
Abstract
Intervening early following the onset of psychosis is not only intuitively appealing but is based on relatively robust evidence of a relationship between the length of untreated psychosis and clinical and social outcomes [1–3]. In a recent critical review, Norman and Malla [3] concluded that duration of untreated psychosis (DUP) is related to time to remission, the level of remission achieved and other measures of, at least, short-term outcome such as the level of residual positive and negative symptoms. Delay in treatment may also affect outcome on measures of social functioning and quality of life [4–6]. Patients with a first-episode of psychosis are likely to obtain the greatest benefit if treatment provided is specifically designed for this early phase of the illness in addition to these interventions being provided early following the onset of psychosis [4, 7, 8].
Following the publication of several key papers in Schizophrenia Bulletin in 1996 [4, 7, 9, 10], early intervention in psychotic disorders has attracted a significant interest in many countries. Growth of several clinical and research programmes has been observed in Australia, New Zealand, Europe and Canada. In this paper, a brief overview of the progress made in developing early intervention programmes in Canada will be presented, followed by a more detailed description of one of the Canadian clinical/research programmes and a summary of published data evaluating the effectiveness of this early intervention programme.
Nationwide Canadian early intervention initiatives
While investigations regarding first-episode psychosis have been carried out for many years in several Canadian centres, more integrated early psychosis programmes have only emerged in the last 5 years. Four such clinical/ research programmes were developed independently in Calgary, London (Ontario), Toronto and Halifax. While each of these programmes has distinct characteristics and specific research interests, they all serve mostly urban populations and provide phase-specific treatment to individuals newly diagnosed with psychosis. Brief descriptions of these programmes are available in a recent book edited by Edwards and McGorry [11].
More recently, several other programmes have been initiated or are being planned in almost all of the Canadian provinces, primarily through efforts of clinicians and advocacy on the part of families. The public policy initiatives are invariably lagging behind the enthusiasm shown by clinicians and families. Within the province of Ontario (population of 11.8 million) a working group of clinicians/researchers, consumers of service (patient and family members), self-help and other community organizations has been established in order to influence mental health policy and funding decisions. This group has been successful in obtaining research funding for tracking outcomes of first-episode psychosis (FEP) in four academic centres.
Prevention and Early Intervention Programme for Psychosis (PEPP), London, Ontario
This early intervention programme was established in 1997 following significant modifications to an earlier community-orientated programme for treatment of schizophrenia and related psychotic disorders [12]. PEPP is based on a conceptual framework that promotes a stressvulnerability hypothesis for understanding psychotic disorders and targeting nonaffective psychoses rather than a specific diagnosis of schizophrenia. The programme consists of two essential components: a phase-specific integrated medical and psychosocial assessment and treatment; and early community case detection to reduce delays in treatment.
An overview of the model (for details see http://www.pepp.ca)
The PEPP utilizes an assertive case management model, modified to suit the needs of mostly young people and their families [13], as its central framework (see Fig. 1). The model involves a comprehensive approach with intensive medical and psychosocial management being provided by a nurse or social worker case manager. The case manager's role includes the functions of assessment, treatment and working through the patient's recovery from psychosis. This is achieved through a close partnership with families, a strong therapeutic relationship with the patient and, whenever possible, reliance on liaisons with generic community services, educational institutions and employers to reintegrate the young person to his/her full potential over an initial 2-year follow-up period. Involvement in the direct delivery of one or more specific psychosocial group interventions and individual supportive therapy are important components of a case manager's role. The goal is to normalize the young person's environment as soon as possible, including re-establishment of peer relations. Housing through special group homes and utilization of long-term disability benefits is actively discouraged to avoid the assumption of a chronic sick role.
Case management model.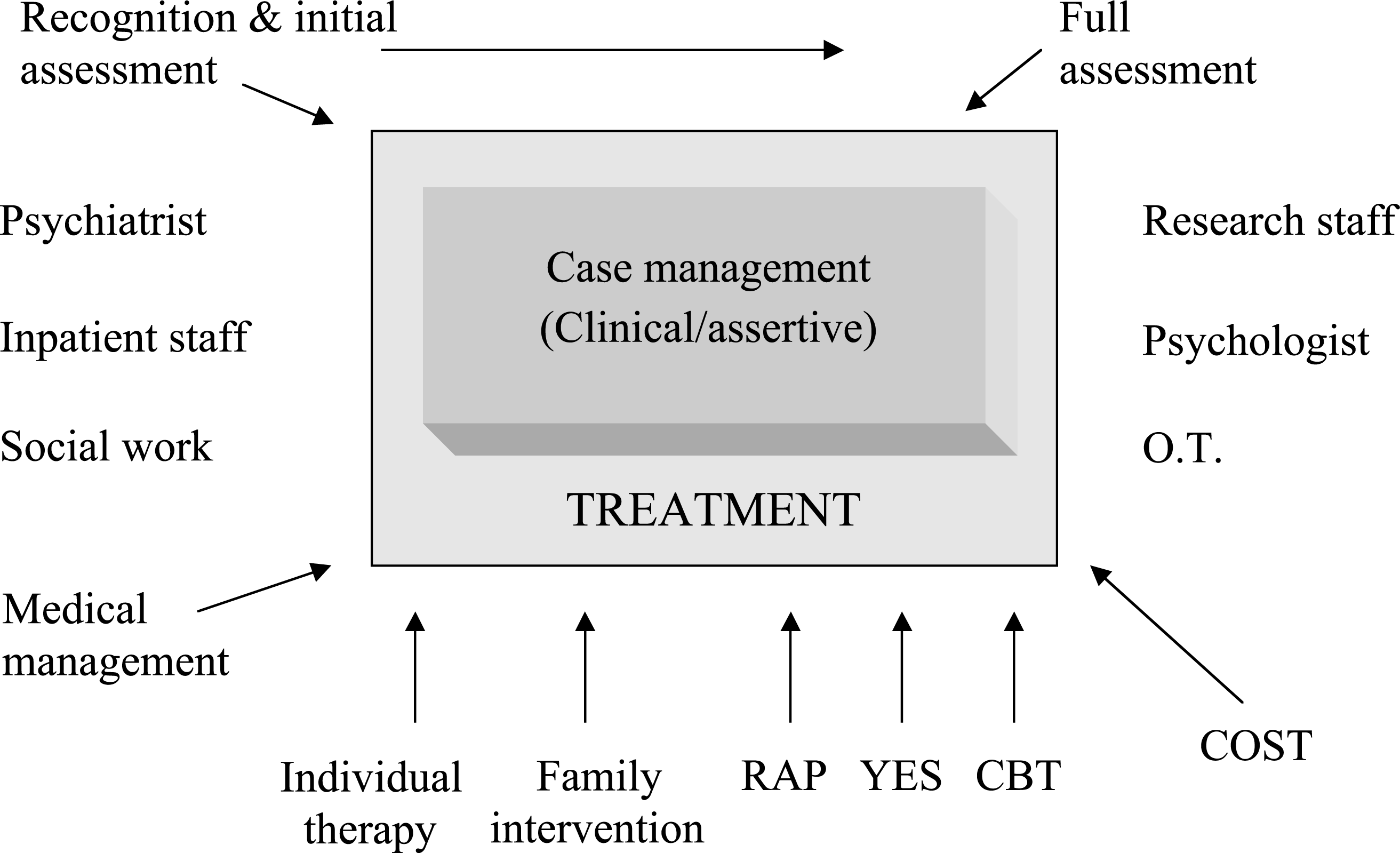
Patients stay in the core programme utilizing all interventions, especially case management, for a minimum of 2 years. Patients not recovered sufficiently to assume independent functioning and/or not in remission are provided extended case management for an additional 1–3 years, while the majority (82%) graduate and are followed by their programme psychiatrist. For the latter, case management is reintroduced temporarily in case of relapse or a crisis until the crisis is resolved. All patients continue with medical management with their respective psychiatrists in the programme for at least 5 years. Most are seen every 1–3 months while stable.
Case finding and assessment
Strategies for reducing delays in treatment of psychosis
Barriers to appropriate care for individuals suffering from a first-episode of psychosis are likely to exist at different levels of a traditional referral/treatment system, but may vary across various health care systems [9]. These include the difficulty primary care physicians and other health care workers experience in identifying early signs of psychosis and often result in multiple visits before an appropriate referral is made [14]. A necessary component of an early intervention programme therefore consists of strategies that would reduce delays in new cases of psychosis receiving assessment and treatment [4, 15, 16]. We have chosen to introduce strategies for reduction of delay in treatment in two phases. The contents of the phase-specific treatment programme are being maintained unchanged throughout both phases.
Phase I (1997–1999), funded from within the clinical service funds, involved improving access through adoption of an open referral policy, provision of a prompt response with an assessment carried out within 24–48 h in the clinic or at the patient's home. All health-related referral sources in the catchment area were identified and informed through brochures describing the establishment of the programme, the nature of psychosis and the process of assessment, integrated medical and psychosocial treatments, as well as research conducted in the programme.
Phase II of the strategy for reducing delays in treatment has consisted of a community-wide case-detection programme added to the procedures already in place and funded by the Ministry as a special one time youth project. This initiative includes provision of information regarding identification of psychotic symptoms and behaviour to potential sources of referral and providing basic information regarding psychosis to all members of the community. The latter has involved community-wide campaigns using written materials (pamphlets, posters, calendars and bookmarks), the media (TV and radio) and setting up specific education programmes in all secondary schools and postsecondary institutions and providing public forums for education. The posters consist of a brief description of key symptoms of psychosis and the brochures and calendars provide a detailed description of the nature and early signs of psychosis and the advantages of early intervention. These have been placed in key locations such as shopping malls, pharmacies and the public transit system. Consumers of service (patients and families) have been involved in the planning, fundraising and wider community dissemination of information regarding psychosis. In addition, direct contact established with each educational institution and referral source has been followed by presentations, seminars and workshops.
Assessment and engagement
Following direct contact with the source of referral an assessment clinician conducts a brief screening to ensure that the patient may have psychotic symptoms or be at high or imminent risk for psychosis followed by a formal initial assessment carried out within a maximum of 48 h (depending on the urgency) by an experienced clinician (a nurse) either in the clinic setting or at the patient's home. A full assessment of the patient with a psychiatrist is carried out following a review of the initial assessment, in order to confirm the presence of a nonaffective psychosis followed later by a Structured Clinical Interview (SCID-IV) to confirm DSM-IV diagnosis of a psychotic disorder. For clinical purposes, only a generic diagnosis of psychosis is made at this stage, to be reviewed 1 year later. Patients (16–50 years old) who meet criteria of a nonaffective psychosis, live in the defined catchment area (population 360 000 urban and 30 000 rural) and have not received antipsychotic treatment for a period greater than 1 month are asked to sign a consent for assessment and treatment. Patients presenting other diagnoses are referred to respective treatment programmes. However, approximately 10% of patients still receive a diagnosis of affective psychosis following completion of the SCID-IV at 1 year. Patients who do not meet criteria for diagnosis of a psychotic disorder but are judged to meet criteria for ‘at risk mental state’, a state of pre-psychosis as defined by the PACE clinic [17, 18] are followed-up regularly by individual clinicians and their mental state monitored to gauge transition to psychosis or recovery.
Following admission to the programme an assessment of the patient's quality of life (client, provider and family versions of the Wisconsin Quality of Life scale [19]), and cognition is conducted as early as clinically feasible. The cognitive assessment encompasses several areas of functioning: intellectual (premorbid and current), executive, attention, working memory, speed of processing, learning and short-term and long-term/auditory and visual memory, self-reported cognition and emotional functioning [20]. Symptom and side-effect assessments are repeated at regular intervals with standard instruments while cognitive and quality of life assessments are repeated at the end of 1 and 2 years.
Treatment
Medication management
While specific treatment for psychosis begins with the initiation of antipsychotic medication, patients who initially refuse drug therapy are provided support and education along with their families. This may extend for weeks and, occasionally, several months. The choice of antipsychotic medication is established through a treatment protocol (see Fig. 2) that is explained to the patient and family by the psychiatrist. Patients are started on a dosage as low as 0.5 mg to 1 mg of risperidone, 5 mg of olanzapine or, less frequently, 50–100 mg of quetiapine and increased over several days to 2, 10 and 300 mg a day, respectively. If needed, the dose of the medication is increased to a maximum tolerated dose up to 6 mg, 20 mg and 900 mg, respectively. While side-effects are monitored closely by all clinical staff involved, standard ratings of movement disorders and sexual dysfunction are carried out by the treating physician biweekly for the first month, on a monthly basis for the subsequent three months and every three months thereafter over the 2-year period of follow-up. Failure of treatment to adequate trials with two novel antipsychotics results in the discussion of clozapine therapy with the patient and the family. Typical antipsychotic medications are used only as depot preparations when adherence to oral medications becomes problematic.
Medication protocol guide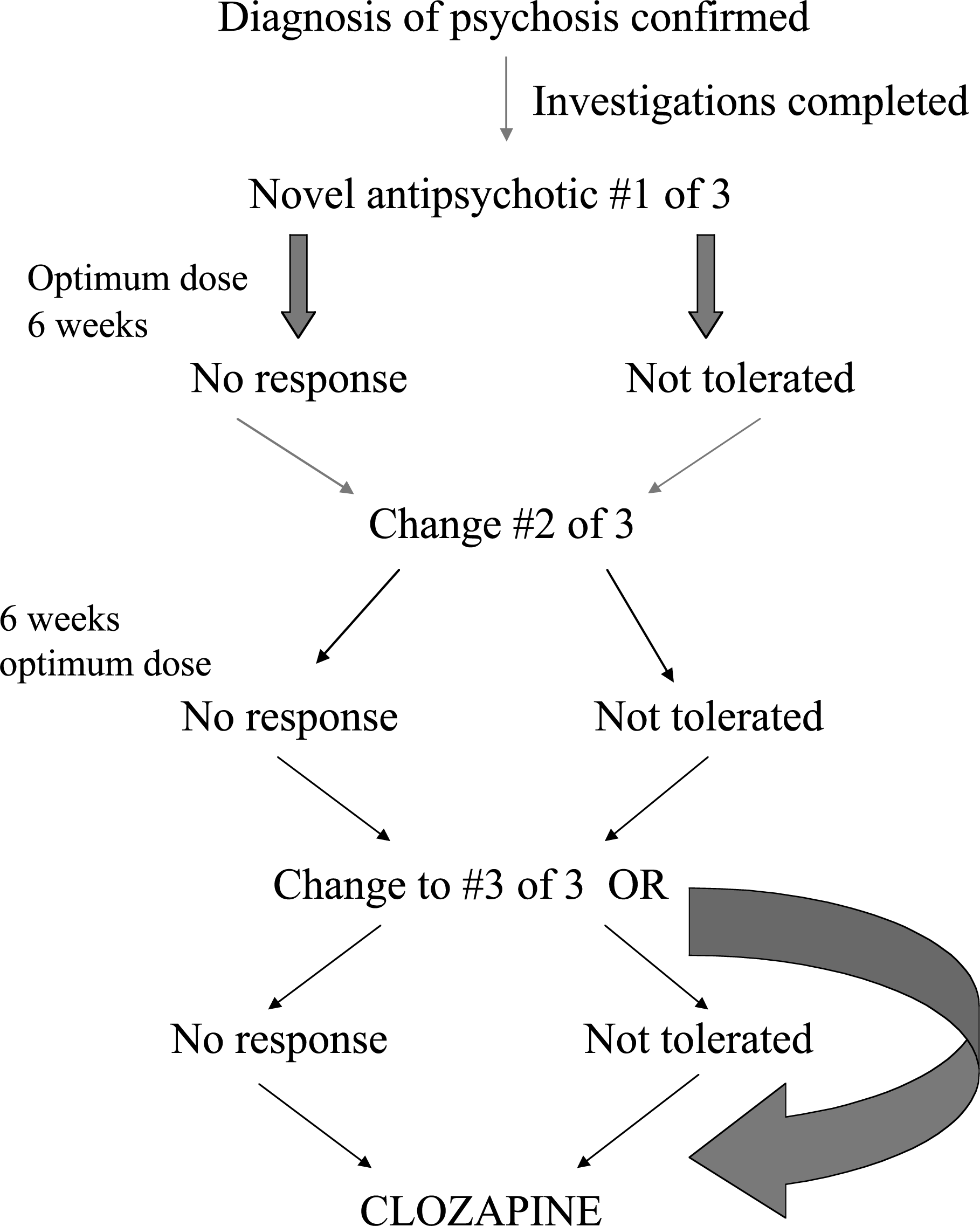
Specific psychosocial interventions
Evaluation
While there is substantial evidence of a relationship between DUP and, at least, short-term outcome, it remains unclear whether the improved outcome reported from early intervention [4] is related to improved treatment specifically designed for this phase of the illness or to intervening early or both. There is some suggestion that phase-specific treatment, if provided within a crucial period following onset of psychosis, produces the greatest benefit [33]. The PEPP project is designed to evaluate the relative effect of assertive community early case detection on 1 and 2 year outcomes as distinct from any improvement achieved through phase-specific treatment. The content of such treatment is being kept constant before and after the introduction of the case detection initiative. Here we will summarize findings from the first phase regarding outcome on clinical, quality of life and cognitive measures, and the impact of the first phase of systemic strategies on rates of treated incidence and reduction in DUP. These findings have been published in greater detail in several papers [34–36].
Sample
Over the first two and a half years a total of 201 patients were assessed and 130 met criteria for a first-episode of psychosis. Of these, 106 (81.5%) completed 1 year of treatment and complete data were available on 88 (68% of total) patients. At the time of initial assessment 60% of these met criteria for schizophrenia spectrum psychosis and 20% psychosis not otherwise specified (NOS) and the rest had diagnosis of affective psychosis (8%), substance-induced psychosis (9.7%) and delusional disorder (2.3%). At 1 year, 81% met criteria for schizophrenia spectrum psychosis, 8% affective psychosis, 6% psychosis NOS and 5% had substanceinduced psychosis or delusional disorder.
Treatment
At 1 year the vast majority (83%) were treated with novel antipsychotics including clozapine (2.4%). Typical antipsychotics (depot) were received by 7.2% of participants; 3.6% were participating in double-blind trial with a novel and a typical antipsychotic and 6% refused to take any medication regularly. The distribution of DUP was positively skewed with a mean of 44 weeks and a median of 22 weeks. Three-quarters of patients were in remission (all SAPS global item scores 2 or <) at 1 year. Of those not in remission, the majority (n = 18) had only moderate positive symptoms (global SAPS item scores 3), and only four showed moderately severe or severe symptoms (SAPS global item scores 4 or 5) at 1 year. Eleven unremitted patients agreed to take clozapine, of which nine responded.
While significant improvement occurred in both positive and negative symptoms, 40% of patients showed no change in negative symptoms compared to 11% for positive symptoms at the end of 1 year. Patients with a DUP of less than 6 months were significantly more likely to remit (83% vs 65%, χ2 3.9, p < 0.05) than those with DUP of greater than 22 weeks (median split). The level of positive symptoms at 1 year was associated with DUP and premorbid adjustment during adolescence which together with length of the prodrome accounted for 14% of explained variance. Negative symptoms were predicted by premorbid adjustment during adolescence, which together with gender and diagnosis of schizophrenia versus other psychoses accounted for 16% of explained variance. Residual symptoms of disorganization were associated with early age of onset, premorbid adjustment during early adolescence, gender and length of prodrome, accounting for 13.5% of explained variance. The lack of association between outcome and childhood adjustment and likely contiguity of adolescent adjustment with prodromal period may suggest a deteriorating process that does not begin until early adolescence. These findings could argue against the significant impact of early neurodevelopment on the course of the illness.
Nearly half of the patients were initially treated as outpatients. The initial venue of treatment did not influence later utilization of inpatient resources during the follow-up period of 1 year. Significant improvements have also been observed in several cognitive domains [37] and indicators of social relations and community functioning after 1 year of treatment [36, 38]. The results reported are comparable to more recent investigations of effectiveness of a phase-specific approach to treating FEP [4, 39] but better than that with traditional approaches [40, 41].
Impact of strategies to reduce delays in treatment
Previous reports have detailed strategies for reducing delays in treatment and their impact on such delays [42]. The first phase of the programme to reduce delay in treatment, involving primarily systemic changes, produced a substantial increase in new cases seen in the second year (from 44 to 62). Based on the number of positive cases identified, PEPP's annual treated incidence rates were 20.8, 30 and 24.7 for 1997, 1998 and 1999 for population at risk (age 16–50). Not withstanding variations in estimation of the yearly incidence of new cases of schizophrenia has been reported to range from 7 to 28 per 100 000 [43]. The rates may be underestimated compared to those in other programmes (e.g. EPPIC) and may reflect exclusion of affective psychosis and criterion of a narrow time frame for exposure to antipsychotic treatment for entry to the programme. There was a significant difference in median DUP over the three years (p = 0.02). From 1997 to 1998 the median DUP decreased slightly from 26.6 to 24.0 weeks, followed by a decrease to 11.6 weeks in 1999 [44]. The second phase of active case detection has been underway for 2 years and data are being collected.
Conclusion
Early intervention in psychosis is gaining momentum in Canada, largely as a result of mounting evidence as well as enthusiasm generated by clinicians, researchers and families. Improved access appears to reduce delay in treatment.