
Abstract
Objective:
The aims of this study were to (a) describe patterns of tobacco smoking among Australians living with a psychotic illness and (b) explore the association between smoking and measures of psychopathology, psychiatric history, psychosocial functioning, physical health, substance use and demographic characteristics.
Methods:
Data were from 1812 participants in the 2010 Australian Survey of High Impact Psychosis. Participants were aged 18–64 years and resided in seven mental health catchment sites across five states of Australia. Bivariate statistics were used to compare smokers with non-smokers on the measures of interest, and to compare ICD-10 diagnostic categories on measures of smoking prevalence, nicotine addiction and quitting history. Multivariate logistic regression was used to test whether (a) demographics and psychiatric history were associated with having ever smoked and (b) whether symptoms and psychosocial functioning were independently associated with current smoking, after controlling for demographics, psychiatric history and substance use.
Results:
The prevalence of current tobacco smoking was 66.6% (72% of men and 59% of women); lifetime prevalence was 81%. In univariate analyses, individuals with a diagnosis of schizophrenia or schizoaffective disorder were most likely to be smoking tobacco (70%) and were more nicotine dependent. Smokers reported worse perceived physical health, lower body mass index and waist circumference, and more lifetime medical conditions. A younger age of illness onset, male gender and low education were associated with having ever smoked. Associations with current smoking included low education, male gender, no formal employment, worse negative symptoms, higher daily caffeine consumption, and alcohol dependence and substance abuse/dependence.
Conclusions:
The prevalence of tobacco smoking is high amongst people with a psychotic disorder, and is associated with adverse mental health symptoms as well as high rates of other substance use, poorer subjective physical health, and a higher risk of the many known health consequences of smoking.
Introduction
Tobacco smoking is one of the leading preventable causes of death and disability in Australia (Collins and Lapsley, 2008). A widely cited international meta-analysis found that 62% of people living with schizophrenia smoke (de Leon and Diaz, 2005). The smoking prevalence among people with bipolar disorder has been reported as 58% in Australia (Lawrence et al., 2009), similar to 61% reported in the US (Lasser et al., 2000). During 1997–1998, a nationally representative Australian study of people with a psychotic illness found that the prevalence of smoking was 73% for men and 56% for women (Jablensky et al., 2000), far in excess of the prevalence of smoking in the Australian general population – which was around 26% at that time (Scollo and Winstanley, 2008). In the presence of public anti-smoking campaigns and increased uptake of support services for quitting smoking, the proportion of the Australian general population who smoke had declined to 19% in 2007 (Scollo and Winstanley, 2008).
Physical health problems, particularly heart disease, are a significant contributor to premature death among people with a psychiatric disorder (Lawrence et al., 2000). People with schizophrenia are at an increased risk of dying from all causes of mortality (Saha et al., 2007). It has been estimated that, compared to the general population, average life expectancy for people with schizophrenia is reduced by 19 years for men and 16 years for women, and by 14 years for men and 12 years for women for people with bipolar disorder (Laursen, 2011). Although smoking is just one risk factor for premature death and excess disability in people with a severe mental illness, a cohort study of 370 people with schizophrenia concluded that most of the excess natural mortality is due to cigarette smoking (Brown et al., 2000). Thus, there is a need to examine the physical health correlates of smoking in people with psychosis.
A number of explanations have been put forward to account for the association between smoking and psychosis. Some researchers contend that smoking and psychotic illnesses share common aetiological factors (de Leon et al., 2007). Social factors thought to influence smoking rates among people with a severe mental illness include systemic barriers to quitting within the mental health system (Lawn, 2004), boredom (Mann-Wrobel et al., 2011), low socioeconomic status (McCloughen, 2003) and a lack of targeted smoking cessation interventions (Lawrence et al., 2009). Nicotine’s role as a dopamine agonist has led to the hypothesis that smoking may decrease the severity of the symptoms and cognitive deficits of schizophrenia and/or side effects of antipsychotic medication, thus increasing the reward value of smoking (Dalack et al., 1998; Kumari and Postma, 2005). Empirical evidence has been inconsistent with this hypothesis. Smoking has been linked to improved cognitive outcomes (Kumari and Postma, 2005). However, studies among people with schizophrenia or schizoaffective disorder have found an association between smoking and more severe psychotic symptomatology, including worse negative symptoms (Hall et al., 1995; Patkar et al., 2002), worse positive and disorganized symptoms (Aguilar et al., 2005; Ucok et al., 2004), poorer psychosocial functioning (Kotov et al., 2010; Vanable et al., 2003) and more frequent hospitalisations (Aguilar et al., 2005; Kobayashi et al., 2010). Smoking is also associated with more severe psychopathology among people with bipolar disorder (Berk et al., 2008; Corvin et al., 2001; Waxmonsky et al., 2005). Others have found decreased negative symptoms among smokers (Ziedonis et al., 1994) or no association between smoking and psychotic symptomatology (Barnes et al., 2006; Herran et al., 2000; Kotov et al., 2010).
Previous research on the association between smoking, psychopathology and psychosocial functioning has been limited by small or non-representative samples and limited evaluation of potential confounding variables. For example, an early age of illness onset is associated with both the uptake of smoking (Kelly and McCreadie, 1999) and illness severity (Harrison et al., 2001), whilst alcohol and illicit substance use are highly prevalent amongst people with psychosis and are associated with tobacco smoking and poorer illness trajectories (Degenhardt and Hall, 2001a, 2001b). Yet few studies have examined the association between smoking, psychopathology and illness severity, controlling for both psychiatric history and substance use.
The current study
This study investigated the characteristics of smokers with a psychotic illness in a large representative Australian sample. Using the estimate of smoking prevalence from the 1997–1998 Australian National Low Prevalence (Psychotic) Disorders Study (Jablensky et al., 2000), we investigated whether the smoking rate in this population has declined as it has in the general population. We then focused on tobacco smoking and compared smokers and non-smokers on measures of demographics, physical health, psychiatric history, psychopathology, psychosocial functioning, and substance use. As we had a large sample (n = 1812), we were able to examine the association between smoking, psychopathology and psychosocial functioning whilst controlling for possible confounds. This study also allowed an exploration of the smoking characteristics, including quitting history and smoking behaviour, across diagnostic categories.
Materials and methods
Participants and procedure
Data are from 1812 participants of the 2010 Australian Survey of High Impact Psychosis (SHIP). The SHIP survey was developed as a two-phased sampling design. In phase 1, potential participants were screened for psychosis during March 2010. In phase 2, 2000 individuals aged 18–64 were randomly selected for interview from those who screened positive for psychosis. Participants resided in seven mental health catchment sites across five states of Australia (New South Wales, Queensland, South Australia, Victoria and Western Australia). The study was approved by institutional human research ethics committees at each of the seven study sites and all participants provided written, informed consent. A detailed description of the sample, methods and aims of the SHIP survey can be found elsewhere (Morgan et al., 2012).
Measures
Demographic information
Data were collected on each participant’s age at the time of interview, gender, highest level of education level (did not complete high school, completed high school, vocational qualification, or university) and employment in the previous 12 months. Employment was defined as: (1) paid employment; (2) unpaid activity (studying, home duties, caring for relatives, volunteering/unpaid work, or retired); and (3) no formal vocational activity.
Smoking variables
Participants were asked whether they had ever regularly smoked cigarettes, tobacco, cigars or a pipe and, if they had, whether they had smoked in the previous 4 weeks. Participants were categorized as having never been a regular smoker, being an ex-smoker (not smoked in the previous 4 weeks) or a current smoker (smoked in previous 4 weeks). Those who reported ever regularly smoking were asked the age they started smoking regularly, the heaviest ever daily cigarette use, and whether they had tried to stop smoking for at least 24 hours. Those who had tried to quit were asked how many times they had tried to quit, time since last quit attempt, longest time ever that they did not smoke (in weeks) and whether they had ever sought help to quit smoking. They were also asked about the main reason they started smoking again: (1) I felt too stressed; (2) people around me smoked (including ‘my partner/people I live with smoke’ and ‘a lot of my friends smoked’); (3) craving or unpleasant withdrawal symptoms (including ‘I couldn’t resist the craving for a cigarette’ and ‘withdrawal symptoms were too unpleasant’); and (4) other (including ‘enjoy smoking too much/didn’t want to quit’, ‘I put on weight’, and ‘other’). Nicotine dependence was measured using the Fagerstrom Test for Nicotine Dependence (FTND) (Heatherton et al., 1991), a six-item questionnaire (scoring between 0 and 10) that is a reliable and valid measure widely used in smoking research. Participants who had not smoked in the previous 4 weeks were not administered the FTND.
Physical health
Participants underwent a physical examination in which blood pressure, height, weight and waist circumference were measured. They were considered in the ‘at risk’ range for blood pressure if they had a systolic blood pressure greater than 130 mmHg and/or a diastolic pressure greater than 85 mmHg (International Diabetes Federation, 2006). Body mass index (BMI) was calculated as weight (kg) divided by height (m2). Participants were also asked whether they had a history of high cholesterol, and whether they had diabetes or had been told that their blood sugars were high. Physical activity during the previous 7 days was assessed using the short format of the International Physical Activity Questionnaire (IPAQ) (Craig et al., 2003), which rates activity levels as low, moderate or high. Perceived physical health was measured on a five-point scale (1 = ‘excellent’ to 5 = ‘poor’). To assess the number of lifetime chronic illnesses, participants were read a list of medical conditions and asked to indicate which ones a doctor had diagnosed. Diagnosed cardiovascular disease was ascertained by asking participants whether they had ever been told by a doctor that they had any of the following: heart attack, angina, stroke/transient ischaemic attack (TIA), or other heart disease (e.g. arrhythmias).
Psychopathology and psychiatric history
Measures of psychopathology and psychiatric history were determined using the Diagnostic Interview for Psychosis (DIP) (Castle et al., 2006). A detailed description of the DIP can be found elsewhere (Castle et al., 2006). Measures of psychopathology from the DIP included in the current study were the presence in the previous month of hallucinations, subjective thought disorder (thought insertion, broadcasting, withdrawal and echo), delusions, manic symptoms, depressive symptoms (either depressed mood or loss of pleasure); and the severity of negative symptoms in the previous year (score 1–18). Participants were asked whether they been hospitalized for their mental health in the previous 12 months. The Personal and Social Performance scale (PSP) (Morosini et al., 2000) was used to measure psychosocial functioning. The PSP scale refers to the previous 12 months and considers the level of functioning in social activities including work and study, relationships, self-care and disturbing and aggressive behaviours. Three levels were computed: (1) absence of disability or mild difficulties (scores between 71 and 100); (2) moderate to severe degree of disability (scores between 31 and 70); and (3) extremely severe disability, requires intensive support (scores between 1 and 30). Psychiatric history variables included were age of illness onset, mode of onset (abrupt/acute/moderately acute versus gradual/insidious), course of illness (single episode/partial recovery versus chronic) and International Classification of Diseases-10 (ICD-10) diagnoses of schizophrenia/schizoaffective disorder, bipolar (mania) disorder, depression with psychotic features, and other disorders. The ‘other’ category included depression without psychosis and those who screened positive for psychosis but did not meet the criteria for a diagnosis.
Substance use
Alcohol dependence in the previous 12 months was assessed using the Alcohol Use Disorders Identification Test (AUDIT) (Babor et al., 2001). Probable alcohol dependence was identified as having an AUDIT score of 20 or above. Abuse of or dependence on cannabis and other drugs in the previous 12 months was assessed using the 10-item Drug Abuse Screening Test (DAST-10) (Skinner et al., 1982). Participants who were likely to meet the criteria for a DSM-IV diagnosis of substance abuse or dependence were identified using a DAST-10 score of 3 or above. These data are reported in full elsewhere (Moore et al., 2012). Caffeine use was assessed by asking about the type and quantity of caffeinated drinks consumed per day on average during the previous 4 weeks, from which we calculated how many milligrams of caffeine were consumed on an average day.
Statistical analyses
Analyses were conducted using Stata version 11.2. For all analyses, a value of p < 0.05 was considered significant. Means and standard deviations were calculated for continuous variables, and frequencies were measured for categorical variables. For categorical variables, differences between groups were analysed by chi-square or Fisher’s exact test as appropriate. The Fisher’s exact tests were applied in case of an expected frequency of less than 5. For continuous variables, group differences were examined using t-tests and one-way analyses of variance (ANOVA). For ANOVAs with a significant effect of diagnostic group, planned contrasts with Bonferroni correction (p < 0.016) were applied to the comparisons of the schizophrenia/schizoaffective disorder group to the three other diagnostic groups, respectively. When the homogeneity of variance assumption was violated, t-tests with Welch’s approximation and Welch’s ANOVA were used.
Two stepwise multivariate logistic regressions were performed. The dependent variable in the first regression was having ever smoked (i.e. former/current smokers versus those who had never smoked). Variables were entered in two steps: step 1 demographic variables: age at interview, gender and highest level of education; and step 2 psychiatric history variables: ICD-10 diagnostic category (schizophrenia/schizoaffective versus all other), age of illness onset, course of illness, and mode of illness onset. In the second logistic regression, the dependent variable was current smoking (versus non-smoking). The first two steps were identical to above. In a third step, variables were entered to examine the association between current smoking, symptoms and functioning, whilst controlling for demographics and psychiatric history. Variables in this step included hallucinations, delusions, subjective thought disorder, negative symptoms, PSP categories, employment in the previous 12 months, and whether participants had been hospitalized for mental health in the previous 12 months. Variables entered in a fourth step included daily caffeine use and alcohol dependence and substance abuse/dependence in the previous 12 months. Each model met the Stata convergence criterion and satisfied the Wald test for rejection of the global null hypothesis (p < 0.001). For each model, independent variables were systematically evaluated for second-order interactions and the degree of association among correlates.
Results
Sample characteristics
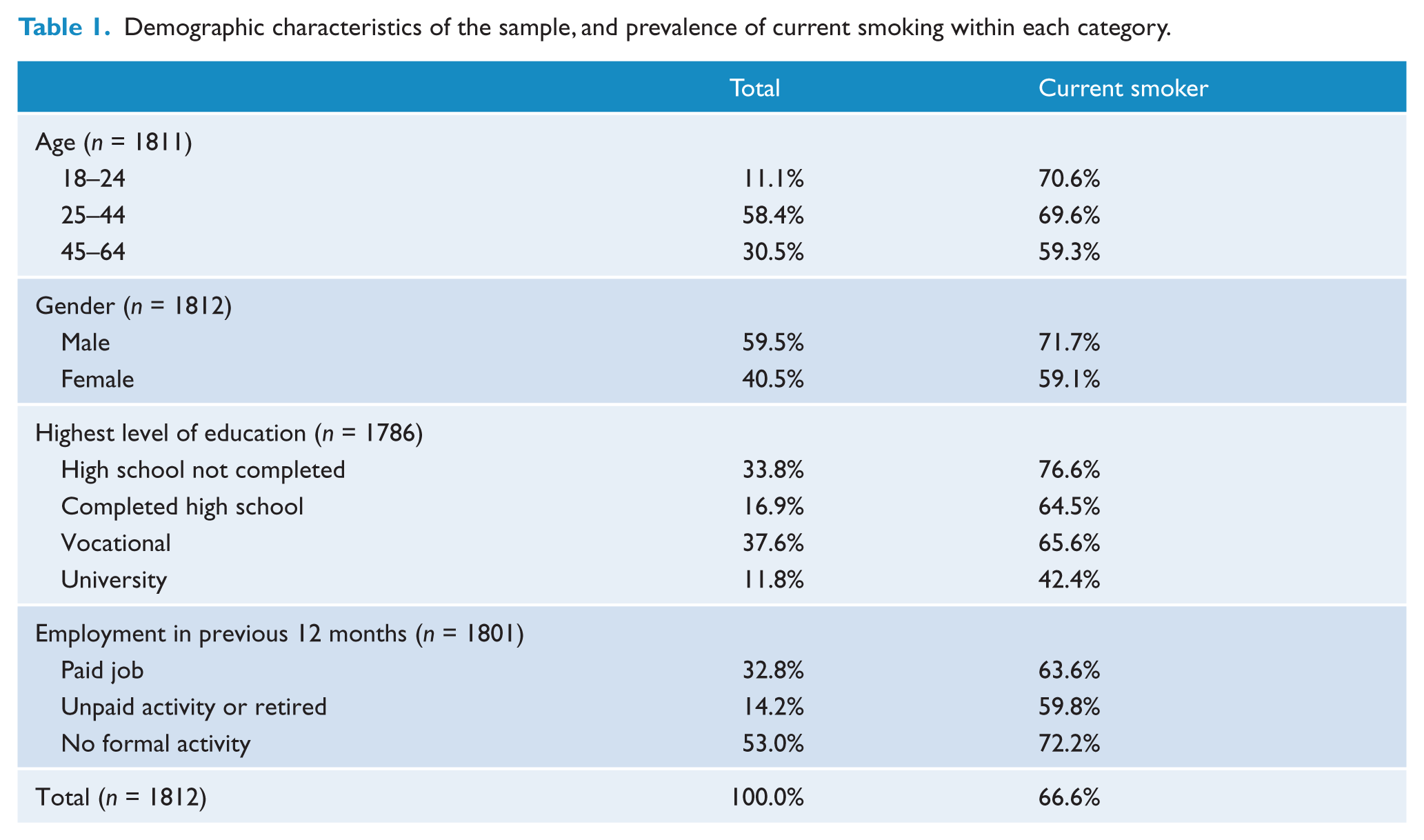
Table 1 shows the demographic characteristics of the sample and the proportion of current smokers in each category. The average age of the sample was 38.4 years (standard deviation = 11.2). The smoking prevalence was 66.6% for the whole sample, and was significantly (p < 0.001) higher for men (71.7%) than women (59.1%). The prevalence of smoking was also significantly lower among older participants (p < 0.001) and significantly higher among those who did not complete high school (p < 0.001) and those who had not engaged in any formal vocational activity in the previous 12 months (p < 0.001).
Demographic characteristics of the sample, and prevalence of current smoking within each category.
Smoking characteristics
Table 2 shows the smoking status and the smoking characteristics for the sample as a whole and for each diagnostic group. In addition to the two-thirds who were current smokers, 14% smoked previously but not in the 4 weeks prior to the interview, and 19% reported that they had never regularly smoked tobacco. People with a diagnosis of schizophrenia/schizoaffective disorder had a significantly higher prevalence of current smoking (70%) and were less likely to have never been regular smokers (17%). They were also significantly younger (16.2 years) when they started regular smoking compared to individuals with bipolar disorder (17.2 years) (F[1,1462] = 7.5, p < 0.01). No other significant between-group differences were found for the age at which participants began regularly smoking.
Smoking characteristics of the sample, and within each ICD-10 diagnostic category.
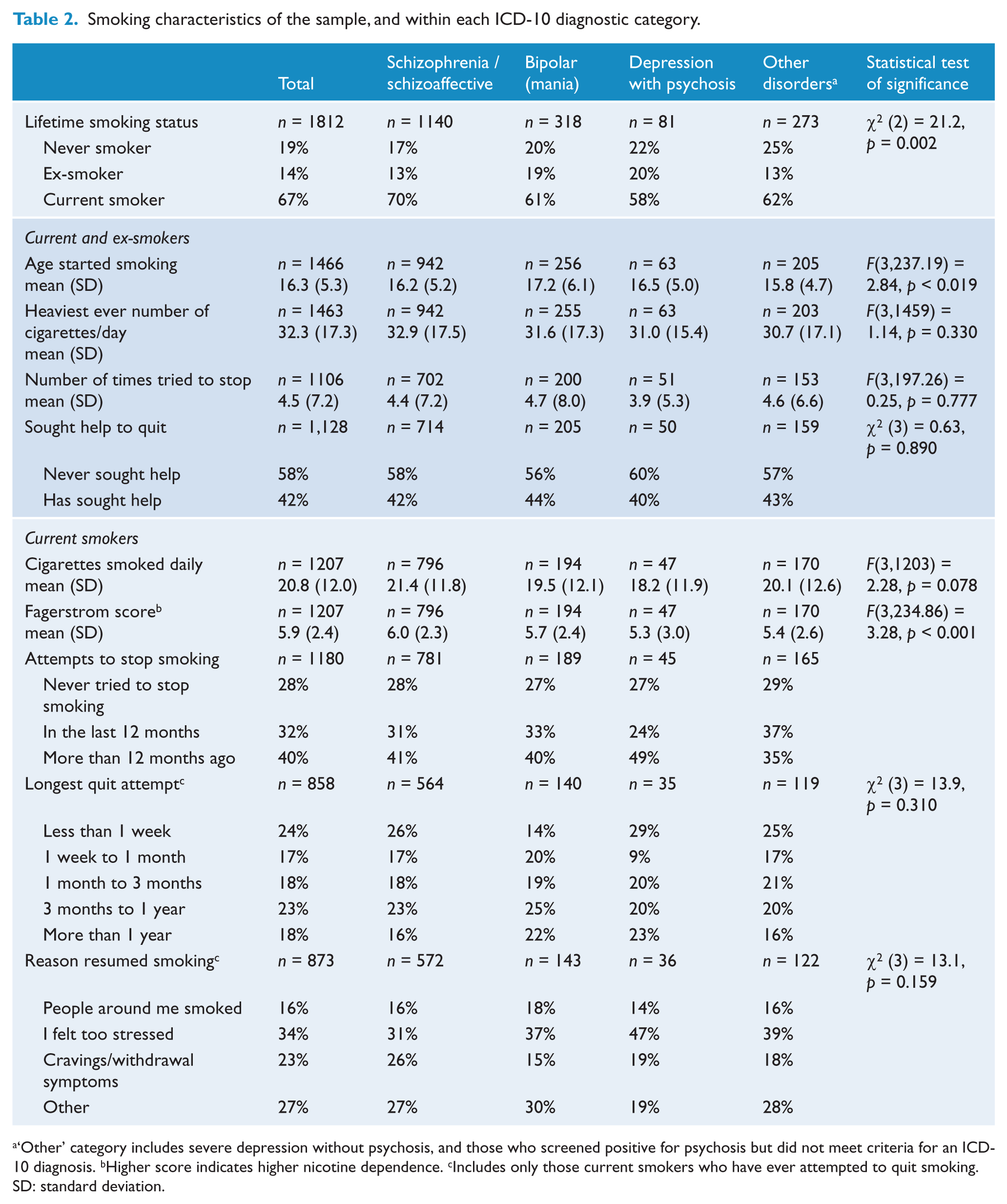
‘Other’ category includes severe depression without psychosis, and those who screened positive for psychosis but did not meet criteria for an ICD-10 diagnosis. bHigher score indicates higher nicotine dependence. cIncludes only those current smokers who have ever attempted to quit smoking.
SD: standard deviation.
The majority of current smokers (72%) reported that they had attempted to quit smoking. Of those who had tried to quit smoking, the average number of attempts was 4.5. There was no significant difference in the average number of quit attempts between ex-smokers (4.07) and current smokers (4.60). Of the ex-smokers, 71% reported they had quit smoking more than 12 months previously. Table 2 shows the distribution of the longest quit attempt for current smokers. The most common primary reason for resuming smoking was stress (34%). Other reasons for resuming smoking included: put on weight (1%); enjoyed smoking too much/did not really want to quit (15%); lived with a partner or people who smoked (5%); a lot of friends smoked (11%); and cravings or unpleasant withdrawal symptoms (20% and 3%, respectively). Almost half (42%) reported seeking help to quit; a further 10% had not sought help but would have liked it.
Current smokers smoked on average 20.8 cigarettes per day. Individuals with schizophrenia/schizoaffective disorder smoked significantly more cigarettes per day (21.4) than those with bipolar disorder (19.5) (F[1,1461] = 11.47, p < 0.001) and psychotic depression (18.2) (F[1,1461] = 6.65, p < 0.016). They were also significantly (χ2 (9) = 30.05, p < 0.001) more likely to report smoking the first cigarette within 5 minutes of waking (66%) compared to people with bipolar disorder (60%), psychotic depression (55%) and other disorders (59%). More people with schizophrenia/schizoaffective disorder (44%) reported difficulty not smoking in forbidden places compared to 34% of people with bipolar disorder, 38% of people with depression with psychotic features and 36% of people with other disorders (χ2 (3) = 9.11, p < 0.05).
Most of the sample reported they would most hate to give up the first cigarette of the morning (68%); smoked more frequently in the morning (53%); and smoked even when they were sick (55%). There were no significant differences between diagnostic groups for these variables. The mean FTND score among current smokers was 5.9, indicating high nicotine dependence. Current smokers with schizophrenia/schizoaffective disorder had a significantly higher FTND score (6.0) than those with bipolar disorder (5.7) (F[1,1821] = 11.98, p < 0.001), psychotic depression (5.3) (F[1,1821] = 6.52, p < 0.016) and other disorders (5.4) (F[1,1821] = 13.39, p < 0.001).
Physical health
Table 3 shows the difference between smokers and non-smokers on measures of physical health. On average, smokers had a significantly lower BMI and a significantly smaller waist circumference. Smokers reported significantly worse perceived physical health than non-smokers. There was no significant difference in reported lifetime cardiovascular disease/stroke, history of high cholesterol, diabetes/high blood sugar, or ‘at-risk’ blood pressure. Smokers reported significantly more lifetime medical conditions overall.
Physical health characteristics of smokers and non-smokers.
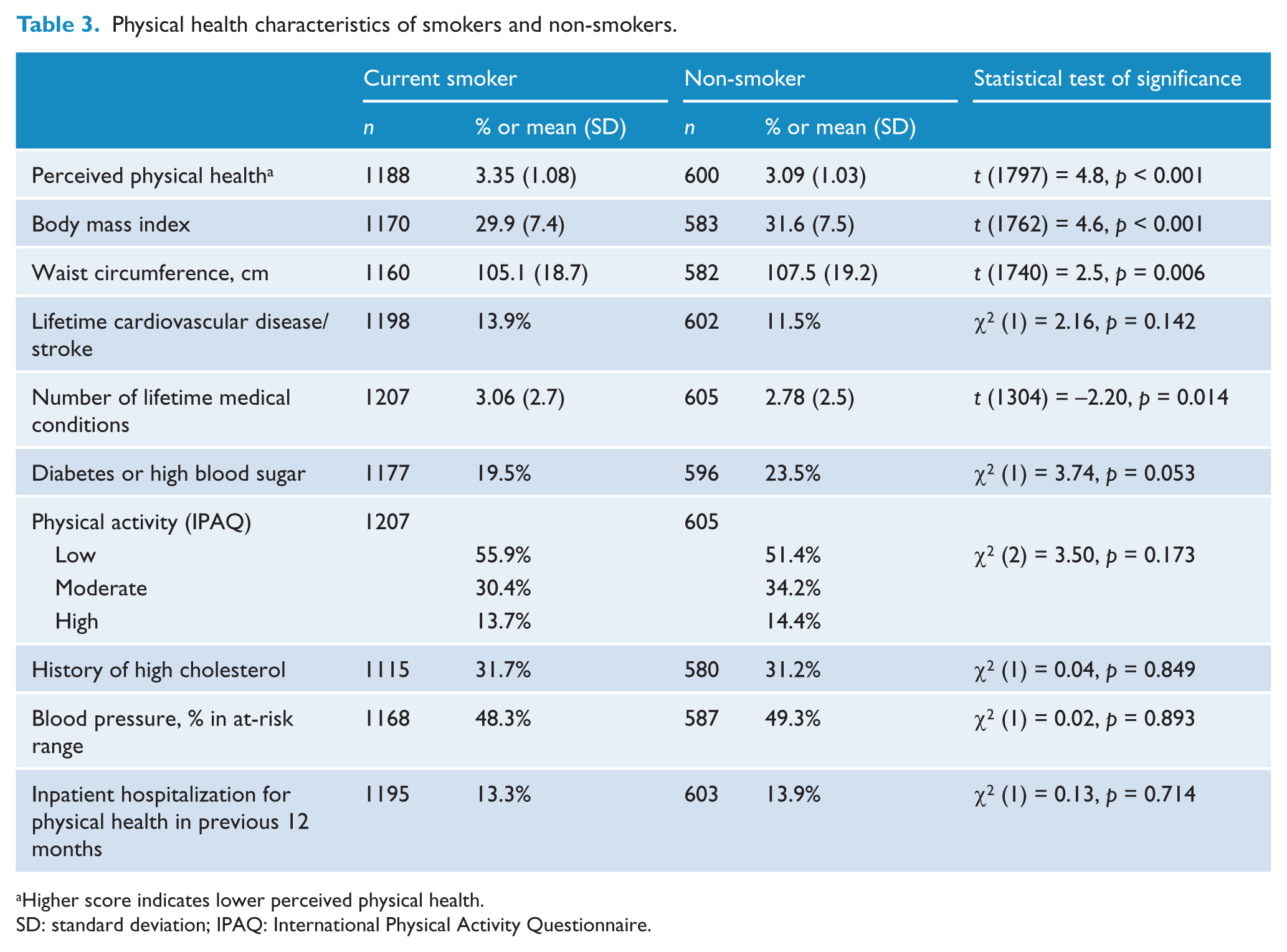
Higher score indicates lower perceived physical health.
SD: standard deviation; IPAQ: International Physical Activity Questionnaire.
Associations between smoking status, psychiatric history, psychopathology and substance use
Table 4 shows the univariate comparisons between current smoking and demographics, psychiatric history, positive psychotic symptoms, depressed mood/loss of pleasure and manic symptoms in the previous month; negative symptoms in the previous year; and psychosocial functioning and substance use. Current smokers had an average age of illness onset at 1.8 years earlier than non-smokers. They were significantly more likely than non-smokers to report experiencing hallucinations, delusions and subjective thought disorder in the previous month and had significantly higher scores on the negative syndrome scale (indicating worse negative symptoms over the previous year). They were also significantly more likely to have experienced moderate psychosocial disability in the previous year as measured using the PSP scale; were significantly more likely to report a chronic course of illness; and (though not statistically significant) more likely to have been hospitalized for their mental health in the previous 12 months. Current smokers consumed an average of 178 more milligrams of caffeine per day than non-smokers; were more than twice as likely to report alcohol dependence in the previous 12 months; and were four times more likely to report abuse of/dependence on either cannabis or other drugs in the previous 12 months.
Psychopathology and substance use among smokers and non-smokers.
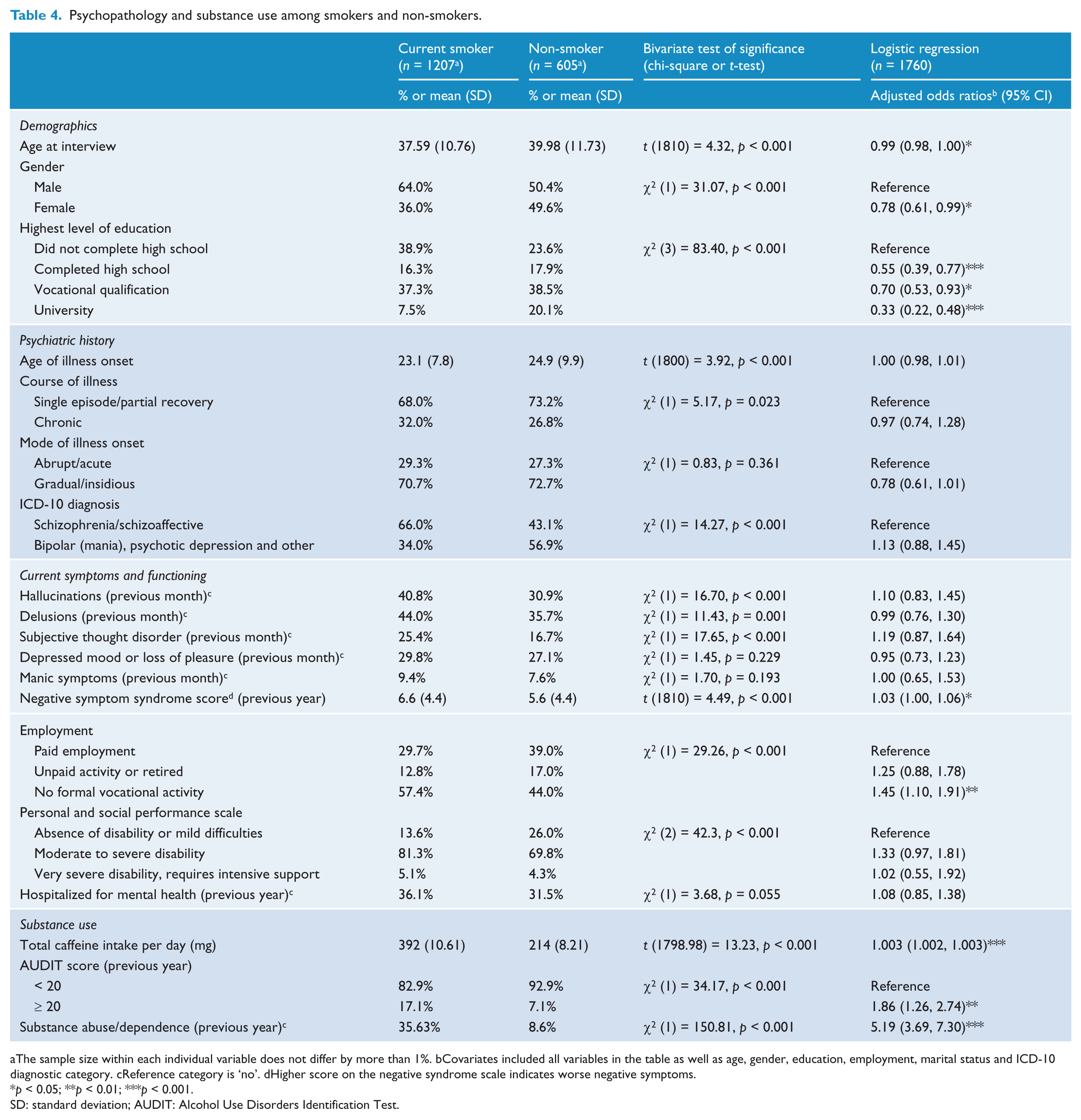
The sample size within each individual variable does not differ by more than 1%. bCovariates included all variables in the table as well as age, gender, education, employment, marital status and ICD-10 diagnostic category. cReference category is ‘no’. dHigher score on the negative syndrome scale indicates worse negative symptoms.
p < 0.05; **p < 0.01; ***p < 0.001.
SD: standard deviation; AUDIT: Alcohol Use Disorders Identification Test.
In the first multivariate logistic regression, we looked at the association between demographic variables and psychiatric history amongst ever smokers compared to never smokers. At steps 1 and 2, gender and the highest level of education were significantly associated with ever smoking. Females were less likely to have ever smoked (odds ratio (OR) = 0.50, 95% confidence interval (CI) = 0.39, 0.64). Compared to those who had not completed high school, those who had completed high school (OR = 0.50, 95% CI = 0.35, 0.74), had a vocational qualification (OR = 0.55, 95% CI = 0.40, 0.76), or had a university qualification (OR = 0.30, 95% CI = 0.20, 0.44) were less likely to have ever smoked. At step 2, a younger age of illness onset (OR = 0.97, 95% CI = 0.96, 0.99) was significant. We further explored the significant main effect of age of illness onset on smoking status with an ANOVA comparing never smokers, former smokers and current smokers (F[2,1799] = 12.10, p < 0.001). Post hoc Tukey HSD pairwise comparisons with Bonferroni correction (p < 0.025) indicated that patients who never smoked (mean = 25.67, SD = 10.64) had a significantly later age of illness onset compared to current smokers (mean = 23.11, SD = 7.82) and former smokers (mean = 23.92, SD = 8.82).
In the second multivariate logistic regression, we looked at variables associated with being a current smoker (versus not smoking in the previous 4 weeks). Younger age at interview, male gender and lower education level were significant at all four steps. None of the psychiatric history variables were significant on step 2. On the third step, having no formal vocation in the previous 12 months (OR = 1.33, 95% CI = 1.03, 1.71) and reporting symptoms of subjective thought disorder (OR = 1.38, 95% CI = 1.03, 1.85) were significant. Compared to those with an absence of disability or mild impairment, those with moderate to severe degrees of disability were more likely to be current smokers (OR = 1.45, 95% CI = 1.09, 1.94). At the fourth step, higher daily caffeine use and a 12-month history of alcohol dependence and other substance abuse/dependence were all independently associated with current smoking (see Table 4). For every 100 mg of caffeine consumed, the odds of being a smoker increased by 32%. With the addition of the substance use variables on the fourth step, subjective thought disorder and the PSP scale were no longer significant and higher scores on the negative syndrome scale became marginally significant (see Table 4). For every increase of one point on the negative syndrome scale, the odds of smoking were increased by 3%. We also repeated the model (not shown) with the schizophrenia/schizoaffective disorder group only. The only notable difference was that the PSP scale remained significant after controlling for substance use such that those with moderate to severe degrees of disability were more likely to smoke (OR = 1.61, 95% CI = 1.06, 2.44) than those with an absence of disability/mild impairment.
Discussion
The prevalence of smoking in this large representative sample of Australians with a psychotic illness was 66.6%, essentially the same prevalence as found in the 1997/1998 survey (Jablensky et al., 2000). Over the last 15 years, smoking has declined in the mainstream Australian population from approximately 26% to 19%. Clearly, people with a psychotic illness are being left behind in the effort to reduce tobacco smoking. As a result, a disproportionate number of people with a psychotic illness continue to suffer the economic and health costs of smoking. Young people with a psychotic illness reported the highest rate of smoking, suggesting that tobacco control efforts are not just failing to help older smokers quit but are also failing to prevent the uptake of smoking among adolescents and young adults with a psychotic disorder.
A recent national survey found that approximately two-thirds of Australians aged over 14 years have never been smokers, whilst approximately a quarter are ex-smokers (Australian Institute of Health and Welfare, 2011). In the current study, only 19% reported never having regularly smoked, while a further 14% had not smoked in the previous 4 weeks. This supports previous findings that people with a psychotic illness are both more likely to take up smoking and less likely to quit (de Leon and Diaz, 2005). On average, smokers in our sample began smoking before the onset of their illness and had spent the duration of their illness as a smoker or trying to quit smoking. Qualitative research has illustrated how smoking can become an intrinsic part of living with a psychotic illness (Lawn et al., 2002). Nevertheless, the majority of smokers in our sample had attempted to quit smoking and reported having tried to do so four to five times. This supports a common finding that people with a psychotic illness are interested in quitting smoking (e.g. Ashton et al., 2010; Moeller-Saxone, 2008). Research has shown that population-level anti-smoking campaigns have increased the knowledge and awareness of the dangers of smoking among people with psychosis, but in order to effectively reduce smoking prevalence there needs to be targeted strategies that address the unique barriers to cessation in this population (Thornton et al., 2011).
Whilst smoking is a major contributor to cardiovascular disease, it was not related to ‘at-risk’ levels of blood pressure, cardiovascular disease or high cholesterol in this study. This may be explained by the already high prevalence of cardiovascular risk factors in this population such as low levels of physical activity, poorer diets, disabling psychiatric symptoms and medication side effects. The lower BMI score among smokers may be attributed to the appetite- suppressing effects of nicotine (Mineur et al., 2011). Perceived physical health is a reliable predictor of mortality (DeSalvo et al., 2006), and the smokers in this study reported lower perceived physical health than non-smokers. Whilst this is hardly surprising, it underscores the impact that smoking has on subjective wellbeing.
We found few differences between factors associated with ever smoking compared to current smoking. Being younger at the time of interview was marginally associated with current smoking but was not significantly associated with ever smoking. Psychiatric history was not associated with current smoking when we controlled for demographic factors, but we found that those who reported a younger age of illness onset were more likely to have ever started to smoke, consistent with previous findings (Kelly and McCreadie, 1999). There was no difference in age of illness onset between current or former smokers.
Previous studies that have found an association between psychopathology or illness severity and current smoking may have been confounded by the associations between smoking and substance use and factors that are related to both the uptake of smoking and severity of the illness (e.g. being male and younger age of illness onset). Once we controlled for demographic factors, psychiatric history and substance use we did not find an association between current smoking and the positive symptoms of psychosis, depressed mood or loss of pleasure and manic symptoms. We did, however, find a marginally significant association between more severe negative symptoms and current smoking. Our results suggest that people with a psychotic illness share some of the same risk factors for smoking as the general population. Having a lower education, being male and being unemployed in the previous 12 months were associated with current smoking in our sample, similar to the general population (Siahpush and Borland, 2001). Among the subset of participants with schizophrenia/schizoaffective disorder, moderate to severe psychosocial disability was associated with current smoking after controlling for demographic factors, psychiatric history and substance use. This warrants further investigation.
Current smoking was associated with higher daily caffeine intake. This may be attributed to the increased metabolism of caffeine in the presence of nicotine (Zevin and Benowitz, 1999), or to personality traits such as high novelty seeking which have been linked to both tobacco and caffeine use (Gurpegui et al., 2007). Alcohol dependence and substance abuse/dependence in the previous 12 months were independently associated with current smoking, consistent with previous research among people with a psychotic illness (Hall et al., 1995; Heffner et al., 2012; Ostacher et al., 2006; Vanable et al., 2003; Waxmonsky et al., 2005). Problematic alcohol and substance use is associated with tobacco smoking in the general population (Degenhardt and Hall, 2001a) and is more prevalent among those with a severe mental illness (Degenhardt and Hall, 2001b). Moore and colleagues (2012) showed that problematic alcohol or cannabis use is far more common among individuals aged 18–24 years and among men in this patient sample. Problematic use of alcohol or cannabis is also associated with a younger initiation to smoking and fewer reasons for quitting smoking among people with a psychotic illness (Baker et al., 2007). There is also evidence to suggest that smoking is a risk factor for developing a substance use disorder (Lewinsohn et al., 1999). Further research is needed to understand the relationship between use of tobacco and other substances among people with a psychotic illness and the potential implications for prevention and cessation of tobacco smoking.
There were limitations to this study. The main limitation is the cross-sectional design of this study, meaning we cannot test for causal relationships. In this regard, care should be taken about inferring from the findings of the multivariate analyses, which only show associations whilst controlling for other variables. For example, we do not know whether the higher drug use in smokers is due to smokers being more likely to take drugs, drug users being more likely to smoke, or some unmeasured shared correlate. We relied on self-report and bias may have been present. Quit attempts, especially short ones, are often forgotten over time (Borland et al., 2012). Thus, the proportion of participants who reported that they have tried to quit and the number of attempts reported are likely to be underestimates. The present sample was representative of people receiving support from community mental health centers and non-government organisations. However, the sample may not be representative of those receiving privately funded treatment or those who have dropped out of treatment altogether. We explored associations between our measures of interest and current smoking and therefore we cannot say anything about how they might change with level of nicotine dependence.
In summary, the prevalence of smoking among people with a psychotic illness does not appear to be declining in Australia as it is for the general population. Further research is needed to explore whether the lack of decline is consistent across age, socioeconomic status, degrees of illness severity and functioning, and patterns of substance use. Given the increasing gap, it is imperative that clinicians and researchers increase the efficacy and application of targeted interventions to reduce tobacco smoking in this disadvantaged sector of the community. Smoking cessation strategies that also address other cardiovascular risk factors such as diet and exercise (e.g. Baker et al., 2009) might help reduce premature cardiovascular death risk and disability amongst people with psychosis. Clearly, our current strategies are not delivering reductions in smoking among Australians living with a psychotic illness. More research is needed as to what additional barriers people with psychotic illness face in successfully quitting, with interventions developed to target these issues.
Footnotes
Acknowledgements
This publication is based on data collected in the framework of the 2010 Australian National Survey of High Impact Psychosis. The members of the Survey of High Impact Psychosis Study Group are: V. Morgan (National Project Director), A. Jablensky (Chief Scientific Advisor), A. Waterreus (National Project Coordinator), R. Bush, V. Carr, D. Castle, M. Cohen, C. Galletly, C. Harvey, B. Hocking, A. Mackinnon, P. McGorry, J. McGrath, A. Neil, S. Saw and H. Stain. Ethics approvals for the study were obtained from relevant institutional human research ethics committees. This report acknowledges, with thanks, the hundreds of mental health professionals who participated in the preparation and conduct of the survey and the many Australians with psychotic disorders who gave their time and whose responses form the basis of this publication.
Funding
This research was funded by the Australian Government Department of Health and Ageing.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.