
Abstract
Background:
Concerns about low levels of service utilisation for mental and substance use disorders in Australia – especially among males – have prompted targeted help-seeking and stigma-reduction initiatives. Resulting changes in service utilisation according to gender are unknown. We modelled the percentage of Australian males with a mental or substance use disorder who used services each year between 2006–2007 and 2011–2012, and the types of services they used, relative to females.
Methods:
Twelve-month prevalence of mental and substance use disorders, stratified by gender, was synthesised from existing estimates. The percentage of males and females with these disorders who used mental health services in each year from 2006–2007 to 2011–2012 was modelled from published programme activity data, supplemented by analyses of epidemiological survey data. Uncertainty analysis quantified the effects of sampling error and assumptions on the estimates.
Results:
Modelling showed a significant increase in the percentage of people with mental or substance use disorders who used services for their mental health – from 32.0% in 2006–2007 to 40.0% in 2011–2012 in males and from 45.1% in 2006–2007 to 54.6% in 2011–2012 in females. Growth was driven largely by uptake of private specialised services – males’ use of these services grew by 92.7% and females’ by 115.4%. There appeared to be a non-significant decrease in use of general practitioner-only mental health care for males (−17.9%), and a significant decrease in the same for females (−35.1%); however, some assumptions made in the modelling of general practitioner-only care require validation. In 2006–2007, the percentage of females treated was 40.9% higher than for males; in 2011–2012, it was 36.6% greater.
Conclusions:
Recently implemented initiatives have improved males’ likelihood of service utilisation, particularly their use of specialised mental health services. Although the gender gap may have narrowed, improving males’ access to services should remain a policy priority.
Introduction
A significant proportion of the burden associated with mental and substance use disorders is avertable with existing therapies (Andrews et al., 2004) but, in developed countries, less than half of people with these disorders will seek professional help in a given year (Burgess et al., 2009; Wang et al., 2005). Attempts to understand the patterns of, and reasons for, low treatment coverage in the general population have consistently demonstrated shortfalls in service utilisation among males relative to females.
In Australia in 2007, males with a mental or substance use disorder were about one-third less likely than females to consult health professionals for their mental health in the previous year (27.5% vs 40.7%). They were 40% less likely to consult general practitioners (GPs; 18.0% vs. 29.9%) or non-mental health professionals (4.7% vs 8.0%). With respect to mental health professionals, the percentage of males consulting psychologists was equivalent to females (13.1% vs 13.2%), but was 11% lower for psychiatrists (7.5% vs 8.3%) and 18% lower for other mental health professionals (6.9% vs 8.4%; Australian Bureau of Statistics [ABS], 2008). Broadly, these patterns mirror findings from other developed countries (e.g. Dezetter et al., 2013; Gagne et al., 2014; Wang et al., 2005).
In Australia, as elsewhere, public concerns about poor treatment coverage have prompted targeted help-seeking and stigma-reduction initiatives. Two major programmes were introduced to improve access to evidence-based mental health interventions provided by specialists for the entire population – in 2001, the Access to Allied Psychological Services (ATAPS) programme (Bassilios et al., 2013) and, in late 2006, the Better Access to Psychiatrists, Psychologists and General Practitioners through the Medicare Benefits Schedule (MBS; Better Access) programme (Pirkis et al., 2011). The key feature of these programmes is the provision of a capped number of free or low cost psychological services provided mainly by psychologists, social workers and occupational therapists, following referral from a medical provider (usually a GP). Information-based initiatives such as beyondblue were introduced to improve mental health literacy and mental health service demand (Jorm, 2011).
Alongside these broader reforms, concerns about gender differentials in help-seeking and mental health literacy have sharpened the focus on men’s mental health needs. Australia’s National Male Health Policy identifies men as a hard to reach and underserviced group in primary mental health care (Department of Health, 2010). Men are also identified as a priority population in most Australian suicide-prevention policies (e.g. Department of Health and Ageing, 2007; NSW Department of Health, 2010), reflecting the higher rate of suicide in men (ABS, 2013b). Investment in government-funded male mental health initiatives, including Australian Men’s Shed Association (www.mensshed.org), the Older Men’s Network (www.tomnet.org.au) and the Men’s’ Health Information and Resource Centre (www.uws.edu.au/mhirc), has increased. In the not-for-profit sector, organisations such as beyondblue (www.beyondblue.org) and Movember (www.movember.com) have implemented efforts to improve males’ help-seeking and perceptions of stigma surrounding people with mental disorders.
Whether service utilisation for males with mental and substance use disorders has improved in response to these efforts is challenging to determine. Nationally representative mental health surveys are conducted infrequently, and there is no single, authoritative source of mental health service utilisation data that takes into account all disorders across all age groups. To overcome these limitations, Whiteford et al. (2014) modelled changes in population treatment rates in Australia from independent datasets describing the utilisation of various mental health programmes and service types. They estimated that the percentage of Australians with mental and substance use disorders who used services for their mental health increased by 23% between 2006–2007 and 2009–2010 (from 37% to 46%), primarily as a result of increased access to allied mental health care via the Better Access programme. However, these estimates are now several years old and were not produced separately for males and females.
The aim of this study was to estimate changes in the percentage of male and female Australians with mental or substance use disorders who used mental health services each year between 2006–2007 and 2011–2012, and differentials between the genders in the types of services used. We applied similar methods and assumptions as in a previous study (Whiteford et al., 2014) but did so over a longer time period and incorporating gender-specific estimates and additional programme data to improve precision.
Method
Design and data sources
We conducted a four-step modelling exercise drawing on multiple data sources, including published administrative data routinely collected by mental health services, published evaluation studies and purpose-designed analyses of epidemiological survey data. For each step in the modelling, Table 1 shows the primary data sources, the estimates derived from each and their main strengths and limitations as relevant to this study. The modelling procedure is explained below, with additional detail in the online Supplementary Tables. The University of Queensland Behavioural and Social Sciences Ethical Review Committee approved the study.
Primary data sources a used and the estimate(s) derived in each step of the modelling.
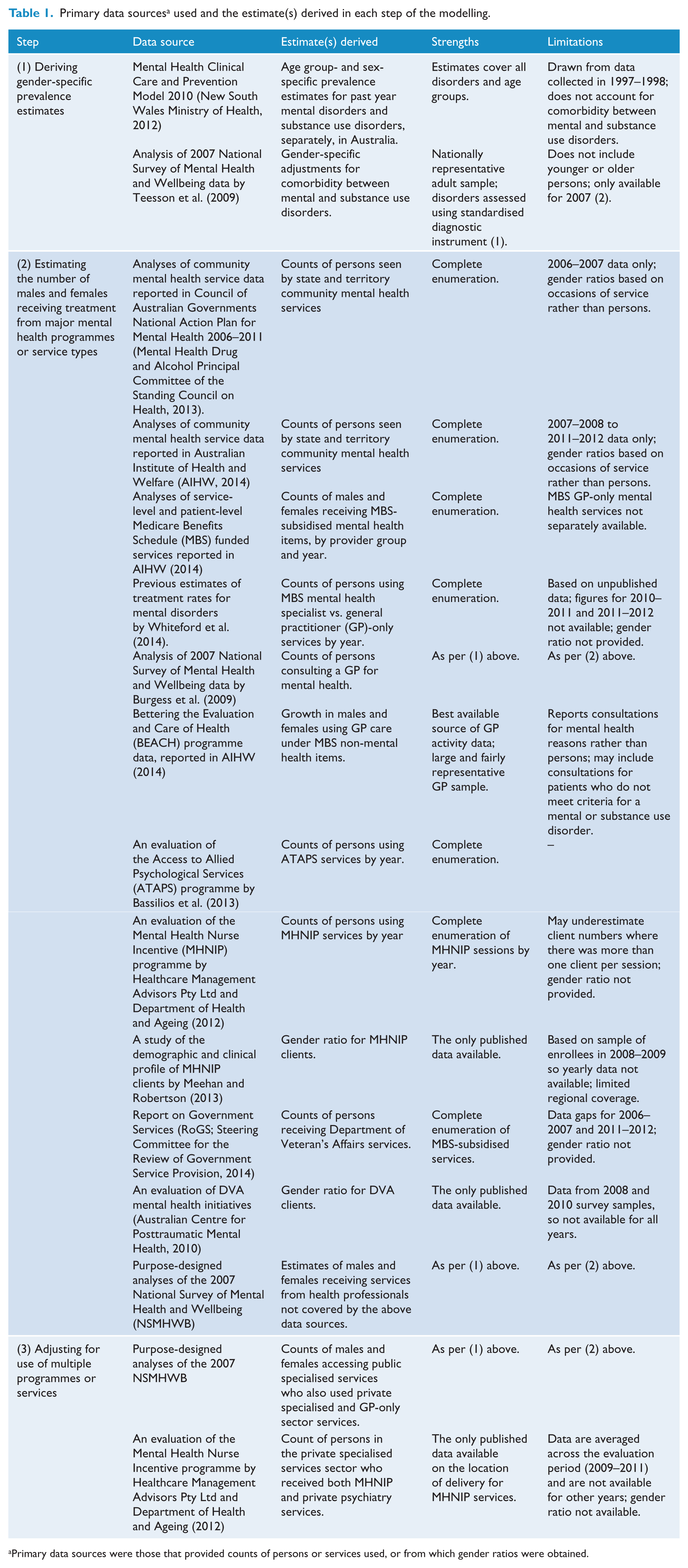
Primary data sources were those that provided counts of persons or services used, or from which gender ratios were obtained.
Steps in the modelling procedure
Deriving gender-specific prevalence estimates
The first step involved quantifying the percentage of Australians with a past year mental disorder or substance use disorder for each year 2006–2007 to 2011–2012. Although psychiatric epidemiological surveys have been conducted in Australia (Department of Health and Ageing, 2013: 18), they do not cover all age groups (e.g. children under 4 years, people aged 65 or over in hospitals or residential aged care facilities) and disorders (e.g. eating disorders and personality disorders). To overcome this, we sourced comprehensive age- and sex-specific Australian prevalence estimates from the Mental Health Clinical Care and Prevention Model 2010 (MH-CCP 2010; New South Wales Ministry of Health, 2012). MH-CCP 2010 estimates are drawn largely from the Australian Burden of Disease study (Begg et al., 2007) which combined data from Australian psychiatric epidemiology surveys conducted 1997–1998 with estimates from overseas studies to fill gaps in the Australian evidence base, to produce overall prevalence estimates.
Because MH-CCP 2010 prevalence estimates are provided separately for mental disorder and substance use disorders, we applied an adjustment based on previous findings that 38.6% of adult Australian males aged 16–85 years and 48.5% of same-aged women with substance use disorders have at least one co-occurring affective or anxiety disorder (Teesson et al., 2009). In the absence of other suitable estimates, this adjustment was applied to all age groups. The number of prevalent cases in each year was calculated by applying the prevalence estimates to the estimated resident population in each year (ABS, 2013a), based on evidence that the prevalence of mental disorders in the Australian community is unlikely to have changed much over time (Jorm, 2011).
Estimating the number of males and females receiving treatment from major mental health programmes or service types
The second step involved determining the number of Australians who used mental health services in each year of interest (Note that ‘mental health services’ include services providing treatment to people with mental health and or substance use problems). Because there is no single source of mental health service utilisation data, we assembled estimates from independent data sources describing the utilisation of major mental health programmes or service types nationally, supplemented by additional sources or assumptions as required.
State and territory mental health services
Counts of persons seen by state and territory community mental health services were sourced from Council of Australian Governments National Action Plan for Mental Health 2006–2011. Final Progress Report covering implementation to 2010–2011 (Mental Health Drug and Alcohol Principal Committee of the Standing Council on Health, 2013) for 2006–2007 and Mental Health Services in Australia (MHSA) (AIHW, 2014) for 2007–2008 to 2011–2012. Data for Victoria were adjusted to national average per capita rates to account for its higher threshold for recording a ‘case’ (Department of Health and Ageing, 2013: 165). Person counts were not available by gender, so were apportioned using the ratio of male-to-female community mental health occasions of service in each year (excluding Victorian counts), based on evidence that the gender ratios for persons seen and occasions of service are similar (Short et al., 2010). We assumed that most people using state and territory inpatient mental health services would have also received community mental health services. People in hospital for more than 1 year may not have had community contact in a given year, but their number was considered negligible (Whiteford et al., 2014).
MBS-subsidised mental health services – specialist versus GP-only
Medicare subsidises a range of mental health coordination and treatment services provided by GPs and mental health specialists. MHSA (AIHW, 2014) provides counts of males and females receiving MBS mental health services in each year, overall and separately for GPs and for each of three specialist provider groups (psychiatrists, psychologists and other allied health professionals; AIHW, 2014). Published MBS data do not contain information on whether GP mental health services were GP-only (i.e. a GP was consulted for mental health in a given year, but not one of the specialist providers named above) or whether specialists were seen as well. However, estimates for 2006–2007 to 2009–2010 were available from a previous study (Whiteford et al., 2014) that used internal government data. As the proportion was relatively stable over time, we applied the 2009–2010 proportion to 2010–2011 and 2011–2012. Then, persons using MBS specialist mental health services were apportioned to males and females using the average of the reported gender ratios for the psychiatrists, psychologists and other allied health groups, and persons using GP-only MBS mental health services were apportioned to males and females using the reported gender ratio for all GP MBS mental health services (AIHW, 2014; see Supplementary Table 2 footnote (c)).
Other GP-only mental health care
Data from the Bettering the Evaluation and Care of Health (BEACH) survey of GPs indicate that the majority of mental health-related consultations provided by GPs are billed using MBS general consultation items rather than mental health items (Britt et al., 2013). However, BEACH data count consultations rather than persons, and may include consultations for persons who have symptoms but do not meet criteria for a mental or substance use disorder. Consequently, we adapted a previously developed method (Whiteford et al., 2014) to obtain estimates of GP-only care provided under non-mental health MBS items for males and females with mental and substance use disorders. Briefly, we used BEACH data to obtain the gender ratio and per capita growth in GP mental health encounters for males and females for all years of interest (AIHW, 2014). Because BEACH data may include persons who do not meet criteria for a 12-month mental disorder, we took the estimated total number of persons with a mental or substance use disorder who had seen a GP in the past 12 months for their mental health in 2006–2007 from the National Survey of Mental Health and Wellbeing (NSMHWB) as a baseline and applied the BEACH gender ratio for that year. For each subsequent year, the 2006–2007 estimates were adjusted for population growth and for growth in GP encounters. The estimated number of people treated by GPs not under MBS mental health-specific items was calculated by subtracting the number of people receiving MBS-subsidised GP mental health services from the total number receiving GP services (Supplementary Table 3).
ATAPS
The numbers of males and females receiving ATAPS psychological services in each year were obtained from an ATAPS evaluation report covering July 2003 to December 2012 (Bassilios et al., 2013). These data represent virtually complete enumeration of ATAPS users.
MHNIP
Enumeration of persons receiving Mental Health Nurse Incentive Program (MHNIP) nurse sessions, in each year since the programme’s implementation in 2007, was obtained from an evaluation report; this may underestimate persons seen as case studies indicate that not all nurses record every patient contact where they support more than two patients per session (Healthcare Management Advisors Pty Ltd and Department of Health and Ageing, 2012). The gender ratio (58% female:42% male) was drawn from a study of 309 MHNIP clients enrolled between June 2008 and December 2009 in one region in Queensland (Meehan and Robertson, 2013). In the absence of further information, this gender ratio was applied across all years.
DVA
Total number of persons using Department of Veterans Affairs (DVA) services was obtained by calculating the difference between the total number of people receiving GP, psychiatrist or allied health professional mental health services funded under the MBS or DVA (from the Report on Government Services [RoGS]; Steering Committee for the Review of Government Service Provision, 2014) and people receiving these services funded by the MBS (from MHSA; AIHW, 2014). Data for 2006–2007 and 2011–2012 were assigned the average annual person count for 2007–2011 due to lack of RoGS data for 2006–2007 and inconsistencies between data published in the RoGS and MHSA reports for 2011–2012. The gender ratio (87.8% male) was calculated from an evaluation of DVA mental health initiatives (Australian Centre for Posttraumatic Mental Health, 2010) and applied across all years (see Supplementary Table 2 footnote (g)).
Other mental health providers and other health providers
Persons not receiving any of the services in (a)–(f) but who saw a mental health specialist (psychiatrists, mental health nurses, psychologists or specialist allied health providers) funded solely through private health insurance, consumer full out-of-pocket payment or another means (but not via the MBS or public sector services) in 2006–2007 were calculated from the NSMHWB (3.8% of those with mental or substance use disorders; 49.7% males and 50.3% females). Persons using other health providers (other medical practitioners, allied health professionals in generalist settings or complementary or alternative medicine providers), but no GP or mental health professional, for their mental health in 2006–2007 was calculated from the NSMHWB (1.6% of those with mental or substance use disorders; 17.1% males and 82.9% females). The estimates were applied to the prevalence data for each year from MH-CCP 2010 to obtain counts of males and females. In the absence of further information, we assumed no change since 2006–2007.
Adjusting for use of multiple programmes or services
The third step involved aggregating the counts of males and females seen by the various mental health programmes or service types in Step 2 up to one of four mutually exclusive, hierarchically ordered mental health service ‘sectors’: public specialised services, private specialised services, GP-only services and other health professional only services. Before doing so, adjustments were applied to prevent double counting of individuals treated in more than one sector. The main adjustments involved accounting for overlap in the use of state and territory-funded mental health services and mental health specialists or GP services, reducing the counts of persons receiving GP-only services to allow for persons using mental health specialists via programmes such as ATAPS and MHNIP and reducing counts of persons in the private specialised services sector who received both MHNIP and private psychiatry services (see Supplementary Table 4 for details).
Modelling uncertainty
Modelling exercises such as this may be subject to uncertainty due to sampling error arising from the use of sample-based data (such as the NSMHWB), and error arising from possible misclassification, incomplete coverage or double counting. To account for this, uncertainty analyses were conducted in Microsoft Excel, using the Ersatz Monte Carlo simulation add-in (EpiGear, 2012). For estimates we considered most subject to uncertainty, an appropriate distribution was specified, along with credible parameters indicating the lowest, most likely and highest values based on information about sampling error or other known constraints (see Supplementary Table 5 for details). Uncertainty around individual parameters was carried forward from each step to be considered simultaneously. We drew from the distributions 2000 times to arrive at 95% uncertainty intervals around the final model estimates.
Statistical analyses
Descriptive statistics from the 2007 NSMHWB Basic Confidentialised Unit Record File (CURF; April 2009 version) data were generated using Stata version 11 (StataCorp, 2009). Data were weighted to account for the differential probability of survey selection and to match known population distributions. Percentages and 95% confidence intervals (CIs) were calculated using jackknife repeated replication to accommodate the complex survey design.
Results
The estimated 12-month prevalence of mental or substance use disorders, adjusted for comorbidity, was 20.4% for males and 19.5% for females. Unadjusted estimates showed that substance use disorders were more prevalent among males than females (9.5% vs 3.2%), and mental disorders were less prevalent (14.6% vs 17.9%; Supplementary Table 1).
Figure 1 shows the percentages of males and females being treated by the main mental health-specific programmes or service types for which data were available, and how these changed between 2006–2007 and 2011–2012. Individuals may have used more than one type of programme or service. The percentage change in the use of almost all programmes or service types was larger for males than females. Uptake of MHNIP services overall grew sharply since the programme’s introduction in 2007, although relative growth between males and females could not be modelled due to lack of data. The exception was non-MBS GP-only mental health services; use of these services declined although the pattern of change was not linear for males. Change in persons using services provided by DVA, other mental health professionals and other health professionals could not be modelled due to lack of data (see Supplementary Tables 2 and 3 for further detail).
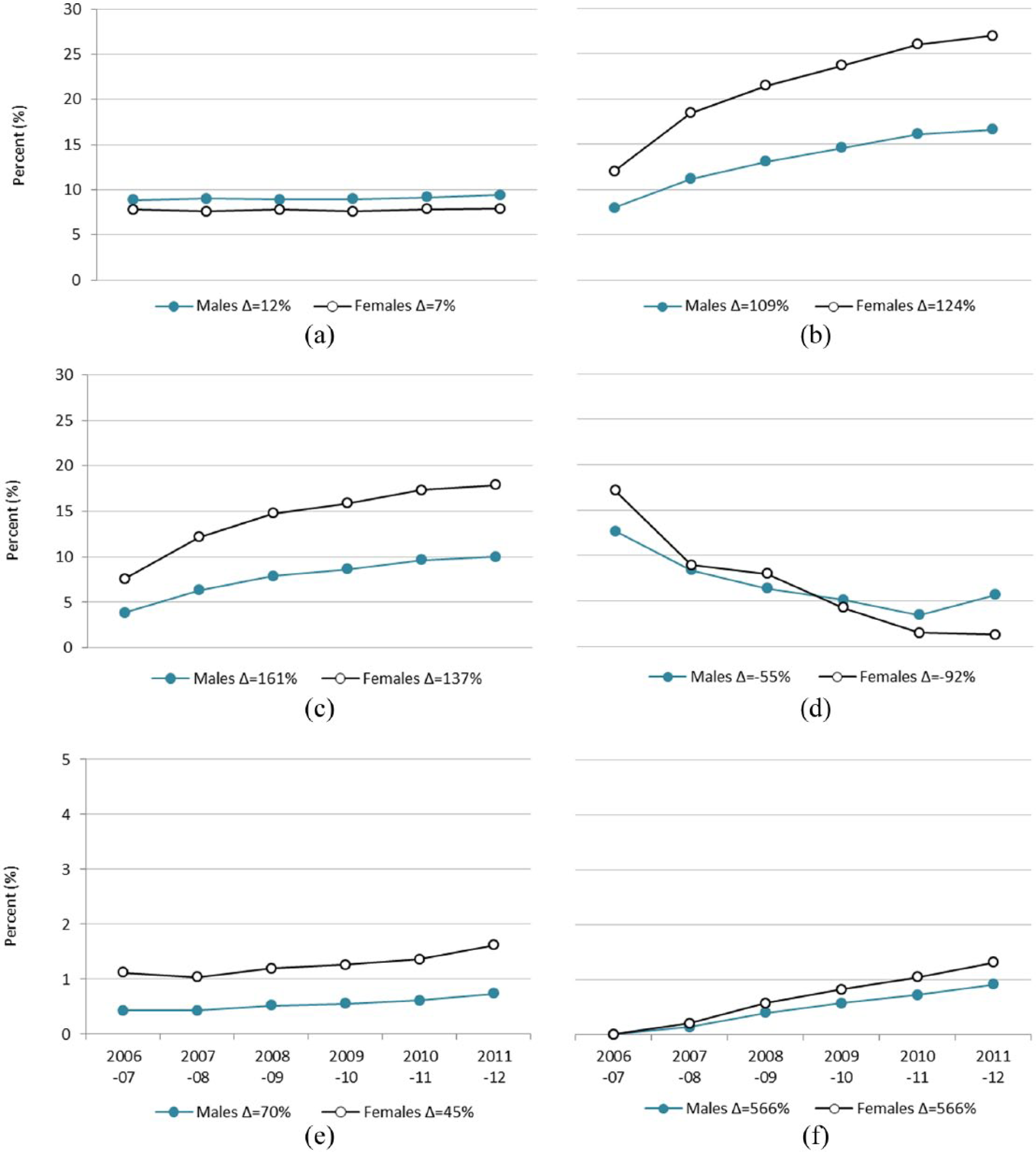
Percentage of males and females with a mental or substance use disorder using services for their mental health, by programme or service type, 2006–2007 to 2011–2012: (a) state and territory mental health services, (b) MBS psychiatry/allied health services, (c) GP-only MBS mental health services, (d) GP-only non-MBS mental health services, (e) Access to Allied Psychological Services (ATAPS) and (f) Mental Health Nurse Incentive Program (MHNIP) services.
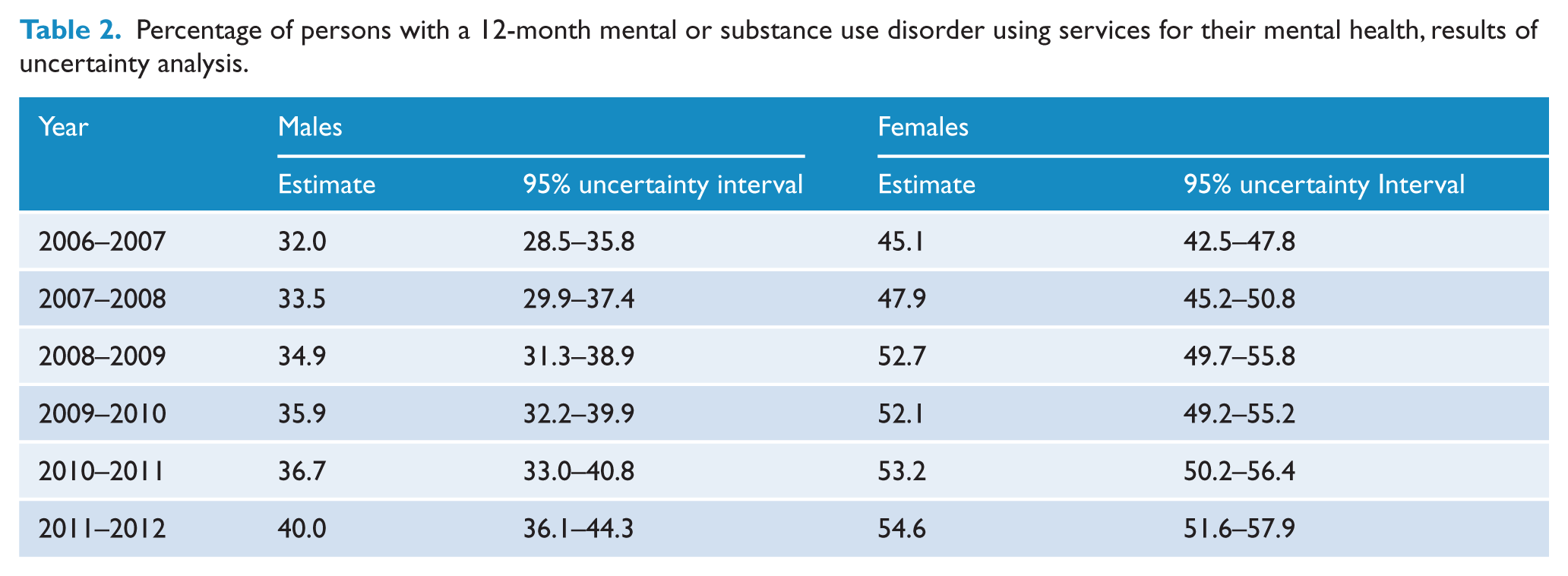
The primary results of the uncertainty modelling are shown in Table 1 (and Supplementary Table 4). Non-overlapping uncertainty intervals indicate significant differences between estimates (Schenker and Gentleman, 2001). Between 2006–2007 and 2011–2012, the estimated percentage of Australians with mental or substance use disorders who used mental health services increased significantly, from 32.0% to 40.0% for males and from 45.1% to 54.6% for females. This equates to overall growth of 25.0% for males and 21.2% for females. In all years considered, the percentage treated was significantly higher for females than males, but the gap between males and females appears to have narrowed slightly. In 2006–2007, the percentage of females treated was 40.9% higher than for males; in 2011–2012, it was 36.6% greater.
Secondary results from the uncertainty modelling (Tables 2 and 3 and Figure 2) indicate that a significantly greater percentage of males than females used public specialised services in all years considered, but the observed growth was not significant for either gender. A significantly lower percentage of males used private specialised services than females in all years considered, and use of these services approximately doubled for both genders. A significantly lower percentage of males used GP-only services than females in all years considered except 2011–2012. Use of these services decreased significantly for females; they also decreased significantly for males between 2006–2007 and 2010–2011 but increased again in 2011–2012.
Percentage of persons with a 12-month mental or substance use disorder using services for their mental health, results of uncertainty analysis.
Percentage of persons with a 12-month mental or substance use disorder using services for their mental health in four mutually exclusive, hierarchically ordered ‘sectors’, results of uncertainty modelling.
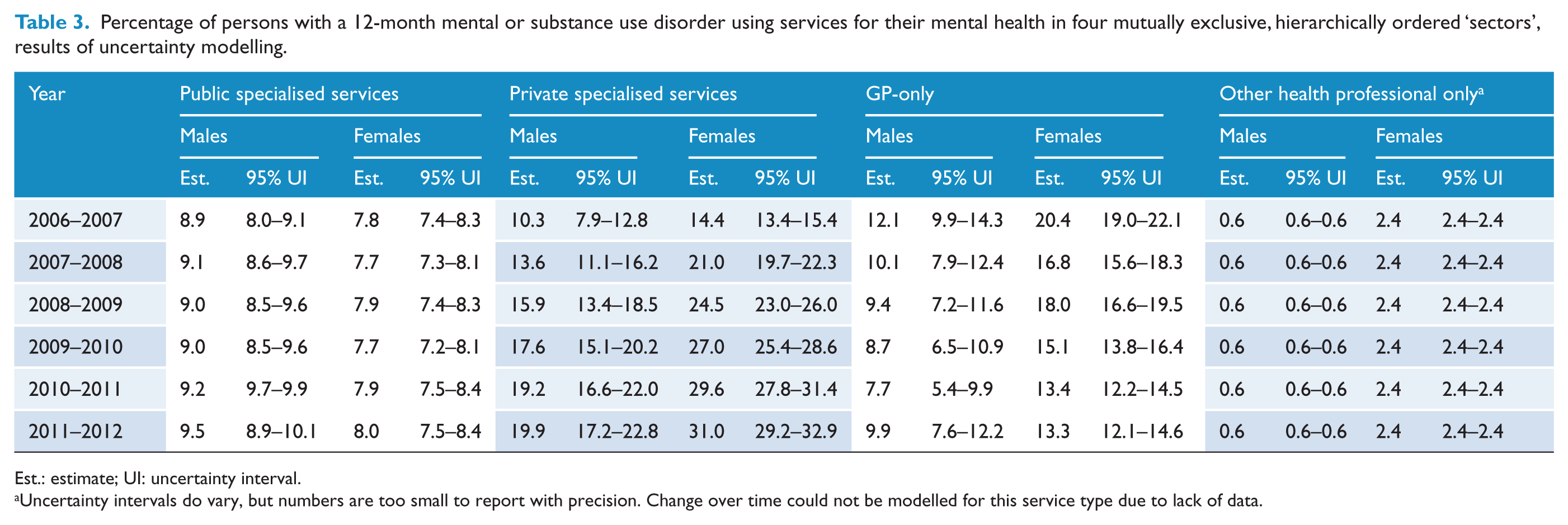
Est.: estimate; UI: uncertainty interval.
Uncertainty intervals do vary, but numbers are too small to report with precision. Change over time could not be modelled for this service type due to lack of data.
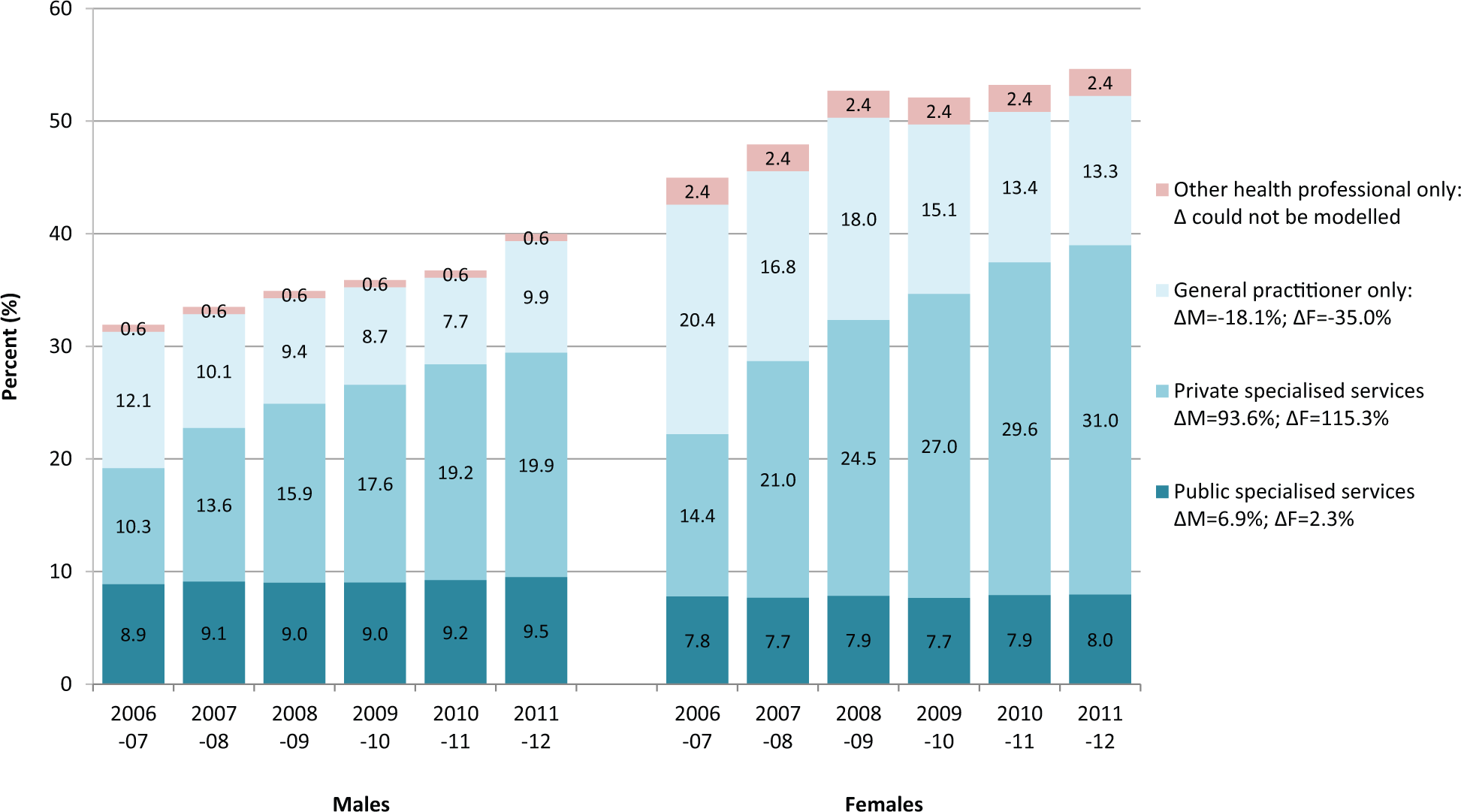
Estimated percentages of Australian males and females with a mental or substance use disorder using services for their mental health in four mutually exclusive, hierarchically ordered mental health service ‘sectors’, 2006–2007 to 2011–2012.
Discussion
This paper extends previous findings of significant growth in service utilisation for mental or substance use disorders in Australia 2006–2007 (Whiteford et al., 2014). It contributes three new findings. First, we estimated that one-quarter (25.0%) more males and one-fifth more females (21.2%) used services for a mental or substance use disorder in 2011–2012 than they did in 2006–2007. Second, the use of specialised private services approximately doubled for both genders but less so among males than females (92.7% vs 115.4%), whereas the use of GPs as the sole provider of mental health care decreased but less so for males than females (−17.9% vs −35.1%). Third, although proportionally fewer males than females used services in each year, the stronger overall growth in the percentage of males receiving services appears to have resulted in a modest narrowing of the gender gap.
Limitations
Several potential limitations should be taken into account. Gender-specific prevalence estimates were synthesised from multiple sources, but were similar to those reported from the 2007 NSMHWB (Slade et al., 2009; Teesson et al., 2009), the best available comparison. The 2006–2007 service use estimates in the current study were somewhat higher than those from the 2007 NSMHWB – males: 27.5% (95% CI = [21.0, 34.0]); females: 40.7% (95% CI = [36.0, 45.3]) (Burgess et al., 2009) – although within the bounds of the 95% CIs. This might be expected because the 2007 NSMHWB included only affective, anxiety and substance use disorders and did not include other disorders, some of which (e.g. schizophrenia and other non-affective psychoses) have considerably higher service utilisation rates (Andrews and the Tolkien II Team, 2007).
Counts of persons using some mental health programmes and service types were not available; however, we considered their impact on our estimates is likely to be small. For example, we did not have data on people using mental health community support services provided by non-government organisations (NGOs) but assumed that most would have been seen by a clinical service provider captured elsewhere in the modelling (Whiteford et al., 2014). This assumption is broadly supported by data from the 2010 Survey of People Living with Psychotic Illness which showed that, of those seen solely by NGOs in the preceding month (n = 205/1825), 54% had had a community mental health service contact and 61% had consulted a GP for their mental health in the past 12 months (Raudino et al., 2014). Similarly, counts of people treated in private psychiatric hospitals were not available; however, individuals admitted to these hospitals must be under the care of a medical practitioner (almost always a psychiatrist) so it is reasonable to assume that they would be counted in the counts of persons using MBS-subsidised psychiatrist or GP services. People receiving services from headspace centres were assumed to have utilised MBS mental health items. People accessing specialised drug and alcohol services were likely to be captured by the NSMHWB analysis which recorded other mental health professionals and other health providers not covered by state and territory mental health services or the MBS. We did not have person-level data on emergency department (ED) presentations among people with mental disorders. Males use twice as many mental health-related ED presentations as females, although this preponderance did not change between 2006–2007 and 2010–2011 (AIHW, 2014).
We relied primarily on publicly available data sources and applied assumptions, where required, to overcome gaps in available data. This resulted in uncertainty for some estimates. Notably, our methods for deriving year- and gender-specific counts of persons using non-MBS GP-only services, and adjusting to avoid double counting of people receiving ATAPS and MHNIP services, require validation. The precision of these estimates could be improved with access to more detailed reports or direct source data. Collection methods for state and territory mental health services vary and adjustment was made for one known difference, relating to the exclusion of ‘assessment only’ cases in Victoria. We estimated that approximately one-third of males and one-quarter of females receiving state and territory services were also receiving other services in 2007 (based on the NSMHWB); however, we do not know whether patterns of overlap have changed over time. Addressing this problem requires either common information systems employing unique patient identifiers or record linkage studies.
It was beyond the scope of this study to estimate changes in gender-specific treatment patterns according to disorder type. This is a question of interest given that males are more likely than females to have substance use disorders – either alone or in combination with mental disorders (Teesson et al., 2009) – which are associated with poorer health service utilisation (Burgess et al., 2009). A future iteration of the NSMHWB may enable this. It was also beyond the scope of the study to examine regional variability in service use patterns. Although it is likely that increases in service use are linked to various mental health initiatives, studies such as this cannot establish causation and other demographic, social and cultural changes may also play a role.
Implications
Findings from this study have implications for policy and research. First, on a positive note, the significant increase in the percentage of males receiving treatment for mental and substance use disorders was mostly due to programmes enabling greater referral to, and uptake of, services provided by mental health specialists (i.e. Better Access programme, ATAPS and the MHNIP). That said, growth in males’ use of private specialised services (93% between 2006–2007 and 2011–2012) was exceeded by growth in females’ use of these services (115%). This indicates a continued need to supplement whole-of-population initiatives to improve access to specialised care with initiatives targeted specifically to males to ensure equitable gains.
Second, modelling indicated a possible reduction in males’ reliance on GP-only mental health care; this appears to be driven by the reduction in persons using non-MBS GP-only mental health services. BEACH data support this finding, showing that the proportion of GP encounters for mental health not billed under the MBS mental health items has decreased and that the proportion of encounters resulting in referrals to specialists has increased (Britt et al., 2013). On one hand, this is a positive change. The 1997 NSMHWB showed that 29% of adults with affective, anxiety and substance use disorders had consulted only a GP for mental health care in the previous 12 months (Meadows et al., 2001). These findings informed the design of Better Access and other new initiatives aimed at providing better referral avenues for GPs and/or improving support for them to provide mental health care. On the other hand, we found that males continue to be less likely than females to consult GPs for mental health reasons, a concern given that GPs are the point of referral to mental health specialists in many instances.
A number of strategies have been suggested to encourage males to consult GPs. For example, targeted information initiatives that focus on changes in functioning rather than symptoms may be useful, given evidence that males with affective and anxiety disorder have greater levels of disability than their female peers and that males may be less willing to discuss emotional concerns with GPs (Scott and Collings, 2010). Being employed has been identified as a barrier to GP consultation for mental health in males in some studies (e.g. Tedstone Doherty and Kartalova-O’Doherty, 2010), highlighting the workplace as a valuable setting for engaging men in health care (Malcher, 2009). Given that three-quarters of males with mental health concerns will consult a GP for physical health reasons in a given year (Parslow et al., 2011), tools such as prompts and checklists may improve GPs’ ability to efficiently detect mental health problems among male attenders (Brownhill et al., 2003) although the potential for increasing the duration of consultation may be a limiting factor (Parslow et al., 2011). Tailoring appointment procedures and the physical environment of GP practices according to men’s preferences has also been suggested (Malcher, 2009).
Third, as already noted, the observed patterns of service use may indicate that new models of care (e.g. Better Access, ATAPS and the MHNIP) are filling a gap in demand for mental health care among males who previously wanted services but did not access them, for example, because the desired services were too costly or they preferred tomanage themselves (Harris et al., forthcoming article). Itis also likely that efforts to improve population mental health literacy (Jorm et al., 1997) and reduce stigma have contributed to increased service use. Stigma-reduction and mental health promotion are now central features of mental health policies and programmes in Australia (Department of Health and Ageing, 2009). Such programmes aim to facilitate early treatment seeking by improving recognition of mental disorder signs and symptoms, knowledge of appropriate treatments and minimising the impact of stigma as a barrier to help-seeking. Mental health literacy surveys have revealed improvements in the public’s recognition of signs and symptoms of mental disorders between 1995 and 2011, particularly depression, and beliefs about the helpfulness of mental health interventions have moved closer to those of health professionals (Reavley and Jorm, 2012). Whether these improvements have been equivalent for males and females is unknown. Furthermore, the vignettes used in these surveys have tended to focus on mental disorders; we know less about mental health literacy in regard to substance use disorders. Given the poor treatment rates for people with substance use disorders, especially where they are not comorbid with a mental disorder (Burgess et al., 2009), further research in this area is indicated.
Fourth, these findings have implications for the development of mental health policies. Although males’ mental health needs feature in broader health and suicide-prevention policies in Australia, most mental health policies do not emphasise gender differences and those that do tend to highlight the needs of women. Future consideration could be given to including a policy focus on overcoming male-specific barriers to help-seeking, including traditional constructions of masculinity (Moller-Leimkuhler, 2002), comorbidity and low rates of help seeking for substance use disorders. The latter tends to be associated with higher levels of stigma and a perception of greater personal responsibility than for mental disorders such as depression and anxiety (Glass et al., 2014). This focus could, in turn, also inform the mental health content of broader male health policies and suicide prevention policies.
Fifth, at 40%, the percentage of males with mental or substance use disorders estimated to have used servicesfor their mental health in 2011–2012 sits well below proposed targets for the total Australian population. Experts have suggested that providing good quality treatment to between 60% and 67% of people with mental and substance use disorders (Andrews and the Tolkien II Team, 2007; Hickie et al., 2005) is feasible. It was beyond the scope of this study to investigate the quality of treatment received. However, in high-income countries, no more than 50%of people consulting a health professional for mental or substance use disorders receive treatment consistent with practice guidelines (e.g. Lora et al., 2011; Wang et al., 2007). Most studies have found no gender differences in mental health treatment quality (Duhoux et al., 2009; Wang et al., 2005), although some have found better quality of care among females who received specialised services (Wang et al., 2000) or counselling (Young et al., 2008). Equivalent Australian research is needed.
Conclusions
Recently implemented initiatives seem to have improved males’ likelihood of specialised mental health services and reduced their reliance on GP-only care. Although the gender gap may have narrowed, the sustained differential in service utilisation between males and females supports the need for continued policy and planning responses to address gender-specific factors related to access and health care preferences.
Footnotes
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Funding
This project was supported by the Movember Foundation and the NHMRC Centre for Research Excellence in Mental Health Systems Improvement (APP1041131).