
Abstract
Objective:
To describe the prevalence and demographic, clinical and functional correlates of childhood trauma in patients attending early psychosis clinics.
Method:
Participants were recruited from outpatients attending four early psychosis services. Exposure to childhood trauma was assessed using the Childhood Trauma Questionnaire (CTQ). Psychopathology was measured using the Positive and Negative Syndrome Scale and the Depression, Anxiety and Stress Scale. Social and vocational functioning and substance use were also assessed.
Results:
Over three-quarters of the 100 patients reported exposure to any childhood trauma. Emotional, physical and sexual abuse were reported by 54%, 23% and 28% of patients, respectively, while 49% and 42% of patients reported emotional and physical neglect, respectively. Female participants were significantly more likely to be exposed to emotional and sexual abuse. Exposure to childhood trauma was correlated with positive psychotic symptoms and higher levels of depressive, anxiety and stress symptoms; however, it had no impact on social or vocational functioning or recent substance use.
Conclusion:
Exposure to childhood trauma was common in patients with early psychosis, and associated with increased symptomatology. Existing recommendations that standard clinical assessment of patients with early psychosis should include inquiry into exposure to childhood trauma are supported.
Introduction
Childhood trauma (CT) can have persistent adverse effects on an individual’s physical and mental health, social development and wellbeing (Norman et al., 2012). Differing descriptions of CT exist throughout the contemporary literature. While many studies define CT as all forms of physical and/or emotional ill-treatment, sexual abuse, neglect or negligent treatment (Krug et al., 2002; Norman et al., 2012), others have used broader definitions which include bullying and victimisation, parental loss and separation (Varese et al., 2012). For the purposes of this study, CT is defined as physical, sexual and emotional abuse and physical or emotional neglect (Daruy-Filho et al., 2011).
Historically, studies examining the relationship between CT and psychosis have reported inconsistent findings although recently, the association has become widely accepted. For example, a prospective case control study of 1,612 Victorian children identified as being exposed to childhood sexual abuse (CSA) reported increased rates of treatment required for mental illness but no increased risk of schizophrenia (Spataro et al., 2004). However, an extension of this study employing a larger sample (N = 2,759) found those exposed to CSA were 2.1 and 2.6 times more likely to be diagnosed with psychosis and schizophrenia, respectively (Cutajar et al., 2010). The association between CT and psychotic disorders is now well accepted (Bendall et al., 2008; Matheson et al., 2013; Morgan and Fisher, 2007; Shevlin et al., 2007; Varese et al., 2012).
In a literature review, the prevalence of CT in those with psychosis was reported to range widely from 59% to 100% (Read et al., 2005). Similarly, Australian prevalence rates of trauma also vary with physical abuse in the range of 5–10%, neglect in the range of 2–12% and emotional maltreatment in the range of 6–17% (Australian Insitiute of Family Studies, 2013). Sexual abuse has been reported to affect 4–16% of boys and 12–34% of girls (Dunne et al., 2003). The wide variation in the prevalence of CT is due to the definition of childhood trauma utilised, methods of reporting (e.g. self-report vs. use of child protection agency records), sex and age of the individuals. The use of validated standardised measures of CT is one method of overcoming problems arising from definitional variation.
In spite of the many studies examining the association between CT and psychotic disorders, few have examined CT in patients with early psychosis (EP). Ucok and Bikmaz (2007) evaluated the impact of CT among 57 inpatients with first-episode schizophrenia. Those exposed to childhood sexual abuse reported more severe positive psychotic symptoms and were more likely to have made a recent suicide attempt while those exposed to childhood emotional abuse reported more hallucinations and delusions. Similarly, Bendall et al. (2013b) reported that EP patients exposed to childhood sexual abuse had more severe hallucinations and delusions, and Wang and colleagues (2013) found CT was significantly correlated with hallucinations (r = 0.174, P = 0.049) in EP patients but not patients with chronic psychosis. Finally, a study by Ramsay et al. (2011) found correlations between childhood emotional abuse and neglect and positive and negative psychotic symptoms, respectively, in disadvantaged, African-American EP inpatients.
The impact of CT on other symptom domains of patients with EP is not well established. While depression, anxiety and stress symptoms have been shown to be higher in patients with persistent psychotic disorders exposed to CT (Lysaker and Salyers, 2007; Schenkel et al., 2005), no studies have examined this association in patients with EP. By contrast, increased rates of lifetime substance abuse have been reported in EP populations with a history of CT (Schafer and Fisher, 2011). A study of 61 EP inpatients with concurrent substance use found 85% had a history of CT (Fraser et al., 2012) while Ramsay et al. (2011) reported CT was associated with lifetime cannabis use and a younger age of onset of alcohol use. Although social and vocational functioning has been identified as a key treatment outcome for clinicians (Figueira and Brissos, 2011) and patients with psychosis (Stain et al., 2012), very few studies have examined the impact of CT on functioning in EP patients. Poorer premorbid functioning was associated with a history of sexual and/or physical abuse in first-episode mania (Conus et al., 2010) and a history of any CT in 102 EP patients (Stain et al., 2013). In summary, there are few studies examining the impact of CT on the clinical presentation and functioning of patients with EP. Those available suggest patients with a history of CT are more symptomatic and have poorer levels of premorbid functioning.
This study aimed to establish the prevalence of CT in patients attending EP outpatient services in an Australian city. A further aim was to examine the demographic, clinical and functional correlates of childhood trauma in EP patients. It was hypothesised that exposure to CT would be associated with increased positive and negative psychotic symptomatology and higher levels of anxiety, depression and stress. Furthermore, we hypothesised that those exposed to CT would report greater levels of substance use and have poorer levels of social and vocational functioning.
Method
Participants
Participants were recruited from four specialist EP outpatient clinics in South-East Queensland, Australia. Patients attending these services were in the age range 15–25 years, diagnosed with a psychotic illness and had not received greater than 2 years of mental health treatment for psychosis. Participants were informed of the aims of the study by their treating clinician and those willing to participate provided written consent.
Instruments
Demographic and clinical information
Demographic data including age, sex, relationship status, country of birth, language spoken at home, ethnicity, dependents and employment status were collected using a standardised questionnaire completed by participants. Clinical data collected were primary and secondary diagnoses made by a consultant psychiatrist using the 10th Edition of the International Classification of Diseases (ICD-10) (World Health Organization, 1992) and estimated duration of untreated and treated psychosis which was verified by treating clinicians and clinical records. Duration of untreated psychosis (DUP) was defined as the time between onset of psychotic symptoms as reported by participants or carers and first contact with psychiatric services.
Psychotic symptoms
The Positive and Negative Syndrome Scale (PANSS) is an interviewer-rated scale measuring psychotic and general symptoms in patients with psychosis. Prior to initiating the study, clinicians were trained in the PANSS by an investigator experienced in using the instrument. Clinicians were required to obtain an inter-rater reliability score of α = 0.80 or greater using the PANSS on a videotaped clinical interview before being permitted to collect data for the study.
Childhood trauma
The 28-item Childhood Trauma Questionnaire (CTQ) was used to assess levels of exposure to childhood abuse and neglect (Bernstein, 1998; Scher et al., 2001). It was chosen as it examines emotional, physical and sexual abuse, as well as emotional and physical neglect and yields an overall childhood trauma score. Each item is scored on a 5 point Likert scale. An example of an item is ‘Someone tried to make me do sexual things or watch sexual things’ to which responses range from ‘never true’ (1) to ‘very often true’ (5), producing scores in the range of 5 to 25 for each trauma sub-scale and 25 to 125 for the overall trauma score. Trauma prevalence was estimated using thresholds described in the CTQ manual (Bernstein, 1998). Sub-scale classifications of none to minimal were categorised as trauma absent while sub-scale classifications of minimal to moderate, moderate to severe and severe to extreme were categorised as trauma present. For correlation with clinical measures data remained in continuous form as used in previous research (Ucok and Bikmaz, 2007).
Depression, anxiety and stress
The depression, anxiety and stress scale (DASS21) is a 21-item self-report measure examining symptoms in these three domains over the previous seven days (Lovibond and Lovibond, 1995). Total scores for each subscale were used for correlation analysis.
Social and vocational functioning
The Activity and Participation Questionnaire (APQ6) is a retrospective, self-report instrument assessing vocational activity and social participation in the previous 7 days (Stewart et al., 2010). Measures of vocational activity include hours spent in current employment, studying, job seeking and volunteer work. Social participation measures include hours spent engaged in social activities (e.g. visiting a friend or relative or participation in a sporting or recreational group). For statistical analysis, patients were categorised dichotomously as vocationally active if they were employed or studying for a minimum of 1 hour in the previous 7 days, or not in education, employment or training (NEET). Social functioning within the previous 7 days was categorised into three groups: absent; low; and high. Patients who did not engage in any social activity were classed as absent, those participating in social activities for between 1 and 6 hours were categorised as low functioning and patients who engaged in 7 or more hours were classed as high functioning.
Current and lifetime substance use questionnaire
Participants’ substance use over the previous 28 days was rated by clinicians using a standardised questionnaire. Levels of use were categorised into four groups: no use (no substance use within the last month); infrequent use (used once to twice in the previous month); regular use (used one to twice per week for the previous month); and frequent use (used three or more times per week for the previous month). For statistical analysis, substances were grouped into four forms: alcohol; tobacco; cannabis; and other illicit drugs. Illicit drugs included amphetamines, ecstasy, opiates, benzodiazepines, volatile substances (e.g. inhalants, glue, petrol) and other drugs (e.g. ecstasy, cocaine, LSD).
Procedure
Following ethics approval, patients identified by their treating clinician as being able to provide informed consent were invited to participate in the study. We have previously reported an analysis of this recruitment strategy revealing clinicians were more likely to approach patients who were less symptomatic and had better insight (Patterson et al., 2014). Patients who agreed to participate were more likely to be actively engaged in treatment (Patterson et al., 2014). Consent of both participants and guardians was obtained for those aged under 18 years. The PANSS, APQ6 and substance use questionnaire were administered by PANSS-trained clinicians. Following this, participants completed self-report questionnaires (CTQ and DASS21). Participants received a gift card for participating. No information was available on those patients who refused to participate or who were not approached.
Statistical analysis
As CTQ scores were not normally distributed, associations between CTQ scores, positive and negative symptom scores and DASS21 responses were examined using Spearman’s correlations. Positive and negative symptom scores were transformed from interval to ratio data by subtracting the theoretical minimum (7 points) from each score (Obermeier et al., 2011). The association between CTQ scores and vocational functioning was examined using Mann-Whitney U-tests with a median split used to define groups. Analysis of the relationship between CTQ scores and social functioning was completed using Kruskal-Wallis H-tests also using a median split used to analyse groups. Univariate ANOVA calculations with bootstrapping were used to examine the association between CTQ scores and substance use in the past month. Tests of significance were two-tailed, Holm-Bonferroni corrections were implemented in post-hoc analysis where applicable and the software used to perform analyses was IBM SPSS for Windows version 22.0 (IBM Corporation, 2013).
Results
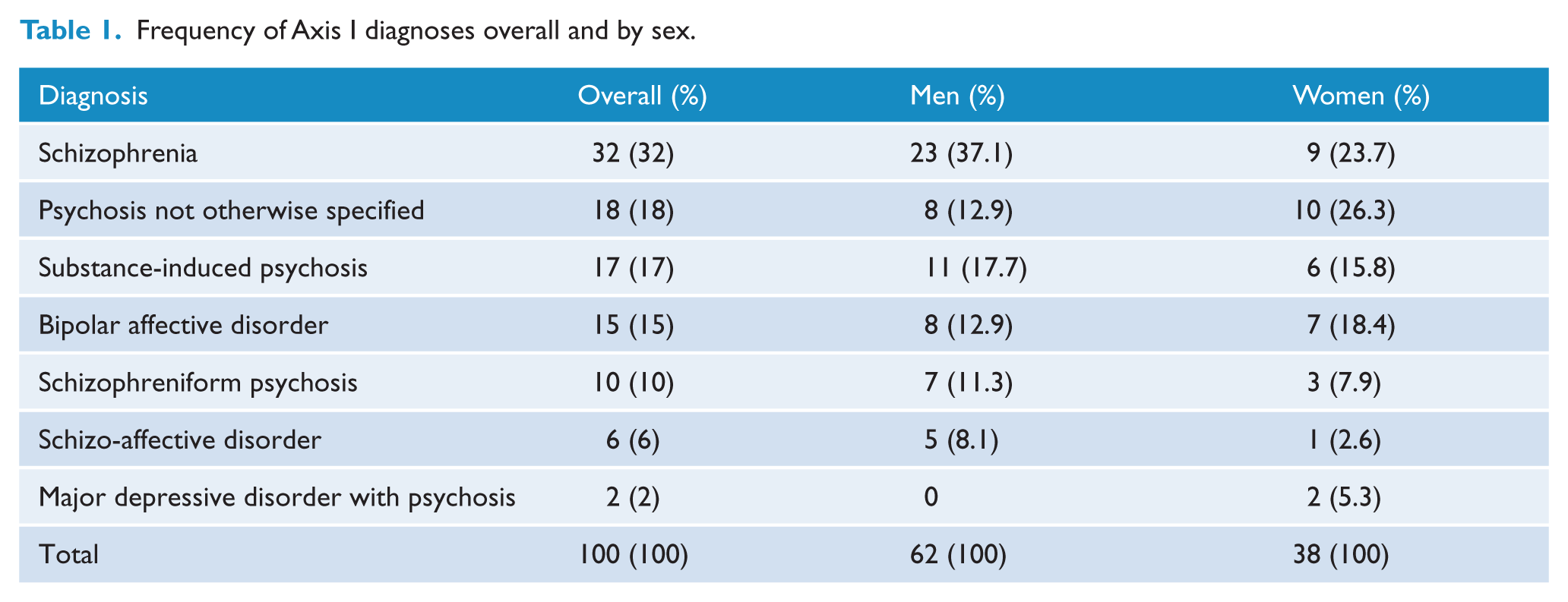
One hundred and six patients consented to participate; however, only 100 completed all measures and were included in final analysis. This sample consisted of 62 men and 38 women with a mean age of 21.4 years (SD = 2.28, range = 17–26 years) and a median DUP of 4 weeks (SD = 44.4, range = 1–266 weeks). Eighty-seven percent were single, 76% were born in Australia and 93% had no dependents. Fifty-six percent were unemployed, 12% were employed part-time while 9% were employed full-time. A further 18% were engaged in educational activities (university or technical college). Schizophrenia was the most common diagnosis (32%) followed by substance-induced psychotic disorder (18%) and psychotic disorder not otherwise specified (17%). A complete list of diagnoses for the total sample and by sex is reported in Table 1. Men were more frequently diagnosed with schizophrenia while women were more likely to receive a diagnosis of psychotic disorder not otherwise specified.
Frequency of Axis I diagnoses overall and by sex.
More than three-quarters (N = 82) of patients receiving treatment from an EP clinic reported exposure to any form of abuse or neglect, with 64 patients (64%) exposed to at least one form of abuse while 62 patients (62%) were exposed to one or more forms of neglect. Sex differences were observed with women significantly more likely to report exposure to emotional and sexual abuse (Table 2) and this abuse was more severe in women (Table 3).
Rates of trauma in patients with early psychosis.
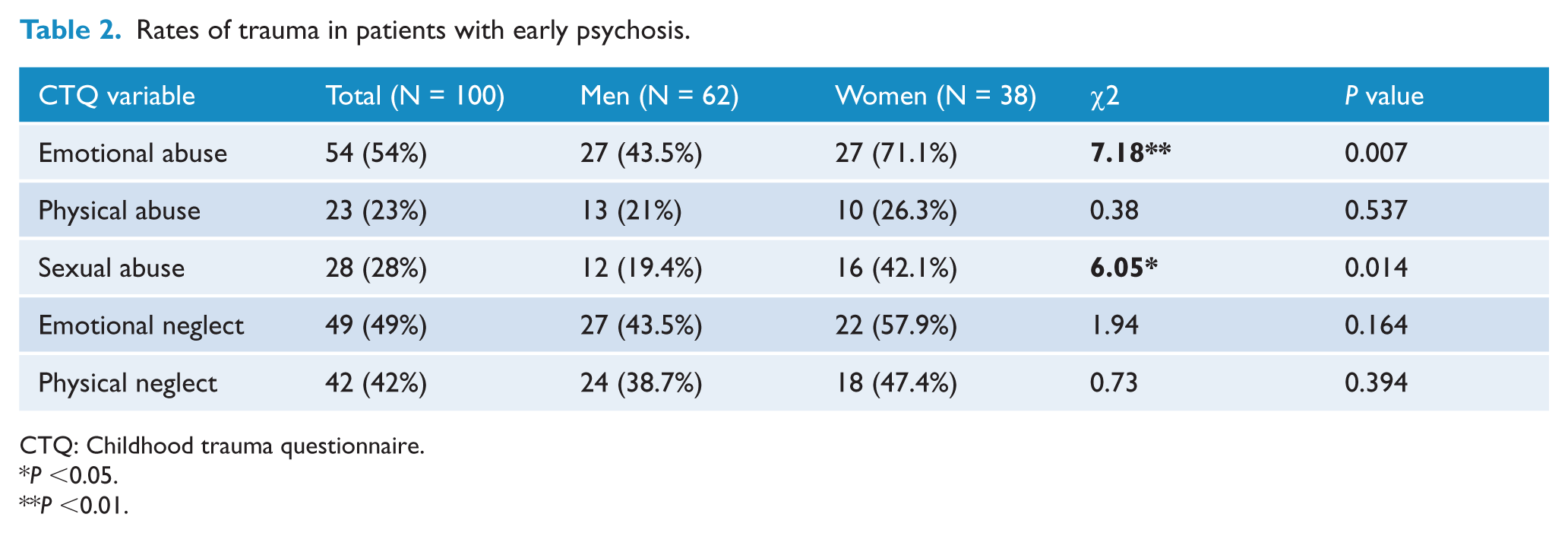
CTQ: Childhood trauma questionnaire.
P <0.05.
P <0.01.
Distribution of trauma severity overall and by sex.
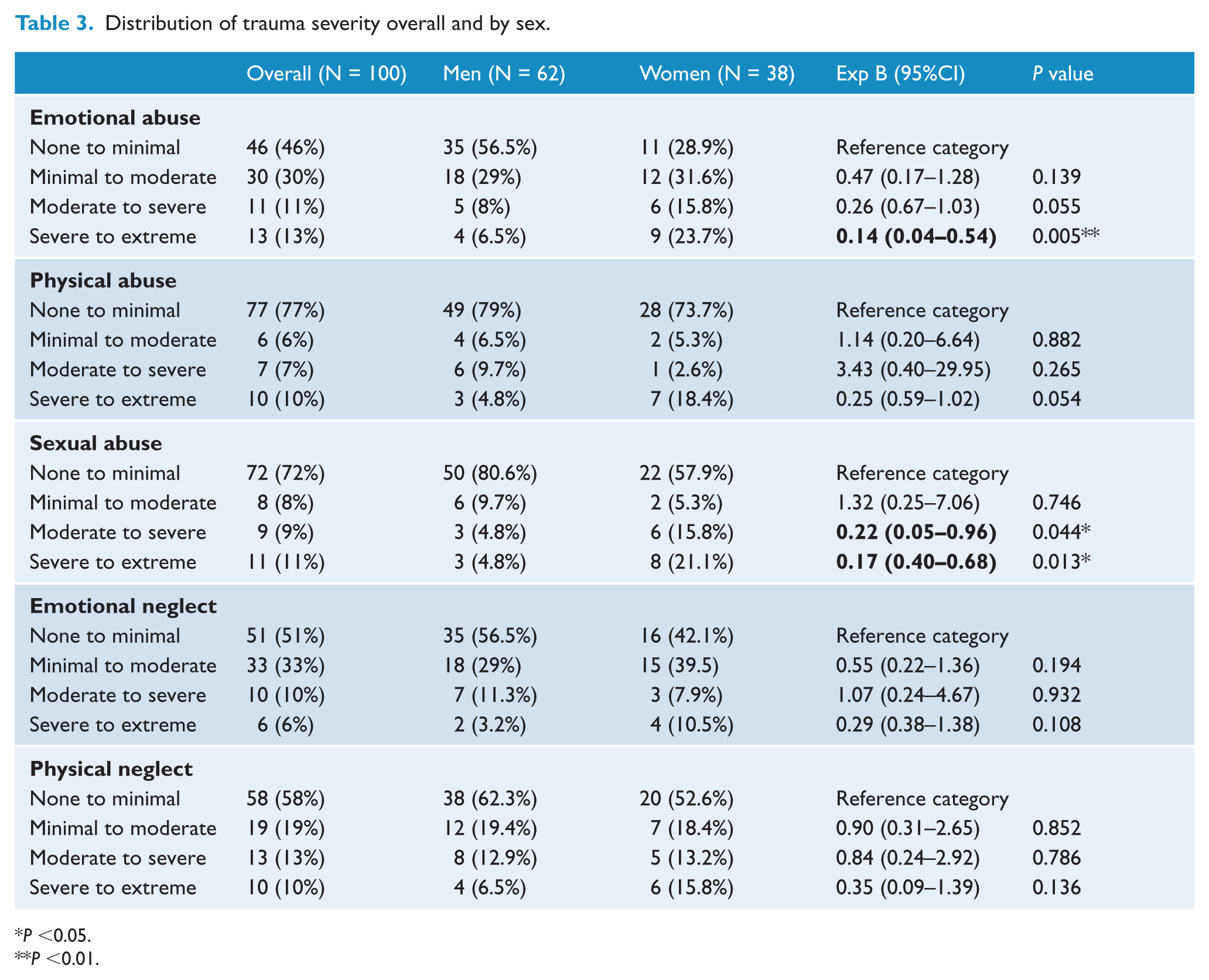
P <0.05.
P <0.01.
The total CTQ score was significantly positively correlated with positive psychotic symptoms only while physical neglect was significantly correlated with both positive and negative psychotic symptoms. After controlling for multiple comparisons, correlations between total CTQ score and positive symptoms and physical neglect and negative symptoms did not reach statistical significance. This was most likely due to the restricted sample size and limited power for multiple comparisons. There was a trend towards significance of emotional neglect also being correlated with both psychotic symptom domains. Exposure to other types of CT was not significantly correlated with positive or negative psychotic symptoms (Table 4). When stratified by sex, physical neglect was correlated with both positive and negative psychotic symptoms in men and women (Supplementary Table 1).
Correlations of childhood trauma and positive and negative psychotic symptoms.
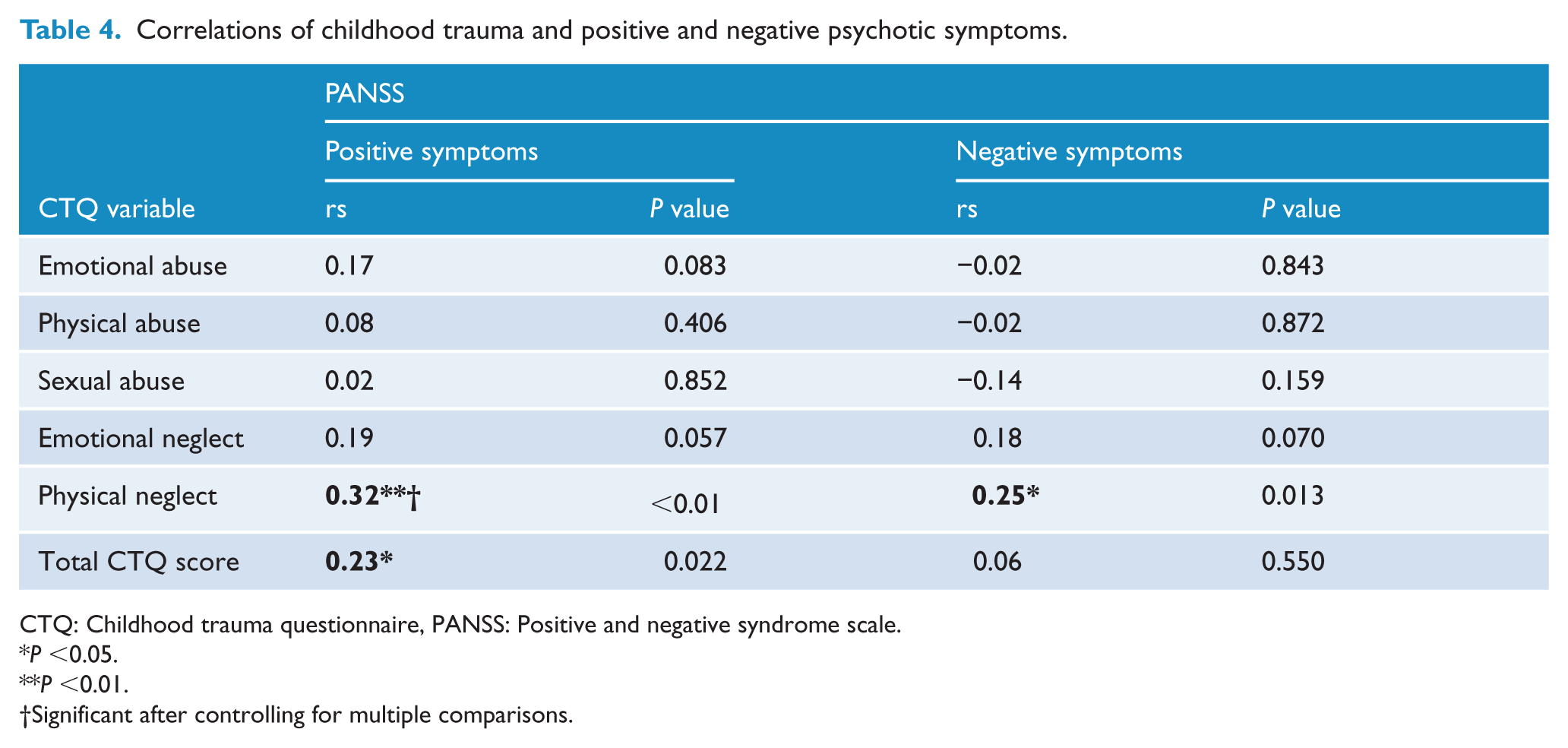
CTQ: Childhood trauma questionnaire, PANSS: Positive and negative syndrome scale.
P <0.05.
P <0.01.
Significant after controlling for multiple comparisons.
Total CTQ scores were significantly positively correlated with all forms of emotional distress. Exposure to emotional or physical abuse or physical neglect were correlated with increased depression, anxiety and stress symptoms while sexual abuse was correlated with increased symptoms of depression only (Table 5). The correlations between trauma exposure and emotional distress were very similar when the sample was stratified (Supplementary Table 2).
Correlation of childhood trauma and depression, anxiety and stress symptoms.
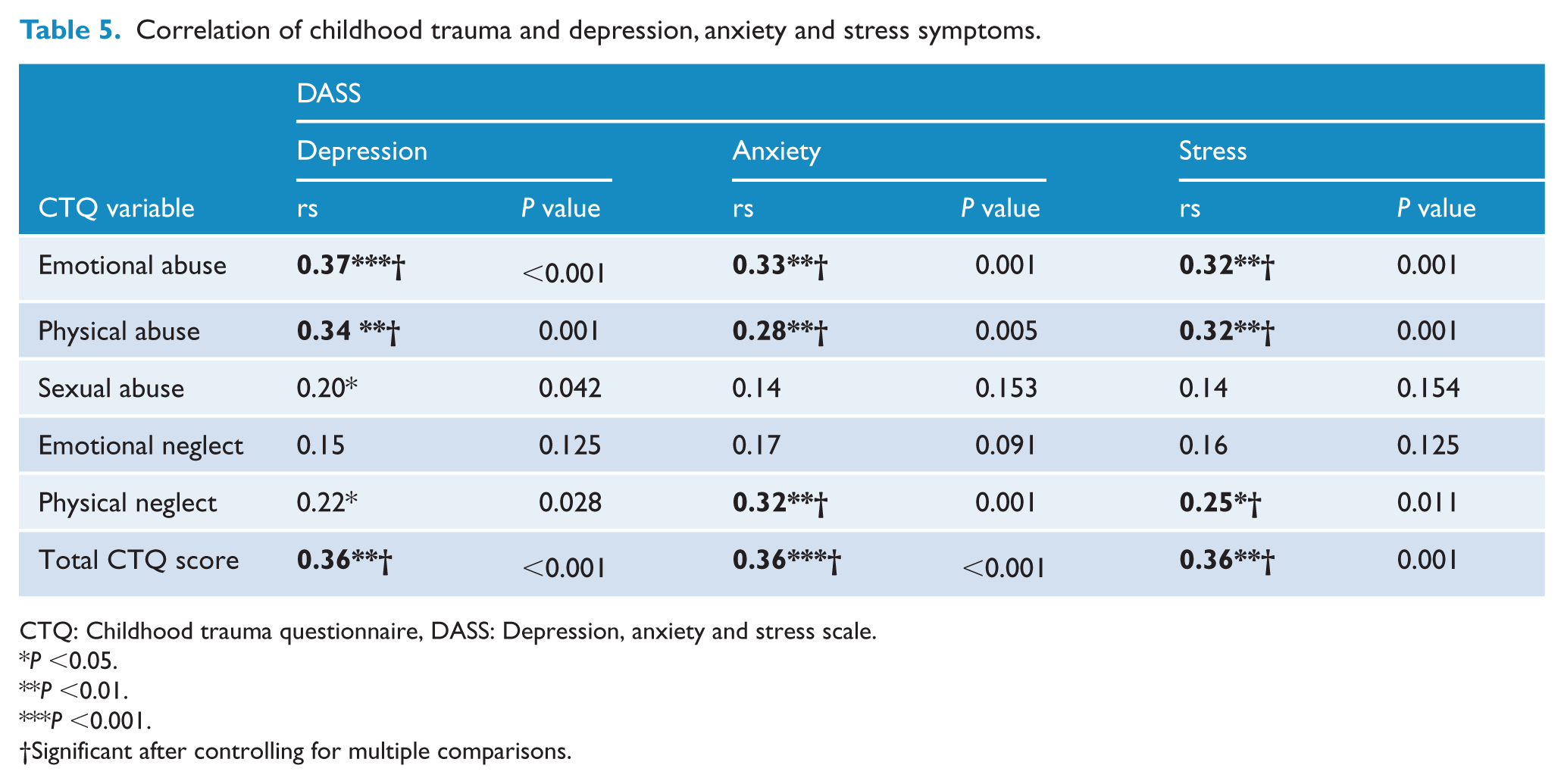
CTQ: Childhood trauma questionnaire, DASS: Depression, anxiety and stress scale.
P <0.05.
P <0.01.
P <0.001.
Significant after controlling for multiple comparisons.
Forty-five percent of patients were vocationally active in the previous 7 days. Exposure to CT was not significantly associated with vocational activity in patients with EP overall (Supplementary Table 3) or when stratified by sex (Supplementary Table 4). Six percent of patients did not engage in any social activity within the previous 7 days, whereas 39% engaged in low levels and 53% engaged in high levels of social functioning. There was no statistically significant difference in mean scores for any trauma or total CTQ score for each level of social functioning overall (Supplementary Table 5) or when stratified by sex (Supplementary Table 6).
In the previous month, both alcohol and tobacco were used by 67% of patients while 27% reported using cannabis and 17% reported illicit drug use. No associations between exposure to CT and the level of tobacco, alcohol, cannabis or other illicit drugs used in the past month were found (Supplementary Tables 7 and 8). When stratified by sex, no correlations were observed for either sex regarding alcohol use (Supplementary Table 9), tobacco use (Supplementary Table 10), cannabis use (Supplementary Table 11) and illicit drug use (Supplementary Table 12).
Discussion
This observational study reports more than three-quarters of patients attending early psychosis services in Queensland, Australia had been exposed to CT, a prevalence comparable to other samples of EP patients (Ramsay et al., 2011; Ucok and Bikmaz, 2007; Wang et al., 2013). Compared to Australian population samples (Australian Insitiute of Family Studies, 2013), prevalence rates of all forms of CT are increased in patients with EP. Contrasting previous EP studies, women were significantly more likely to report childhood sexual and emotional abuse than men. The increased rate of sexual abuse for women is consistent with a meta-analysis reporting Australian women in the general population are three times more likely to be sexual abused compared to males (Stoltenborgh et al., 2011). Patients with early psychosis exposed to CT were more likely to have higher levels of positive psychotic symptoms and depression, anxiety and stress symptoms. After controlling for multiple comparisons, the association between total CTQ and positive symptoms did not reach statistical significance most likely due to a lack of power leading to a type II error. Depression in those with EP has been associated with poorer outcomes (Challis et al., 2013), increased risk of suicidal ideation and deliberate self-harm (Upthegrove et al., 2010).
Conversely, EP patients exposed to CT did not have lower levels of social or vocational functioning or increased risk of recent substance use. Although people exposed to CT in the general population have higher rates of substance use (Afifi et al., 2012), substance use is also elevated among those with EP (Barnett et al., 2007; Sevy et al., 2001). As such, the lack of association between substance use and CT in this clinical sample is most likely due to the mediating effect of EP.
Emotional abuse was prevalent in this sample with 54% of all participants and 71.1% of girls reporting this experience during childhood. These rates are consistent with those previously reported in patients with early psychosis (Bendall et al., 2012; Ucok and Bikmaz, 2007), though much more common than other populations attending health services. For example, Hollingsworth et al. (2012) reported that 37% of women (N = 239) attending an antenatal service in the same city as the current study experienced childhood emotional abuse as measured by the CTQ. The high rates of emotional abuse in this study are consistent with previous reports suggesting that childhood trauma is a risk factor for psychosis (Varese et al., 2012).
Consistent with previous studies of EP populations, total CTQ scores were correlated with positive psychosis symptom scores (Ucok and Bikmaz, 2007; Wang et al., 2013). This association was driven in particular by neglect and emotional abuse. Relative to other forms of childhood maltreatment, exposure to neglect and emotional abuse during childhood adversely impacts adolescent mental health (Mills et al., 2013) and are associated with personality and mood disorders during adulthood (Carr et al., 2013). Neglect, in particular, has been shown to increase the risk of atypical neurodevelopment (Glaser, 2014; Panzer, 2008). It is therefore not surprising that neglect and emotional abuse were correlated with increased positive symptoms.
Several theories have been proposed to explain the relationship between CT and positive psychotic symptoms. One such theory is that post-traumatic stress disorder (PTSD) and psychosis involve shared mechanisms such as dissociation, attributional style and interpretation of intrusions (Bendall et al., 2013b; Morrison et al., 2003). Post-traumatic intrusions may be misattributed by individuals to an external source and are subsequently experienced as hallucinations (Bentall, 2003; Bentall and Fernyhough, 2008). Another theory proposes exposure to CT is associated with both an externalising attribution style and a tendancy to perceive the world as hostile (Bentall and Fernyhough, 2008; Johns et al., 2014). Psychological interventions for psychcotic symtoms (Thomas et al., 2014) in those who have experienced CT are infromed by these theoretical frameworks.
Consistent with previous reports, physical neglect was correlated with negative psychosis symptom scores (van Dam et al., 2014) . Multiple hypotheses have been suggested for this relationship with most postulating the association is a result of an abstinence from stimulating experiences as a child leading to psychosocial deficits (Colvert et al., 2008). These deficits have been associated with increased levels of positive and negative symptoms in those with EP (Addington et al., 2003) and schizophrenia (Gallagher and Jones, 2013).
The most significant limitation of this study was the aforementioned recruitment biases (Patterson et al., 2014). We were unable to obtain data on those who did not participate and therefore cannot make meaningful comparisons between participants and non-participants. This was a reflection of undertaking observational research in real-world clinical services. The other significant limitation was the use of a self-report measure of CT which could not be independently verified. However, the CTQ is a well validated, standardised instrument for measuring CT and previous research has shown good reliability of self-reporting CT in those with psychosis (Read et al., 2005) and EP (Fisher et al., 2011).
In spite of the above limitations, this is the first study to examine and show that exposure to CT is associated with increased symptoms of depression, anxiety and stress in those with early psychosis. It supports previous research showing that CT is common in those with early psychosis and associated with higher levels of positive psychotic symptoms (Bendall et al., 2013b; Ramsay et al., 2011; Ucok and Bikmaz, 2007; Wang et al., 2013). With this in mind, incorporating trauma informed care into EP treatment programs for patients who have experienced CT may improve outcomes (Bendall et al., 2013a). However, clinicians are sometimes reluctant to inquire if patients have experienced CT for fear that it may fracture rapport (Bendall et al., 2013a) and information regarding CT is rarely disclosed voluntarily by patients (Read et al., 2006, 2007). Similar to other patient groups, clinicians’ understanding of the childhood experiences of patients with early psychosis can improve therapeutic alliance and inform psychotherapeutic interventions (Nafisi and Stanley, 2007). Therefore, given the high prevalence of CT and the associated psychological distress that occurs in patients with EP, we support previous recommendations (Bendall et al., 2013a; Scott et al., 2007; Ucok and Bikmaz, 2007) that standard clinical care of patients with EP should include inquiry into exposure of CT in order to inform treatment.
Footnotes
Acknowledgements
The authors would like to thank the clinicians and patients who kindly donated their time during data collection.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.