
Abstract
Objective:
This study aims to describe the clinical course of psychotic disorders, including the premorbid history, symptoms and level of functioning in a group of children and adolescents treated by paediatric mental health services, mainly as inpatients.
Method:
A sample of 45 children and adolescents with a psychotic disorder (mean age 13.2 years) was assessed using questionnaires, semi-structured interviews, parent interviews and file audit. The symptoms of those with a schizophrenia spectrum disorder (SSD) were compared to those with a mood disorder (MD).
Results:
This population showed a high level of premorbid impairment, including previous treatment for other psychiatric disorders. As well as hallucinations and delusions, high levels of self-harm, aggression, anxiety and depression were reported. The SSD and MD groups differed mainly in their levels of premorbid functioning.
Conclusions:
While it is well known that childhood-onset schizophrenia is a severe disorder with a poor outcome, this study found that young people diagnosed with other psychotic disorders also have significant impairment and are likely to require high levels of care to maximize their functional recovery.
Introduction
Psychotic disorders in children and younger adolescents are uncommon. However, despite the recent interest in high-risk mental states, there is little information on the longitudinal course of psychotic symptoms in children and younger adolescents. Auditory hallucinations have been widely documented in non-psychotic children attending child psychiatry services (Dhossche et al., 2002; Schreier, 1998) but follow-up studies are limited. Older studies such as Garralda (1984) hypothesised that hallucinations in children were a benign phenomenon, as she found that no children reporting hallucinations (from a small inpatient sample with diagnoses of anxiety or conduct disorder) had a psychotic disorder as adults. More recent studies suggest that a subgroup of children with hallucinations go on to develop a psychotic illness. A consecutive outpatient clinic sample of 90 French children aged from 5 to 12 years found that half of the 15% who reported hallucinations initially were hallucination free at 12 months, while a third had ongoing symptoms and came close to meeting criteria for major mental illness (Askenazy et al., 2007). Sixty percent of a sample of 80 Dutch children with auditory hallucinations (recruited from clinics and media appeals) reported no hallucinations 3 years later, but 16% had developed delusions (Escher et al., 2002). Symptoms were more likely to persist in those with diagnoses of anxiety, depression or dissociative disorder. Other risk factors were behaviour problems, negative symptoms and more frequently heard or more negative voices (Escher et al., 2004).
Children and adolescents with post-traumatic stress disorder (PTSD) were particularly at risk of auditory hallucinations (Hlastala and McClellan, 2005; Jessop et al., 2008). Some authors report PTSD hallucinations as phenomenologically different to those in schizophrenia (Hardy et al., 2005), while others report them as being indistinguishable (Jessop et al., 2008).
Children in community samples also report auditory hallucinations, with two studies reporting a rate of 8% (McGee et al., 2000; Scott et al., 2006). Hallucinations were more likely in children with anxiety, depression, family dysfunction and inattention or hyperactivity. When the cohort reported by McGee and colleagues was followed up 15 years later, at age 26, a quarter of those with psychotic symptoms at age 11 met criteria for schizophreniform disorder (Poulton et al., 2000).
In clinical situations, many children will be brought for assessment because of other concerns, but also report transient psychotic symptoms, typically auditory hallucinations with associated distress. At first presentation they often meet diagnostic criteria for depression, PTSD and anxiety or behaviour disorder but not any of the psychotic disorders. Some will have a clear onset of symptoms and good premorbid functioning, but many have a long history of developmental, behavioural and emotional problems and may have a confusing mix of symptoms that meet criteria for several disorders.
Symptom constellations seen in children and adolescents include pervasive developmental disorder (PDD) with bizarre thoughts and behaviours, or children with a history of abuse and neglect who have problems with mood regulation, behaviour and transient psychotic symptoms. Some symptom constellations, such as multiple complex developmental disorder (MCDD) (De Bruin et al., 2007) or the multidimensionally impaired group (MDI) (Stayer et al., 2005) are well described but their relationships to other disorders are unclear. In practice, the differential diagnosis of psychotic symptoms in childhood can be so difficult that some authors talk about ‘diagnostic hypotheses’ rather than an accurate diagnosis, especially at first presentation (Lee et al., 2003). Complicating factors include the difficult task of assessing a decline in functioning in children with chronic premorbid impairment and the need to consider symptoms in a developmental context, particularly in those with intellectual impairment or PDD (Starling and Dossetor, 2009). As with the late adolescent/early adulthood-onset psychotic disorders an accurate diagnosis may only be possible with time.
There is one psychotic disorder described in children, childhood-onset schizophrenia (COS), where a large amount of information about the phenomenology and natural history is available. COS is a rare disorder with a prevalence of less than 1/10,000 (Thomsen, 1996) where children aged 12 years and under display symptoms meeting full criteria for schizophrenia (Asarnow et al., 2004; Frazier et al., 2007; McDonell and McClellan, 2007; Rapoport et al., 2008). The latest information about COS comes from large research cohorts such as the Childhood-onset Schizophrenia Study at the National Institute of Mental Health (NIMH) (Rapoport and Inoff-Germain, 2000). These studies tend to draw from a wide geographical range and have strict exclusion criteria. COS appears to be a severe form of the more common late adolescent/early adult-onset disorder (Alaghband-Rad et al., 1995; Frazier et al., 2007). Specific findings include more premorbid impairment than seen in those with adult-onset schizophrenia, with an increased prevalence of cytogenetic (Addington and Rapoport 2009; Nicolson et al., 1999) and developmental abnormalities, including PDD and mental retardation (Rapoport et al., 2009; Sporn et al., 2004). Premorbid social difficulties (Nicolson et al., 2000) and motor abnormalities (Whitfield et al., 2005) are more commonly reported. A strong family history of schizophrenia is also more likely (Nicolson et al., 1999). The onset of illness is often insidious (Russell, 1994), with cognitive deterioration (Bedwell et al., 1999) and neuroanatomical changes (Arango et al., 2008) tending to occur early in the illness. However, very few children with psychotic symptoms meet diagnostic criteria for COS, and by the time diagnostic criteria are met they tend to be unwell with significant disability.
Bipolar affective disorder can also present in childhood, but lengthy discrete episodes of mania with psychotic symptoms are rare (Pavuluri et al., 2004, Anonymous, 2001). Prepubertal bipolar disorder is currently an area of controversy, a detailed discussion of which is beyond the scope of this paper, but, in summary, those who favour widening the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) criteria for children consider irritability or labile mood in children to be equivalent to elevated mood in adults. Their justification for this is that retrospective studies of adults suggest that many had several years of untreated emotional lability, irritability and mixed mood states before they were correctly diagnosed with bipolar disorder (Biederman et al., 2003; Pavuluri et al., 2005). Critics of this expanded definition say that it includes other disorders such as attention deficit hyperactivity disorder (ADHD) and oppositional defiant disorder, has an unknown natural history, and may even risk identifying normal children as disordered, exposing them to inappropriate treatments (Parry and Allison, 2008).
In summary, there is a limited amount of information available about the presentation and course of psychotic symptoms in children and adolescents, apart from the rarest and most severe variant, COS. While transient or isolated symptoms were previously thought to be benign, there is now increasing evidence that a percentage of children with such symptoms will go on to develop psychotic disorders. This study aims to describe the clinical course of psychotic disorders, including the premorbid history, symptoms and level of functioning in a group of children and adolescents seen by paediatric mental health services.
Methods
Study subjects
The subjects for this study were 45 children and teenagers all under the age of 17 years with positive symptoms of psychosis (hallucinations and delusions or formal thought disorder that persisted for a minimum of 3 days). They were recruited from psychiatry services at either the Children’s Hospital at Westmead (CHW) (a tertiary referral hospital for a large part of the state of NSW that also supplies emergency and outpatient services to Western Sydney) or the Western Sydney Area Health Service (two community child and adolescent psychiatry teams and an adolescent inpatient unit) between July 2006 and December 2010. All but five subjects had spent time as inpatients at CHW, and one was admitted to another Western Sydney inpatient unit. Three subjects were initially seen in the community but were later admitted owing to severity of symptoms. Subjects were referred to this study by their treating psychiatrist and were included in the study if both they and a parent consented and their presentations met the diagnostic criteria for inclusion.
Two of the authors (JS, a child and adolescent psychiatrist; CH, a psychologist and mental health nurse) conducted the interviews with the subjects. Two other child psychiatrists confirmed the diagnosis of a psychotic disorder using DSM-IV criteria, after questionnaire and file review. Exclusion criteria were epilepsy, previous head injury causing a loss of consciousness for 10 minutes or greater, an organic cause for the psychotic symptoms, treatment with electroconvulsive therapy (ECT) in the past 6 months, or an inability to speak sufficient English to understand the study questions. Prior mental health contact with non-psychotic symptoms did not disqualify them from inclusion in the study.
Parents and adolescents gave written informed consent to participate, in accordance with Australian National Health and Medical Research Council guidelines. The Human Research Ethics Committees of the Children’s Hospital at Westmead, the Western Sydney Area Health Service and the University of Sydney approved the study.
Study measures
Diagnoses were made using the Structured Clinical Interview for DSM-IV-TR Axis 1 Disorders (SCID-1) (First et al., 2002). The adult version of the SCID was used as the psychosis and mood disorder modules are identical to those used in the child version, but the modified probe questions of the KID-SCID were used if needed (Matzner et al., 1997). The diagnoses made were schizophrenia spectrum disorders (schizophrenia, schizophreniform and schizoaffective disorder), mood disorder (bipolar affective disorder, psychotic depression), psychotic disorders not otherwise specified (PD NOS) as diagnosed by SCID-1 criteria and isolated psychotic symptoms (IPT), where there were hallucinations or delusions that did not reach the threshold to diagnose any of the other disorders.
The severity of psychotic symptoms was measured using the Positive and Negative Symptom Scale (PANSS) (Kay et al., 1986). Mood symptoms were assessed using The Childhood Depression Inventory (CDI) (Sitarenios and Kovacs, 1999), the Young Mania Rating Scale (YMRS) (Young et al., 1978), and the Depression, Anxiety and Stress Scale (DASS) (Lovibond and Lovibond, 1995). Premorbid social adjustment in childhood and adolescence was measured using the Premorbid Social Adjustment Scale (PSAS) (Cannon et al., 1997), a parental report of five domains of child adjustment: sociability, peer relations, scholastic performance, adaptation to school and interests. The Role Functioning Scale (RFS) (Goodman et al., 1993) was used to measure current social functioning across four domains (working/education, self-care, immediate social network (i.e. friends and family) and extended social networks). Information collected from the clinical records of subjects included demographic details, developmental history and family psychiatric history (elicited by drawing a family genogram and then asking about psychiatric history for each first- and second-degree relative). A variable called ‘Ever developmentally normal’ was created including subjects with a history of normal milestones and intellectual functioning. Past history was obtained at interview from the SCID and by reviewing medical records.
Symptoms were compared across diagnostic groups by removing the IPT group and comparing the mood disorder with the combined schizophrenia spectrum and PD NOS group. These groups were combined because some authors have suggested that the PD NOS group in childhood is most closely related to schizophrenia because of the high level of cognitive and functional impairment (Kumra et al., 2000). Statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS), Version 20. As this was an exploratory study the level of significance was kept at p < 0.05.
Results
Description of the study subjects
The average age at interview was 13.2 years (SD = 2.3 years, range 7–17 years) and 49% were female (22/45). The diagnostic groups were 33% schizophrenia spectrum disorders (15/45), 40% affective disorder (18/45), 20% psychosis NOS (9/45) and 7% IPT (3/45). Other diagnoses made prior to the diagnosis of psychosis included developmental disability (pervasive developmental disorders 16% (7/45) and intellectual disability 9% (4/45)), major depression 40% (18/45), anxiety disorders (including generalized anxiety disorder, panic disorder and obsessive compulsive disorder) 47% (21/45), ADHD 13% (6/45), other behaviour disorders 13% (6/45) and PTSD 11% (5/45). Three subjects reported tic disorders, two an eating disorder and one a conversion disorder. Three subjects had no previous psychiatric history. The median number of previous diagnoses was 2 (SD = 1.1).
Three subjects had a history of problematic drug use and seven were smokers (history checked with family and by pre-admission urine screens). A history of deliberate self-harm was reported by 53% (24/45) and physical aggression by 62% (28/45).
Obstetric histories were abnormal in 47% (most commonly emergency caesarian sections and pre- or post-partum fetal distress), with normal deliveries in 36% and 11% unknown. There was a strong family history of psychiatric disorder in many subjects. Those with a reported history included 67% of mothers (4/45 schizophrenia, 3/45 bipolar disorder, 16/45 major depression, 4/45 anxiety disorder, 3/45 drug abuse), 47% of fathers (8/45 bipolar disorder, 8/45 major depression, 3/45 anxiety disorder, 2/45 alcoholism), 12 grandparents and nine other second-degree relatives with schizophrenia. This was despite several subjects being in alternate care without knowledge of family history, or living with parents who were unaware of the psychiatric history of the other parent.
The median dose of antipsychotic medication was 134.5 mg chlorpromazine equivalents (range 0–556 mg) at the time of interview. All but five subjects were admitted at some stage of their illness, with an average length of stay of 35 days (SD 37 days). At discharge from hospital, 84% returned home while 13% were transferred to another facility for ongoing care. Forty percent were discharged to mainstream school, 31% to special education services, and 16% did not return to any form of schooling at discharge (13% no data available).
Symptom clusters by diagnosis (schizophrenia spectrum and psychosis NOS compared with mood disorder)
Table 1 compares the history given by those with schizophrenia spectrum disorders combined with psychosis NOS (SSD) with those with mood disorders (MD). There was no significant difference in mean age at first onset of symptoms, or at testing. There were more males with SSD and fewer with MD, but this difference was not significant. The mood disorders group was more likely to have a past history of major depression (83% vs 54%, p = 0.05, χ = 3.9), a period of normal development prior to illness development (72% vs 21%, p = 0.001, χ2 = 11.1) and had a significantly higher prevalence of self-harm (72% vs 42%, p = 0.05, χ = 3.9). There was no difference in the history of physical violence.
History by diagnosis (Schizophrenia spectrum and Psychosis NOS compared to mood disorder).
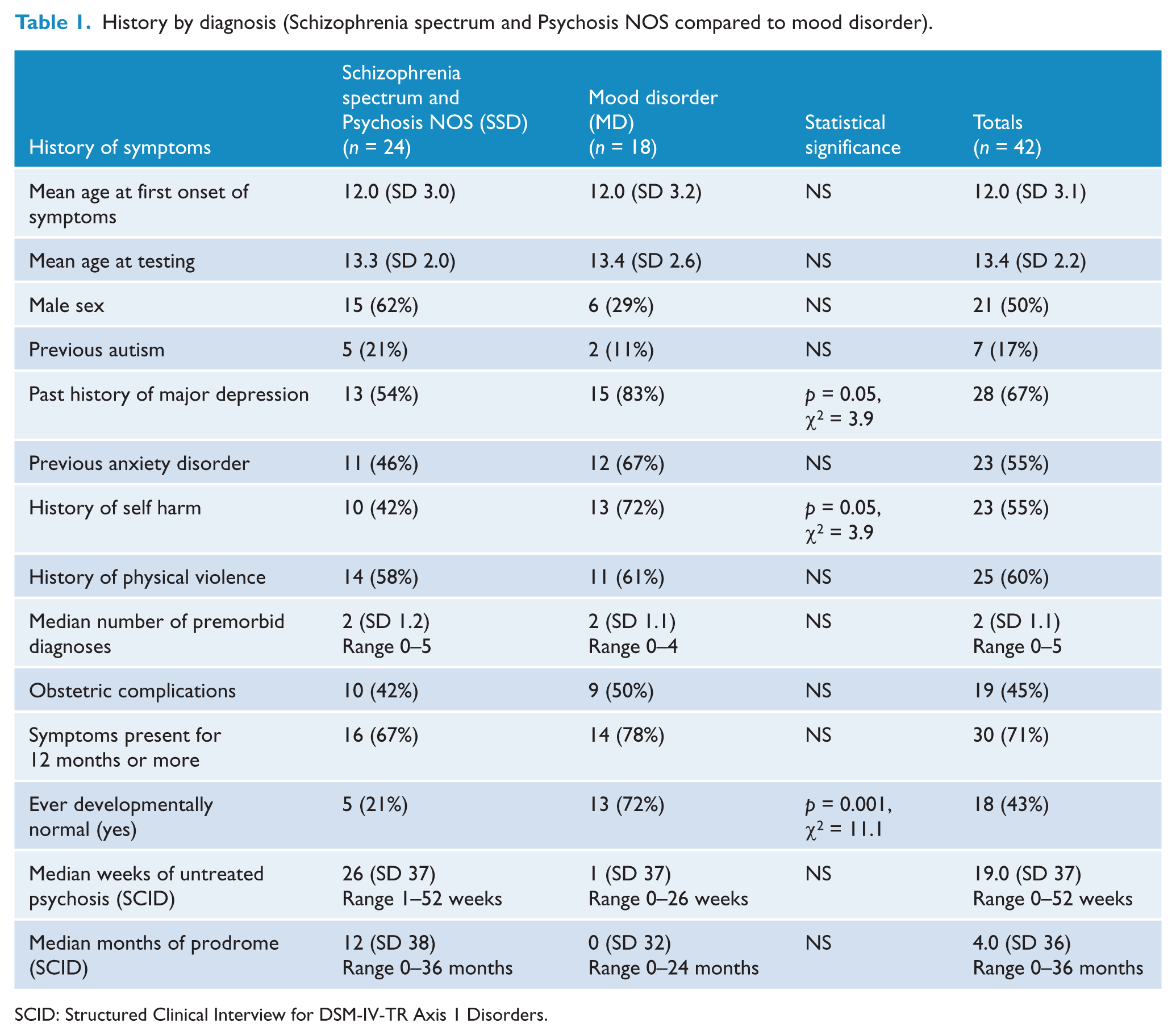
SCID: Structured Clinical Interview for DSM-IV-TR Axis 1 Disorders.
Table 2 compares symptom rating scales by diagnosis. While neither the MD nor the SSD groups had YMRS or CDI scores in the clinical range, they were highly symptomatic on the DASS, with total score and DASS depression in the moderate clinical range, anxiety in the severe range and stress in the mild range for SSD and moderate for MD. None of the DASS scores was significantly different by diagnostic group. The MD group had higher scores for adolescent social adjustment (p = 0.01, t = 2.6) and total role functioning (p = 0.01, t = −2.6), as well as higher scores on the immediate (p = 0.01, t = −2.6) and extended social network (p = 0.02,t = −2.5) subscales of the RFS. Subjects in the SSD group had higher scores on the PANSS negative (p = 0.01, t = 2.6) and PANSS general score (p = 0.007, t = 2.9) but there were no significant differences in the PANSS positive score.
Symptom rating scales by diagnosis (Schizophrenia spectrum and Psychosis NOS compared to mood disorder).
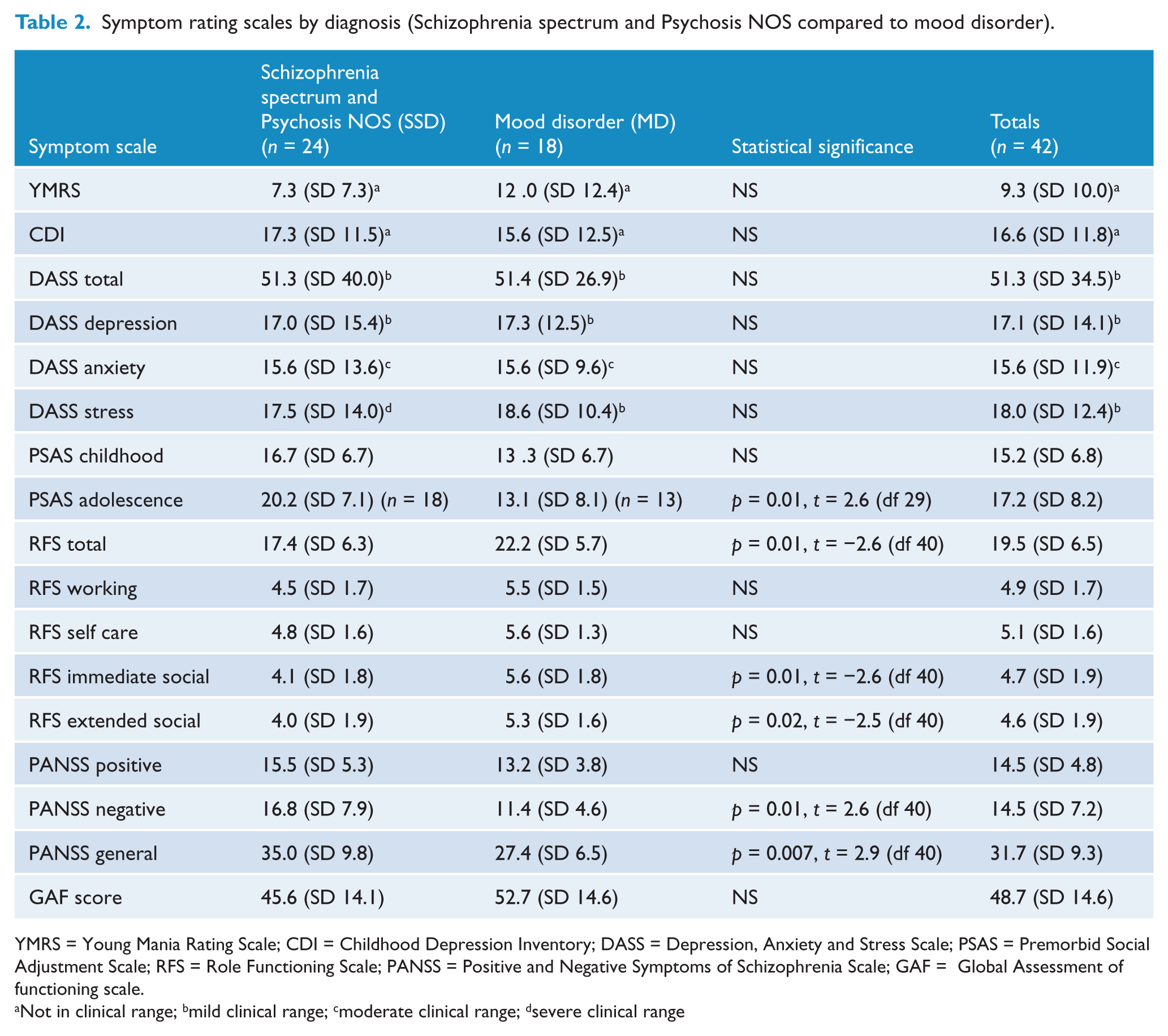
YMRS = Young Mania Rating Scale; CDI = Childhood Depression Inventory; DASS = Depression, Anxiety and Stress Scale; PSAS = Premorbid Social Adjustment Scale; RFS = Role Functioning Scale; PANSS = Positive and Negative Symptoms of Schizophrenia Scale; GAF = Global Assessment of functioning scale.
Not in clinical range; bmild clinical range; cmoderate clinical range; dsevere clinical range
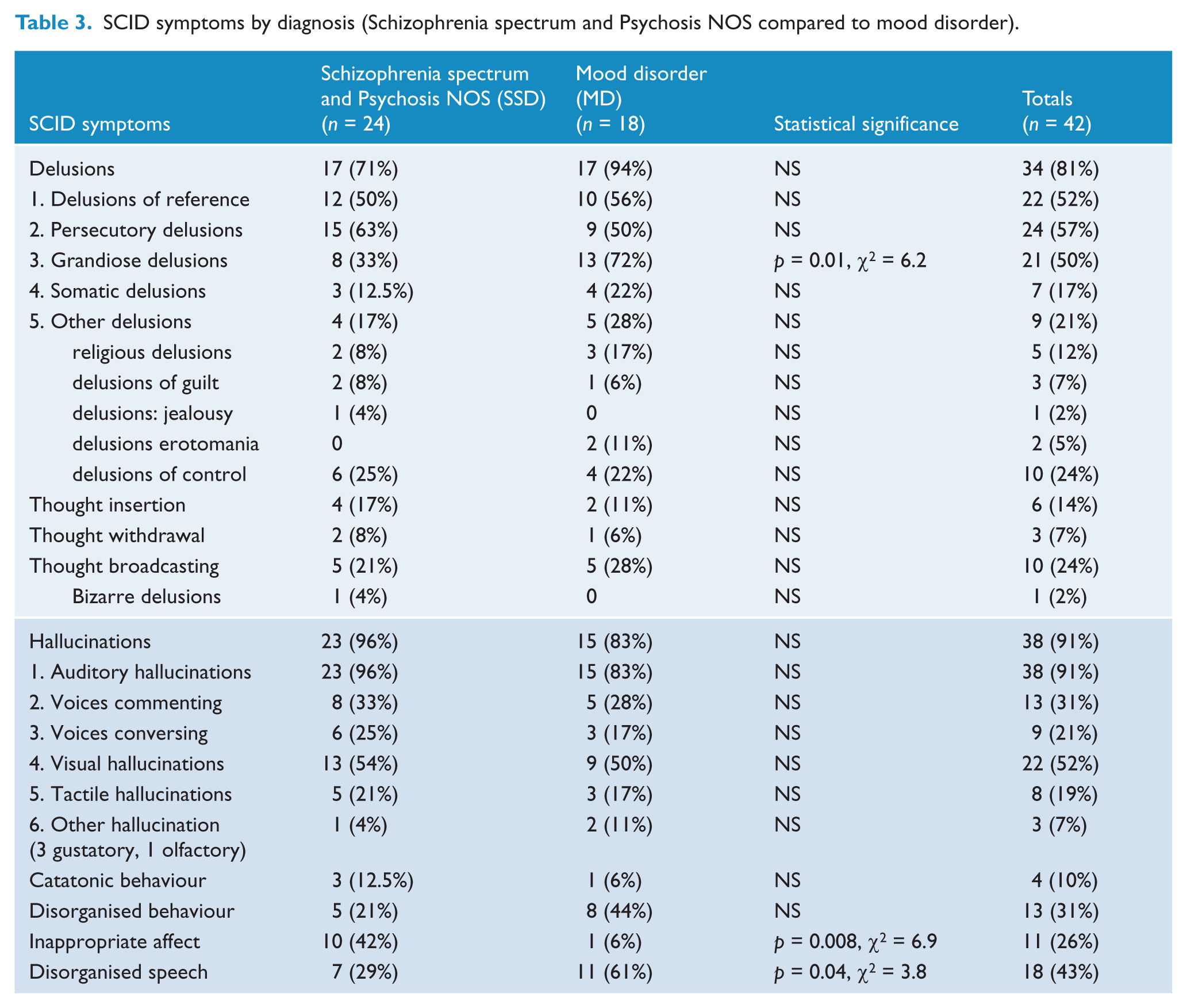
Table 3 compares symptoms from the SSD and MD groups obtained at SCID interview. The only statistically significant differences were that grandiose delusions (p = 0.01, χ2 = 6.2) and disorganized speech (p = 0.04, χ2 = 3.8) were more common in mood disorder and inappropriate affect in SSD (p = 0.008, χ2 = 6.9).
SCID symptoms by diagnosis (Schizophrenia spectrum and Psychosis NOS compared to mood disorder).
Discussion
This study describes a group of children and adolescents with psychotic disorders who presented to paediatric mental health services, and were interviewed at an average age of 13 years. The most notable clinical feature of this group was the high levels of distress at the time of presentation, with scores in the high clinical range for anxiety and stress, and in the clinical range for depression. There was also a high level of disturbed behaviour with more than half reporting a history of self-harm and aggression to others. Most young people had previous treatment for other psychiatric disorders (median = 2) prior to their presentation with a psychotic illness, with anxiety and depression the most common but pervasive developmental and behavioural disorders also seen. There was also a high level of social and functional impairment, which was significantly worse in the non-mood disorder group, who also had more negative symptoms and was less likely to have ever been developmentally normal. These findings fit with previous research, in particular the high level of impairment seen in COS (Hollis, 2000), although only one of our subjects met criteria for COS as the others either had a later age of onset of schizophrenia or another psychotic disorder. The results are also consistent with other studies, suggesting that those with an onset of psychosis prior to the age of 18 years are likely to be more impaired than those with adult-onset (Schimmelmann et al., 2007).
There were fewer differences than expected between the subgroup with bipolar affective disorder and the other psychotic disorders, emphasising the high level of disability that bipolar disorder can cause. It is possible that either the small sample size or a bias in subject recruitment may be the explanation for this finding. The psychosis NOS group, while small, was almost entirely male with high levels of pre-existing intellectual disturbance and obstetric complications, strongly suggestive of premorbid neurodevelopmental impairment and consistent with an evolving schizophrenia. This group had many of the characteristics of the ultra-high-risk group of subjects (Yung et al., 2008).
In early psychosis research, the duration of prodrome (DP) and duration of untreated psychosis (DUP) are crucial variables, particularly in outcome research (Harrigan et al., 2003), with the goal of early intervention to minimise the length of time with untreated symptoms. In this study, the interviewers were unable to determine the DP or DUP in many subjects, for several reasons. Many of the subjects had lifelong developmental difficulties, so there was no clear history of a period of normality with later functional decline. Most also had a substantial period of treatment for other disorders such as depression or anxiety before the appearance of psychotic symptoms. Others were unable to clearly remember the time the first positive psychotic symptom, such as auditory hallucinations, first appeared. This also undermines the concept of premorbid functioning when it is difficult to establish if a child was ever in the normal range of educational or social achievement.
Despite being a small sample, does this study have any implications for services for the very early-onset psychosis population? Currently, Child and Family Community teams (CAFT) in Australia treat the younger age group, and Early Intervention in Psychosis teams (EIP) the older adolescents. Because of the rarity of the diagnosis, clinicians in CAFT may lack knowledge about the trajectory of psychotic symptoms such as hallucinations in this population and may even erroneously believe that such symptoms are universally benign. However, they have the skills to manage the high level of comorbid conditions, including anxiety disorder, depression and developmental disability. Working with families and liaising with schools are also core skills. In contrast, EIP teams are experts in the identification and treatment of the early presentations of psychosis, but work in a setting appropriate for older adolescents and young adults. The skill sets of both EIP and CAFT services are needed for the optimum treatment of these rare, but serious disorders.
Limitations of this study
While the authors attempted to recruit from community mental health services, most subjects were recruited from acute and tertiary services, so may be more impaired or unrepresentative of the wider population with very early-onset psychosis in other ways. Longitudinal studies would be necessary to confirm the accuracy of diagnosis and differences between diagnostic groups. Our study did not include questionnaires on family functioning or trauma. Finally, despite information from the medical file and family interviews, as well as the interview measures, we would expect that there were still many gaps in information, particularly in under-reporting information that may be considered shameful, such as a family history of mental illness. Nonetheless, this study presents a symptomatic profile of this under-reported group of patients and as such is useful to the psychiatric community.
Footnotes
Acknowledgements
With thanks to Associate Professor Jenny Peat for advice on statistical methods and analysis, and Dr Stephen Koder and Dr Catherine Wiltshire for assistance with confirmation of diagnosis.
This work was carried out at the Department of Psychological Medicine, Children’s Hospital at Westmead, Sydney, NSW, Australia, the Western Sydney Area Health Service, NSW, Australia and the Brain Dynamics Unit, Westmead Hospital, Westmead, NSW, Australia
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.