
Abstract
High rates of substance use disorders among people with psychosis have been reported in the USA [1], the UK [2] and Australia [3, 4]. Among people with psychotic disorders in Australia, a lifetime diagnosis of alcohol use disorder was found in 39% of male and 17% of female subjects, with corresponding figures of 36% and 16% for a lifetime diagnosis of other drug abuse or dependence [4]. Slightly higher rates were reported in an earlier Australian study of outpatients with schizophrenia [3]. The odds of having a substance use disorder in specialist mental health treatment settings are approximately double that of the non-treated population with mental disorders [1]. A range of psychosocial problems have been associated with comorbidity, including polydrug use and crime [5] and poorer outcomes, in the domains of psychiatric symptomatology and social dysfunction [6]. Implications are that interventions for comorbidity should be the core business of health services; and skill in their delivery needs to be a fundamental capability of mental health practitioners [7].
Three randomized controlled trials (RCTs) have been conducted with the aim of reducing substance use among people with psychotic disorders, within the context of ongoing provision of usual assertive case management in the community. Two RCTs of individual motivational interviewing (MI) and cognitive behaviour therapy (CBT) among people with psychotic disorders have reported only modest results on substance use outcomes, with better general functioning among those who received the MI/CBT interventions compared to those who received usual treatment, around 9 months after treatment [8–10]. Short-term results from a third RCT among people with psychotic disorders [11], which used group MI and CBT within a harm minimization paradigm over six 90 min sessions, were promising. Compared to a control condition that received a single hour-long session of education regarding drug use, the MI/CBT condition showed significantly greater reductions in global psychopathology, drug use, severity of dependence, antipsychotic medication dose and a lower rate of hospitalization at 3 months after intervention. Longer-term follow-up results have not been reported.
There are several reasons for conducting group interventions among people with comorbid psychotic and substance use disorders, including: promotion of exploration of the social (and other) benefits and negative impacts of substance use; opportunities to share experiences and coping strategies, as well as increasing connections with friends who do not use drugs and alcohol problematically; and cost-effectiveness, in terms of therapist time [12]. A review of 36 research studies assessing group interventions for people with comorbid severe mental and substance use disorders concluded that the most encouraging interventions include the following features: assertive outreach; integration within the treatment setting; MI for substance abuse; and follow up longer than 1 year, to attain clinically meaningful reductions in substance use over time [13]. The intervention reported in the present study incorporated these features and, to the authors’ knowledge, it is the first Australian effectiveness study to do so. In addition, the intervention was conducted in a rural area by mental health and drug and alcohol clinicians and results have implications for clinical implementation within rural settings.
The primary aim of this service evaluation project was to evaluate whether an open-ended weekly outpatient group intervention was effective in reducing substance use and improving symptomatology and general functioning among people with psychosis. It was hypothesized that, compared with baseline, at follow up the intervention would be associated with: lower ratings of negative consequences from substance use; improved treatment compliance; improved control of psychiatric symptoms; fewer inpatient stays; fewer unscheduled outpatient treatment contacts; and improved global psychosocial functioning. It was also hypothesized that participants who remained in the group intervention longer would demonstrate significantly greater or more sustained improvement on these variables compared to those who attended fewer sessions.
Method
Sample
The study was conducted in the Mid North Coast Mental Health Region (Northern Sector) of New South Wales (NSW), Australia, approximately 500 km north of Sydney. The Coffs Harbour Mental Health Team serviced a population of 80 000 people over an area of approximately 450 km2. Participants were recruited from the three existing community mental health services in the area between June 1992 and June 1998. Inclusion criteria were: (i) a clinical diagnosis of an Axis I, DSM-IV [14] psychotic-spectrum disorder or bipolar disorder, confirmed by a psychiatrist and present for at least 2 years prior to recruitment to the study; and (ii) a concurrent DSM-IV diagnosis of substance abuse or dependence [14], or periodic substance use that resulted in habitual patterns of problematic negative psychosocial outcomes, including exacerbations of psychiatric symptoms and/or anti-social behaviours, for at least the preceding 2 years. People who had previously met these substance use criteria, but who were in remission at the time of recruitment into the study, were included as participants. This methodological approach of defining substance use problems by their effect, rather than strict reference to diagnostic criteria, has been used recently by several researchers [15]. Exclusion criteria were: (i) Axis II diagnosis in the absence of an Axis I disorder; or (ii) an inability to benefit from the group intervention due to symptom severity or cognitive impairment. When selection criteria were met, participants were invited to attend the weekly groups. Because this was primarily a service evaluation project, formal approval from the regional ethics committee was not required, with the key outcome measures all being based on ratings by clinicians from within the participating services.
Procedure
Clinician ratings were completed for four retrospective 3 monthly baseline observations and up to 12 3 monthly post-recruitment observations, over a maximum period of 3 years of the open-ended group intervention. The outpatient group intervention was ongoing and was held weekly for 60–90 min. Each group was co-convened by experienced mental health and drug and alcohol clinicians, a psychologist or drug and alcohol counsellor and a nurse, who were trained in the group intervention. The goal of MI in the groups was to assist participants to understand more about their mental and substance use disorders and to make informed choices about treatment. Group leaders worked with the four general principles outlined by Miller and Rollnick [16]: expressing empathy; developing discrepancy; rolling with resistance; and supporting self-efficacy. Substance use reduction goals were determined collaboratively with each individual. The substance associated with the most harm at commencement of the group was initially focused on, with the goal of reducing use to non-problematic levels of consumption. Each group member was encouraged to identify the drugs that they had ever used, and the usage levels and contexts within which psychiatric symptoms and adverse social and legal consequences had been found to commence. Relapse prevention (RP) strategies to avoid psychiatric relapses, related to substance abuse and other behaviours and stressful situations, were developed and reinforced with individual group members. Guidelines for substance abuse relapse prevention approaches were followed, although these were not specifically developed for people with psychotic disorders [17]. In this way, behavioural rehearsal of effective prevention strategies tailored to each group member was achieved and reinforced both by reported successes and lapses.
A flexible agenda was set each session, allowing the group leaders to reduce confrontation and to maintain participant interest and involvement. Due to the low attention span of some participants, members were able to enter and leave each session while it was in progress if they felt the need. Information was kept simple, brief and specific, with conclusions and behavioural suggestions defined succinctly.
Measures
Service records were used to measure duration of time in psychiatric hospital and unscheduled and out-of-hours service contacts. Case manager ratings of participant functioning were recorded on three rating schedules: the Case Manager Rating Scale (CMRS) [18], the Case Manager Rating Form (CMRF) [19], and the Life Skills Profile (LSP) [20]. All measures were coded in the same direction, such that higher scores indicated poorer functioning or higher service usage.
Case Manager Rating Scale
The CMRS, which was designed for application by experienced long-term case managers, rates levels of substance-related problems found among people with severe mental disorders residing in the community [18]. It has shown very high interrater reliability and better concurrent validity rates than for self-report questionnaires [21]. Global severity ratings were initially made for each of the substances currently being used, with reference to specific criteria reflecting negative physical and psychosocial consequences of use, rather than quantity and frequency of use. There were five categories of substance use severity, each with detailed descriptors: (i) none; (ii) mild; (iii) moderate; (iv) severe; and (v) extremely severe. Such ratings allow for the detection of possible disturbances in functioning associated with relatively low level substance use [21]. Average maximum CMRS ratings per assessment interval were used in the present analyses (i.e. using the highest CMRS rating at each time point, regardless of the substance used).
Case Manager Rating Form
The three dimensions used in the present study were severity of psychiatric symptoms; substance use; and level of treatment non-compliance, each rated from least to most severe (1–7). The CMRF shows good inter-dimension correlation and good concurrent validity when measured against independent indicators of diagnosis and treatment resources required [19].
Life Skills Profile
The LSP is a 39-item global measure of psychosocial functioning [20], with the full-scale score reported in the present study. The LSP contains items with low subjectivity, is sensitive to small variations in levels of functioning over time, has high interrater reliability, was normed on people with schizophrenia, and can sensitively differentiate levels of functioning between patients being treated in the community [20, 22, 23].
Group intervention and other service attendance
The number and length of inpatient stays and type of outpatient treatment (scheduled and in hours, unscheduled and in hours, or unscheduled and out of hours) were accessed from medical records. Group intervention attendance was defined as the number of times that a participant was present at the weekly 60–90 min group treatment session.
Statistical analysis
Analyses pertained to the baseline period and the subsequent 3 years. To reduce the impact of missing data points within the designated time period (comprising 18.8% of the follow-up data), aggregate ratings for each year were calculated by averaging each person's data for all available quarters. Thus, average ratings per quarter were calculated for the baseline year and for years 1, 2 and 3. Missing follow-up data for year 3 (n = 12) were estimated by carrying forward aggregate data for year 2.
Data were analysed using SPSS for Windows (version 12.0; SPSS, Chicago, IL, USA). For the continuous outcome variables, analyses of variance (ANOVAs) were used to examine patterns of change over time. Separate analyses were conducted for each of the seven selected outcome measures: severity of substance-related problems (maximum CMRS ratings); CMRF ratings for substance abuse, psychiatric symptoms, and treatment non-compliance; psychosocial functioning (LSP total score, reverse scored); days spent in psychiatric inpatient facilities; and unscheduled service usage. In addition, these measures were included in a T-technique (i.e. total-variation) factor analysis, using data from across all four phases (baseline, years 1–3; n = 156 records). A two-factor solution emerged, which accounted for 59.8% of the variance. The first factor, which we have labelled ‘F1: overall severity’, consisted of five measures: the two substance use indices (from the CMRS and CMRF); psychiatric symptoms; treatment non-compliance; and LSP total score. The second factor, labelled ‘F2: acute mental health (MH) services usage’, consisted of two measures: psychiatric inpatient days; and unscheduled service usage. Scores on these two factors were obtained by standardizing the measures loading on each factor (against the relevant grand mean and SD) and then averaging these standardized scores (i.e. using unit weights, not factor loadings). Profiles for these two factors are reported because they provide a convenient summary of the study's findings.
Results
Baseline patient characteristics
Forty-nine people were referred to the group, of whom 10 were excluded from the project (three with severe and chronic cognitive dysfunction; three living in remote areas, who experienced transport problems; and four who relocated out of the area before group attendance). Thus, 39 participants commenced the group. Their mean age was 33.42 years (SD = 8.95) and the majority were male (73.7%): Australian born (100.0%); single (97.4%); and receiving welfare support (100.0%). The mean age at onset of psychiatric disorder was 22.69 years (SD = 4.83). Schizophrenia was the primary diagnosis (79.5%), followed by bipolar disorder (12.8%) and schizoaffective disorder (7.7%). One-tenth of the sample (10.3%) had a DSM-IV Axis II diagnosis (personality disorder), in addition to an Axis I diagnosis. Nearly one-third of the sample (30.8%) had an Axis III diagnosis (general medical condition), the most common being chronic obstructive airways disease (12.8%). Except for one participant (2.6%), the sample reported problematic substance use (as defined earlier), with the main substances used at baseline being alcohol (43.6%), cannabis (28.2%), and polydrug use (25.6%). In terms of severity of substance use at baseline (based primarily on CMRS ratings), 10.3% were ‘mild’, 53.8% were ‘moderate’ (the equivalent of DSM-IV ‘substance abuse’), 28.2% were ‘severe’, and 7.7% were ‘extremely severe’ (with the latter two categories corresponding to DSM-IV ‘substance dependence’).
The left-hand columns of Table 1 report mean substance use, symptomatology and service usage profiles for the group at baseline. Interpreting these scores in terms of the original rating scale anchors, the sample experienced: substance use-related problems at a level of moderate severity (i.e. evidence of persistent problems or dangerous use, mean maximum CMRS rating = 3.21, range 1–5); current substance use of more than once a week (low quantity; mean CMRF substance abuse rating = 6.16, range 3–7); positive or negative psychiatric symptoms that were significant but intermittent (or mild but constant; mean CMRF rating = 5.44, range 2–7); moderate treatment compliance, with around 60–70% of treatment recommendations being carried out (mean CMRF rating = 4.18, range 1–7); and mid-range psychosocial functioning (mean total LSP score = 83.68, range 58.33–137). They also spent an average of 5.48 days per quarter in an inpatient psychiatric facility (range 0–55.75) and made an average of 4.12 unscheduled service contacts (range 0–17.50).
Mean aggregate scores for substance use, psychiatric symptomatology and service use over time (n = 39)
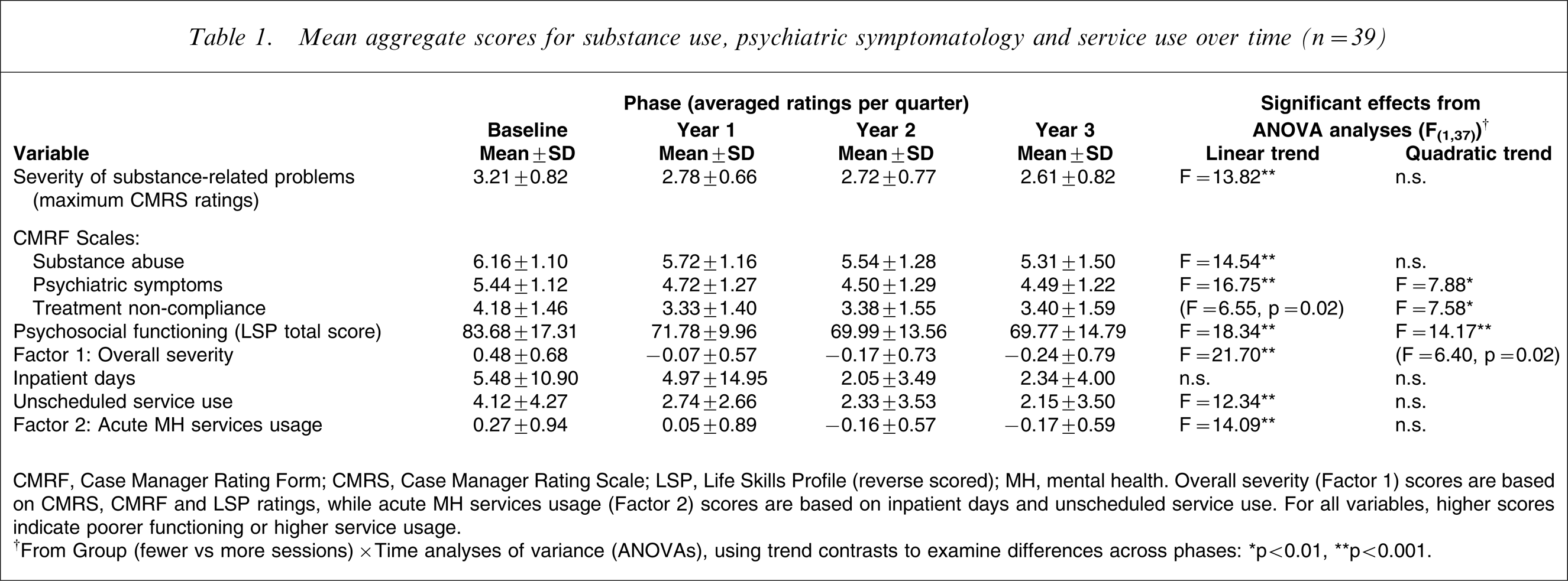
CMRF, Case Manager Rating Form; CMRS, Case Manager Rating Scale; LSP, Life Skills Profile (reverse scored); MH, mental health. Overall severity (Factor 1) scores are based on CMRS, CMRF and LSP ratings, while acute MH services usage (Factor 2) scores are based on inpatient days and unscheduled service use. For all variables, higher scores indicate poorer functioning or higher service usage.
†From Group (fewer vs more sessions)×Time analyses of variance (ANOVAs), using trend contrasts to examine differences across phases: ∗p < 0.01, ∗∗p < 0.001.
A preliminary series of analyses was also conducted using ratings and service usage data from the four quarters of the baseline year. Repeated measures ANOVAs were used to examine differences across quarters for each of the seven outcome measures and the two aggregate factors (i.e. overall severity and acute MH services usage). There were no statistically significant differences in any of these analyses, reinforcing our decision to average the four quarters to obtain scores for the baseline year, but also suggesting that, on average, clients recruited to the study had relatively stable illness trajectories (i.e. they were neither recovering nor deteriorating).
Treatment group attendance
The average number of group sessions attended was 28.51 (SD = 24.61, range 1–116). Based on a median split of treatment group attendance, two subgroups were identified: those who attended fewer sessions (n = 19), who participated in an average of 10.63 sessions (SD = 7.26, range 1–21); and those who attended more sessions (n = 20), who participated in an average of 45.50 sessions (SD = 23.18, range 23–116). In addition to attending fewer sessions overall, the first subgroup displayed less regular attendance, with an average session attendance rate during quarters spent in treatment of 30.5%, compared with 57.6% for the other subgroup. There were no differences between the treatment attendance subgroups in age, gender, diagnostic characteristics, or the overall severity of their baseline symptoms or substance use (Factor 1).
Changes in substance use, symptomatology and service usage
The right-hand columns of Table 1 present mean scores for the selected substance use, symptomatology and service usage measures for years 1, 2 and 3. A series of Group (fewer vs more sessions)×Time (baseline, years 1–3) ANOVAs was conducted to examine changes in substance use, symptomatology and service usage. Within these analyses, trend contrasts (i.e. orthogonal polynomials) were used to examine differences across phases, which was considered to be an appropriate strategy given the open-ended nature of the treatment intervention. There were no significant main effects for group in any of these analyses and the only significant group×time interaction contrasts related to patterns of service usage. However, as shown in Table 1, there were significant time effects (improvements) for all variables except for inpatient days. Specifically, there were significant linear reductions for the two substance use measures, for unscheduled service use, and for overall acute MH services usage (Factor 2). For two of the remaining measures, there were effects (p = 0.02) that approached the threshold for statistical significance. Treating these effects and the remaining significant effects reported in Table 1 as a block, there were significant curvilinear reductions (i.e. linear and quadratic effects) in psychiatric symptomatology, treatment non-compliance, psychosocial functioning, and overall severity (Factor 1), with the largest improvements on these measures occurring between baseline and year 1.
There was a significant group×cubic trend interaction contrast for overall acute MH services usage (Factor 2; F(1,37)=8.55, p < 0.01) and a comparable effect for one of its constituent variables, unscheduled service use (F(1,37)=6.56, p = 0.02). These differences are illustrated in Figure 1, which displays changes in overall severity (Factor 1) and acute MH services usage (Factor 2) for the two subgroups defined by their treatment session attendance. Those who attended more sessions reported an initial reduction in their usage of acute MH services (from baseline to year 1), followed by a rebound from year 1 to year 2, and then a levelling out. However, the opposite pattern was observed among those who attended fewer sessions, with little change between baseline and year 1, and between years 2 and 3, but a substantial reduction between years 1 and 2.
Changes in overall severity (Factor 1) and acute mental health (MH) services usage (Factor 2) over time by treatment session attendance (n = 39).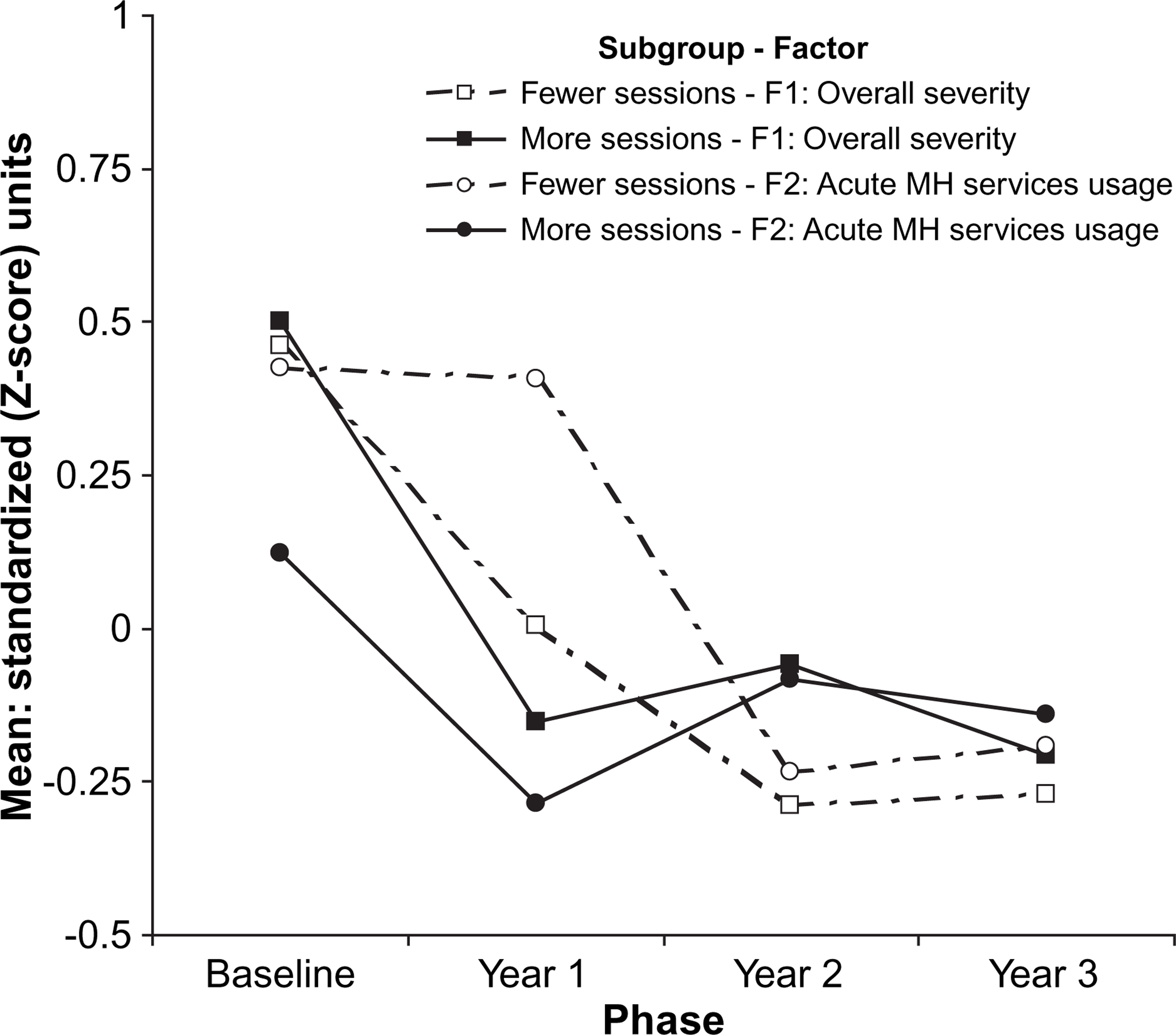
Ignoring differences between subgroups, and as shown in and Figure 1, there was a more marked reduction across the course of the project in overall severity (Factor 1: 0.48 to −0.24) relative to acute MH services usage (Factor 2: 0.27 to −0.17), corresponding to net reductions of 0.72 and 0.44 standardized (or effect size) units, respectively. Moreover, three-quarters of the observed reduction in overall severity occurred in the first year (0.55/0.72), compared with half of the reduction in service usage (0.22/0.44). The correlation between overall severity and acute MH services usage (i.e. scores on the two factors) was negligible for the baseline period and year 1 (r = 0.18 and 0.10, respectively) but somewhat higher in years 2 and 3 (r = 0.25 and 0.47, respectively).
Discussion
The present results support the view that extended group interventions are feasible for the subsample of individuals with comorbid psychosis and substance use disorders referred to such programmes [12]. Because the average number of group sessions attended was 28.51, it appears that people with psychotic disorders who are rated by clinicians as having (on average) moderate levels of substance abuse and psychiatric symptomatology are willing to attend several months of group outpatient intervention. Further, the results of the present study also support the view that outpatient group interventions can be effective in reducing substance use among people with psychotic disorders when delivered within the context of assertive outreach, integrated treatments, MI for substance abuse, and with follow-up available longer than 1 year [13]. Compared to a baseline period of 1 year, the present group intervention was associated with significant improvements in substance use measures, symptomatology, treatment non-compliance, and overall psychosocial functioning (comprising Factor 1), as well as reductions in acute MH services usage (Factor 2) and, in particular, unscheduled service usage.
Consistent with other recent research [24], it appears that reduced substance use among people with psychotic disorders is associated with significant benefits in other behavioural domains, and that harm reduction approaches are feasible [25]. Other researchers have argued for allowing people with severe mental and substance use disorders to choose harm minimization goals [26–28] and that by doing so, more participants, especially young people, could be engaged in treatment. In the current study, significant linear reductions in substance use ratings were accompanied by significant curvilinear changes in symptomatology, treatment non-compliance and general functioning, the latter being more marked during the first year. These differential rates of change (i.e. progressive vs more marked in year 1) between variables indicate that some behavioural domains may respond more rapidly than others to intervention. Across the years in which the highest levels of substance use, treatment attendance and/or change occurred, scores on the aggregate severity and MH service usage indices were relatively independent, but they were moderately associated during more stable periods. This pattern suggests that treatment attendance (or, possibly, service engagement) could have contributed to a more stable or predictable service utilization profile, or it could simply reflect idiosyncratic features of this particular sample. A recent report of 10 year recovery rates for clients with co-occurring schizophrenia and substance use disorders also suggests that recovery is a multidimensional concept, with steady improvement overall but relative independence between the different outcome domains [29].
In addition, it appears that significant change in functioning (including substance use and symptomatology) can occur within the context of a regular but relatively short outpatient group intervention. Those participants who attended an average of 10.63 sessions (the fewer-sessions subgroup) experienced comparable improvements in substance use, symptomatology and functioning relative to those participants who attended an average of 45.50 sessions (the more-sessions subgroup). However, the significant group×cubic trend interaction effects that were found for acute MH services usage suggest that retention in the group intervention was associated with a reduced likelihood of relapse. On the basis of these results, clinical recommendations would be that attendance for at least 10 group sessions may be associated with significant reductions in substance use and symptomatology and that attendance over a 1 year period may be further associated with prevention of relapse and comparatively less unscheduled service use.
To our knowledge this is the first report of the effectiveness of a group intervention for this population conducted in a rural setting and with groups led by local clinicians from mental health and drug and alcohol services, including co-leaders who were not originators of the intervention model. The interventions delivered here should be generalizable to other clinical settings, staff and clients, especially considering the open-ended nature of the group, allowing group entry at any point, and the flexible delivery of MI and RP interventions using published treatment strategies [16, 17].
Limitations of this service evaluation project include small group numbers, the lack of a no-intervention control condition, reliance on clinician ratings of symptomatology and substance use, and the absence of the individual assessment and follow-up procedures that tend to characterize formal research studies. However, these limitations largely reflect the clinical and rural nature of the sample. The absence of changes within the baseline year also suggested that the recruited clients had stable illness trajectories that might otherwise benefit from a targeted intervention. Although concordance between clinician ratings in different domains lends veracity to the findings, additional self-report measures would have allowed measurement of change across substance use classes, thereby allowing analysis of possible differential effectiveness of the intervention between substances.
Clearly, this evaluation of a group intervention led by mental health and drug and alcohol clinicians within the context of usual clinical care requires replication among larger samples, using an RCT group design, in various settings, with blind assessor ratings and administration of clinician and self-report instruments. However, it would be extremely difficult to undertake a long-term follow up within the context of an RCT and, for example, to exclude people from treatment for an extended period. Therefore, ideally, complementary service-based evaluation projects and more formal research trials need to be undertaken in parallel, preferably using comparable recruitment, assessment, intervention and analysis procedures.
Footnotes
Acknowledgements
Staff and clients of the participating centres provided valuable encouragement and support for the project. Funding was received from the Australian Commonwealth Department of Human Resources, through a National Drug Crime Prevention Grant. We also wish to thank Louise Thornton for her assistance with manuscript preparation.