Australian adults who met the criteria for a common mental disorder in the last 12 months had used formal mental health services, we found that a further 24% had used support services and self-management strategies without these services. Together, these estimates provide a more comprehensive picture of the proportion and number of Australians who participate in activities with the goal of improving their mental health. Further research is needed to determine whether the self-management may be an appropriate alternative or adjunct to formal health services.