
Abstract
Objective:
To describe the extent to which parents report that 4- to 17-year-olds with symptoms meeting Diagnostic and Statistical Manual of Mental Disorders, 4th edition criteria for mental disorders need help, the types of help needed, the extent to which this need is being met and factors associated with a need for help.
Method:
During 2013–2014, a national household survey of the mental health of Australia’s young people (Young Minds Matter) was conducted, involving 6310 parents (and carers) of 4- to 17-year-olds. The survey identified 12-month mental disorders using the Diagnostic Interview Schedule for Children – Version IV (n = 870) and asked parents about the need for four types of help – information, medication, counselling and life skills.
Results:
Parents of 79% of 4- to 17-year-olds with mental disorders reported that their child needed help, and of these, only 35% had their needs fully met. The greatest need for help was for those with major depressive disorder (95%) and conduct disorder (93%). Among these, 39% of those with major depressive disorder but only 19% of those with conduct disorder had their needs fully met. Counselling was the type of help most commonly identified as being needed (68%). In multivariate models, need for counselling was higher when children had autism or an intellectual disability, in blended families, when parents were distressed, and in the most advantaged socioeconomic areas.
Conclusions:
Many children and adolescents meeting Diagnostic and Statistical Manual of Mental Disorders, 4th edition criteria for mental disorders have a completely unmet need for help, especially those with conduct disorders. Even with mild disorders, lack of clinical assessment represents an important missed opportunity for early intervention and treatment.
Introduction
Many mental health problems have onset in childhood and adolescence making this a critical stage for early intervention to reduce the burden of mental health problems in the community (Department of Health and Ageing, 2013; Kessler et al., 2005, 2007; Patel et al., 2007; Slade et al., 2009). About 14% of children and adolescents in Australia have 12-month mental disorders, and just over half (56%) have attended services for their problems (Johnson et al., 2016; Lawrence et al., 2016). The level of need for mental health services in the community can be assessed in several ways including by measuring the prevalence of mental disorders, the frequency of attendance at mental health services and the extent to which parents report needing help (Sawyer and Patton, 2000). In the 2007 national survey of Australian adults, less than half of those adults with mental disorders (43%) identified a need for help – of these, nearly a quarter had no service contact in the previous 12 months representing a substantial unmet need for help among adults (Meadows and Burgess, 2009).
Among children and adolescents, especially younger children, identification of problems and help-seeking is initiated by parents, teachers and other significant adults (Rickwood et al., 2007; Sawyer and Patton, 2000). Parental perception of a child’s need for help is a key determinant of service use (Ryan et al., 2015; Sawyer et al., 2004). Service use is higher when parents and young people have a higher level of mental health literacy (Jorm, 2012; Jorm et al., 2007). Even with recognition of problems, the process of seeking appropriate services and negative experiences with services can serve as a major barrier to parents (Boulter and Rickwood, 2013; Sayal, 2006; Sayal et al., 2010) and adolescents (Gulliver et al., 2010). Understanding what factors drive perceptions of a need for help is an important step in targeting interventions to increase mental health literacy, help-seeking behaviours and contact with appropriate services for young people experiencing mental health problems.
Factors known to be closely tied with the use of services by young people with mental health problems are problem severity, problem persistence, comorbidity and the degree of associated burden that the problem imposes on parents and families (Angold et al., 1998; Boulter and Rickwood, 2013; Logan and King, 2001; Ryan et al., 2015; Zwaanswijk et al., 2003). The presence of additional medical and school problems is also associated with greater help seeking for the child (Zwaanswijk et al., 2003). Problem identification by parents and teachers can be more difficult for emotional or internalising problems that are not so readily identifiable or burdensome on the family (Angold et al., 1998; Boulter and Rickwood, 2013; Logan and King, 2001; Sawyer and Patton, 2000). An overrepresentation of mental disorders in socially and economically disadvantaged families has been observed in adult (Allen et al., 2014; Enticott et al., 2016) and child and adolescent populations (Ford et al., 2003; Green et al., 2005; Kessler et al., 2012; Sawyer et al., 2001), but the link between disadvantage and help-seeking and service use is poorly documented. A recent systematic review found higher levels of service use for mental health problems among children in single parent households, and where there had been a change in family structure. In contrast, the authors concluded that there was no consistent association of service use with parental education, employment status or household income once adjusting for mental health symptoms (Ryan et al., 2015).
The association between parental and child psychological problems is well known (Reupert et al., 2012; Van Santvoort et al., 2015) and current evidence suggests that having a parent with psychological problems is associated with greater use of services, especially specialist mental health services for the child (Ryan et al., 2015). However, history of service use in the family for mental health problems is not linked with service use (Ryan et al., 2015). Parents with psychological problems may be better at recognising similar symptoms in their child than those without problems. Qualitative research with parents who had sought help from a mental health professional for their child identified that having mental health problems in the family (recognition of family vulnerability) was a contributing factor to their seeking help (Boulter and Rickwood, 2013). Conversely, parental psychopathology can reduce help-seeking if problems are severe and as a consequence, even though the parent may recognise problems in their child, they are less likely to seek help due to their reduced psychological availability or capacity to do so (Mendenhall and Frauenholtz, 2015; Zwaanswijk et al., 2003). In respect to other psychosocial factors, there is presently insufficient and contradictory evidence of a link between service use by children with mental health problems and either family functioning or parent–child relationship quality (Ryan et al., 2015). While family stress does increase the likelihood of help seeking for children’s mental health problems (Zwaanswijk et al., 2003), a young person’s problems can also be a cause or consequence of family stress (Logan and King, 2001). Overall, these findings suggest that parental psychopathology and psychosocial factors in the family are important for problem identification and help seeking for children with mental health problems but associations are complex. Further research is needed to untangle these relationships.
This study uses data from a nationally representative sample of families with 4- to 17-year-olds to report parents’ views about the help needed for Australian children and adolescents meeting the diagnostic criteria for mental disorders as described in the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (American Psychiatric Association) (DSM-IV). We contribute to current knowledge by examining parental perceptions of the need for different types of help for the most prevalent disorders in children and adolescents: anxiety disorders, major depressive disorder, attention-deficit/hyperactivity disorder (ADHD) and conduct disorder. In light of inconsistent and contradictory findings in respect to predictors of mental health service use by children and adolescents, we further examine whether sociodemographic factors, parental mental health and family functioning are associated with parental perception of need for different types of help.
The study was designed to answer four questions:
What proportion of parents of 4- to 17-year-olds meeting DSM-IV criteria for mental disorders report that their child/adolescent needs help?
What types of help are identified by parents?
What factors are associated with a need for help?
To what extent is this need for help being met?
Methods
Population
The second Australian Child and Adolescent Survey of Mental Health and Wellbeing (Young Minds Matter/YMM) was conducted during 2013–2014 by the Telethon Kids Institute, The University of Western Australia in partnership with Roy Morgan Research, and funded by the Australian Government Department of Health. In total, 6310 parents/carers (for brevity referred to as parents) across Australia participated in face-to-face interviews (55% of eligible households). Interviews with parents (84% female; 81% biological mothers) were conducted using a computer-assisted personal interview (CAPI). Where there was more than one child in a family eligible for the study (aged 4–17 years), the study child was randomly selected. The YMM survey is a nationally representative sample of 4- to 17-year-olds. The survey methodology has been described in detail as published in this journal (Hafekost et al., 2016).
Participation in the survey was voluntary and all participants gave written consent to participate in the survey. The research protocol for the study was approved by the Australian Government Department of Health Human Research Ethics Committee, and The University of Western Australia Human Research Ethics Committee.
Variables
Mental disorders
Mental disorders were assessed using the Diagnostic Interview Schedule for Children Version IV (DISC-IV) (Fisher et al., 1993) and for the purpose of the study were defined on the basis of the diagnostic criteria described in the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV; American Psychiatric Association, 2000). The DISC-IV is an internationally validated tool designed primarily for epidemiological research and can be administered by trained, lay interviewers. Seven mental disorders were assessed using the relevant DISC-IV modules completed by parents. These were as follows: anxiety disorders (social phobia, separation anxiety disorder, generalised anxiety disorder and obsessive-compulsive disorder), major depressive disorder, ADHD and conduct disorder.
A new measure of disorder severity was developed for YMM. Items in the measure asked about the degree to which symptoms were impacting the child’s functioning in four life domains: at school or work, with friends, impact on family and impact on self, including personal distress. Using responses to these items, disorder severity was then classified as mild, moderate or severe by applying the national mental health service planning standard ratio of severity (Zubrick et al., 2015). Overall, 14% of all 4- to 17-year-olds met the criteria for a 12-month mental disorder – about 60% were mild, 25% moderate and 15% severe (Lawrence et al., 2016).
Parent perceived need for help for their child
A separate module asked parents about their child’s need for help with emotional or behavioural problems in the previous 12 months. The module was adapted from the instrument used in the 1998 (Meadows et al., 2000) and the 2007 adult surveys (Meadows and Burgess, 2009). Adaptation of these materials was undertaken by the survey team in consultation with members of the YMM Survey Reference Group. This allowed for the item pool to be modified so it was appropriate for help seeking relevant to children and adolescents (see Figure 1). Parents were asked questions about perceived needs if they had directly identified a problem with their child (either by directly reporting service use, or the need for services for emotional or behavioural problems), or if through their responses to earlier questions in the DISC-IV modules or the Strengths and Difficulties Questionnaire (Goodman, 1994) a possible problem had been indicated (i.e. it was established through programming of the CAPI that thresholds on these instruments had been met). Overall, two-thirds of all parents completed the module.
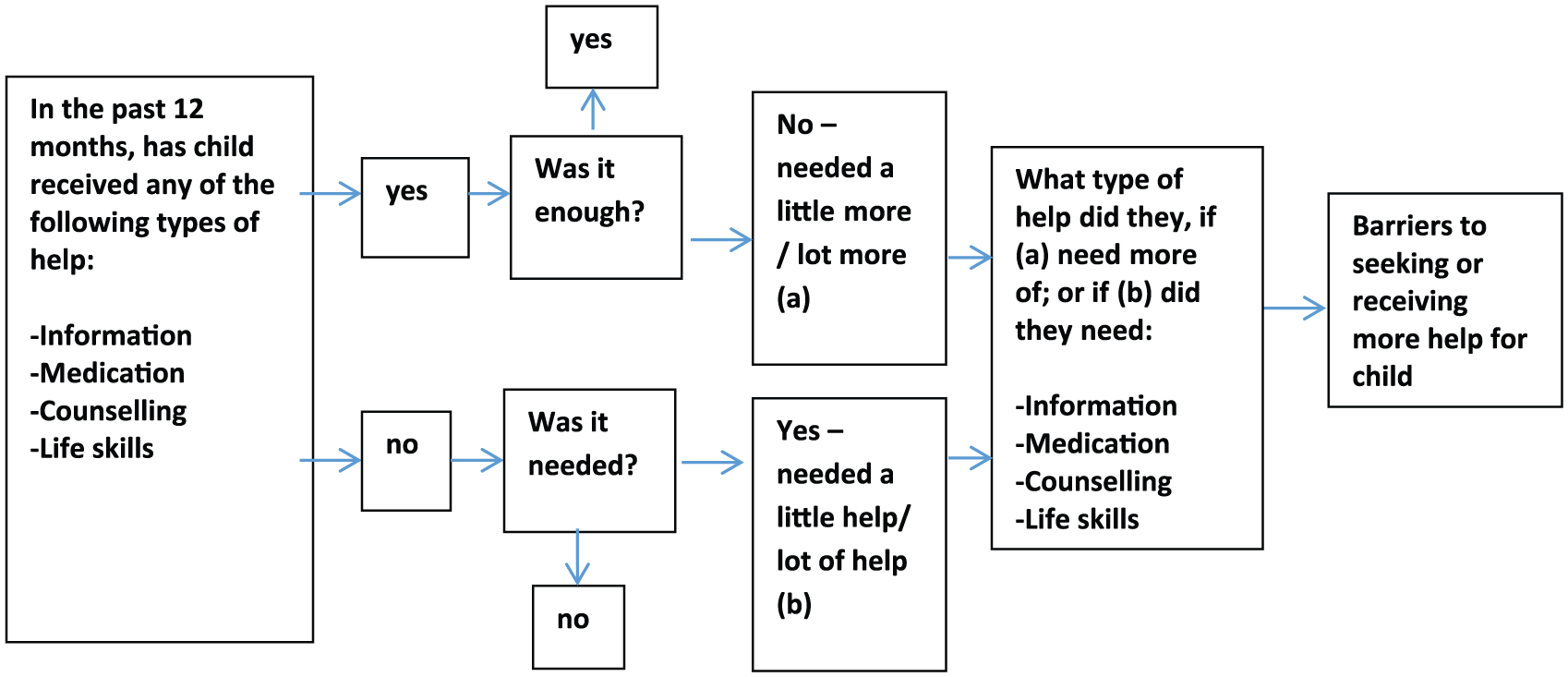
Flow of questions in perceived need module.
Need for four types of help was assessed:
Information about emotional or behavioural problems, treatment and available services (‘information’);
Prescribed medication for emotional or behavioural problems (‘medication’);
Counselling or a talking therapy about problems or difficulties (either one-on-one, as a family or in a group) (‘counselling’);
Courses or other counselling for life skills, self-esteem or motivation (‘life skills’).
For each of the four types of help, parents were asked if their child had received that help; if so, did they receive enough help, and if not was this help needed (see Figure 1). The level of need was classified as being either ‘fully met’, ‘partially met’, ‘unmet’ or ‘no need’. For those needing more than one type of help, need for ‘any type of help’ was based on a composite measure of the individual ratings for each type of help needed. To obtain population estimates of prevalence, all those not filtered into the module were categorised as having no need.
Sociodemographics characteristics
Family blending, household income, highest level of parent education and labour force status were collected and classified using the Australian Bureau of Statistics standard questions. Employment status was recoded to indicate whether there was no employed parent in the household. Area-level socioeconomic status was taken from the 2011 ABS Index of Relative Socio-Economic Disadvantage (IRSED) and together with remoteness was assigned based on the Statistical Area 1 (SA1) of residence.
Psychosocial characteristics
Family functioning was measured by a shortened version of the General Functioning Subscale of the McMaster Family Assessment Device (Boterhoven de Haan et al., 2014). Poor functioning indicates serious problems in the family likely needing clinical intervention (3.7%). The Kessler Psychological Distress Scale (K 10) was used to measure levels of primary carer distress in the previous four weeks (Kessler et al., 2003). The primary carer (parent) was also asked if they had ever been told by a doctor or mental health professional that they have a mental health problem. Parents were asked if their child had been bullied, teased or picked on to the point of distress.
Child factors
Factors included gender and age group, and parent report of diagnosis with autism, or an intellectual disability. Of those meeting DSM-IV criteria for a mental disorder, 19.2% also had either autism or an intellectual disability. This proportion was higher for children or adolescents with ADHD (27.1%), lowest for those with major depressive disorder (11.5%) and similar for those with an anxiety disorder (20.0%) or conduct disorder (22.3%).
Sample characteristics are described in Table 1.
Sample characteristics (n = 870) and proportion with any need for help.
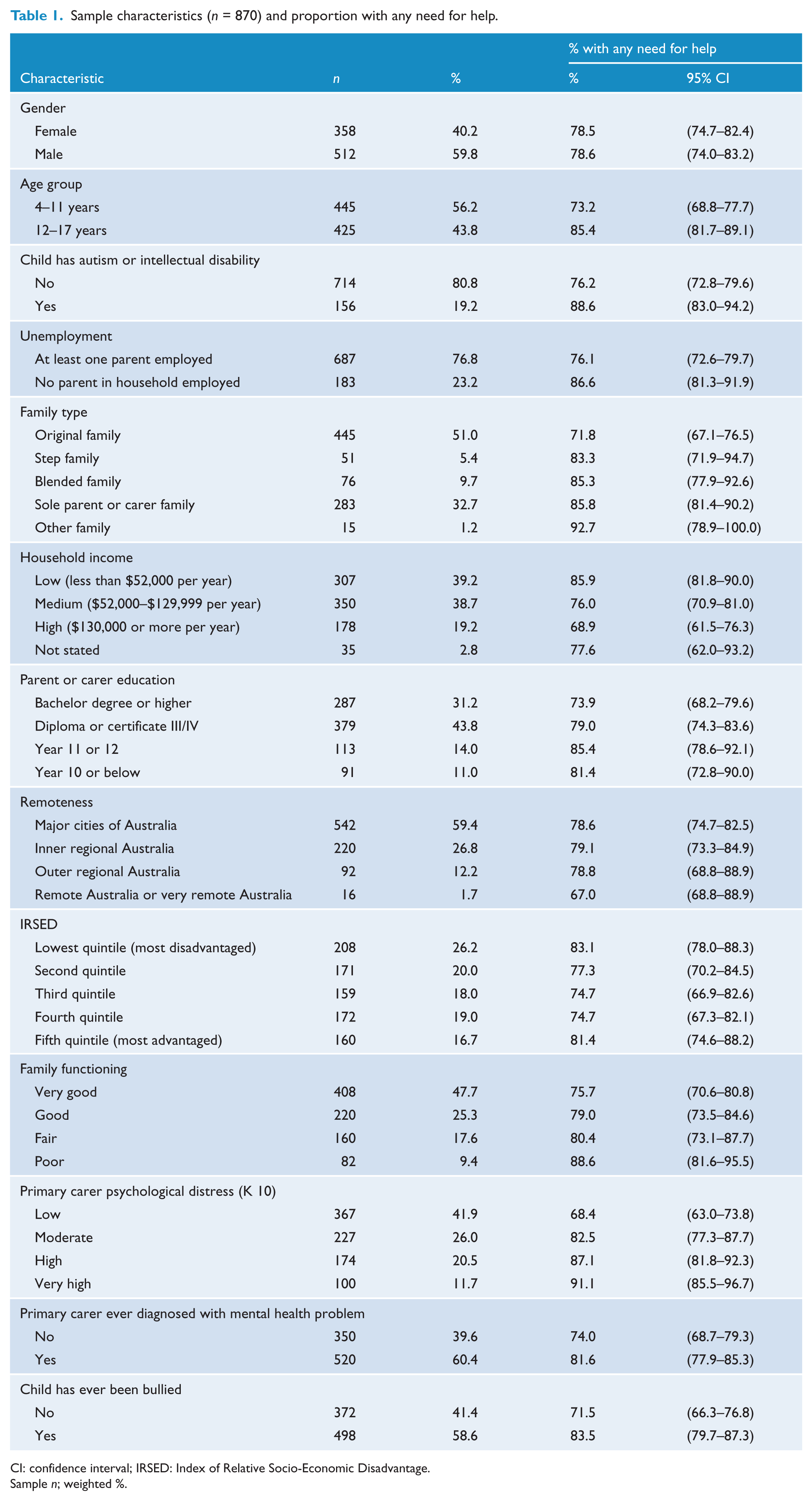
CI: confidence interval; IRSED: Index of Relative Socio-Economic Disadvantage.
Sample n; weighted %.
Analysis
All the results have been weighted to represent 4- to 17-year-olds in the Australian population. The relationship between child, sociodemographic and psychosocial characteristics with need for help was modelled using PROC SURVEYLOGISTIC in SAS Version 9.4.
Results
The proportion of 4- to 17-year-olds with mental disorders needing help
About three quarters (78.6%) of young people with mental disorders were identified as needing at least one of the four types of help – more 12- to 17-year-olds (85.4%) than 4- to 11-year-olds (78.6%) – although a higher proportion of 4- to 11-year-olds had their needs completely unmet (Figure 2).
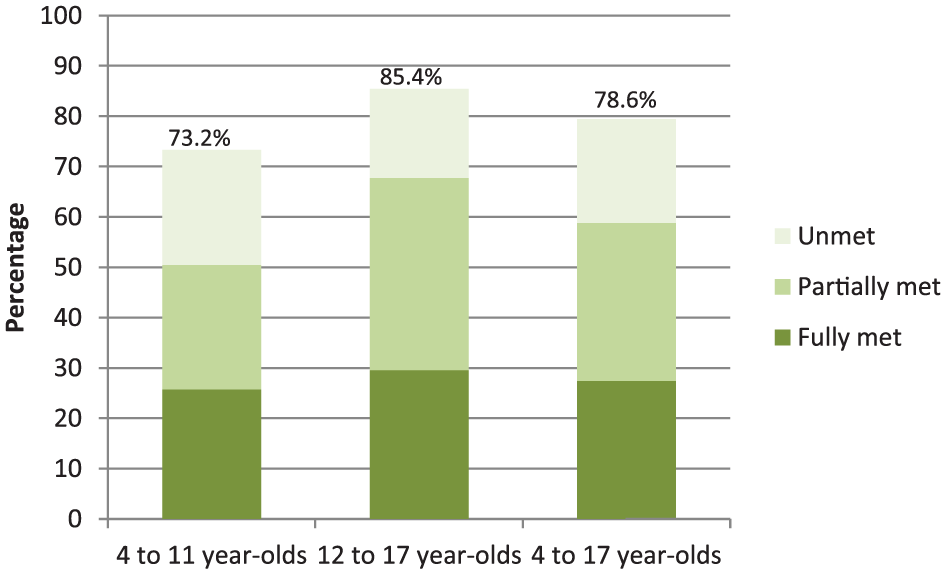
Proportion of 4- to 17-year-olds with mental disorders with any need for help and the proportion of these whose needs were unmet, partially met or fully met by age group (n = 870).
The type of help needed and levels of met need
The greatest identified need was for counselling (68.1%) followed by information (41.7%), life skills (36.0%) and medication (22.3%). A greater need for counselling than for other types of help was consistent across disorder groups (Table 2).
Type of help needed by 4- to 17-year-olds with mental disorders and the extent to which this need was met during the previous 12 months.
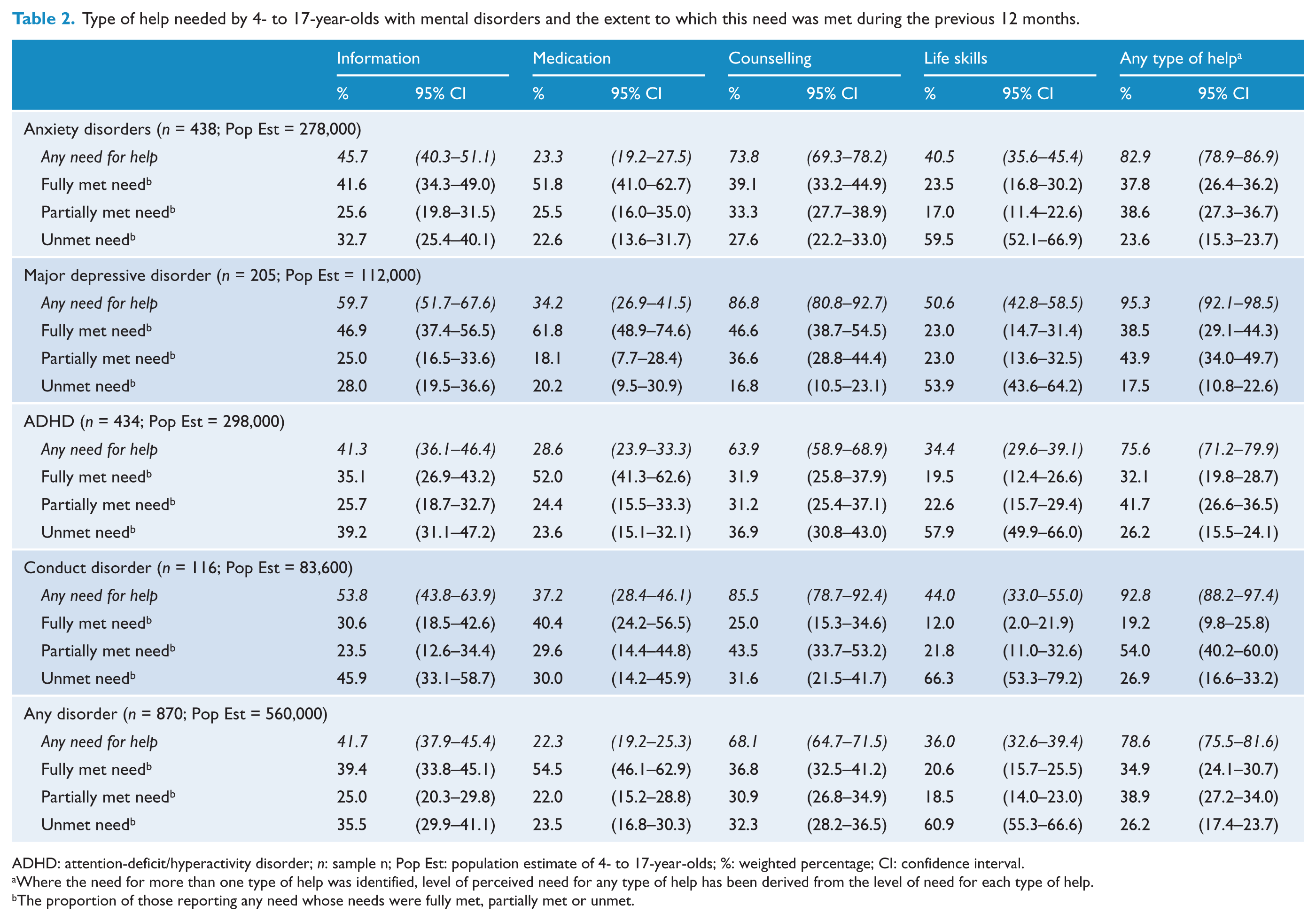
ADHD: attention-deficit/hyperactivity disorder; n: sample n; Pop Est: population estimate of 4- to 17-year-olds; %: weighted percentage; CI: confidence interval.
Where the need for more than one type of help was identified, level of perceived need for any type of help has been derived from the level of need for each type of help.
The proportion of those reporting any need whose needs were fully met, partially met or unmet.
The greatest area of unmet need was for life skills. In this area, when a need was identified, 60.9% meeting DSM-IV criteria for mental disorders had an unmet need for this type of help. Around one third had unmet needs for information (35.5%) and counselling (32.3%) and about one quarter (23.5%) had unmet need for medication representing 14.8%, 22.0% and 5.2% of 4- to 17-year-olds meeting DSM-IV criteria for mental disorders, respectively.
The type of help required by those with different disorders
The highest level of need for any type of help was for children and young people who met DSM-IV criteria for major depressive disorder (95.3%) and conduct disorder (92.8%). However, only 38.5% of parents whose children met DSM-IV criteria for a major depressive disorder and 19.2% of those parents with children who met DSM-IV criteria for conduct disorder reported that their need for any type of help was fully met. This pattern by disorder class was consistent across all four types of help. Levels of unmet need were also highest for conduct disorder with the exception of counselling where young people meeting DSM-IV criteria for ADHD had the highest level of unmet need (36.9%).
The type of help required by those with different levels of disorder severity
Level of need for all types of help was highest for those with more severe disorders (Figure 3). Two-thirds (68.3%) of 4- to 17-year-olds with mild mental disorders needed help. Nearly all 4- to 17-year-olds with moderate or severe mental disorders (91.8% and 100.0%) had a need for some kind of help.
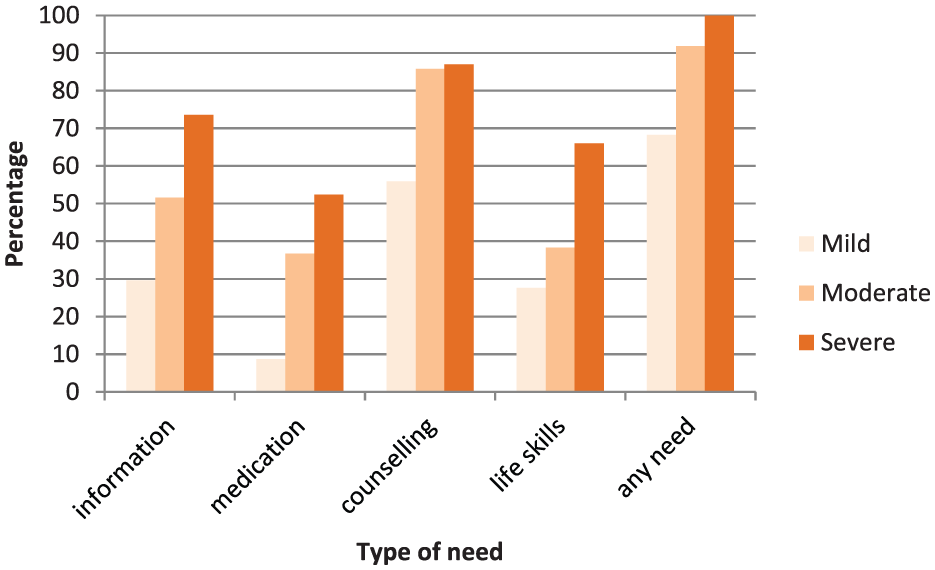
Type of help needed for 4- to 17-year-olds with mild, moderate or severe mental disorders (n = 870).
Factors associated with need for help
Any help
In the multivariate model, factors associated with a need for any type of help were as follows: The child meeting DSM-IV criteria for an anxiety disorder (OR = 2.7), major depressive disorder (OR = 8.9) or conduct disorder (OR = 5.1) compared to meeting the criteria for any other disorder, being diagnosed with autism or intellectual disability (OR = 2.7), being in a blended compared to an original family (OR = 2.3) and having moderate (OR = 1.9), high (OR = 2.4) or very high (OR = 2.8) compared to low levels of parental distress (Table 3). Being in the second versus fifth (most advantaged) quintile of disadvantage was associated with a lower perceived need for help (OR = 0.5) with a similar pattern observed for the first, third and fourth quintiles of disadvantage.
Logistic regression model predicting any need for help a for 4- to 17-year-olds with mental disorders (n = 870)
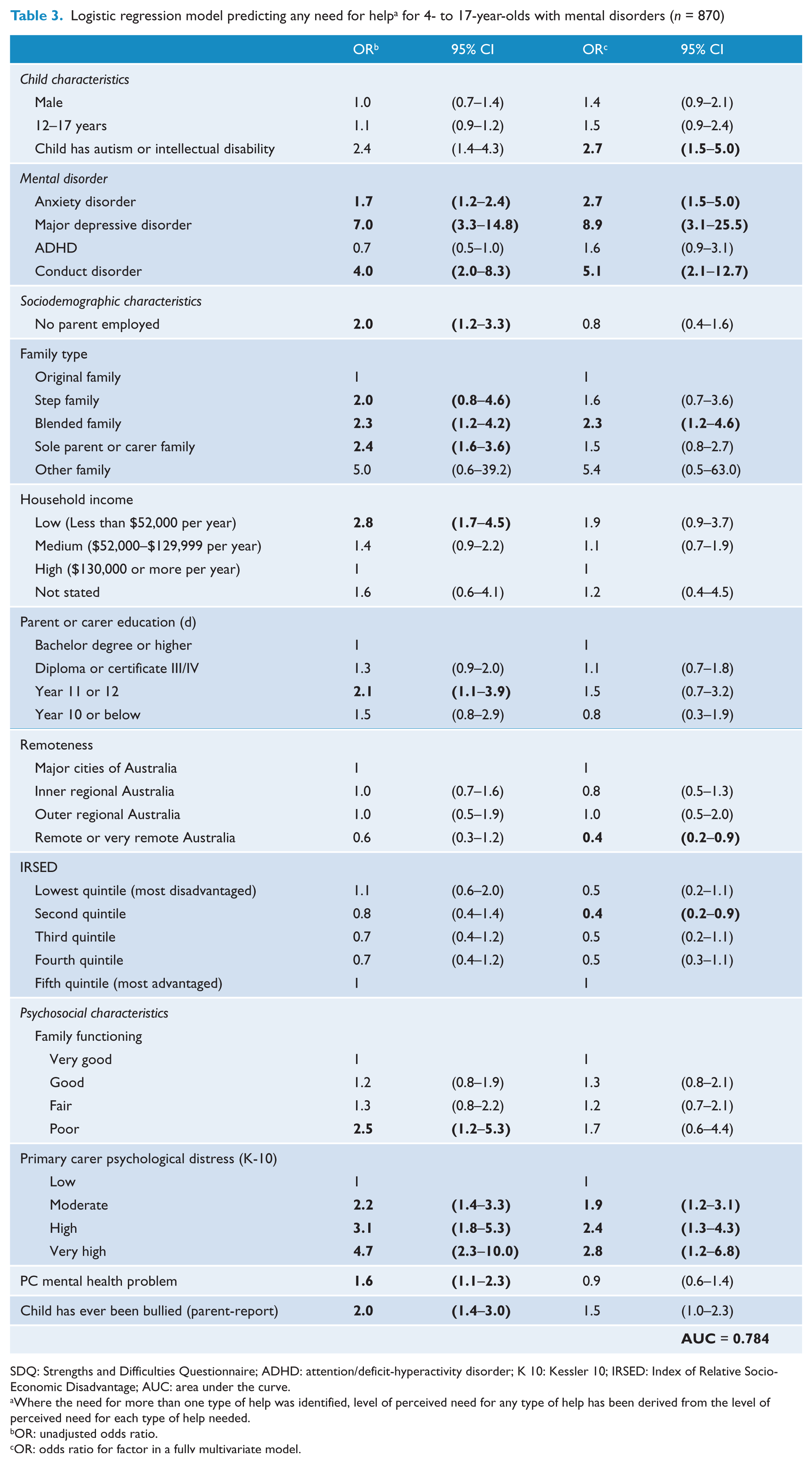
SDQ: Strengths and Difficulties Questionnaire; ADHD: attention/deficit-hyperactivity disorder; K 10: Kessler 10; IRSED: Index of Relative Socio-Economic Disadvantage; AUC: area under the curve.
Where the need for more than one type of help was identified, level of perceived need for any type of help has been derived from the level of perceived need for each type of help needed.
OR: unadjusted odds ratio.
OR: odds ratio for factor in a fully multivariate model.
Highest level of education of either primary or secondary carer.
Type of help
Multivariate models were repeated for each of the four types of help (Table 4). All mental disorders were significantly associated with the need for each type of help except for no increased need for counselling associated with ADHD, or for life skills associated with ADHD or conduct disorder compared to those with any disorder. If the child also had autism or an intellectual disability, they had a greater need for information, counselling and medication.
Logistic regression model predicting need for different types of help for 4- to 17-year-olds with mental disorders (n = 870).
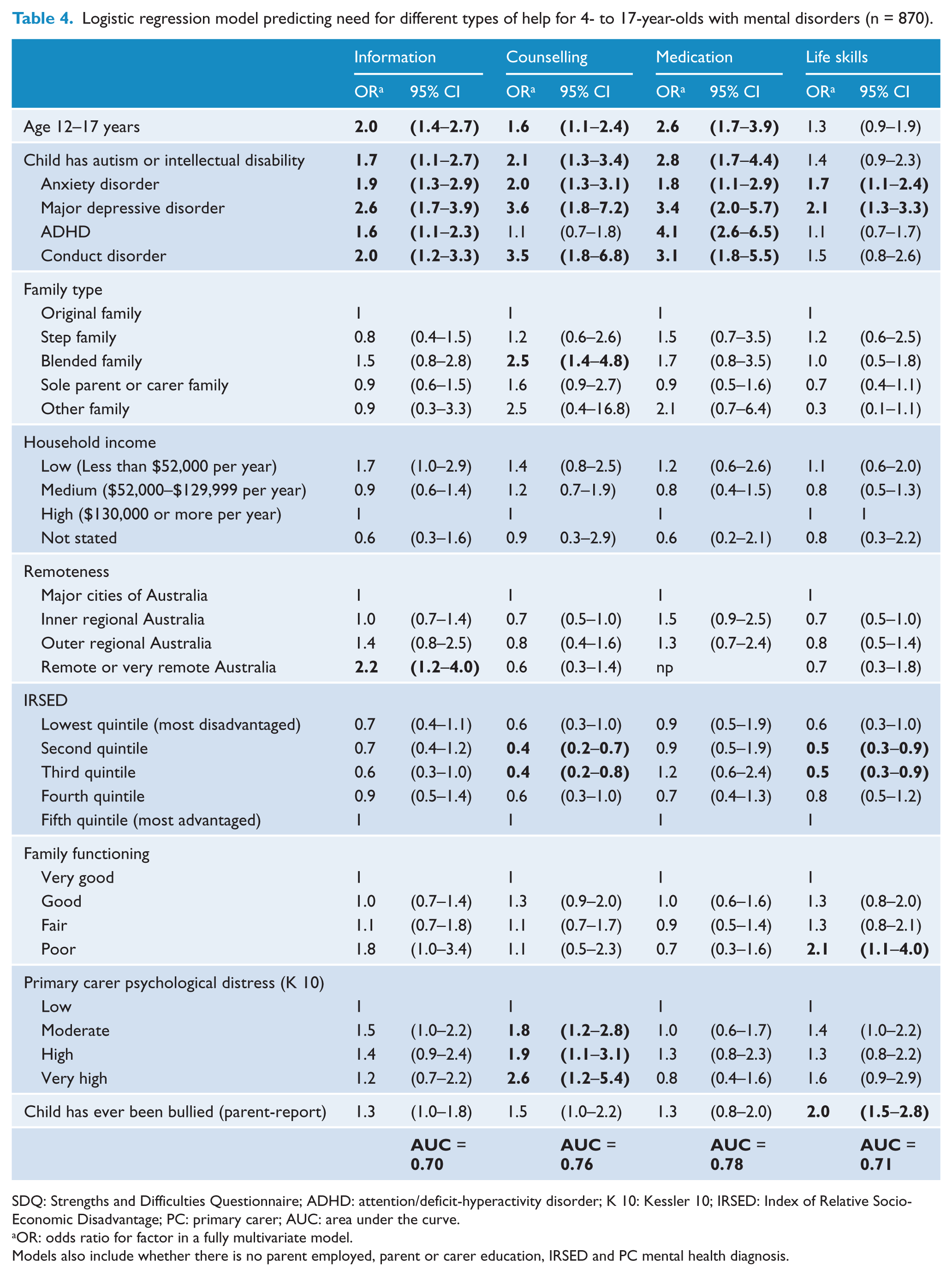
SDQ: Strengths and Difficulties Questionnaire; ADHD: attention/deficit-hyperactivity disorder; K 10: Kessler 10; IRSED: Index of Relative Socio-Economic Disadvantage; PC: primary carer; AUC: area under the curve.
OR: odds ratio for factor in a fully multivariate model.
Models also include whether there is no parent employed, parent or carer education, IRSED and PC mental health diagnosis.
Family type was only significantly associated with the need for counselling – in particular, being in a blended family compared to an original family (OR = 2.5). Living in a family with a low versus high income was associated with a higher odds ratio of need for information (OR = 1.7), although this just failed to reach statistical significance. Overall, there was a pattern of lower levels of need for counselling and life skills in quintiles other than the most advantaged but contrasts were still significantly lower in comparisons of the second and third quintiles with the highest (OR range = 0.4–0.5).
Having a poor level of family functioning was associated with greater need for life skills (OR = 2.1) but not the need for information (OR = 1.8; just failed to reach statistical significance), counselling or medication. Need for counselling was higher when parents had moderate (OR = 1.8), high (OR = 1.9) or very high (2.6) levels of psychological distress compared to low distress levels. Bullying was associated with twice the odds ratio of needing help for life skills (OR = 2.0).
Discussion
There are several key findings in this study. First, among children meeting DSM-IV criteria for mental disorder, including clinically significant impairment of functioning, 21% of parents did not identify any need for help for their child. This was particularly evident with 4- to 11-year-olds. Second, a higher proportion of parents whose children and adolescents met DSM-IV criteria for major depressive disorder or conduct disorder identified a need for help, while fewer parents felt that help was needed for those with ADHD or an anxiety disorder. Third, the highest levels of unmet need were for those meeting DSM-IV criteria for conduct disorder. Fourth, the type of help parents felt was most needed was counselling for their child, while the highest level of unmet need was help with life skills. Fifth, children and adolescents with autism or an intellectual disability were identified by parents as having a high level of need for all types of help assessed in the study. Finally, a higher proportion of parents from blended families identified a need for counselling for their child.
First, our results showed that the majority of parents of 4- to 17-year olds meeting DSM-IV criteria for mental disorders (79%) thought that their child needed some type of help, more parents of adolescents (85.4%) than children (73.2%). A remaining one fifth of parents with children who met DSM-IV criteria for mental disorders reported no need for help (about 119,000 4- to 17-year-olds). This latter finding may partly reflect the level of severity of the disorder, as most parents reporting ‘no need’ for help had children with mild disorders. Both burden and severity are known to be stronger drivers of help-seeking (Angold et al., 1998; Boulter and Rickwood, 2013; Logan and King, 2001; Ryan et al., 2015; Zwaanswijk et al., 2003). Children meeting DSM-IV criteria for mental disorders whose parents reported no need for help also tended to be in families with more resources (higher income, more highly educated parents) and that faced fewer psychosocial challenges such as family disruptions and parental distress. Parents may have thought that the problem would get better or prefer to manage it themselves (Sayal, 2006), especially with younger children as previously identified in this sample (Lawrence et al., 2015). Nonetheless, although some disorders were classified to be of mild severity, these children had still met all DSM-IV diagnostic criteria, including clinically significant distress or impairment of functioning. As such, the child or family is still impacted by the disorder. Lack of proper clinical assessment even for mild disorders, may represent an important missed opportunity for early intervention, treatment and monitoring with integration across school and health services.
Second, we found higher and comparable levels of need for help for those meeting DSM-IV criteria for major depressive disorder and conduct disorder, and again this can be explained partly by the higher level of severity carried by these disorders relative to ADHD and anxiety disorders (Lawrence et al., 2015). This is consistent with results from adult surveys (Meadows and Burgess, 2009). Based on data from the US National Stigma Study-Children which measured public response to child mental health problems, it was found that the public had greater recognition of the need for professional help for children with symptoms associated with diagnostic criteria of depression than ADHD (Pescosolido et al., 2008). The authors also demonstrated a much higher level of mental health literacy in females as has been found among young Australians (Cotton et al., 2006). In our sample, more than 80% of primary carers were females. In the first national child and adolescent survey conducted in 1998, about 30% of parents of children with ADHD (either inattentive or hyperactive) thought that their child needed professional help of some kind; 46% if the child had both types of ADHD (Sawyer et al., 2004). This compares with about two-thirds of children meeting DSM-IV criteria for ADHD (either type) in this study having a need for counselling suggesting that there has been an increase in awareness and understanding in the community regarding the need for help for children with ADHD. Parental recognition of symptoms of mental disorders as distinct from behaviour that is normal at a particular developmental stage is a key first step towards clinical assessment. Based on our results, there is still a need to improve understanding in the community about symptoms of ADHD (and anxiety disorders) that are not developmentally normal and before problems become severe (Paulus et al., 2014).
Third, although parents identified a similar level of need, needs were most likely to be fully met when the young person met DSM-IV criteria for major depressive disorder, and least likely when meeting DSM-IV criteria for conduct disorder. While there are clinical guidelines and treatment pathways for depression in adults and children, the evidence base for the treatment of conduct disorder is limited. It is a much more difficult problem to treat and services are often not geared to provide the intensity of treatment required. Consequently, young people with conduct disorders fall between the gaps of school services, primary care and mental health services. Conduct disorder is also heterogeneous – comorbidity is common and therefore the most effective treatment will be one that is tailored to the child’s set of problems and circumstances (Brestan and Eyberg, 1998; Kazdin, 1997; Scott, 2008). Two-thirds of those in the survey meeting DSM-IV criteria for conduct disorder had met criteria for at least one other disorder – just under half with ADHD and over a third with either anxiety or depression (Lawrence et al., 2015). Reviews of interventions for conduct disorder conclude that evidence-based parenting, family and school-based interventions are among the most effective for treatment of conduct problems (Brestan and Eyberg, 1998; Kazdin, 1997; Scott, 2008). These reviews also suggest that medication is only effective for treatment of conduct disorder in certain cases, such as if comorbid with ADHD, although our results revealed a similar proportion of parents of children meeting DSM-IV criteria for conduct disorder as those meeting DSM-IV criteria for major depressive disorder thought that their child needed medication. There is a particularly high concentration of conduct disorder in disadvantaged families, more so than other disorders and therefore facing more complex needs and/or greater barriers to service access (Lawrence et al., 2015). These families are more likely to drop out of treatment (Scott, 2008). Data from longitudinal studies show that conduct problems in childhood (including oppositional defiant disorder) are one of the most reliable predicators of mental disorders in adulthood across a spectrum (Copeland et al., 2010; Kim-Cohen et al., 2003).
Fourth, counselling was the most common type of help parents said was needed. In the context of this survey, this included any type of therapy delivered at schools, community services or private practice. In Australia, greater access to individual counselling from mental health professionals has been facilitated by initiatives such as the Better Access Program with increased use of Medicare-funded mental health services by children and adolescents since its introduction in 2006 (Department of Health and Ageing, 2013), as well as the Access to Allied Psychological Services (ATAPS) programme which has also seen increasing rates of services delivered to children (Bassilios et al., 2016). The level of completely unmet need for counselling was greatest among those with mild disorders, and by disorder, for those meeting DSM-IV criteria for ADHD. Children whose disorders have a lower level of impact on their functioning and across domains may be less likely to be referred by a general physician (GP) for counselling under such programmes. In the study by Sawyer and colleagues, less than one fifth of young people with ADHD of any type had received counselling services, and of those that had, over half requested additional counselling (Sawyer et al., 2004). These findings suggest that despite an increase in accessibility and affordability of counselling services, a large proportion of young people with mental disorders have a need for either initial assessment or only a partially met need for ongoing care.
The greatest disparity between a need for care being identified by parents and needs being met was in respect of preventative programmes or counselling to build life skills, self-esteem or motivation. There have been significant investments made over the last 15 years in school-based mental health literacy programmes such as KidsMatter and MindMatters, although uptake has been inconsistent (Department of Health and Ageing, 2013). It is likely that the increasing presence of such programmes in schools has increased awareness among parents. In multivariate models, parental perceived need for life skills training was associated with living in the most advantaged areas (fifth quintile), and this may be because of greater availability of such programmes in more advantaged schools and communities. At present, schools volunteer for participation in these programmes. Furthermore, for young people who have already developed disorders, especially when they are severe, the school may not be able to offer adequate intervention for positive wellbeing and resilience. As 60% of those identifying a need for life skills had completely unmet need for this type of help (approximately 123,000, 4- to 17-year-olds), the implications for greater funding in schools and the community is evident. The multivariate analysis also showed that if a child had been bullied, parents were twice as likely to report that their child needed support with building life skills and self-esteem, and additionally, the need for this type of help was associated with anxiety or depression but not externalising disorders. Greater need among these children is an important point to consider in the context of mental health services and schools offering broader mental health literacy or anti-bullying programmes.
Fifth, one of the most consistent factors associated with need for information, or medication or counselling was if the child also had autism or an intellectual disability – affecting one-fifth of those meeting DSM-IV criteria for mental disorders in this sample, and higher still if meeting criteria for an ADHD diagnosis. This represents a substantial number with specialist needs (about 107,000 4- to 17-year-olds), although Australian research shows that only a small proportion of children with intellectual disability comorbid with mental health problems received specific mental health interventions, and problems were persistent over the 14-year follow-up (Einfeld et al., 2006).
Finally, we found a greater need for help for children meeting DSM-IV criteria for mental disorders in blended families, in particular for counselling which partly corresponds with Ryan and colleagues findings, although they concluded there was a greater need in lone parent and reformed families having adjusted for mental health problems (Ryan et al., 2015). It is difficult to explain why the significant effect might remain in respect to blended families, rather than step or lone parent families where adjustment for other factors accounted for the greater need for help for children with mental disorders in these families. According to the ABS family blending classification as adopted in this study, blended families are those who have two or more children, of whom at least one is the natural or adopted child of both parents, whereas step families have no natural or adopted children of both parents. Prior research on family structure and mental disorders in YMM showed no difference in the prevalence of mental disorders in blended families according to whether the child had one or two parents (Perales et al., 2017). Future research that explicitly examines the family circumstances, dynamics and needs of young people with mental disorders in blended families is warranted to shed light on these findings.
Limitations
When examining perceptions about the degree to which needs have been met, it is not possible to tell how much of a service a young person has received or still needed. It could just be an initial assessment or a number of visits but the parent has perceived a need for ongoing care. As the informant for mental disorders and perception of need for help is the same – parents and carers – this may have overstated proportions of parents thinking that their child needed help. The young person themselves may feel and/or think differently or indeed sought help without their parent being aware.
Conclusion
Parent perceptions of need for mental health services for their child are an important source of information for guiding service planning and development. While the majority of young people have their needs fully or partially met, there are still substantial numbers with completely unmet needs, especially for counselling. There was a particularly high level of unmet need for those meeting DSM-IV criteria for conduct disorder. Results suggest that even though a large number may be in touch with services, for a considerable proportion, these services may not be providing an adequate level of care.
Footnotes
Acknowledgements
The authors would like to thank the 6310 families that gave their time to participate in the survey, Rajni Walia, Gerry Bardsley, and the team at Roy Morgan Research and the Young Minds Matter Survey Reference Group for their input into the design and conduct of the survey. S.J. and S.Z. are supported by the Australian Research Council Centre of Excellence for Children and Families over the Life Course (project number CE140100027). The views expressed herein are those of the authors and are not necessarily those of the Australian Research Council.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The second Australian Child and Adolescent Survey of Mental Health and Wellbeing was funded by the Australian Government Department of Health. Young Minds Matter was funded by the Australian Government Department of Health. Data collection was undertaken by Roy Morgan Research.