
Abstract
Substance use disorder is a common co-morbid diagnosis in patients with a psychiatric disorder. A large community-based co-morbidity study [1] evaluated substance abuse and psychiatric disorders: 47% of the patients with a psychotic disorder had a history of substance use disorder, compared to 32% of the patients with an affective disorder, 23.7% of the patients with an anxiety disorder and 16.7% of the general population. In particular, cannabis use disorder is a common co-morbid diagnosis among patients in the early course of a psychotic disorder [2]. Prevalence estimates of cannabis abuse in individuals with and without a psychotic disorder were calculated in a review [3] in which data from 53 studies of treatment samples and 5 epidemiological studies were considered. The reviewed studies reported consistently higher prevalence of cannabis use disorder in people with a psychotic disorder compared to people without a psychotic disorder.
Studies on the relationship between cannabis use and psychotic disorders have provided more insights in this complex relationship. Arseneault et al. [4] described in a review of five longitudinal studies that cannabis use during adolescence resulted in a two-fold higher relative risk of developing a psychotic disorder later in life. Moore et al. reported in a more recent review [5] an increased risk of psychotic outcome for people who ever used cannabis. When controlled for confounding factors, the relationship between cannabis use and psychotic outcome remained significant in 6 out of the 7 analysed studies. They also reported a dose-response effect in all six studies in which the frequency of cannabis use had been studied: subjects using more cannabis had a higher risk of a psychotic outcome. In conclusion, these studies support the hypothesis that cannabis use is a risk factor for the development of a psychotic disorder.
Specific hypotheses have been formulated regarding the relationship between cannabis abuse and psychotic disorders. Hambrecht and Häfner [6] found support for the ‘vulnerability-stress-coping hypothesis’. The patients with schizophrenia in this study were divided into three groups based on onset of the disorder and onset of cannabis abuse. In the ‘vulnerability group’, the influence of cannabis might have reduced the vulnerability threshold and/or coping resources of the patients. This group of patients had been abusing cannabis before the onset of the first signs of schizophrenia. In the ‘stress group’ patients were already vulnerable to schizophrenia, and cannabis abuse was the stress factor precipitating the onset of the disorder. The onset of cannabis abuse and the first psychotic symptoms occurred within the same month in these patients. The ‘coping group’ consisted of patients abusing cannabis as a form of self-medication against their psychotic (or non-psychotic) symptoms. These patients started abusing cannabis after the onset of the first psychotic symptoms.
Regarding the relationship between cannabis abuse and course of the psychotic disorder, many studies show a more negative course of the disorder in patients with co-morbid cannabis use disorder. Psychosocial functioning was worsened [7], more and earlier psychotic relapses were reported [8] and hospitalization rates were higher [7] for patients with a co-morbid cannabis use disorder.
Literature regarding the relationship between cannabis abuse and severity of psychotic symptoms reflects more varying findings. Moore et al. [5] reported in a review of seven studies a positive association between the use of cannabis and psychotic symptoms in general in people who ever used cannabis. More specifically, Caspari et al. [7] found that patients with a psychotic disorder and cannabis use disorder had higher scores on the psychopathological syndromes ‘thought disturbance’ and ‘hostility’ compared to non-abusing patients with a psychotic disorder. On the contrary, Dervaux et al. [9] and Scheller-Gilkey et al. [10] did not find significant differences between patients with and without cannabis use disorder on psychotic symptomatology. Compton et al. [2] also did not find significant difference between cannabis abusing and not abusing first-episode first-hospitalization patients with a psychotic disorder in positive symptoms and general psychopathology, but reported significant less negative symptoms for patients diagnosed with cannabis use disorder compared to patients without cannabis use disorder. The latter finding was replicated by Bersani et al. [11] who also reported significantly lower scores on the Positive and Negative Syndrome Scale (PANSS) negative symptom subscale. Furthermore, this study reported more positive and fewer negative symptoms in those patients that started abusing cannabis after the onset of the psychotic disorder compared to patients abusing cannabis before onset of the illness. These results suggest that the temporal order of cannabis abuse and onset of the psychotic disorder may play an important role in symptomatic outcomes. To summarize, mixed results regarding severity of psychotic symptomatology are reported in the literature. Terminology, methodological differences, differences in patient populations, and differences in temporal relationship between onset of cannabis use and onset of psychosis, may play a role in the varying findings concerning the association between cannabis abuse and psychotic symptoms.
While many studies have examined the relationship of cannabis abuse and symptomatology of the psychotic disorder in patients with a psychotic disorder, the influence of cannabis on pre-psychotic symptomatology among subjects at ultra high risk (UHR) of developing a psychotic disorder has been studied less. The ultra high risk phase can be recognized by subtle behavioural changes and a decline in function; this occurs prior to the development of the psychosis and lasts on average between 1 and 5 years [12]. To recognize these patients Yung et al. formulated the following criteria: Genetic risk and reduced functioning, Attenuated psychosis and Brief limited intermittent psychotic symptoms (BLIPS) [13]. UHR subjects are of particular interest, because knowing which factors are associated with a higher risk of developing a psychotic disorder could be important to prevent transition to psychosis. Cannabis abuse might be a factor associated with a heightened risk of developing a psychotic disorder in these UHR subjects. One of the few studies so far among UHR patients [14] reported that in a one year follow-up study, UHR patients with cannabis use disorder converted to psychosis significantly more frequently (31.3%) compared to UHR patients without cannabis use disorder (3.1%). However, Philips et al. [12] did not find an association between cannabis abuse and a heightened risk for developing psychosis in their one year follow-up study.
In the present study cannabis abuse and the course of the disorder and severity of symptomatology in patients with a psychotic disorder were examined. We also examined cannabis abuse and severity of pre-psychotic symptomatology in UHR patients. Goals were to (i) determine prevalence of cannabis use disorder in patients diagnosed with a psychotic disorder and UHR patients; (ii) compare patients with a psychotic disorder and comorbid cannabis use disorder with those without cannabis use disorder on severity of psychotic symptomatology, psychosocial functioning, number and duration of psychotic episodes; (iii) compare UHR patients with cannabis use disorder to those without cannabis use disorder on severity of pre-psychotic symptomatology and psychosocial functioning.
The following hypotheses were formulated: (i) cannabis abuse in patients with a psychotic disorder is associated with more severe psychotic symptoms; (ii) cannabis abuse in patients with a psychotic disorder is associated with a worse course of the psychotic disorder, reflected by worse psychosocial functioning and more and longer psychotic episodes; (iii) Cannabis abuse in the ultra high risk group is associated with more severe pre-psychotic symptomatology and worse psychosocial functioning. By performing this study we will expand the knowledge in this area. The literature so far reflects varying findings, and a better understanding of the relationship between cannabis abuse and (pre-)psychotic symptoms could improve treatment and prevention programmes. Moreover, to assess first episode patients and subjects at UHR for a psychotic disorder in one study offers the opportunity to compare the impact of cannabis abuse on (pre-) psychotic symptoms in both groups.
Method
Participants
The participants of this study were patients diagnosed with a psychotic disorder and subjects considered at ‘ultra high risk’ of psychosis. All participants had a diagnostic interview at the Early Psychosis Department of the Academic Medical Center (AMC) in the Netherlands. This clinic has specialist experience of patients with a first episode of psychosis. Patients diagnosed with a psychotic disorder were referred to the Early Psychosis Department for a diagnostic interview and for advice for adequate treatment. Subjects considered at ultra high risk of psychosis were referred to this clinic to assess pre-psychotic symptomatology when psychotic development was suspected. The Early Psychosis Department receives their referrals from general practitioners, psychiatrists and psychologists. All mental health care institutions in Amsterdam agreed to refer all patients with a first psychotic episode or patients with UHR symptoms to our department. Data from all consecutively performed diagnostic interviews in the period from September 2006 to May 2009 were gathered. Both male and female subjects were included in this study.
Procedure
During the diagnostic interview experienced clinicians assessed DSM-IV diagnoses, cannabis use, severity of psychotic symptoms, global functioning and psychotic episodes for the patients with a psychotic disorder. For the ultra high risk group, UHR-status, DSM-IV diagnoses, cannabis use, pre-psychotic symptoms and global functioning were assessed. Criteria for ultra high risk for developing psychosis were as described by Yung et al. [13]: genetic risk in combination with reduced functioning, attenuated positive symptoms (scored with the Scale of Prodromal Symptoms (SOPS)), brief limited intermittent psychotic symptoms.
Cannabis use disorder was defined as the presence of DSM-IV diagnosis of cannabis abuse or dependence. During the diagnostic interview, clinical diagnosis of lifetime substance use disorders was assessed. Data of recent cannabis use (mean amount of joints/week during last month), past cannabis use (maximum mean amount of joints/week in lifetime), and lifetime cannabis use (patients were asked if they had ever used cannabis in their lives) were also gathered. For the assessment of the severity of psychotic symptoms the PANSS [15] was used and the SOPS [16], was used to assess presence and severity of prodromal symptoms. Global functioning was assessed using the Global Assessment of Functioning Scale (GAF) [American Psychiatric Association DSM-IV: Diagnostic and Statistical Manual of Mental Disorders. 4th. ed. Washington, DC: APA, 1994]. The course of the psychotic disorder was measured by the number and duration of the psychotic episodes. Information from the interviews of patients and parents were combined in order to collect information about number and duration of the psychotic episodes.
We included 169 consecutively assessed patients with a first psychotic episode and 59 subjects at ultra high risk of psychosis in this study. Both groups were divided into a group diagnosed with a lifetime cannabis use disorder (CUD) and a group without a cannabis use disorder (NCUD).
Statistical analysis
Statistical analyses were performed using the SPSS [SPSS Inc. SPSS, release 16.0 Chicago: 2007] (16.0) software package. Prevalence rates of CUD were calculated. The CUD group was compared to the NCUD group on clinical variables using the non-parametric Mann-Whitney U test. Spearman's Rho correlational test was used to investigate the effects of intensity of cannabis use on psychotic and pre-psychotic symptoms. We also separated the patients with cannabis use disorder but without other substance use disorder, the pure cannabis abusers (PCUD) from the polysubstance abusers and compared the PCUD patients with the patients without any substance use disorder (NSUD). The significance cut-off point was set at p <0.05.
Results
Sociodemographic characteristics and prevalence rates of cannabis abuse
Of 169 patients with a psychotic disorder, 77 (45.6%) had a co-morbid diagnosis of CUD. No significant differences were found between CUD patients and NCUD patients in terms of age (Z = −0.37, p = 0.711), specific diagnosis (different types of psychotic disorders) (χ2 = 12.82, df = 8, p = 0.118) and mean age of onset of the first psychotic episode (Z = −0.25, p = 0.801). CUD and NCUD groups differed significantly in gender (χ2 = 8.93, df = 1, p = 0.003). Sociodemographic characteristics of patients with a psychotic disorder are listed in Table 1.
Sociodemographic- and clinical characteristics of the CUD and NCUD groups of patients diagnosed with a psychotic disorder
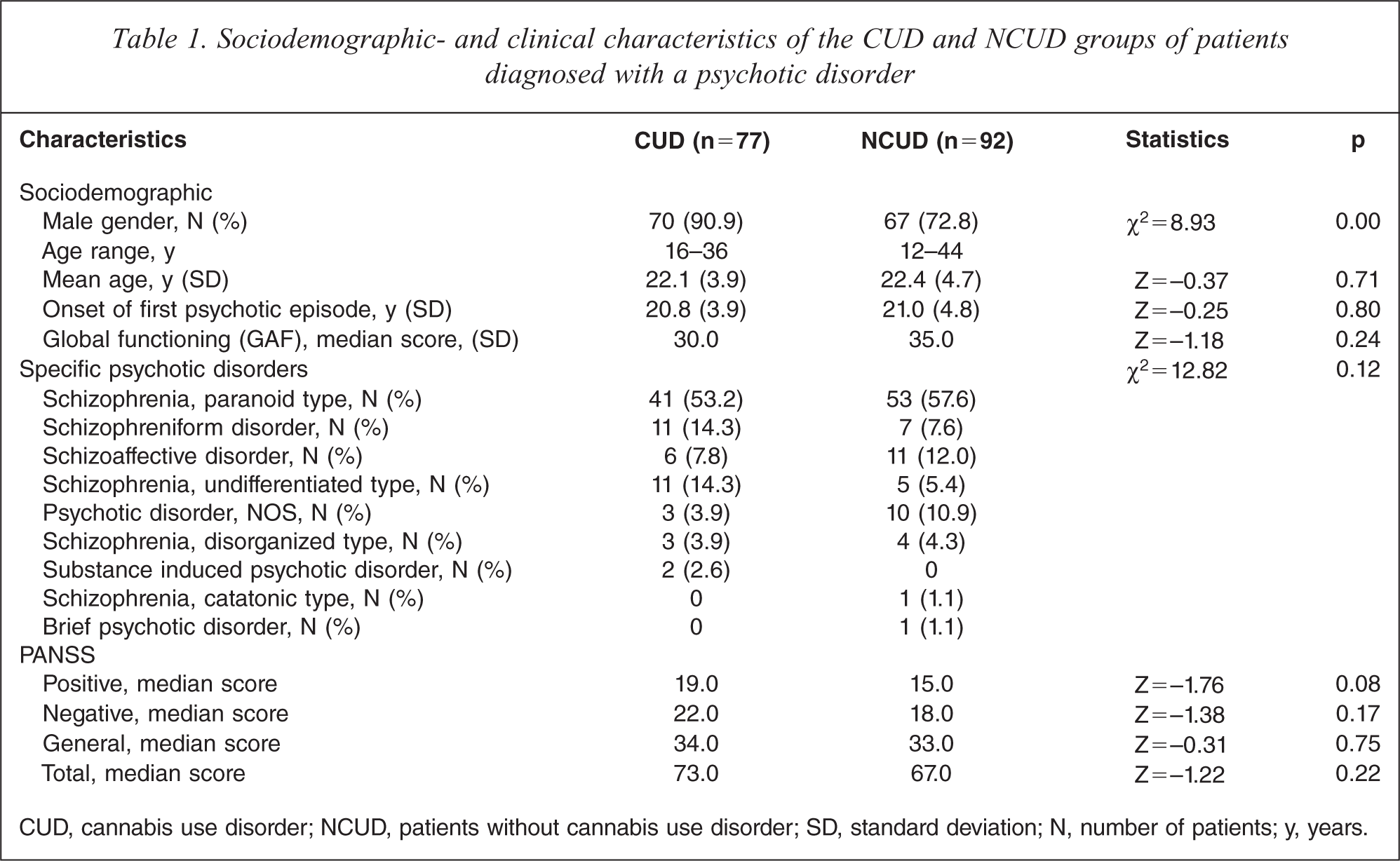
CUD, cannabis use disorder; NCUD, patients without cannabis use disorder; SD, standard deviation; N, number of patients; y, years.
Of 77 CUD patients, 71 (92.2%) started using cannabis before onset of the first psychotic episode. The remaining patients started using cannabis during (n = 4) or after (n = 1) the first psychotic episode. Mean age at which cannabis use started was 15.6 years (± 2.8). We also analysed the relationship between onset of prodromal symptoms and the onset of cannabis use. We found that 38 patients (49.4%) started using cannabis before the onset of the first prodromal symptoms, in 12 patients (15.6%) the prodromal period and the cannabis use started together and in 14 patients (18.2%) the cannabis use started after the beginning of the prodromal symptoms. We were not able to assess the onset of prodromal symptoms in 13 patients, so we could not consider these patients in this analysis.
In the UHR group, 16 (27.1%) of the 59 included UHR subjects had a co-morbid diagnosis of CUD. Table 2 lists socio-demographic characteristics of UHR patients. No significant differences were found between CUD patients and NCUD subjects in terms of gender (χ2 = 0.66, df = 1, p = 0.42). CUD and NCUD groups differed significantly in terms of age (U =2 12.0, p = 0.02).
Sociodemographic- and clinical characteristics of the CUD and NCUD groups of UHR patients
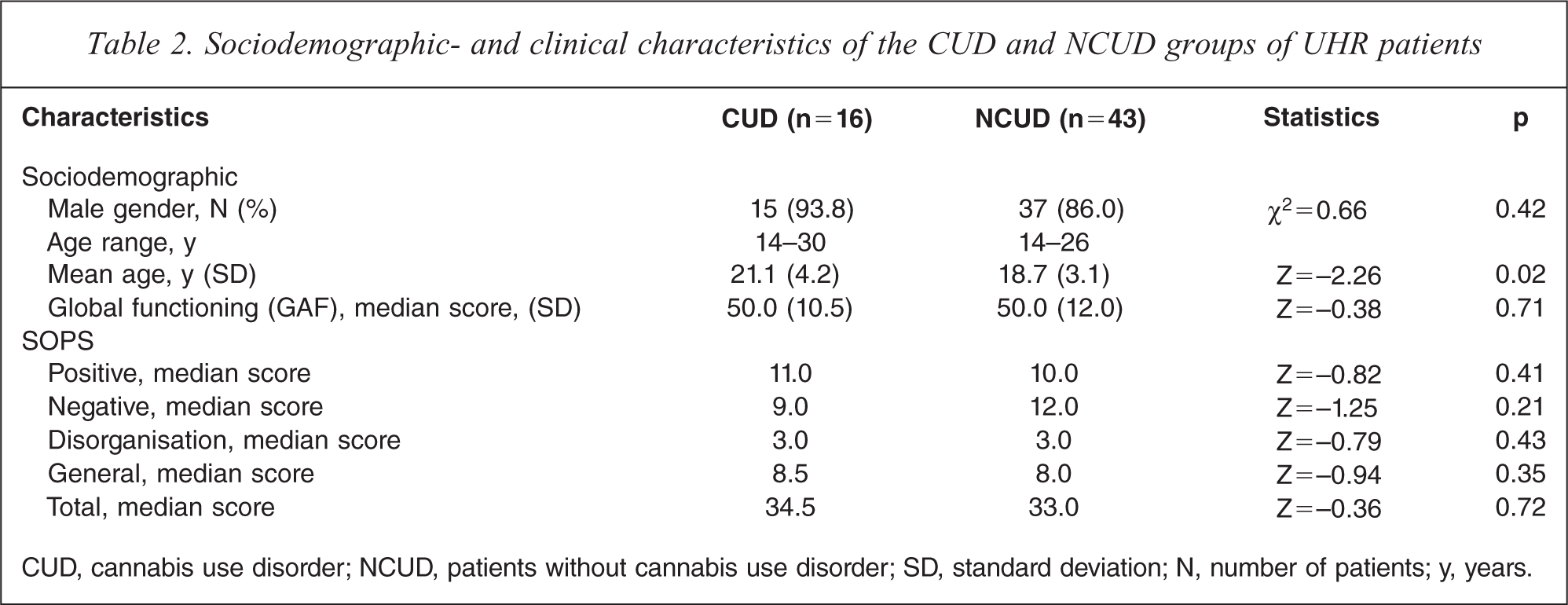
CUD, cannabis use disorder; NCUD, patients without cannabis use disorder; SD, standard deviation; N, number of patients; y, years.
Cannabis abuse and severity of psychotic symptoms in patients with a psychotic disorder
CUD patients did not significantly differ from NCUD patients on scores on the PANSS subscales (Table 1). However, when excluding multiple substance users to compare patients with cannabis use disorder but without other substance use disorder (pure cannabis users, PCUD) (N = 51) with patients without any substance use disorder (no substance use disorder, NSUD) (N=82), a significant difference was found in the scores on the PANSS positive subscale. Scores on this subscale were significantly higher for PCUD patients (Median = 20.00) compared to NSUD patients (Median = 15.00), (Z = −1.98, p = 0.047) (Table 3).
Clinical characteristics of the PCUD and NSUD groups of patients diagnosed with a psychotic disorder
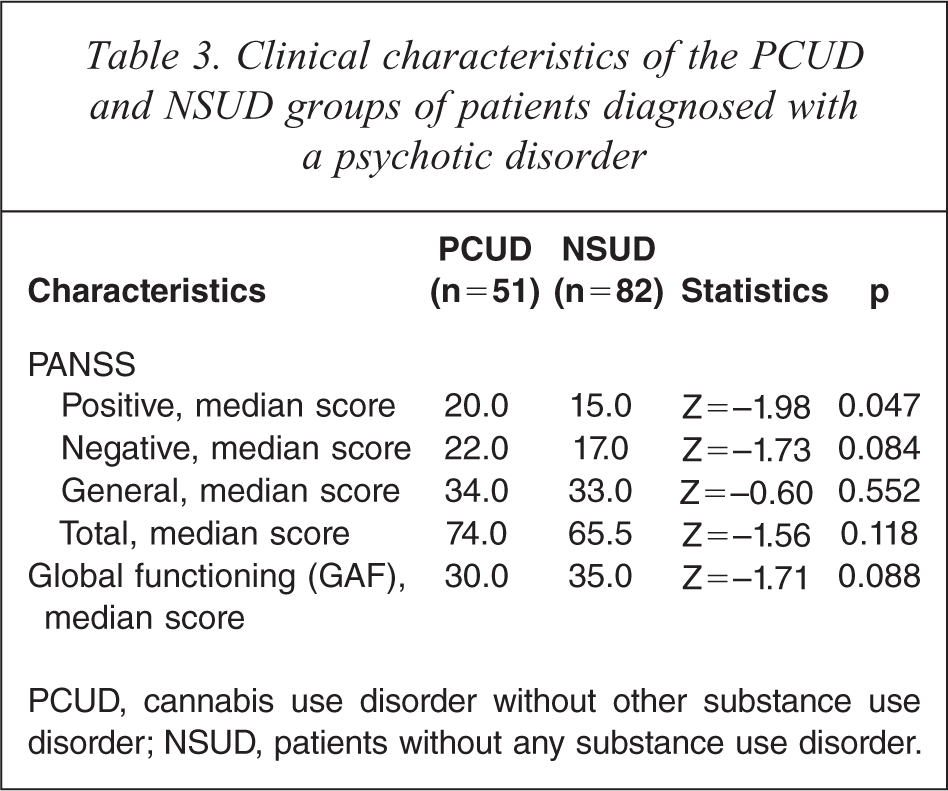
PCUD, cannabis use disorder without other substance use disorder; NSUD, patients without any substance use disorder.
We explored whether there was a correlation between amount of cannabis used during last month and severity of psychotic symptomatology. There was no significant correlation found between amount of cannabis use and scores on the PANSS.
Cannabis abuse and course in patients with a psychotic disorder
In the group of patients with a psychotic disorder, number of psychotic episodes and total duration of the psychotic episodes did not differ significantly between CUD and NCUD groups. Current GAF scores did not differ significantly between CUD and NCUD group. A trend for lower GAF scores in the PCUD group was found (Table 3), when PCUD patients were compared to NSUD patients.
Cannabis abuse, pre-psychotic symptoms and GAF scores in ultra high risk patients
CUD UHR patients did not significantly differ from NCUD patients in scores on all SOPS subscales (Table 2).
We explored whether there was a correlation between amount of cannabis used during last month and severity of pre-psychotic symptomatology on the SOPS subscales. A significant negative correlation was found between the amount of cannabis used during last month and scores on the SOPS negative subscale (rho = −0.309, N = 54, p = 0.023, two-tailed). No other significant correlations were found.
In the UHR group, GAF scores did not differ significantly between both groups.
Discussion
Prevalence of cannabis abuse in patients with a psychotic disorder and in patients at ultra high risk for psychosis
In this study, 45% of 169 patients with a psychotic disorder had a comorbid diagnosis of cannabis use disorder. Compton et al. [2] reported a comparable comorbid prevalence of cannabis use disorder (44%) in their study sample. Hambracht and Häfner [6], Green et al. [3] and Bersani et al. [11] reported a comorbid prevalence of cannabis use disorder in 14.2%, 22.5% and 26% of their study samples respectively.
In our study, almost all patients with comorbid cannabis use disorder started using cannabis before onset of the first psychotic episode (92.2%). Bersani et al. [11] reported on a patient sample in which 67% of the patients started using cannabis before onset of the psychotic disorder. Differences between these groups (patients who started using cannabis before onset of the first psychotic episode compared with patients who started using cannabis during or after the first psychotic episode) regarding psychotic symptomatology could not be studied in our study. However, the finding that such a large part of this patient population started using cannabis before onset of the psychotic disorder is remarkable. These results support the hypothesis that cannabis increases the likelihood to develop a psychotic disorder; however, an alternative explanation could be that patients start using cannabis during the prodromal period as a form of self-medication. In a second analysis we found that in 49.4% of the patients, cannabis use started before the onset of prodromal symptoms, while in 15.6% of the patients the prodromal period and cannabis use started together and in 18.2% cannabis use started after the first prodromal symptoms. Taken together, these results support the hypothesis that the use of cannabis could be a causal factor in the development of a psychotic disorder for most patients.
Mueser et al. [17] and Bersani et al. [11] both found a younger age of onset of the psychotic disorder in patients known with cannabis abuse. We were not able to replicate this finding this in our sample.
Cannabis use disorder in the UHR subjects was less prevalent compared to the group of patients with a psychotic disorder: Of 59 UHR patients 27% were diagnosed with cannabis use disorder. This result is comparable to the study of Kristensen and Cadenhead [14], in which 33% of UHR patients were diagnosed with cannabis use disorder. Phillips et al. [12] found that 18% of the UHR patients were diagnosed with ‘cannabis dependence’. The lower prevalence in the UHR patients compared to the group of patients with a psychotic disorder could possibly be explained by the difference in age between these two groups. UHR patients had a mean age of 19.3 years while the mean age of patients with a psychotic disorder was 22.3 years. Nevertheless, a prevalence rate of 27% in this UHR patient group is still substantial and underlines the need to further study the correlation between cannabis abuse and risk for developing a psychotic disorder.
Cannabis and severity of psychotic symptomatology
Evidence for the view that cannabis consumption increases the risk of psychotic outcome [18] or psychotic symptoms [5] led to our hypothesis that cannabis consumption might have adverse effects on psychotic disorders and could lead to more severe psychotic symptoms.
No significant differences in severity of psychotic symptomatology between cannabis abusing and non-abusing patients were found in our study. An association between the amount of cannabis consumption and severity of psychotic symptomatology was not found, suggesting that cannabis might have little short-term effects on psychotic symptomatology. These results are in accordance with the results reported by Dervaux et al. [9] and Scheller-Gilkey et al. [10]. However, Compton et al. [2] and Bersani et al. [11] reported significantly lower scores on the PANSS negative symptom subscale for patients with comorbid CUD. The study of Compton et al. [2] is comparable to our study on some main characteristics. However, they included 18 patients, which is a small sample compared to our sample size of 169 patients. The study of Bersani et al. [11] differed from our study in various ways and results can thus not easily be compared: they mainly compared a cannabis consumption group (not necessarily diagnosed with CUD) with a non-cannabis consumption group and studied patients with chronic schizophrenia, which differs from our sample of first episode patients.
Bersani et al. [11] excluded polysubstance users in order to study the specific impact of cannabis consumption on psychotic symptoms. We also did this and compared patients with only CUD (PCUD) with the group of patients with no substance use disorder (NSUD) on psychotic symptomatology. Contrary to Bersani et al., our results show no differences in negative symptoms between the groups. However, we found that the PCUD group had significantly higher scores on positive psychotic symptom subscales compared to the NSUD group. This finding is interesting and gives us reason to state that future studies on this subject should control for the use of other substances, as previously mentioned by Zammit et al. [19].
Studies on the relation between psychotic symptoms and substance abuse describe an association between both cannabis and other substances and severity of psychotic symptoms [20,21]. Since we did not find evidence for a protective effect of other drugs on psychotic symptoms in the literature, we think that the best explanation for our results is that patients with less severe positive symptoms represent a subgroup with a less severe psychotic disorder and a higher level of social functioning that is using more than one substance, possibly because this group is more active in obtaining these substances.
Psychosocial functioning and course of the psychotic disorder
Contrary to our hypothesis and to the findings reported by Caspari et al. [7], our results showed no significant difference in GAF scores (measuring level of psychosocial functioning) when patients with cannabis use disorder were compared to patients without cannabis use disorder. When polysubstance users were excluded and the PCUD group was compared with the NSUD group a trend for lower GAF scores in the PCUD group was found. This trend could be explained by the higher level of positive symptoms these patients experienced. Like we mentioned before, it is difficult to explain these findings in pure cannabis abusers because literature on this subject is sparse.
Pre-psychotic symptoms and psychosocial functioning in ultra high risk patients
We hypothesized that cannabis abuse in the ultra high risk group is associated with more severe pre-psychotic symptomatology and worse psychosocial functioning. In our sample, there were no differences between the CUD and the NCUD group on severity of pre-psychotic symptomatology as measured with the SOPS, though a negative correlation was found between the amount of cannabis used during the previous month and scores on the SOPS negative subscale: increased consumption of cannabis was associated with fewer pre-psychotic negative symptoms. There was no significant difference in GAF scores between the two groups. So far, existing literature has not studied the specific relationship between cannabis abuse and pre-psychotic symptoms, and this subject deserves further research. However, a decrease in negative symptoms in patients with a psychotic disorder which used cannabis has been described before [2,11,22–25]. A decrease in pre-psychotic negative symptoms in cannabis abusers could support the self-medicating theory. On the other hand, it is also possible that patients with less severe negative symptoms use more cannabis. The direction of this relationship is unclear and more research is needed to clarify this association.
Strengths and limitations of present study
In the Netherlands, personal use of cannabis is legal and generally accepted. Therefore, patients in our study may have been more reliable in reporting their use of cannabis compared to patient samples in other countries. However, a certain unreliability remains with self-reported data and underreporting may still have been present in our study.
In our study, data regarding other substances used were gathered, by controlling for the influence of other substances, the specific relation between cannabis abuse and psychotic symptoms could be studied. Furthermore, the strict criteria ‘cannabis use disorder in the diagnosis’ was used to explore long-term effects of severe cannabis consumption on psychotic symptomatology. This could be viewed as a strength as well as a limitation of our study. This criterion helps us to identify the group of cannabis users who are most likely to experience problems with their cannabis use; however, if patients use cannabis regularly but do not meet the criteria of CUD an important group could be missed. A limitation of our study is its cross-sectional nature, and cannabis use was retrospectively assessed. Furthermore, (compliance with) antipsychotic treatment was not controlled for; however, there were no differences in medication use between the two groups in our study.
Conclusions
Of the patients with a first episode of a psychotic disorder, 45% had a diagnosis of CUD, which confirms the formerly reported high prevalence rates of comorbid cannabis abuse in patients with a psychotic disorder. Almost all patients started using cannabis before the onset of psychosis. Of the UHR patients, 27% were diagnosed with CUD. No significant differences in severity of psychotic symptomatology were found between the CUD and the NCUD group of patients with a psychotic disorder. However, patients with pure cannabis use disorder (when users of other substances were excluded) had significantly higher scores on positive symptom subscales compared to patients without any substance use disorder. Furthermore, we found a trend for worse psychosocial functioning in patients with pure cannabis use disorder compared to patients without any substance use disorder. The direction of these associations needs further study.
For the UHR group, pre-psychotic symptoms did not differ when CUD patients were compared to NCUD patients. However, a negative correlation was found between the amount of cannabis used during the previous month and scores on the SOPS negative subscale: increased consumption of cannabis was associated with fewer pre-psychotic negative symptoms.
Further research should study the long-term effects of cannabis use, given the early beginning of cannabis consumption and the high prevalence of CUD in our study sample. Our study supports the need for specific treatment interventions for patients with co-morbid substance use disorders.
Footnotes
Acknowledgements