
Abstract
Objective:
Mental disorder is common among people who stalk. However, the nature of this association is unclear and it is not known whether the commencement of stalking is associated with symptoms of disorder. This study used a longitudinal design to examine the association between the onset and cessation of stalking behavior and indicators of mental disorder in the form of mental health service use.
Method:
Data linkage was used to explore public mental health service use among 157 people who engaged in stalking in Melbourne, Australia. Mental health service use across the lifetime, 5 months prior to stalking onset, between the onset and cessation of stalking (during stalking) and 5 months post-stalking was identified. Mixed regression models tested temporal associations between types of mental health service use (acute vs continuing care) and onset and cessation of stalking in a subsample of 130 participants where dates of the stalking episode were available.
Results:
A total of 105 (67%) participants had lifetime use of public mental health services, while 15% accessed mental health services in the 5 months prior to (N = 19) or during the stalking (N = 20) and 22% (N = 29) used services in the 5 months after the stalking ceased. Odds of using acute mental health services and average monthly rate of use were highest during the stalking. Odds and average monthly rate of using continuing care were highest after the episode ceased.
Conclusions:
Most people who stalk have used public mental health services, but a minority access services immediately prior to or during the stalking episode. Acute service use was more common during the stalking, while use of continuing care services was more common after the stalking ceased. These findings provide preliminary support for a temporal relationship between acute mental disorder and stalking behavior.
Over 70% of people whose stalking behavior results in criminal justice system intervention have diagnosable mental disorder, and most have had prior contact with mental health services (McEwan et al., 2020; Nijdam-Jones et al., 2018). Despite this, stalking is thought to be directly attributable to mental disorder in a relatively small number of cases, with symptoms more frequently thought to contribute to stalking indirectly through interaction with personality vulnerabilities, the situational characteristics that trigger and maintain stalking and the broader social context (Birch et al., 2018; Mullen et al., 2009; White et al., 2000). These hypotheses about the role of mental disorder in stalking are largely based on post hoc assessments by forensic mental health clinicians after a stalking episode has commenced, or after it has ceased. The absence of longitudinal research examining the presence and nature of mental disorder prior to and during a stalking episode means it is unclear whether the commencement of stalking is related to the onset or exacerbation of symptoms of mental disorder, whether stalking and mental disorder have some common cause, or whether mental disorder simply co-exists with stalking but has no identifiable temporal relationship. This study aims to examine the associations between onset and cessation of stalking behavior and indicators of mental disorder as measured by mental health service use.
Mental disorder, and particularly mental illness, has long been a focus of attention in the stalking literature (Harmon et al., 1995; Kienlen et al., 1997; Zona et al., 1993). Psychosis received much attention in early research, and erotomanic, persecutory and grandiose delusional states have all been reported in samples of justice-involved stalkers, along with less common delusional beliefs such as delusions of kinship (McEwan and Strand, 2013; Mullen et al., 1999). More recently, Nijdam-Jones and colleagues used structured diagnostic interviews to identify mental disorder in a sample of 137 predominantly ex-partner stalkers (77%) referred by New York courts to a treatment program for stalking. They diagnosed 30% with a mood or anxiety disorder, 10% with a psychotic disorder, 46% with a substance use disorder, and 50% with a personality disorder. In 44% of cases, more than one disorder was diagnosed and only 28% of the sample did not meet criteria for any mental disorder. While methodologically stronger than previous studies, Nijdam-Jones and colleagues’ results are like those reported by studies using less rigorous diagnostic methods (Harmon et al., 1998; James and Farnham, 2003; McEwan et al., 2017, 2020; McEwan and Strand, 2013; Mullen et al., 1999; Rosenfeld and Harmon, 2002). Across these studies, those who stalk strangers and acquaintances (i.e. non-ex-intimates) are usually reported as having significantly higher rates of psychotic disorder than former partners or estranged friends or family (ex-intimates); prevalence estimates range from 26% to 50% in the former group and around 10% in the latter (McEwan and Strand, 2013; Mohandie et al., 2006). Ex-intimates tend to have higher rates of mood disorder and substance use disorder (McEwan and Strand, 2013; Nijdam-Jones et al., 2018). Personality disorder is common among all stalkers, with 40–50% meeting diagnostic criteria at the time of forensic mental health assessment (McEwan et al., 2020; McEwan and Strand, 2013; Nijdam-Jones et al., 2018).
These studies have led to a consensus that mental disorder is an important consideration when assessing and treating those who stalk (MacKenzie and James, 2011; Purcell and McEwan, 2018), and has led to recommendations that mental health assessment should be a routine part of court proceedings in stalking cases (McEwan and Strand, 2013). However, research in this area has some significant methodological limitations (Wheatley et al., 2020). Diagnoses are typically made from a single, cross-sectional assessment with no comparison sample. There are no estimates of the prevalence of mental disorder among stalkers whose behavior does not attract attention from criminal justice or mental health services. Accurate prevalence estimates are difficult to obtain because forensic samples do not reflect the breadth of stalking behavior observed in the community (McEwan et al., 2020; Nijdam-Jones et al., 2018; Purcell et al., 2002). Perhaps the most significant limitation is that the vast majority of diagnoses in studies to date are made after the stalking episode has ceased. This makes it difficult to draw conclusions about the presence of mental disorder at the time stalking occurred, its potential contribution to the stalking behavior or whether it is a consequence of the stalking and criminal justice responses.
There are several potential pathways linking mental disorder and stalking. The most direct concerns delusions about the victim and has been suggested by several authors based on forensic mental health samples (Harmon et al., 1995; Kienlen et al., 1997; Meloy, 2000; Mullen et al., 2000, 2009) and published case studies (Orion, 2001; Peterson and Davis, 1985; Schlesinger, 2002). More recently, McEwan et al. (2017) found that the presence of a psychotic illness, and specifically delusional beliefs about the victim, at the time of forensic assessment was significantly and strongly associated with increased duration of prior stalking, suggesting some level of co-occurrence of symptoms and behavior over time. If psychosis does play a causal role in stalking behavior, then an increase in psychiatric treatment that diminishes the intensity, if not the presence, of psychotic symptoms should be associated with the cessation of stalking behavior.
The other hypothesized pathway is indirect, with stalking and mental disorder thought to share a common cause. This hypothesis reflects the observation that the trigger for the onset of some stalking episodes (e.g. breakdown of a relationship) may also precipitate the onset or exacerbation of symptoms of mental disorder (e.g. a major depressive episode, substance misuse or a period of acute emotional dysregulation and suicidality in someone with personality disorder) (Mullen et al., 2009). It is also possible in these cases that the symptoms of mental disorder contribute to stalking behavior over time through their effects on emotional and cognitive processes. Both scenarios are consistent with the self-report of those who stalk following the breakdown of a relationship, a group that accounts for approximately half of all stalkers (Spitzberg and Cupach, 2014). Many of these people report feelings of hurt, sadness, depression and anger around the time their stalking began (Thompson and Leclerc, 2014), and a substantial minority report suicidal thoughts associated with the situation that precipitated the stalking (McEwan et al., 2010; Thompson and Leclerc, 2014). However, as ex-intimate stalkers are typically referred for forensic assessment via court or probation services, diagnosis often takes place sometime after the stalking has ceased, making it difficult to know whether the symptoms observed at assessment were present prior to the onset of the stalking and/or during the stalking episode. It is possible that mental disorders present in these cases are a consequence of criminal justice system intervention, rather than a contributing factor to stalking. Conversely, it is possible that the delay between the onset of stalking and a later forensic assessment obscures the presence of symptoms that contributed to the onset and persistence of stalking behavior.
Current study
To date, no research has systematically investigated the presence of symptoms of mental disorder prior to, during and after stalking episodes, meaning there is little evidence with which to test the above assertions. This study used mental health service use as a proxy for symptoms of mental disorder and aimed to explore (1) lifetime use of public mental health services in a sample of stalkers; (2) associations between mental health service use and the onset and cessation of stalking episodes; and (3) differences in mental health service use among stalkers who were former intimates of the victim (ex-intimates), and those with other relationships (non-ex-intimates).
Based on existing research (McEwan et al., 2020; Nijdam-Jones et al., 2018), it was hypothesized that most participants would have used mental health services in their lifetime, but that non-ex-intimates would have higher rates of service use than ex-intimates due to higher rates of mental illness in the former group at forensic assessment (McEwan and Strand, 2013; Mullen et al., 1999). Given the prevalence of psychotic disorders among those receiving community continuing care services in Australia (Suggett et al., 2012), and the prevalence of psychotic disorders among non-ex-intimates who stalk (McEwan and Strand, 2013; Mohandie et al., 2016; Mullen et al., 1999), it was hypothesized that non-ex-intimates would have more lifetime use of continuing care services than ex-intimates. No hypotheses were made about between-group (ex-intimates vs non-ex-intimates) differences in use of acute psychiatric services, given the exploratory nature of this question.
When examining the temporal relationship between stalking and mental health service use, it was hypothesized that use of mental health services would be higher during the stalking episode across the entire sample relative to the months prior to and following the end of the stalking. Comparisons of service use among ex-intimates and non-ex-intimates were investigated in an exploratory way, given the lack of previous research.
Method
Participants
Participants were clients of a specialist state-wide publicly funded clinic for people with a history of stalking in Melbourne, Australia. Those referred between July 2010 and December 2013 were invited to participate in the research. While the program is located in a community forensic mental health service, the presence of mental disorder is not a criterion for referral (McEwan et al., 2014). Each client completed an interview with a clinical psychologist or psychiatrist to inform risk assessment and intervention needs. Where consent was provided, data were collected from the interview and supplemented by file review (e.g. police summaries of charges, judges sentencing comments, victim statements, formal criminal histories and the reports of other assessing clinicians). In some cases, additional collateral information was obtained by the assessing clinician from a family member or caseworker.
The project was approved by the authors’ university Human Research Ethics Committee. Of the 231 people who attended an assessment interview, 157 consented to participate (51 refused and 23 were unable to provide consent). Most (87%) consenting clients were referred from criminal justice settings, 10% by mental health services and 3% by their private doctor or lawyer.
Mental health service use data
Mental health service use was used as a proxy measure for mental illness experienced during and around the stalking episode. In Victoria, public mental health services generally cater to consumers with severe mental illness or related disturbance (State of Victoria, 2019). Acute services provide urgent assessment, brief intervention and service linkage for those experiencing significant distress, (re)emergence of acute psychotic symptoms and who may pose a risk to their self or others due to their psychiatric functioning. Continuing care services provide long-term intervention and case management to those with serious mental illness.
All participants consented to researchers accessing their information from the Victorian Psychiatric Case Register (VPCR), which records all direct contact an individual has with public mental health services in Victoria. Of the 130 cases with stalking episode dates, 120 had VPCR records. We assumed an absence of public mental health service use for the remaining 10 cases. Mental health service use was defined in three ways: (1) acute: emergency room presentation, inpatient mental health admissions and contact with a crisis assessment and treatment team (CATT); (2) continuing care: all use that was not acute (e.g. Child and Adolescent Mental Health Service [CAMHS], mobile support and continuing care teams, hospital outpatient units and day programs); and (3) overall, which combined the two previous categories. Use associated with the assessment leading to inclusion in the study was excluded, as was use recorded for the purposes of triage, intake, consultation and liaison and psychiatric geriatric assessment and treatment, as these were thought to be less likely to be associated with diagnosable mental disorder and intervention.
Stalking episode data
Stalking was defined as the presence of a stalking conviction under the Victorian Crimes Act (1958) or evidence of multiple unwanted intrusions on the victim persisting over more than 2 weeks (Purcell et al., 2004). Only information from the first referral for stalking during the data collection period was used. The nature of the prior relationship with the stalking victim, and dates of onset and cessation of stalking were ascertained at the time of assessment from collateral material, usually the police narrative of the victim’s report but sometimes using participants’ accounts where they indicated commencement of stalking prior to or cessation after that indicated by collateral material. Where an exact start date was not available, the first day of the known onset month was substituted (32 cases), while end dates always involved the last known contact with the victim prior to the apparent cessation of stalking. Given the sampling location, in many cases, cessation would have been due to external contingencies (such as police or mental health involvement) rather than being voluntary.
Analyses of mental health service use ‘during the stalking episode’ used the period between the onset date and cessation date of the stalking episode (range = 1 day–3640 days). The pre- and post-stalking periods each consisted of 5 months, the maximum period available as one participant had a second stalking episode recorded as beginning 5 months after the end of the index stalking episode. Twenty-seven participants (19 non-ex-intimates and 8 ex-intimates) were excluded from analyses of the temporal relationship between stalking onset and cessation and mental health service use because the stalking episode start date could not be ascertained. Exclusion was non-random and biased toward non-ex-intimates, affecting only 8.82% of those referred by probation or court, but 61.90% of referrals from other sources (including 11 of the 16 referred by mental health services) (χ2 = 38.28, p < 0.001). This means the results of the temporal analyses are specific to stalkers whose behavior brought them into contact with the criminal justice system.
Diagnoses
Mental disorders are recorded in the VPCR according to the International Classification of Diseases (ICD-10) and are typically diagnosed by psychiatrists. The VPCR does not record contact with general practitioners and private mental health clinicians. Most Victorians with psychotic illnesses receive public health care at some point (Department of Health and Ageing, 2010; Jablenksy et al., 1999) but those with other disorders may not make use of public mental health services unless these disorders are severe or acutely exacerbated (Wallace et al., 2004). All diagnoses recorded in the VPCR were coded into categories used in previous research (Cutajar et al., 2010; Short et al., 2010; Wallace et al., 2004). Table 1 provides details about categorisation of diagnoses.
Concordance between mental health diagnoses recorded at time of forensic assessment and across the lifetime in the VPCR.
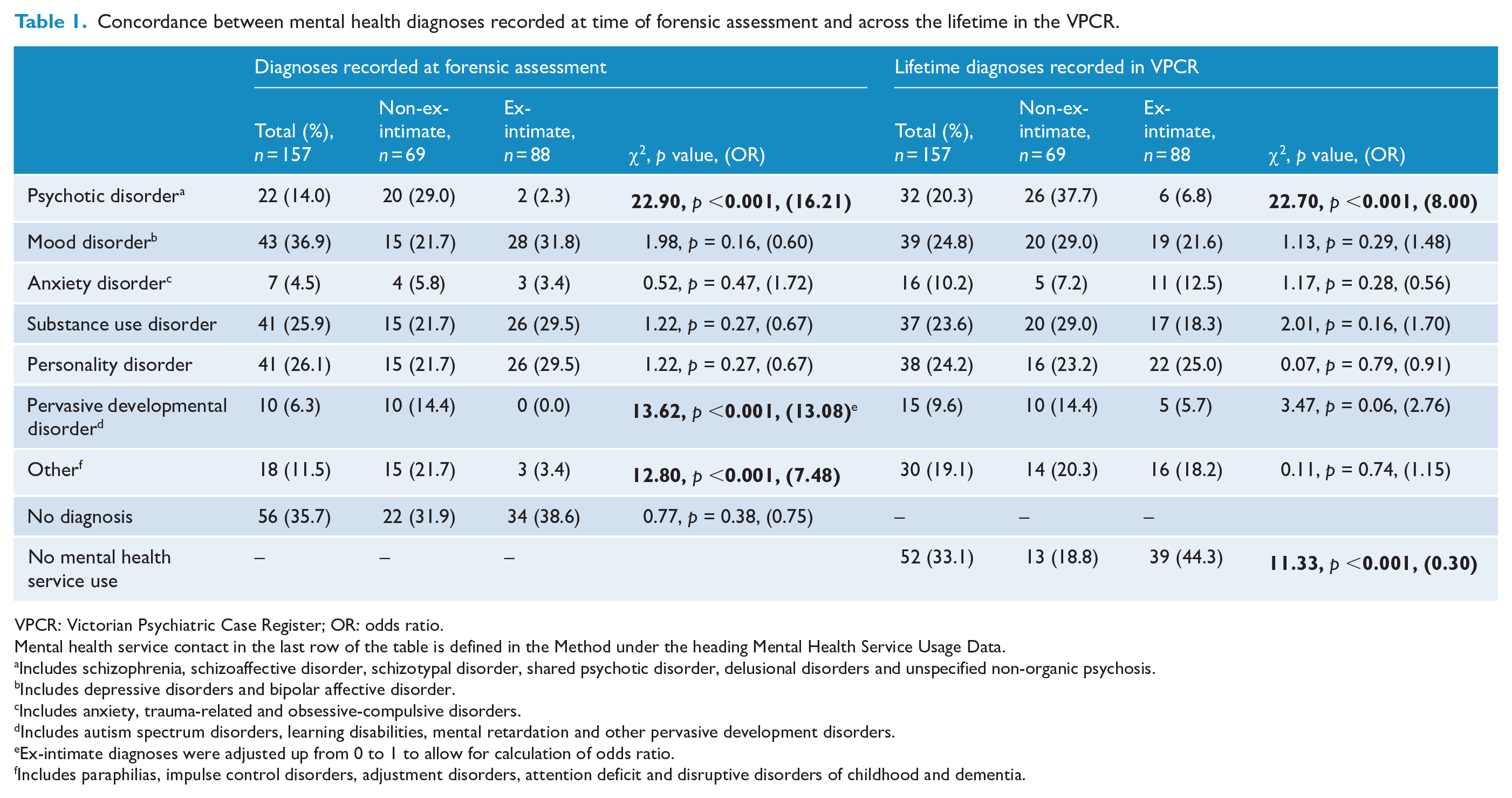
VPCR: Victorian Psychiatric Case Register; OR: odds ratio.
Mental health service contact in the last row of the table is defined in the Method under the heading Mental Health Service Usage Data.
Includes schizophrenia, schizoaffective disorder, schizotypal disorder, shared psychotic disorder, delusional disorders and unspecified non-organic psychosis.
Includes depressive disorders and bipolar affective disorder.
Includes anxiety, trauma-related and obsessive-compulsive disorders.
Includes autism spectrum disorders, learning disabilities, mental retardation and other pervasive development disorders.
Ex-intimate diagnoses were adjusted up from 0 to 1 to allow for calculation of odds ratio.
Includes paraphilias, impulse control disorders, adjustment disorders, attention deficit and disruptive disorders of childhood and dementia.
Data linkage
The data linkage procedure involved extracting exact and then probable linkages from the VPCR using identifying information (first name, surname, aliases, date of birth, age range and gender). Where there were matches, de-identified VPCR records prior to 31 December 2014 were obtained.
Analyses
Chi-square tests of independence (odds ratio for effect size) were used to compare the mental health diagnoses given to ex-intimates and non-ex-intimates, and to compare the prevalence of any mental health service use, use of acute services and use of continuing care services between ex-intimates and non-ex-intimates across the lifetime and at each of the three time points (pre-, during and post-stalking).
Two forms of mixed regression modeling were used to examine the temporal relationship between types of mental health use, the presence of stalking and relationship group (ex-intimate vs non-ex-intimate). Random intercept negative binomial regression was used to examine differences in the monthly rate of mental health service use before, during and after the stalking episode. Due to the large number of time periods with no mental health use, a zero-inflated model was estimated with an additional parameter to model cases with no use. Random intercept logistic regression was used to examine differences in the odds of a mental health service use in each time period.
Finally, because stalking duration differed across cases (range = 1 day–3640 days), an offset term was used to account for the difference in exposure times in the ‘during stalking’ regression analyses. This allows for model adjustment such so that the same number of service uses is weighted by the length of the stalking episode in each case.
Three logistic models and three zero-inflated negative binomial models were calculated to investigate any mental health service use, acute care use and continuing care use. In each case, the models included three fixed effects: a categorical variable for time period relative to stalking (0 = pre-stalking; 1 = during stalking; 2 = post-stalking), a categorical variable for relationship status (0 = ex-intimate, 1 = non-ex-intimate) and an interaction between relationship and time. Type III Wald chi-square tests were used to test the effect of each term, with odds ratios measuring effect sizes between time periods and relationship groups. Interaction terms were displayed graphically with odds converted to probabilities for ease of interpretation. The alpha level was set at p = 0.05, two tailed.
All analyses were conducted in Rstudio 1.1.442. (Rstudio Team, 2016) using the packages foreign (R Core Team, 2018), readxl (Wickham and Bryan, 2019), dplyr (Wickham et al., 2019), zoo (Zeileis and Grothendieck, 2005), stringr (Wickham, 2019), lme4 (Bates et al., 2015), psych (Revelle, 2018), qdap (Rinker, 2019), emmeans (Lenth, 2019), MASS (Venables and Ripley, 2002), glmmTMB (Brooks et al., 2017) and car (Fox and Weisberg, 2019).
Results
The sample comprised 144 men and 13 women (88 ex-intimates and 69 non-ex-intimates), with one identifying as gay. Mean age at the time stalking commenced was 35 years (SD = 10.8). Most (n = 124; 79.3%) were born in Australia, including two who identified as Aboriginal Australian. The most severe mental health diagnosis recorded at the time of the interview and primary lifetime diagnoses are shown in Table 1. Further demographic information and information about the stalking episodes is provided in McEwan et al. (2017).
Nature and timing of mental health service use
In the entire sample, 105 (66.9%) participants had lifetime public mental health service use, with non-ex-intimates having 3.4 times greater odds of lifetime use than ex-intimates, 81.2% vs 55.7%; χ2(1) = 11.3, p < 0.001.
Eighty-one (62.3%) of the 130 participants with intact stalking episode dates had some lifetime use of mental health services, with 55.4% accessing continuing care services, and 34.6% using an acute service. Few participants (n = 10; 6.9%) had childhood psychiatric service use recorded. As shown in Table 2, among those with intact stalking dates, there were no significant differences in any form of lifetime psychiatric service use between ex-intimates and non-ex-intimates. This was likely due to non-random exclusion of cases lacking stalking start dates, more of whom were non-ex-intimates referred by mental health services.
Prevalence of types of service use across the lifetime, and incidence prior to, during and following the stalking episode, with comparisons between relationship groups (among participants with stalking onset and cessation date data).
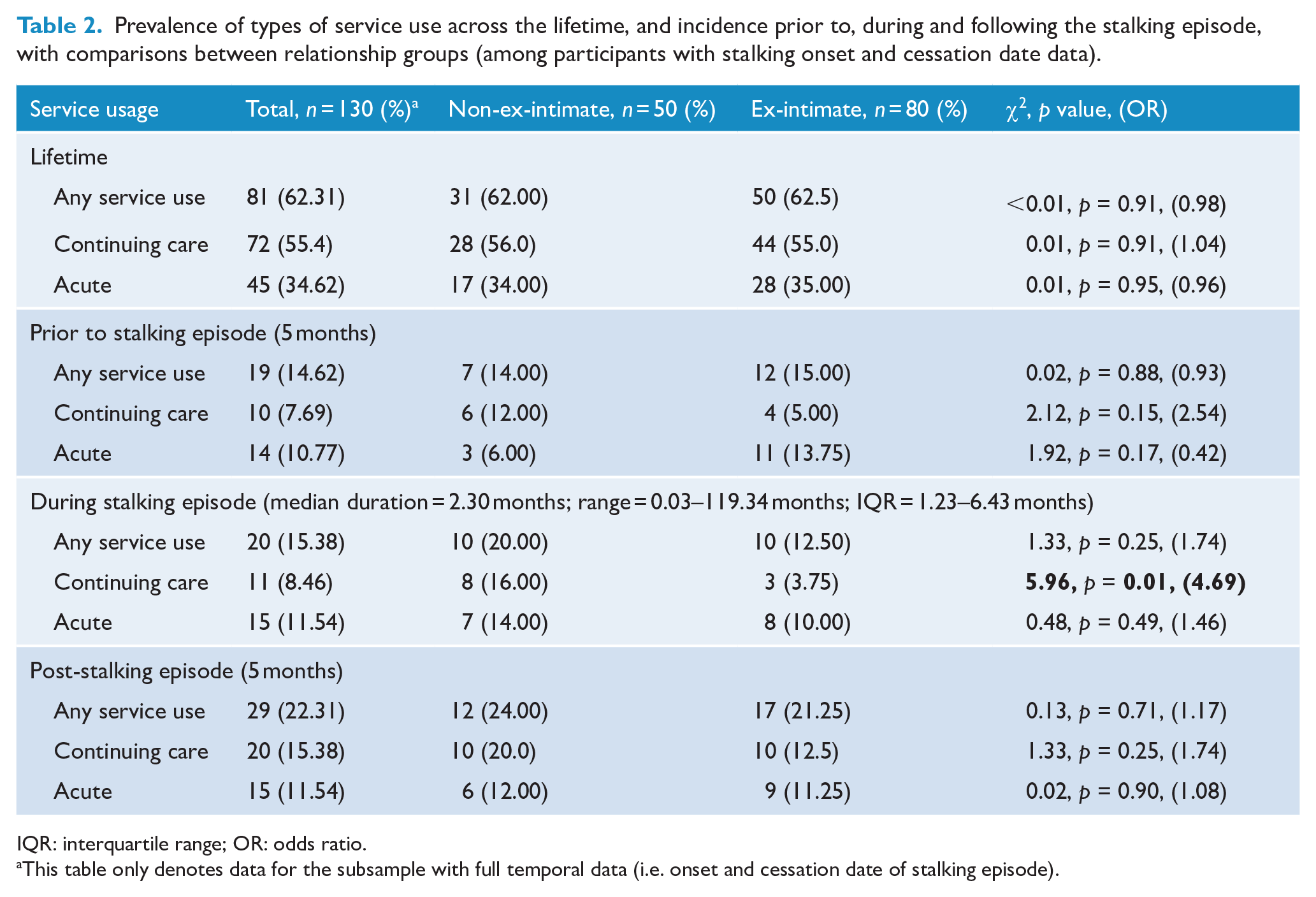
IQR: interquartile range; OR: odds ratio.
This table only denotes data for the subsample with full temporal data (i.e. onset and cessation date of stalking episode).
Fourteen participants (10.7%; six ex-intimates) used mental health services in the month following the onset of the stalking episode, of which half used acute services (n = 7; two ex-intimates). The most common diagnoses recorded in the month following stalking onset were mood (n = 5), personality (n = 4), psychotic (n = 3), substance use (n = 3) and other (n = 4) disorders. One person had suicidal ideation identified, three had ‘no diagnosis’ specified and in five continuing care cases, no entry was made under diagnosis. This may reflect VPCR policy that diagnoses do not need to be recorded at every contact in an episode of continuing care and does not necessarily mean that no mental illness was present.
The incidence of service use pre-, during and post-stalking episode ranged between 15% and 20% of the sample (see Table 2, noting that two-thirds of those referred for forensic assessment by mental health services were excluded from these analyses as stalking episode start dates could not be ascertained). Incidence of acute and continuing care use was similar for ex-intimates and non-ex-intimates, with only the frequency of continuing care use during the stalking episode being greater in the non-ex-intimate group. Acute use was equally likely in both groups during and after the stalking episode. There was a trend toward ex-intimates being more likely to have acute use prior to the stalking episode, and non-ex-intimates being more likely to have continuing care use during the same period, with the latter pattern continuing post-stalking.
The results of the offset adjusted count and binary regression models controlling for variation in the duration of stalking and investigating the interaction between relationship and time period are shown in Table 3. While the odds of service use did not vary by time period, the frequency of use and of different types of use, all varied significantly. There was no significant main effect of relationship status on any form of mental health service use, but time period and relationship status significantly interacted to affect the frequency of acute service use. Table 4 shows differences between time periods. Participants had the lowest odds of any service use prior to the stalking episode, and the highest odds in the period after the stalking ceased. The incident rate ratios (IRRs) show that the estimated monthly rate of use was also higher after the stalking episode compared to before the stalking episode. However, separating usage into acute vs continuing care showed different underlying patterns. The highest odds of acute use were during the stalking episode and the lowest odds were after the episode. The pattern of IRRs was similar, with participants having an estimated monthly rate of acute service use over twice as high during the stalking episode compared to before the stalking episode. The pattern for continuing care showed significantly higher odds and higher estimated monthly rate of service use after the stalking episode relative to during or before the stalking.
Wald chi-square tests for factors in logistic models (showing relationship between presence of service use type across time periods and by relationship status).
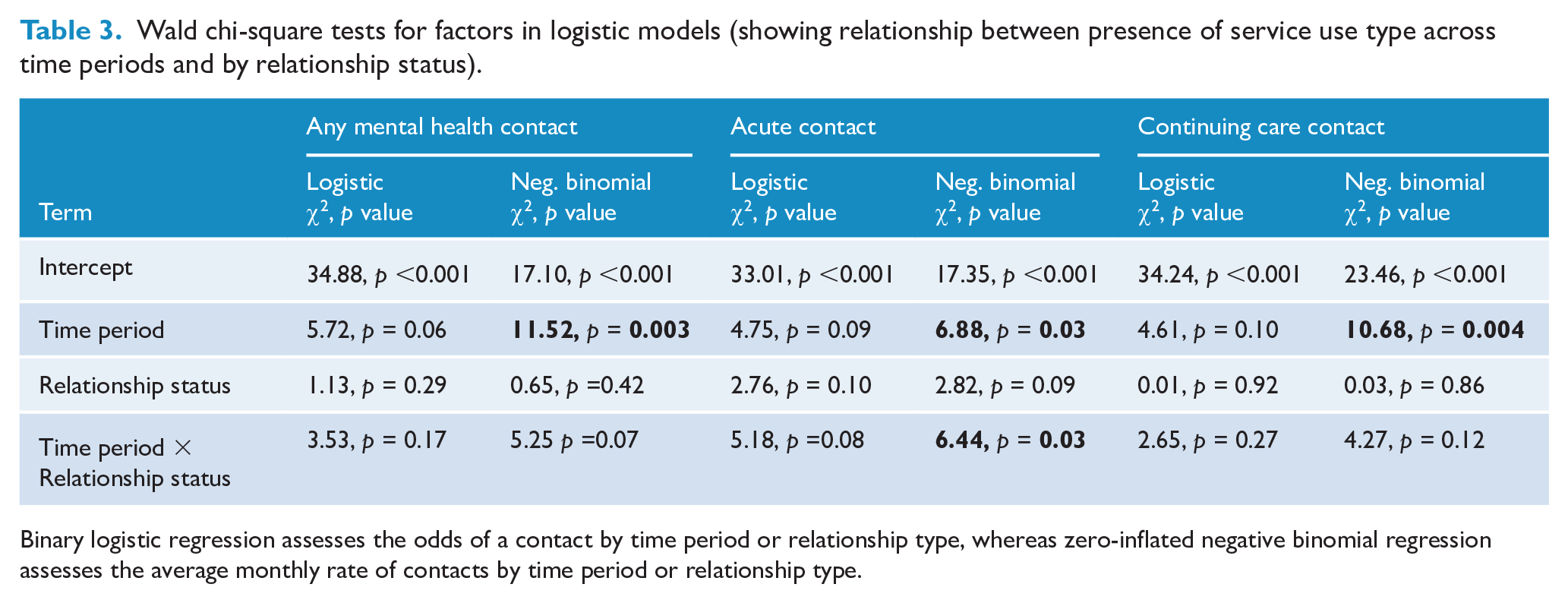
Binary logistic regression assesses the odds of a contact by time period or relationship type, whereas zero-inflated negative binomial regression assesses the average monthly rate of contacts by time period or relationship type.
Incident rate and odds ratios for main terms in each regression model.
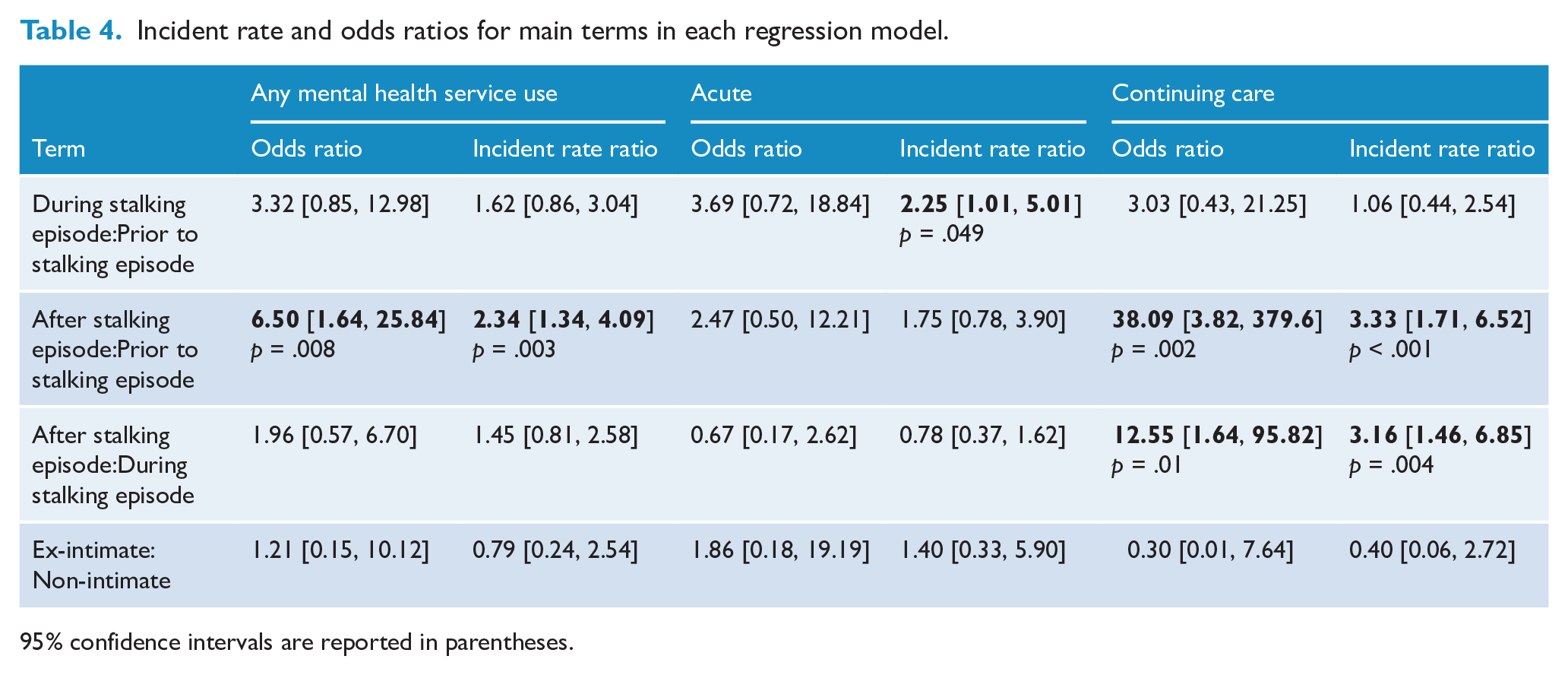
95% confidence intervals are reported in parentheses.
Interaction plots displaying the average monthly rate of service use in each time period (negative binomial models), and probability of use in each time period (logistic regression models) by relationship status are displayed in Figure 1. In only one of the plots—predicted rate of acute use—was the interaction between relationship type and service use type significantly associated with the outcome, t(382) = −2.48, p = 0.01. The non-ex-intimate group had a sharp rise in the predicted probability of acute service use from before to during the episode and did not vary considerably from during or after the episode. The pattern among ex-intimate participants appeared visually different, but differences were not statistically significant.
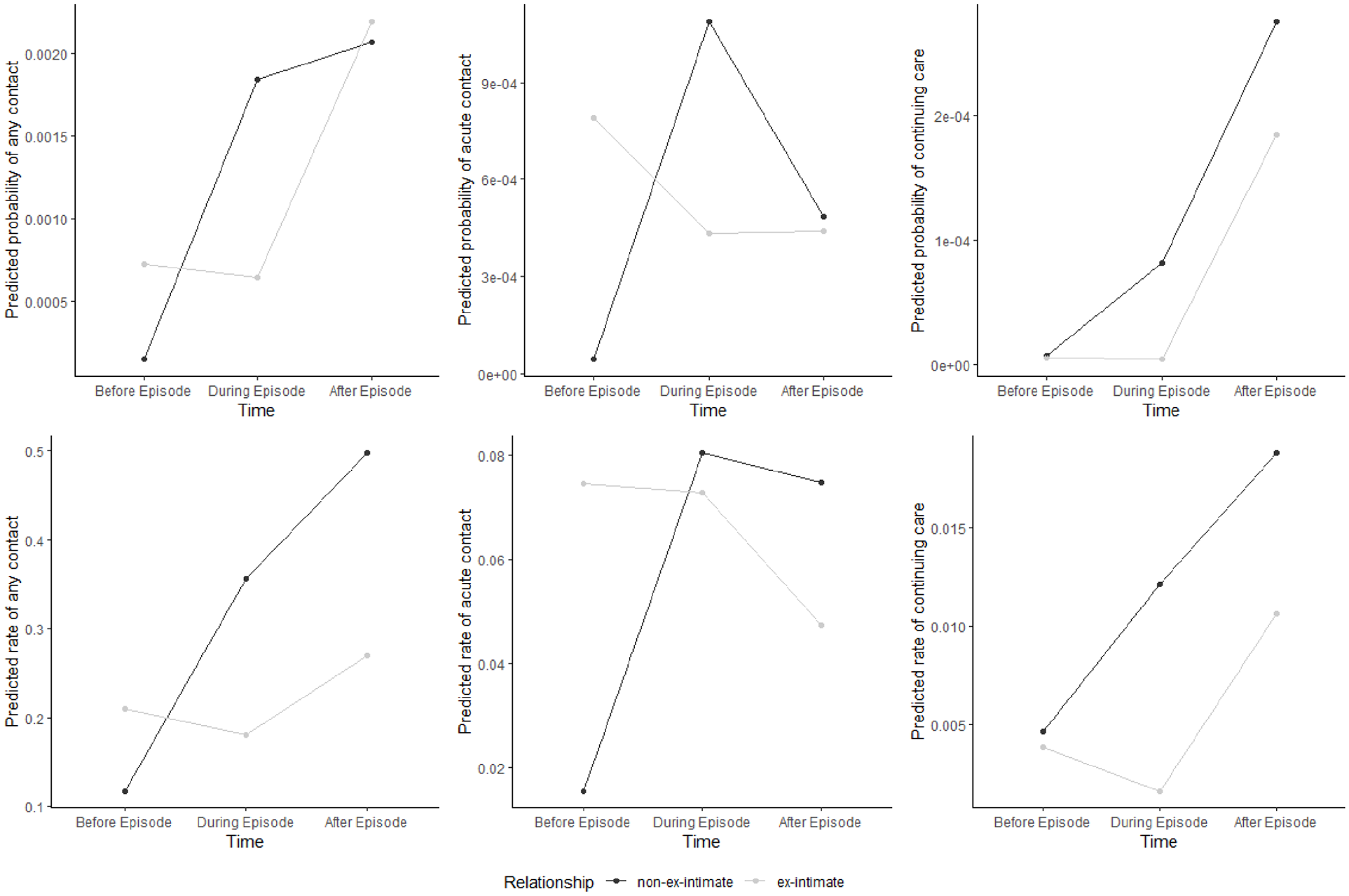
Interactions between time relative to stalking episode and mental health service use (overall and by acute or continuing care status).
Discussion
This study explored (1) lifetime public mental health service use in a sample of stalkers; (2) associations between public mental health service use (as a proxy measure of mental illness) and the onset and cessation of stalking; and (3) differences in public mental health service use among stalkers who were former intimates of the victim (ex-intimates), and those with other relationships (non-ex-intimates). As hypothesized, mental health service use was common in the sample, with two-thirds of participants having lifetime use. This is substantially higher than lifetime service use for the general community in Victoria (8%; Cutajar et al., 2010), but it is also higher than use in a sample of people detained in police cells in the same jurisdiction (55%; Ogloff et al., 2011). Lifetime rates of mental health service use were significantly higher among non-ex-intimates (81% vs 55%), confirming the hypothesis and previous observations based on cross-sectional forensic assessments (McEwan and Strand, 2013; Mohandie et al., 2006).
Some lifetime mental health diagnoses differed markedly between ex-intimates and non-ex-intimates. Most notable were the higher rates of psychotic disorder among non-ex-intimates at both forensic assessment and across the lifetime, consistent with previous cross-sectional research (McEwan and Strand, 2013). Rates of pervasive developmental disorder were also notably higher among non-ex-intimates, again, reflecting observations in previous research that these diagnoses may be associated with increased risk of stalking in pursuit of a relationship (Stokes et al., 2007). Disorders that are perhaps less likely to be directly related to stalking behavior were present at similar rates across relationship groups (i.e. mood, substance use, personality disorder and ‘other’ disorders; Purcell and McEwan, 2018). While the overall pattern of diagnoses at the cross-sectional forensic assessment and over the lifetime (i.e. recorded in the VPCR) were broadly similar, there were lower rates of psychotic and anxiety disorders, and higher rates of mood disorder and ‘other’ disorders recorded at forensic interview.
The proportion of non-ex-intimates and ex-intimates with lifetime mental health service use was more similar in the subsample for whom temporal information was available because more non-ex-intimates (who were more often referred by mental health services) were excluded due to a lack of information about the start of the stalking episode. This means that the temporal analyses are likely only generalizable to stalkers whose behavior brings them into contact with the criminal justice system. Hypotheses about the temporal relationship between the probability and frequency of mental health service use and stalking onset and cessation were partially supported. It was hypothesized that use of mental health services would increase during the stalking episode relative to the months prior to and following the end of the stalking. While this was not observed for mental health service use overall, within acute service use, the hypothesized pattern was observed. Acute service use occurred significantly more often during the stalking episode than prior to it. Unexpectedly, continuing care service use was more likely to occur, and occurred with greater frequency, after the stalking episode than either before or during it. It should be noted that the odds ratio comparing continuing care use after stalking to use prior to stalking was very high. The small numbers involved in this analysis mean the odds ratio is sensitive to small variations in frequencies. Subtracting one use of continuing care from the total number after the stalking reduced the predicted odds ratio by over 50%, though it remained significant (OR = 15.96, 95% CI = [2.37, 107.25]). This suggests that while the odds of using continuing care services are significantly greater after the stalking episode relative to before or during the stalking, the reported size is likely influenced by chance error in this small sample.
Small sample sizes precluded between-group analyses based on diagnosis across time periods. Descriptively, however, approximately 10% of the sample used public mental health services within a month of stalking onset (57.1% being non-ex-intimates). Half of these involved acute services, and psychotic and mood disorders were the most frequently recorded diagnoses at this time.
The overall pattern of findings is consistent with the assertion that a subgroup of participants are significantly affected by acute symptoms of mental illness when the stalking episode commences and while it continues (Mullen et al., 2009). Figure 1 demonstrates that this pattern is most obvious in the non-ex-intimate group, where there was a clear and significant increase in acute mental health service use during the stalking episode. There were no significant changes in the ex-intimate group’s use of acute services from pre- to during or post-stalking. This could mean that non-ex-intimates more often experience acute symptoms of psychosis that directly contribute to the onset of stalking behavior, while ex-intimates access acute services in the context of distress, substance use and depressed mood prior to the stalking episode (associated with relationship conflict and breakdown), which continues during, and post-stalking.
The marked increase in the probability and frequency of continuing care service use in the 5 months following the stalking episode was observable across groups, though the actual proportion of the sample with use in this period remained relatively low at only 15% (20% of non-ex-intimates and 12.5% of ex-intimates). It is possible that for both ex-intimates and non-ex-intimates, acute service use during the stalking led to referrals to continuing care, which then coincided with the end of the stalking episode. While it might be hypothesized that continuing mental health care contributed to the end of the stalking episode in these cases, it is not possible to conclude this from the data available to us.
Limitations and future directions
This study is limited by the non-random sample of stalkers included in this study. As the sample was referred to a forensic mental health service, it is possible that the rates of mental disorder diagnoses over-estimate true rates of mental disorder among stalkers. Also, this study did not consider private mental health service use, those who did not seek treatment or those who may have presented with mental illness needs below the threshold required for public mental health services. This is a substantial limitation and means that the findings should only be interpreted in relation to severe mental health problems that result in public mental health service use. The other major limitation is the small sample size. The retrospective nature of the study design is also suboptimal and future research would ideally be undertaken prospectively with more detail about the nature of the mental health concerns leading to mental health service use, and about the onset of stalking in those referred from mental health. Ideally, such research would also be able to examine the nature of any mental health intervention provided to clients, and the effects of such intervention on the stalking behavior.
Conclusion
This study adds to the existing literature on the role of mental disorder in stalking behavior by providing the first longitudinal analysis of this relationship. Most of the participants had used public mental health services at some stage in their life, though the reasons for use appeared to differ to some degree between people who stalked ex-intimates vs non-ex-intimates. Overall, acute mental health service use increased among participants during the stalking episode relative to service use before or after, while continuing care use was more common after stalking had ceased than either prior to or during the stalking episode. These findings are broadly consistent with the hypothesized pathways linking symptoms of mental disorder to stalking behavior and support the contention that acute symptoms are linked to the onset and persistence of some people’s stalking behavior.
While this study provides useful information and suggests pathways for future research examining the effects of mental health interventions on reducing stalking behavior, it must be noted that a minority of participants (15–20%) used public mental health services around the time of the stalking episode. This likely underestimates the true rate in the sample, as most of those referred by mental health services had to be excluded from the temporal analyses. Nonetheless, the relatively low rates of mental health service usage potentially reflect the severity of disorder that is needed to receive public mental health services in Victoria, and the fact that stalking is not only a product of poor mental health. The personality vulnerabilities of the stalker and the broader social context in which the stalking emerges are very likely equally important contributors, with mental ill health exacerbating the effects of these factors in some cases.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This research received funding from Australian Research Discovery Project DP1092840.