
Abstract
Objective:
To identify the proportion of children and adolescents in Australia and the proportion of those with mental disorders who used services for emotional and behavioural problems, the type of services used and what characteristics were associated with service use.
Method:
During 2013–2014, a national face-to-face household survey of mental health and wellbeing (Young Minds Matter) was conducted, involving 6310 parents and carers of 4- to 17-year-olds (55% of eligible households) and self-report surveys from 2967 11- to 17-year-olds in these households (89% of eligible youth). The survey identified 12-month mental disorders based on the Diagnostic Interview Schedule for Children–Version IV and asked about service use for emotional or behavioural problems in the previous 12 months.
Results:
Overall, 17.0% of all 4- to 17-year-olds used services for emotional or behavioural problems in the previous 12 months. Of those with mental disorders, 56.0% used services (48.9% of 4- to 11-year-olds; 65.1% of 12- to 17-year-olds). Service use was highest among 4- to 17-year-olds with major depressive disorder (79.6%) and lowest for those with attention-deficit/hyperactivity disorder (52.7%). Two-fifths (41.2%), 72.5% and 87.6% of those with mild, moderate and severe disorders used services. General practitioners, psychologists, paediatricians and counsellors/family therapists were the most commonly accessed health service providers. Two-fifths with mental disorders had attended school services. About 5% of adolescents reported use of online personal support or counselling for help with their problems. From multivariate models, service use was higher in sole carer families, but also among those living in the least socially and economically disadvantaged compared to the most disadvantaged areas.
Conclusion:
Rates of service use for mental disorders in Australia’s children and adolescents appear to have increased substantially. Health services and schools are the major providers of services for emotional and behavioural problems, but telephone counselling and online services have become well-established parts of the service environment.
Introduction
Mental health problems in childhood and adolescence are a major public health problem and if left untreated or inadequately treated may continue into adult life (Kessler et al., 2005; Slade et al., 2009). International and national strategies identify prevention and early intervention as critical (Commonwealth of Australia, 2009; World Health Organization, 2013). In 1998, Australia conducted the first national survey of the mental health of children and adolescents and found that just under one-third of 6- to 17-year-olds with mental disorders had used any service for their problems in the 6 months prior to the survey (Sawyer et al., 2000). This paper provides up-to-date estimates of service use for emotional and behavioural problems in Australia from the 2013–2014 second Australian Child and Adolescent Survey of Mental Health and Wellbeing (Young Minds Matter).
The previous findings provided evidence to support large-scale government investment in a range of initiatives aimed at increasing access to mental health services for young people. One major initiative was the Better Access programme introduced in November 2006, which provides rebates via the Medicare Benefits Schedule for mental health consultations with general practitioners (GPs), psychologists and other allied health services. Between 2006–2007 and 2011–2012, there was a threefold increase in the number of children and adolescents receiving Medicare-funded mental health services (0.7–3.6% of 5- to 11-year-olds; 1.1–5.5% of 12- to 17-year-olds) (Department of Health and Ageing, 2013). There has also been a significant investment in mental health promotion and preventative programmes in schools. In 2011, a national survey found that 60% of Australian schools (52% of primary and 73% of secondary schools) were providing mental health programmes (Department of Health and Ageing, 2013: 82). Furthermore, the last decade has seen the introduction of community-based headspace centres providing a variety of multidisciplinary health, drug and alcohol, and other non-health support services for 12- to 25-year-olds (McGorry et al., 2007; Rickwood et al., 2014).
An important and relatively new platform for the delivery of mental health services to young people is the internet and online environment (Burns and Birrell, 2014; Burns et al., 2010). It is an environment in which young people are comfortable interacting, developing relationships, discussing sensitive issues such as their mental health and seeking help and information in a confidential way (Burns and Birrell 2014; Ivancic et al., 2014). Online services such as those provided by reachout (2015), youthbeyondblue (2015) and eheadspace (2015) provide information about mental health issues, online assessment tools, personal counselling, chat rooms and support groups.
These changes in mental health service delivery for young people have produced signs of increased access. However, due to the fragmented way in which data about mental health service use are collected, it is not possible to gain a complete picture across all services without using a representative random sample from the community. This paper provides an opportunity to provide a more comprehensive overview of service use by young people with mental disorders. A key advantage of these data is the reports by adolescents themselves of their use of services from telephone and online providers. Specifically, this paper reports how many 4- to 17-year-olds overall and how many of those with mental disorders used services for emotional and behavioural problems in the previous 12 months and describes the characteristics of those with mental disorders who are using services. For those with mental disorders, the paper also contrasts parent and carer reports of service use with reports by 13- to 17-year-olds themselves.
Methods
Population
Young Minds Matter was conducted during 2013–2014 by the Telethon Kids Institute, The University of Western Australia, in partnership with Roy Morgan Research and was funded by the Australian Government Department of Health. In total, 6310 parents and carers across Australia participated in the survey (55% of eligible households). Self-report questionnaires were completed by 2967 11- to 17-year-olds in these households (89% of eligible youth). The survey was designed to generate data that are representative of children aged 4- to 17-years in Australia referencing the 2011 Census of Population and Housing. The most remote areas were excluded from the sampling frame, as were children who were homeless or in institutional care and children in families where the interview could not be conducted in English. When compared with data from the Census on major demographic characteristics, the sample was found to be broadly representative of the population with two exceptions. It over-represented younger children aged 4–7 years and families with more than one eligible child. Survey methodology has been described in detail elsewhere in this issue (Hafekost et al., submitted).
Participation in the survey was voluntary, and all participants gave written consent to participate in the survey. The research protocol for the study was approved by the Australian Government Department of Health Human Research Ethics Committee and The University of Western Australia Human Research Ethics Committee.
Variables
Mental disorders
Mental disorders were assessed using the Diagnostic Interview Schedule for Children–Version IV (DISC-IV) (Fisher et al., 1993). The DISC-IV implements the criteria for mental disorders set out in the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV; American Psychiatric Association, 2000). Seven DISC-IV modules were completed by parents and carers in relation to their children’s symptoms and the impact of these over the previous 12 months: anxiety disorders (social phobia, separation anxiety disorder, generalised anxiety disorder, obsessive–compulsive disorder); major depressive disorder; attention-deficit/hyperactivity disorder (ADHD); and conduct disorder. The choice of DISC-IV modules to include in the survey was based on the intention to identify the most common mental disorders in childhood and adolescence together with considerations of limiting respondent burden. While having major impact on individuals and families, severe disorders such as schizophrenia were not covered by the survey due to low prevalence in this age group. However, a set of questions screening for psychotic-like behaviours was included. The experience of adults (aged 18–64 years) living with psychotic disorders and utilising public mental health services is the subject of another component of the Australian national surveys of mental health and wellbeing (Morgan et al., 2011). A measure of disorder severity was developed by the survey team and has been described elsewhere in a detailed technical report (Zubrick et al., 2015).
Additionally, young people completed the DISC-IV major depressive disorder module. For the purposes of reporting some results on service use by adolescents in this paper, a combined measure of disorder status (i.e. had a disorder identified by parent/carer report or major depressive disorder identified by adolescent report on the DISC-IV) was created for 13- to 17-year-olds, the sub-group who also self-reported on their service use.
Other indicators of mental health problems or distress
Other questions in the survey were used to indicate the presence of mental health problems or distress that, while not meeting full diagnostic criteria, may be of clinical significance or of concern to parents and carers or children and adolescents. These were as follows: (a) a sub-threshold level of mental disorder on one or more of the DISC-IV diagnostic modules, in which symptoms are present but not at a level of severity and/or for a sufficient duration to meet diagnostic criteria. For this analysis, the sub-threshold level was set at half or more of the required number of symptoms to meet full diagnostic criteria (e.g. DSM-IV criteria for major depressive disorder require the presence of six or more symptoms, and the sub-threshold level was set at three or more symptoms); (b) a score in the ‘abnormal’ range on the Strengths and Difficulties Questionnaire (SDQ; Goodman, 1994); (c) a ‘very high’ level of psychological distress on the Kessler 10 Psychological Distress Scale (Kessler et al., 2003); and (d) having ever attempted suicide as reported by 12- to 17-year-olds.
Service use questions
Parents and carers responded to an extensive set of questions about service use for emotional or behavioural problems in the previous 12 months. To examine overall patterns of service use, a composite measure was created. ‘Services’ comprise the following: (a) health services – any service provided by a qualified health professional, regardless of where that service was provided; (b) school services – any service provided by the school or other educational institution; (c) telephone counselling services; and (d) online services that provided personalised assessment, support, counselling or structured self-help programmes. Self-report information of service use was restricted to 13- to 17-year-olds (n = 2314) who were asked a similar set of questions, but also provided more detailed information about their use of online and headspace services.
Sociodemographics
Family type, household income, highest level of parent/carer education and labour force status were collected, using the Australian Bureau of Statistics standard formats. Area-level socioeconomic status was taken from the 2011 ABS Index of Relative Socio-Economic Disadvantage (IRSED) for Statistical Area 1 (SA1) in which the family was living at the time of the survey (Australian Bureau of Statistics, 2013). Remoteness areas were assigned based on SA1 of residence at the time of the survey.
Analysis
The analysis in this paper uses the whole sample and several sub-samples as follows:
When assessing service use in the child and adolescent population (all 4- to 17-year-olds) based on parent/carer report, the whole sample is used (n = 6310).
When assessing service use based on adolescent self-report, the sample is restricted to 13- to 17-year-old adolescents, all of whom who answered questions about service use (n = 2314).
When examining service use by children and adolescents with mental disorders identified from parent/carer reports on the DISC-IV, the analysis was undertaken on the 860 4- to 17-year-olds who had a mental disorder.
When reporting service use by adolescents with mental disorders, the analysis was based on those young people with mental disorders identified by either their parents/carers or own reports on the DISC-IV where information was available from both informants (n = 481).
All the results have been weighted to represent 4- to 17-year-olds in the Australian population. The weighting accounted for patterns of non-response, specifically the over-representation of younger children and families with more than one child aged 4–17 years, as well as the oversampling component of 16- to 17-year-olds. Survey estimates of service use and associated confidence intervals have been calculated using the method of Taylor Series Linearisation (Wolter, 2007). The p value associated with significant differences in proportions using services has been reported in the text.
Sociodemographic predictors of service use among young people with disorders were assessed with multiple logistic regression methods using the SAS SURVEYLOGISTIC procedure to account for the clustered nature of the sample design and use of survey weights. Predictors of health and school service use were analysed separately as health service use may be more influenced by family decisions, whereas school service use may depend more on availability and influence of school staff. Only the results for sociodemographic predictors have been shown. The association between disorder type and severity has been presented using descriptive statistics. All analyses were undertaken using SAS Version 9.4 (SAS Institute Inc., 2014).
Results
Overall, 13.9% of children and adolescents were found to have a mental disorder in the past 12 months. Of those children and adolescents with 12-month mental disorders, 59.8% of cases were mild, 25.4% were moderate and 14.7% were severe (Lawrence et al., 2015a).
Parent-/carer-reported service use by all 4- to 17-year-olds
Overall, 17% of all 4- to 17-year-olds used services for emotional or behavioural problems in the previous 12 months. Half (50.4%) of these were assessed on the basis of information provided by their parents and carers, or themselves in the case of adolescents, as having a mental disorder according to DSM-IV diagnostic criteria (Table 1). Another two-fifths (40.0%) had symptoms of a mental disorder based on other indicators of mental health problems or distress. Around one in 10 (9.7%) children and adolescents who had used a service did not appear to have significant mental health problems or distress based on any indicators captured in the survey.
Service use in past 12 months among 4- to 17-year-olds by indicators of significant problems.
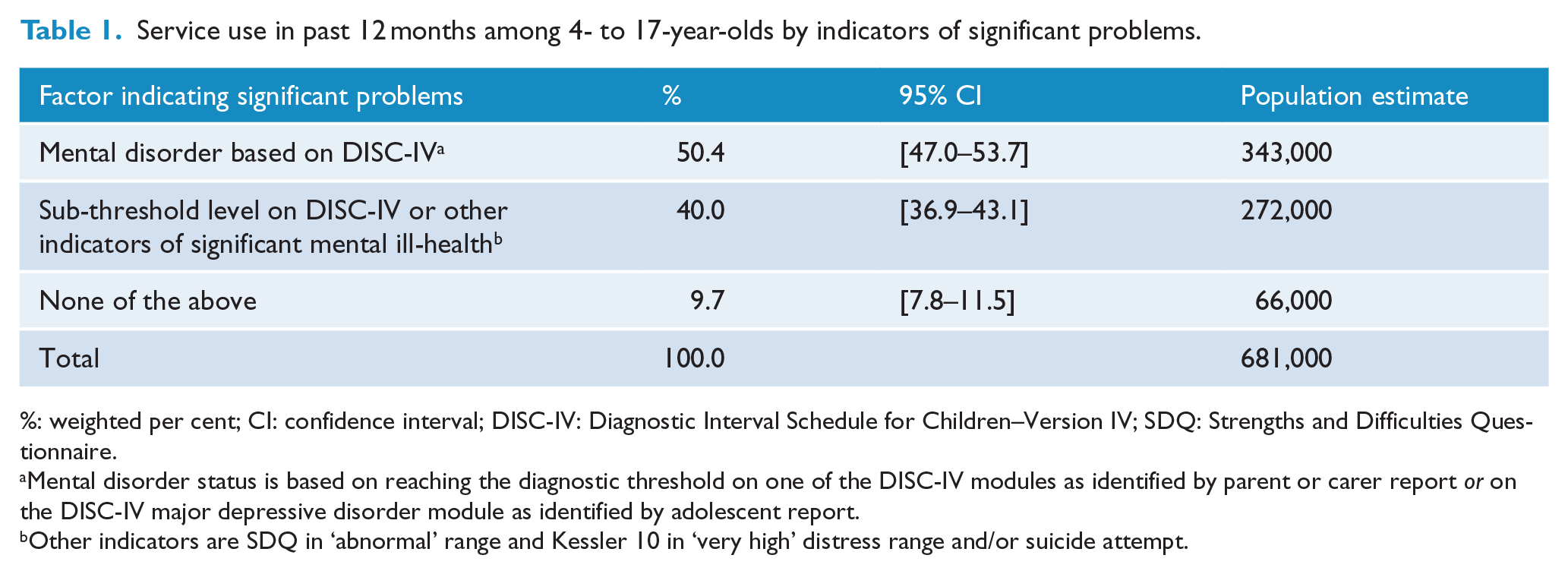
%: weighted per cent; CI: confidence interval; DISC-IV: Diagnostic Interval Schedule for Children–Version IV; SDQ: Strengths and Difficulties Questionnaire.
Mental disorder status is based on reaching the diagnostic threshold on one of the DISC-IV modules as identified by parent or carer report or on the DISC-IV major depressive disorder module as identified by adolescent report.
Other indicators are SDQ in ‘abnormal’ range and Kessler 10 in ‘very high’ distress range and/or suicide attempt.
Parent-/carer-reported service use by disorder type and service sector among all 4- to 17-year-olds
More than half of 4- to 17-year-olds with mental disorders (56.0%) had used services for emotional or behavioural problems in the previous 12 months, as had one-tenth of those without a mental disorder (10.6%; see Table 2).
Parent-/carer-reported service use for emotional or behavioural problems in past 12 months among all 4- to 17-year-olds by disorder type, disorder status and type of service.
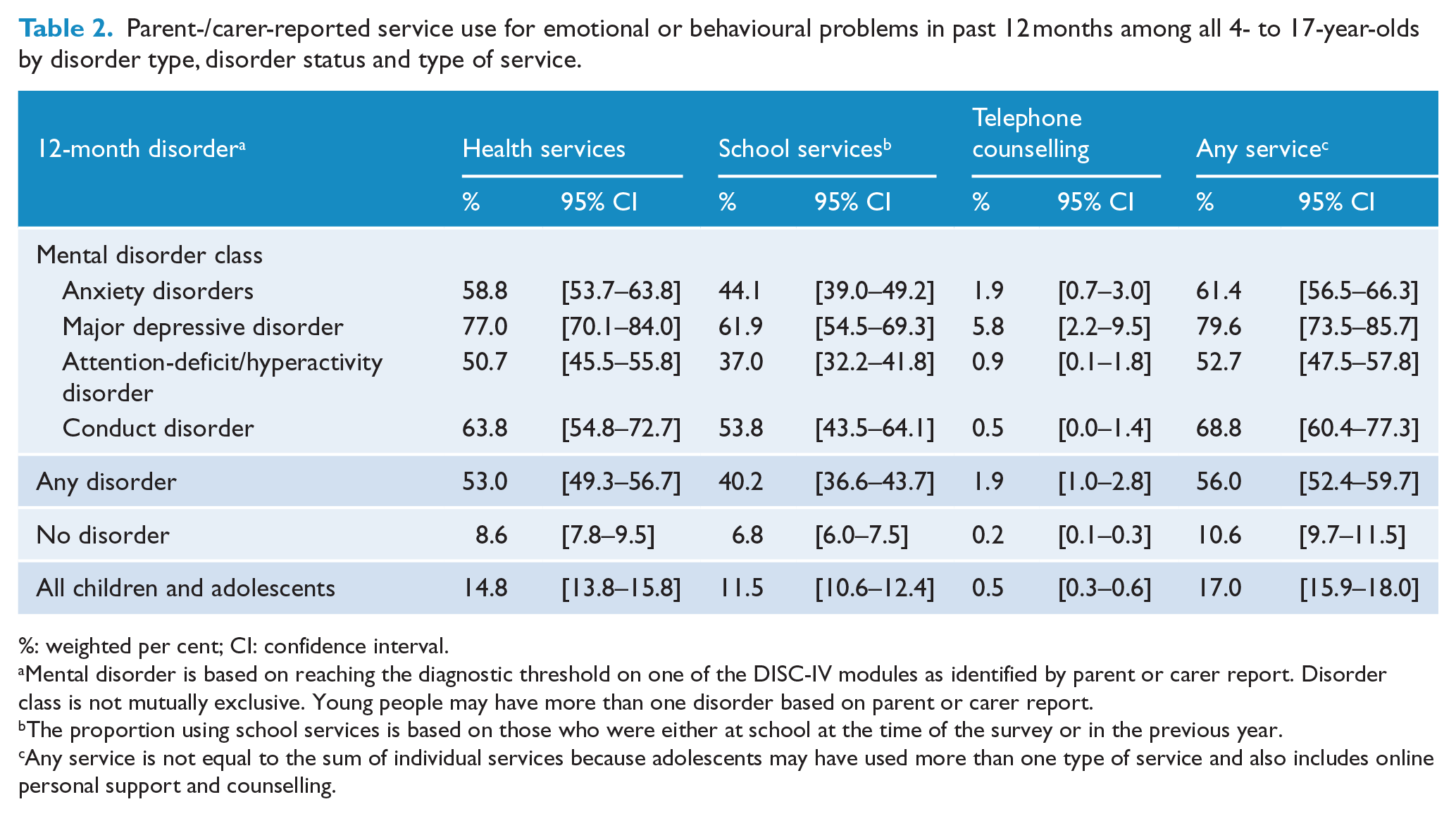
%: weighted per cent; CI: confidence interval.
Mental disorder is based on reaching the diagnostic threshold on one of the DISC-IV modules as identified by parent or carer report. Disorder class is not mutually exclusive. Young people may have more than one disorder based on parent or carer report.
The proportion using school services is based on those who were either at school at the time of the survey or in the previous year.
Any service is not equal to the sum of individual services because adolescents may have used more than one type of service and also includes online personal support and counselling.
Of those with mental disorders, 53.0% had used health services; however, 40.2% had received services through a school or other educational institution that they were attending. Just over one-third with mental disorders (36.2%) had received services from both (not in table). Only 1.9% of young people with mental disorders had used a telephone counselling service in the previous 12 months. There were too few using online services according to parents and carers to report these figures separately, and therefore, we rely on reports from adolescents themselves.
Service use was significantly higher among those with major depressive disorder (79.6%) than among those with anxiety disorders (61.4%, p < 0.01), ADHD (52.7%, p < 0.001) or conduct disorder (68.8%, p < 0.05). Both health and school service use were highest among young people with major depressive disorder. Use of a telephone counselling service in the previous 12 months was also highest among young people with major depressive disorder (5.8%).
Similar proportions of males and females with mental disorders but a significantly higher proportion of 12- to 17-year-olds (65.1%) than 4- to 11-year-olds (48.9%) had used services in the previous 12 months (p < 0.001).
Parent-/carer-reported service use among 4- to 17-year-olds with mental disorders by type of provider and severity of disorder
Overall, rates of service use by young people with mental disorders increased with disorder severity from 41.2% of those with mild disorders to 72.5% of those with moderate disorders and 87.6% of those with severe disorders (see Table 3).
Parent-/carer-reported service use in past 12 months among 4- to 17-year-olds with mental disorders (identified by parent or carer report, n = 870) by severity of mental disorder and service provider.
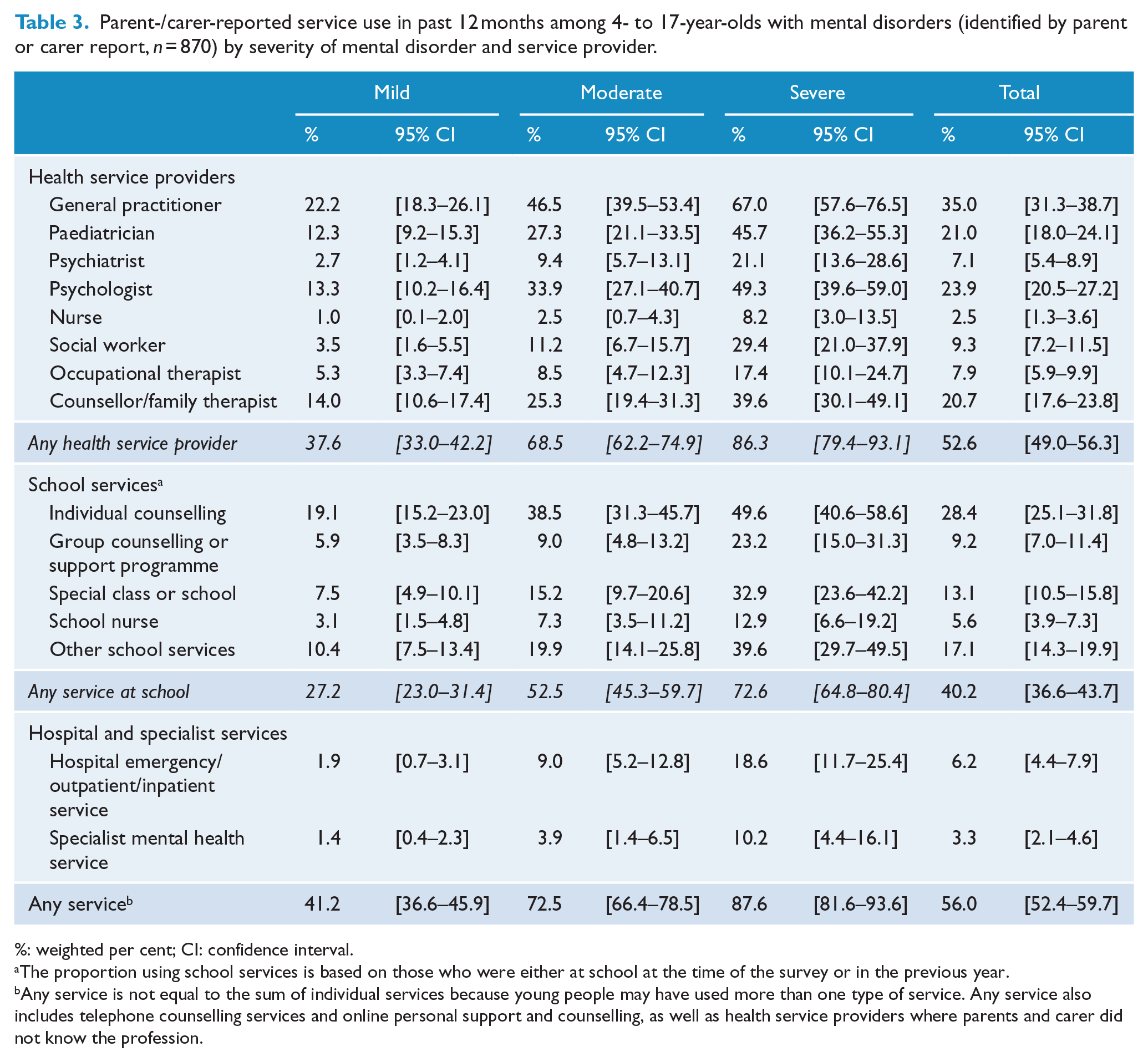
%: weighted per cent; CI: confidence interval.
The proportion using school services is based on those who were either at school at the time of the survey or in the previous year.
Any service is not equal to the sum of individual services because young people may have used more than one type of service. Any service also includes telephone counselling services and online personal support and counselling, as well as health service providers where parents and carer did not know the profession.
The health service providers most commonly seen by young people with mental disorders were GPs (35.0%), psychologists (23.9%), paediatricians (21.0%) and counsellors or family therapists (20.7%).
Of those with mental disorders who had used a health service, 8.1% had only seen a GP, 38.9% had seen a GP as well as a psychiatrist or psychologist and 29.0% had seen a GP as well as a paediatrician in the previous 12 months (not in table).
Young people with severe disorders most commonly visited a GP for emotional and behavioural problems with two-thirds (67.0%) having done so in the previous 12 months. Half of severe cases (49.3%) had seen a psychologist. Just under half of severe cases (45.7%) had seen a paediatrician and one-fifth of severe cases had seen a psychiatrist (21.1%) in the previous 12 months (Table 3).
Almost one-fifth (18.6%) of young people with severe disorders had seen a health professional in a hospital emergency, outpatient or inpatient service and one-tenth (10.2%) had seen a health professional in a specialist child and adolescent mental health service.
Sociodemographic correlates of health and school service use by young people with mental disorders
In univariate analyses, there was a significant relationship between health service use by young people with mental disorders and family type, household income, and parent or carer employment but not with the highest level of parent or carer education, IRSED for the area in which they lived or the remoteness of the area (Table 4).
Sociodemographic (univariate and multivariate) predictors of health and school service use in the past 12 months among 4- to 17-year-olds with 12-month mental disorders (identified by parent or carer report, n = 870).
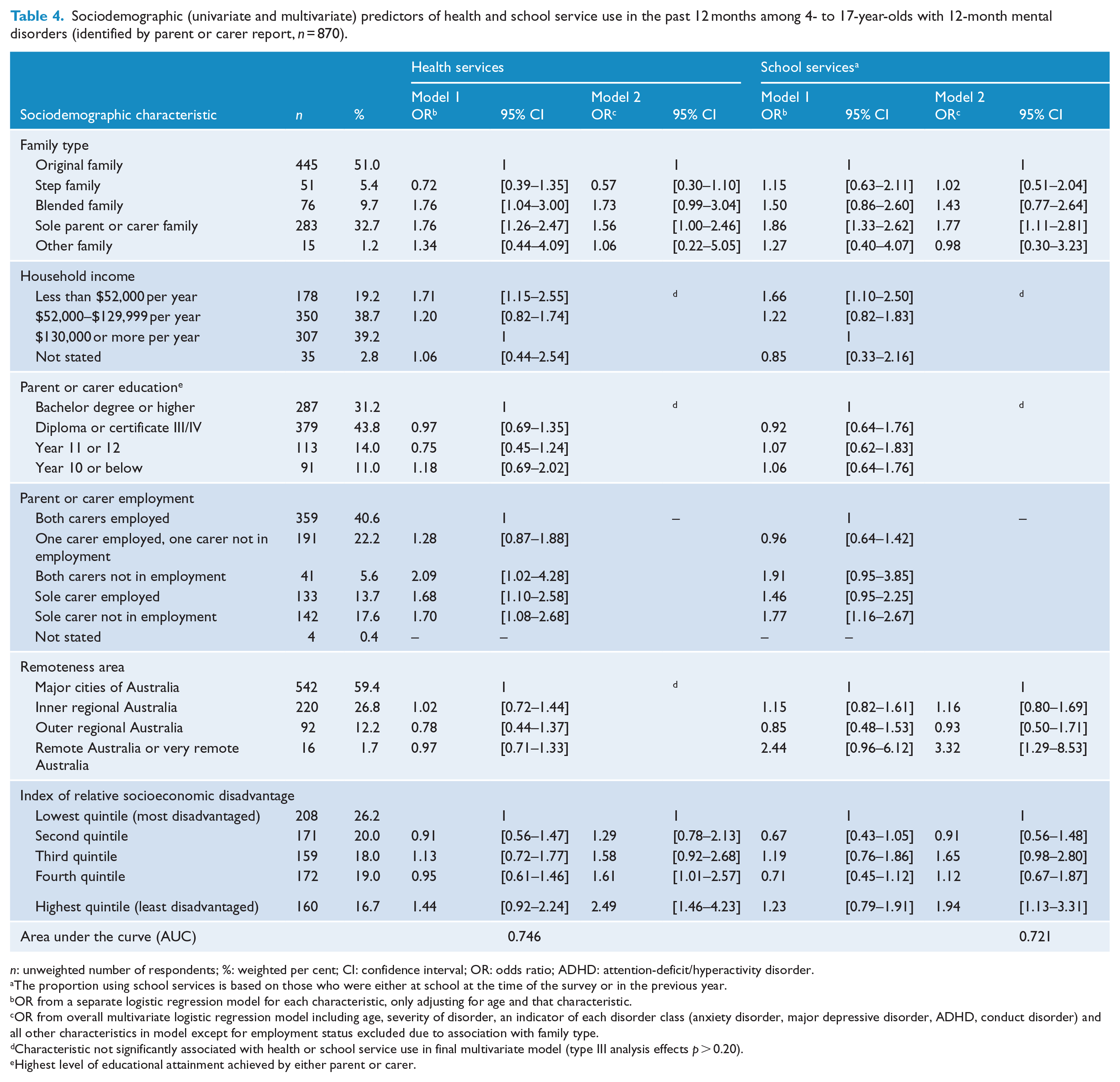
n: unweighted number of respondents; %: weighted per cent; CI: confidence interval; OR: odds ratio; ADHD: attention-deficit/hyperactivity disorder.
The proportion using school services is based on those who were either at school at the time of the survey or in the previous year.
OR from a separate logistic regression model for each characteristic, only adjusting for age and that characteristic.
OR from overall multivariate logistic regression model including age, severity of disorder, an indicator of each disorder class (anxiety disorder, major depressive disorder, ADHD, conduct disorder) and all other characteristics in model except for employment status excluded due to association with family type.
Characteristic not significantly associated with health or school service use in final multivariate model (type III analysis effects p > 0.20).
Highest level of educational attainment achieved by either parent or carer.
In particular, the odds of using health services in blended families (odds ratio [OR] = 1.76, 95% confidence interval [CI] = [1.04, 3.00]) and sole parent/carer families (OR = 1.76, 95% CI = [1.26, 2.47]) were higher compared to health service use by young people living with both their biological parents. Service use was also significantly higher in families with an annual household income of less than $52,000 compared to families with an annual household income of $130,000 or more (OR = 1.71, 95% CI = [1.15, 2.55]). Relative to two-parent families where both carers were employed, the odds of using services in sole parent/carer families irrespective of whether the parent/carer was employed (OR = 1.68, 95% CI = [1.10–2.58]) or not in employment (OR = 1.70, 95% CI = [1.08, 2.68]) were higher than in two-parent/carer families in which both were employed.
In multivariate analysis, the only sociodemographic factors significantly associated with health service use were family type and the IRSED. In particular, young people with mental disorders in sole parent/carer families (OR = 1.56, 95% CI = [1.00, 2.46]) had greater odds of using services compared to those in original families. Compared to young people with mental disorders living in the most disadvantaged quintile, those in the fourth quintile (OR = 1.61, 95% CI = [1.01, 2.57]) and the fifth or least disadvantaged quintile (OR = 2.49, 95% CI = [1.46, 4.23]) had greater odds of using health services.
The relationship between school service use and sociodemographic factors was similar to that found for health service use (Table 4).
Adolescent self-reported service use
In contrast to previous sections, this section presents service use as self-reported by 13- to 17-year-olds. Overall, 18.0% of all 13- to 17-year-olds reported using services for emotional and behavioural problems in the previous 12 months (Table 5). The proportion of females who reported using services was almost twice that of males (23.6% compared with 12.7%, p < 0.001).
Service use for emotional and behavioural problems in past 12 months among all 13- to 17-year-olds by sex and service sector as reported by adolescents (n = 2314).
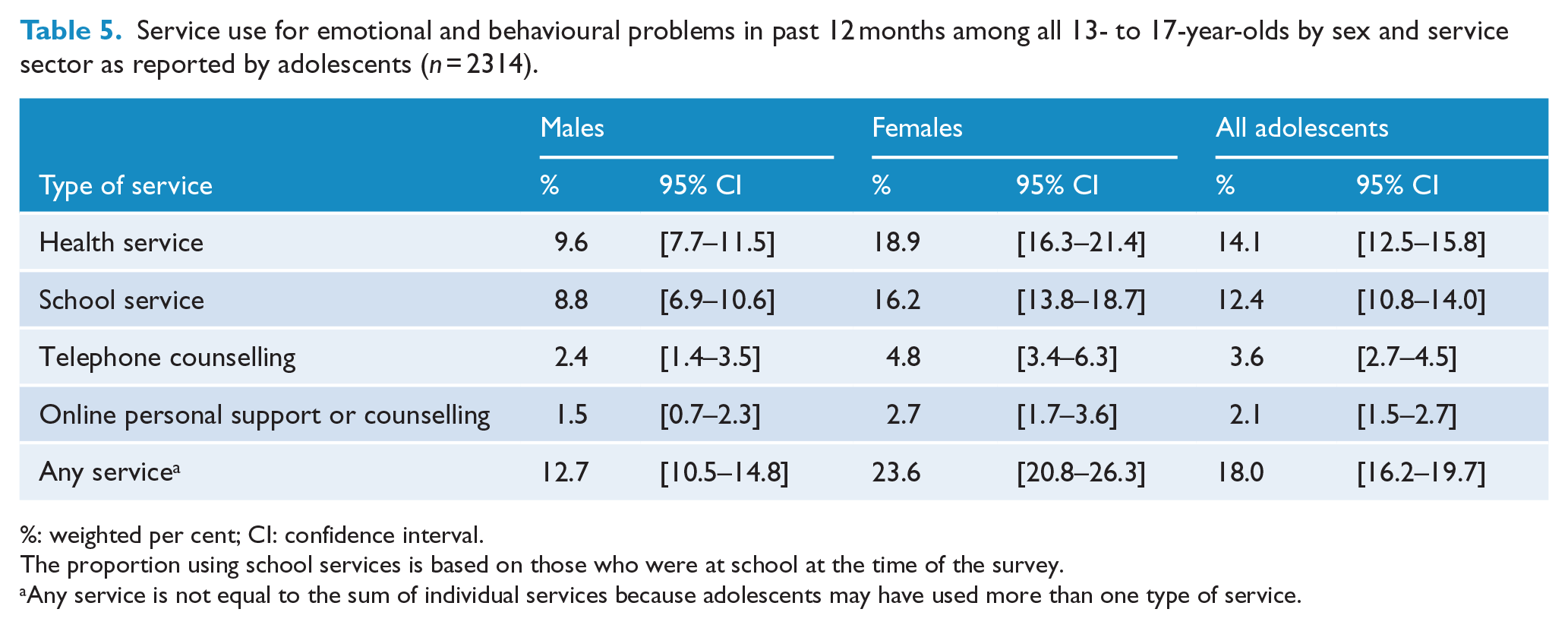
%: weighted per cent; CI: confidence interval.
The proportion using school services is based on those who were at school at the time of the survey.
Any service is not equal to the sum of individual services because adolescents may have used more than one type of service.
Among 13- to 17-year-olds, 19.7% (95% CI = [17.9%, 21.5%]) had 12-month mental disorders based on parent/carer or their own reports on DISC-IV modules.
Just over two-fifths of these adolescents with mental disorders reported to have used services for emotional or behavioural problems in the previous 12 months (44.7%). A significantly higher proportion of females than males had done so (55.2% and 30.8%, respectively; p < 0.001) (Table 6).
Services used for emotional or behavioural problems in past 12 months by 13- to 17-year-olds with mental disorders (identified by parent/carer or adolescent report, n = 481) by sex, informant and service sector.
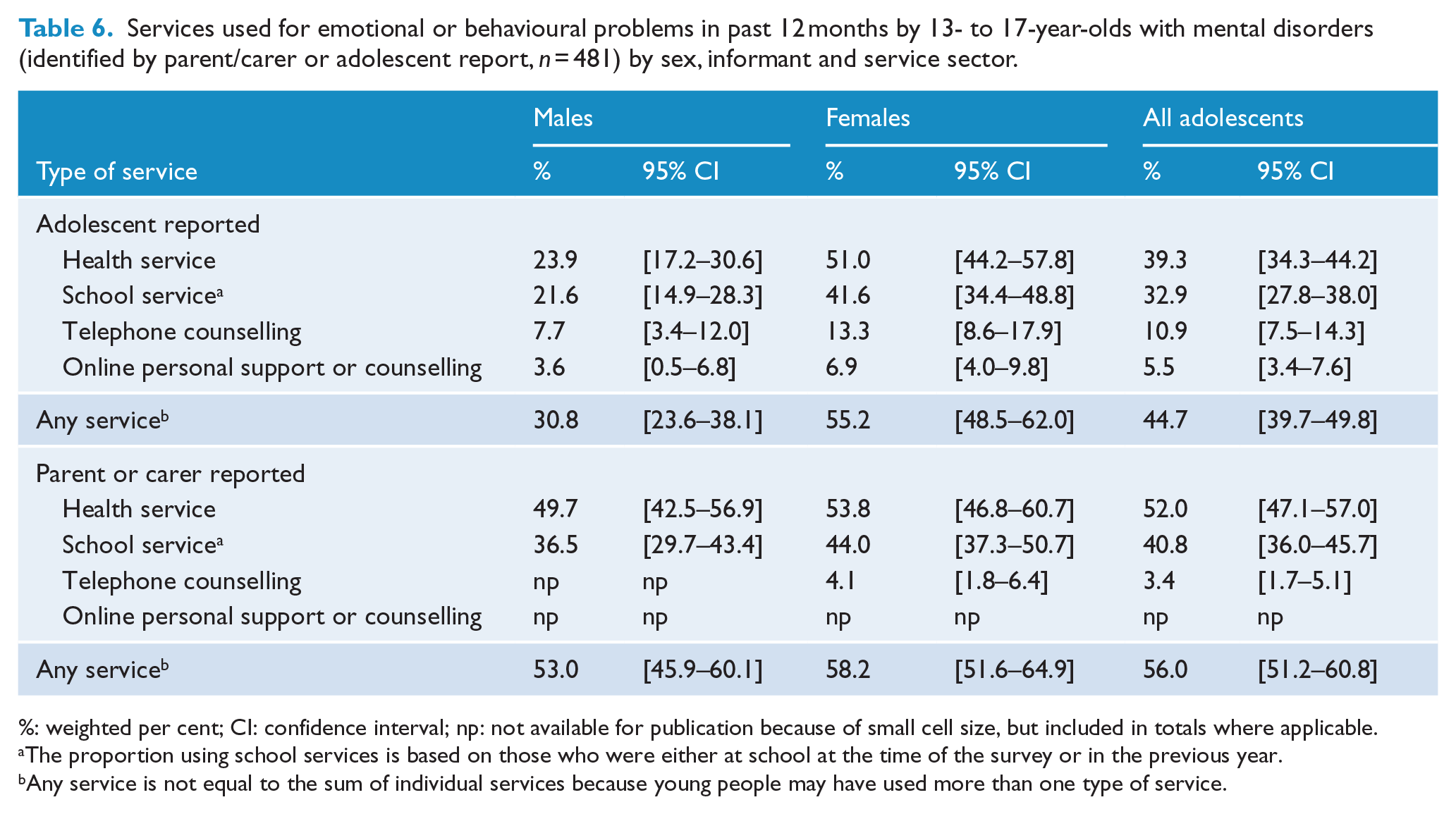
%: weighted per cent; CI: confidence interval; np: not available for publication because of small cell size, but included in totals where applicable.
The proportion using school services is based on those who were either at school at the time of the survey or in the previous year.
Any service is not equal to the sum of individual services because young people may have used more than one type of service.
Health services were the most frequent service use category reported by adolescents with mental disorders (39.3%) followed by school services (32.9%), telephone counselling (10.9%) and online personal support or counselling (5.5%).
Overall, parents and carers reported significantly more 12-month service use than adolescents (56.0% and 44.7%, respectively; p < 0.01), and most of this difference is accounted for by differences in service use reporting between adolescent males and their parents or carers.
Table 6 also highlights the difference in reporting of the use of telephone counselling and online personal support or counselling between parents or carers and young people. A small proportion of young people who used these services did so without the knowledge of their parents. Such privacy is a feature of these services.
About one-third of adolescents with mental disorders (36.6%) had used online services in the previous 12 months, with three-quarters of these using these services to seek information about mental health issues (27.1%) and half of these using an assessment tool (18.0%). Twice the proportion of females to males used online services for help with emotional or behavioural problems (Table 7).
Online and headspace services used for emotional or behavioural problems in past 12 months as reported by 13- to 17-year-olds with mental disorders (identified by parent/carer or adolescent report, n = 481) by sex and type of service.
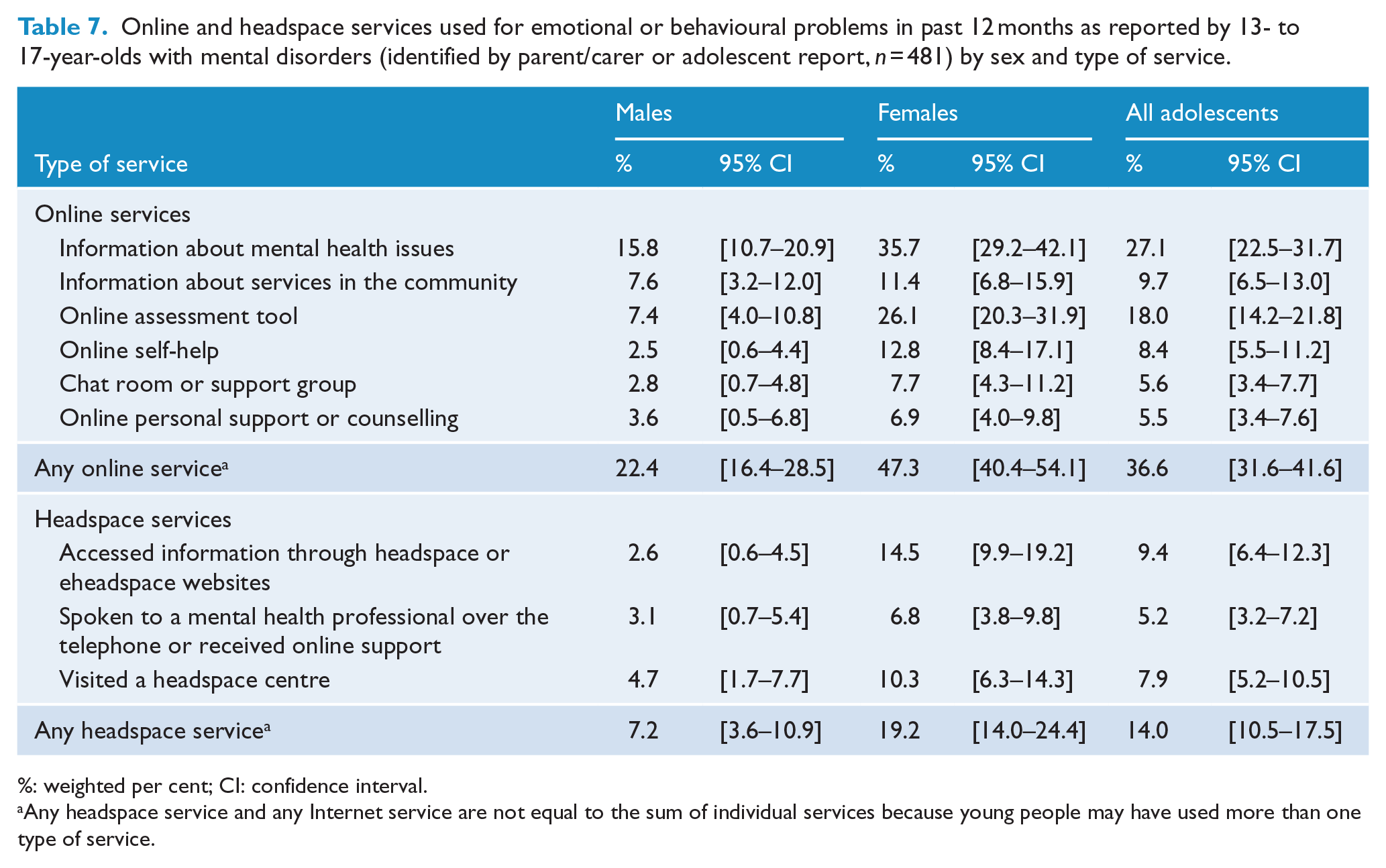
%: weighted per cent; CI: confidence interval.
Any headspace service and any Internet service are not equal to the sum of individual services because young people may have used more than one type of service.
Among adolescents with mental disorders, 14.0% had used any headspace service for help with emotional or behavioural problems in the previous 12 months with 7.9% having visited a headspace centre. Compared to adolescent males, more than twice the proportion of adolescent females with mental disorders had used headspace services in the previous 12 months (19.2% and 7.2%, respectively; p < 0.001).
Discussion
Based on nationally representative survey data from the second Australian Child and Adolescent Survey of Mental Health and Wellbeing, this paper has reported on service use for emotional and behavioural problems by all children and adolescents in Australia and by those with mental disorders.
Of all 4- to 17-year-olds, 17% had used services for emotional or behavioural problems in the previous 12 months. Of those, approximately half had mental disorders, two-fifths had other indicators of clinically significant problems and 10% did not have significant mental health problems based on indicators in the survey. It is possible that this 10% of children or adolescents had previously been diagnosed with a mental disorder, but treatment had resulted in the alleviation of symptoms and therefore the survey did not identify them as having a 12-month disorder. Additionally, many of the services considered, such as GPs and school counselling, are not just provided for those with mental disorders and offer important pathways for prevention and early intervention.
Just over half (56%) of 4- to 17-year-olds with mental disorders used services for emotional or behavioural problems in the previous 12 months. Although not directly comparable, these results suggest a substantial increase from the 29% with mental disorders having used services in the past 6 months as found in 1998 (Sawyer et al., 2000). Consistent with findings in the Australian adult survey, service use was highest in those with severe disorders (Burgess et al., 2009). Most severe cases had received a service – just under 90%. Service use was also highest among those young people with major depressive disorder and mirrors findings for Australian adults (Burgess et al., 2009). This is partly explained by the higher proportion of severe cases among those with major depressive disorder (43% compared to 19% of those with anxiety disorders and 10% of those with ADHD) (Lawrence et al., 2015b).
The health service providers most commonly seen were GPs, psychologists, paediatricians and counsellors or family therapists. Of those with mental disorders who had used any health service, many had seen a GP in combination with a mental health professional or a paediatrician. Just 8% had only seen a GP. Initial survey results show that multiple visits were common. For example, one-quarter of those visiting a psychologist, and one-fifth of those visiting a psychiatrist, had been on 10 or more occasions in the previous 12 months (Lawrence et al., 2015b). Together, these results provide strong evidence of the use of Medicare-funded mental health services consistent with reports of increased uptake by young people (Department of Health and Ageing, 2013).
Use of specialist child and adolescent mental health services was low as had been found in the 1998 survey (Sawyer et al., 2001). This was evident even among those with severe disorders. About 10% of those assessed as having a severe disorder had used specialist child and adolescent mental health services and 18% of severe cases had used hospital services (both emergency and inpatient) in the previous 12 months. However, young people with severe disorders were accessing mental health professionals in primary care and other settings – one-half had seen a psychologist and one-fifth had seen a psychiatrist in the previous 12 months.
Results highlight the major role played by the school sector in servicing for mental health problems. In 1998, 12% of 4- to 17-year-olds with mental health problems had received counselling in schools in the previous 6 months (Sawyer et al., 2001). In this current survey, 40% of 4- to 17-year-olds with mental disorders had used any school service and 28% had received individual counselling at school in the previous 12 months. As with the first survey, it is not known who provided the counselling, and in Australia, the professional background, training and experience of school counsellors vary among school systems and schools, as does their availability (Australian Psychologists and Counsellors in Schools, 2013). Because of the major role played by school counsellors, it is important that they are appropriately qualified and skilled to identify and manage mental health problems and liaise with health and other community services so that young people receive the help that they need.
Young people with mental disorders living in families with a low income, unemployed parents or with a sole parent or carer had higher rates of 12-month service use compared to those in families that were least disadvantaged. As reported by Lawrence et al. (2015b), mental disorders were more prevalent among young people in disadvantaged families, and it is likely that these disorders were also more severe, therefore resulting in greater service use. From the results of the multivariate analyses, it was evident that, after adjusting for type of disorder and severity, only family type and the IRSED were statistically significant. It is possible that young people with mental disorders in sole parent/carer families are more easily detected by schools or others in the community or that the impact of these problems is more acutely experienced (Teagle, 2002). Furthermore, after adjustment for type of disorder, severity and family characteristics, it was evident that young people with mental disorders living in the least disadvantaged geographical areas (higher socioeconomic status) were more likely to have used services than those living in the most disadvantaged areas. Because IRSED was not significant in univariate analysis, it was likely that its association was being masked by the greater concentration of more severe cases and other at-risk families (e.g. sole carer families) in the most disadvantaged areas (as represented in quintiles of the IRSED distribution) that had greater service use.
Based on adolescent reports, online services were being accessed for information or help by about one-third of 13- to 17-year-old young people with mental disorders. This was especially evident among adolescent females, consistent with previous reports ((Burns and Birrell, 2014; Burns et al., 2010); Ivancic et al., 2014). Additionally, a higher proportion of adolescent females with mental disorders were accessing headspace services, consistent with the recent profiling of headspace clients indicating two-thirds were female (Rickwood et al., 2014). These results show an uptake of online and youth mental health centres by adolescents alongside traditional health and school services. Not reported in this paper, but important to acknowledge, is the use of online services by parents seeking information and help in respect of their child or adolescent’s emotional or behavioural problems, possibly without their knowledge. Initial survey results showed that 38% of parents and carers of young people with mental disorders had used online services to get help or information about their child’s problems (Lawrence et al., 2015b).
More parents and carers of 13- to 17-year-olds reported any service use in the past 12 months than did 13- to 17-year-olds themselves (56% compared with 45%). The difference, however, was mostly due to adolescent males self-reporting only half as much service use as reported by their parents and carers. Some of the differences in reporting of service use may be due to different perceptions of symptoms and their severity between parents/carers and adolescents. If parents are perceiving problems where adolescents are not, reports of service use (especially of health services) for those problems may also appear to be higher according to parental reports (Sawyer et al., 2007; Whalin and Deane, 2012). Differences between parents and young people in their perceptions and understanding of symptoms, and the need for help are relevant to the design of services. These differences point to the importance and value of consulting both parents and young people about their experiences so as to facilitate better the design of services that meet their needs.
Limitations
The survey has some limitations that could have influenced the results. First, the response rate of 55% may have introduced some bias not accounted for by weighting. Second, service use was self-reported and this could have resulted in either under-reporting or over-reporting for reasons such as poor recall or social desirability. Third, it was not possible to link service use with a particular mental disorder. Fourth, it was not possible to gauge the adequacy or appropriateness of the services accessed and the treatment provided relative to the presenting problems. Finally, it is difficult to compare rates of service use with the first survey in 1998 primarily due to the different reference periods but also due to changes in question wording and determination of disorder status.
Conclusion
Many parents seek help and advice if they believe that their child or adolescent has emotional or behavioural problems. Health services and schools are the major providers of services for emotional and behavioural problems in young people, but telephone counselling and online services have also become well-established parts of the service environment. GPs are the most commonly accessed health service providers by young people with mental disorders. Service use for mental disorders appears to have increased over the past 15 years, and there are high rates of service use for those with severe disorders, but overall coverage could be further improved. The results of this survey highlight the need to examine why those, particularly those with more severe disorders, who are not using services are not doing so. Findings from the survey about the prevalence, severity and burden of disorders together with information about service use and areas of unmet need should inform policy and planning of mental health services for young people well into the future. Further analyses will address perceived need for mental health care and barriers to accessing services.
Footnotes
Acknowledgements
Data collection was undertaken by Roy Morgan Research. The authors would like to thank the 6310 families that gave their time to participate in the survey; Rajni Walia, Gerry Bardsley and the team at Roy Morgan Research; and the Survey Reference Group for their input into the design and conduct of the survey. Professor Zubrick is supported by the Australian Research Council Centre of Excellence for Children and Families over the Life Course (CE140100027).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The second Australian Child and Adolescent Survey of Mental Health and Wellbeing was funded by the Australian Government Department of Health.