
Abstract
Young male suicide in Australia as recorded by the Australian Bureau of Statistics (ABS) has declined dramatically from its peak in 1998, after steadily increasing for more than 20 years [1]. Rates of young male suicide in those aged 20–34 years increased substantially during the 1980s and 1990s, and peaked in 1998 at approximately 40 per 100 000 before declining to levels not seen since the early 1980s (approx. 20 per 100 000). The reasons for this dramatic decline are as yet unclear, and are made more complex by differential patterns of secular trends in suicide based on area of residence [2,3] and method [1]. For example, male suicide rates declined significantly in higher socioeconomic status (SES) groups but continued to increase in low SES groups [3], and male suicide rates declined in metropolitan and regional areas, but continued to increase in remote areas [2]. Additionally, most of the decline in male suicide has been attributed to decreases in hanging, whereas there have been fewer and smaller changes in secular trends for suicide by other means [1].
There are a number of proposed explanations for this decline in male suicide, such as the effects of national suicide prevention activity (implemented from 1995 just prior to the decline) [1], changes in antidepressant consumption [4], and social and cultural effects of changes to the distribution of wealth in the period after the 1980s [5]. An additional explanation proposed is that part of the observed decline in young male suicide is artefactual, particularly in the most recent period (from 2000), due to an increase in the number of open verdicts by Coroners, which were then coded by the ABS under external cause of death codes relating to ‘unintentional injury’ and other ‘undetermined’ cause of death categories [6–8]. Cases of suicide are likely to have been under-enumerated across jurisdictions in Australia, with potential cases of suicide being allocated to external cause of death categories relating to ‘undetermined intent’ [9–11]. Misallocation in the most recent period following the implementation of the International Classification of Diseases–Edition 10 (ICD-10), however, has been characterized by classifications of likely cases of suicide to unintentional causes of injury, namely accidental hanging and strangulation, unintentional poisoning and unintentional shooting [8]. Based on a detailed comparison of coronial information and ABS mortality data it has been estimated that suicide for the period 2000–2005 is likely to have been under-enumerated by approximately 9%, largely attributable to misclassification of death to the aforementioned unintentional causes [8]. The present study aims to use this reported estimate of under-enumeration and patterns of misclassification by external cause of death to adjust recent trends in young male suicide (20–34 years) and determine the extent to which the recent decline is an artefact of such data misclassification.
Methods
Data
De-identified unit record mortality data were obtained from the ABS for the period 1976–2005 for men aged 20–34 years. Young adult men were selected because this was the demographic group in Australia that experienced an epidemic of suicide over the study period [1]. There was no substantial increase or decline in male adolescents, and suicide rates remained stable in men aged ≥35 years over the same period. Suicide rates in female subjects (young adults, and all ages) showed no increase or decrease in trend over this period [1]. ICD-9 and ICD-10 were used to classify deaths as cases of suicide and self-inflicted injury (ICD codes E950-E959, X60-X84), cases of injury in which the cause of death was undetermined as accidentally or purposely inflicted (E980-E989, E970-E978, Y10-Y36, Y87, Y88), or any external cause (including suicide and undetermined causes; E800-E999, V01-Y98). Cases of undetermined intent also comprised indirect causes of war and de facto executions, and other cases of injury in which sequelae of intentional self-harm were present: additional categories for which suicide has reportedly been misclassified [12]. Additional unintentional cause of death codes were also defined, because a previous investigation of suicide misclassification has noted that in the most recent period (2000–2005) a number of likely suicide cases were classified as accidental hanging and strangulation (E913.1, E913.8, E913.9, W76), unintentional poisoning (E850-E858, E860-E869, X40-X49) and unintentional shooting (E922, W32, W33, W34). Corresponding population counts for men aged 20–34 years for the period 1976–2005 were also obtained from the ABS.
Analysis
Secular trends in young male suicide rates (per 100 000 population) were investigated over the period 1976–2005. Published under-enumeration estimates [8] were used to adjust these suicide rates for the period after 1998 (the peak of the epidemic) to estimate the recent trend in young male suicide after accounting for misallocation of likely suicide cases to unintentional and unknown causes of death (or open verdicts). The period after 1998 was the period of decline in young men, and also the period during which misallocation of likely suicide cases to other external causes reportedly increased (especially 2000–2005) [8]. Much of the decline in young male suicide during this period after 1998 occurred prior to the period (2000–2005) in which reports of a significant increase in the number of open verdicts occurred [7,8]. Prior to 2000–2005 (when the proportion of unknown or open cases was approximately 13% [8]), open verdicts were <5% [7]. Secular trends in young male suicide cases and proportional mortality (of all external causes, ICD codes E800-E999, V01-Y98), by specific means of suicide, other unintentional categories, and undetermined categories were also investigated over the period 1976–2005.
Two scenarios to adjust suicide rates were defined. The first assumed that the reported under-enumeration estimate of 9% for the period 2000–2005 (6–11%) [8] was allocated non-differentially by sex and age (and other demographic factors). For this scenario, young male suicide counts were inflated by 9% for each year after 1998. The range of reported under-enumeration estimates (6–11%) were also presented for this scenario to show likely upper and lower estimates for this scenario.
The second scenario incorporated an estimate of the proportion of likely suicide cases reported in the category of unknown or open cases in addition to likely suicide cases misclassified to unintentional causes of death. The unknown or open cases category included cases for which no information was reported by the ABS, but intentional self-harm was ascribed by the National Coronial Information System (NCIS) [8]. Assuming that the proportion of open cases in the period prior to the peak of the epidemic in 1998 was approximately 5% [7], then the difference between the reported proportion of open cases (13%) in the period 2000–2005 [8] and the period prior to 1998 is 8%. For this scenario young male suicide counts were inflated by 17% (adding misclassified unintentional causes and possible open cases together), with a corresponding range of 15–20% for the 2000–2005 period.
The first scenario described here is perhaps the most realistic adjustment for misallocation of likely suicide cases. It is not clear whether misallocation is non-differential by sex and age across all jurisdictions of Australia for the period under study, although analyses of misallocation in Queensland by sex and age indicate that this is a reasonable assumption [7]. The second scenario assumes that the under-enumeration in suicide due to misallocation to unintentional causes is the same for open cases for which no coronial information was reported, and that the underlying proportion of open cases was 5%. This is a lower estimate of the proportion of open cases in the period prior to 1998, with other studies suggesting a range of 5–10% [11], and so is a likely overestimate of the degree of misal-location of young male suicide, because the proportion of open cases in the earlier period may be higher than 5% [11] and the distribution of suicides in these open cases may not be the same (and perhaps lower) for those misal-located cases for which an unintentional cause was ascribed.
Revised case numbers for each of the aforementioned two scenarios were used to provide two alternative numerators and corresponding 95% confidence intervals based on the Poisson distribution [13] for estimates of suicide rates (per 100 000 population) adjusted for misallocation of cause of death. Differences between observed and adjusted suicide rates were assessed by investigating whether there was overlap of 95% confidence intervals of rates.
Secular trends in proportional mortality investigated trends in those causes of death that were likely to contain misallocated suicides, and also to investigate whether declines in suicide cases were reflected in increases in these other external causes. The majority of likely suicides were misallocated to unintentional poisoning, accidental hanging and strangulation, and unintentional shooting in the period 2000–2005 [8]. Therefore, trends in these unintentional causes were compared with trends in suicide by poisoning, suicide by hanging, and suicide by firearms. Additionally, total mortality rates for the period and mortality due to other external and non-external causes were also examined. While under-enumeration of suicide cases could occur due to misallocation of likely suicide cases to alternative causes of death, the fact of death is unlikely to be under-enumerated in the Australian vital registration system. Misallocation of likely suicide cases to alternative causes should not affect total mortality trends, unless declines in suicide (and possibly other causes) are real and not artefactual.
Results
Recorded male suicide in the 20–34 year age group increased over the study period, peaking in 1998 at 39 per 100 000, before declining sharply in the period 1999–2005 by 44% to 22 per 100 000 in 2005. Following adjustment for misallocation of likely suicide cases to unintentional causes under the first scenario, suicide rates declined 38% to 24 per 100 000 (Figure 1). Adjustment for misallocation of likely suicide cases to unintentional and unknown causes under the second scenario suggested a decline of 33% to 26 per 100 000 (Figure 1). Revised suicide rates under both scenarios did not differ from recorded suicide rates over this period based on 95% confidence intervals, with the exception of suicide rates in 1999–2002 under the assumption of misallocation to both unintentional and unknown causes (Table 1).
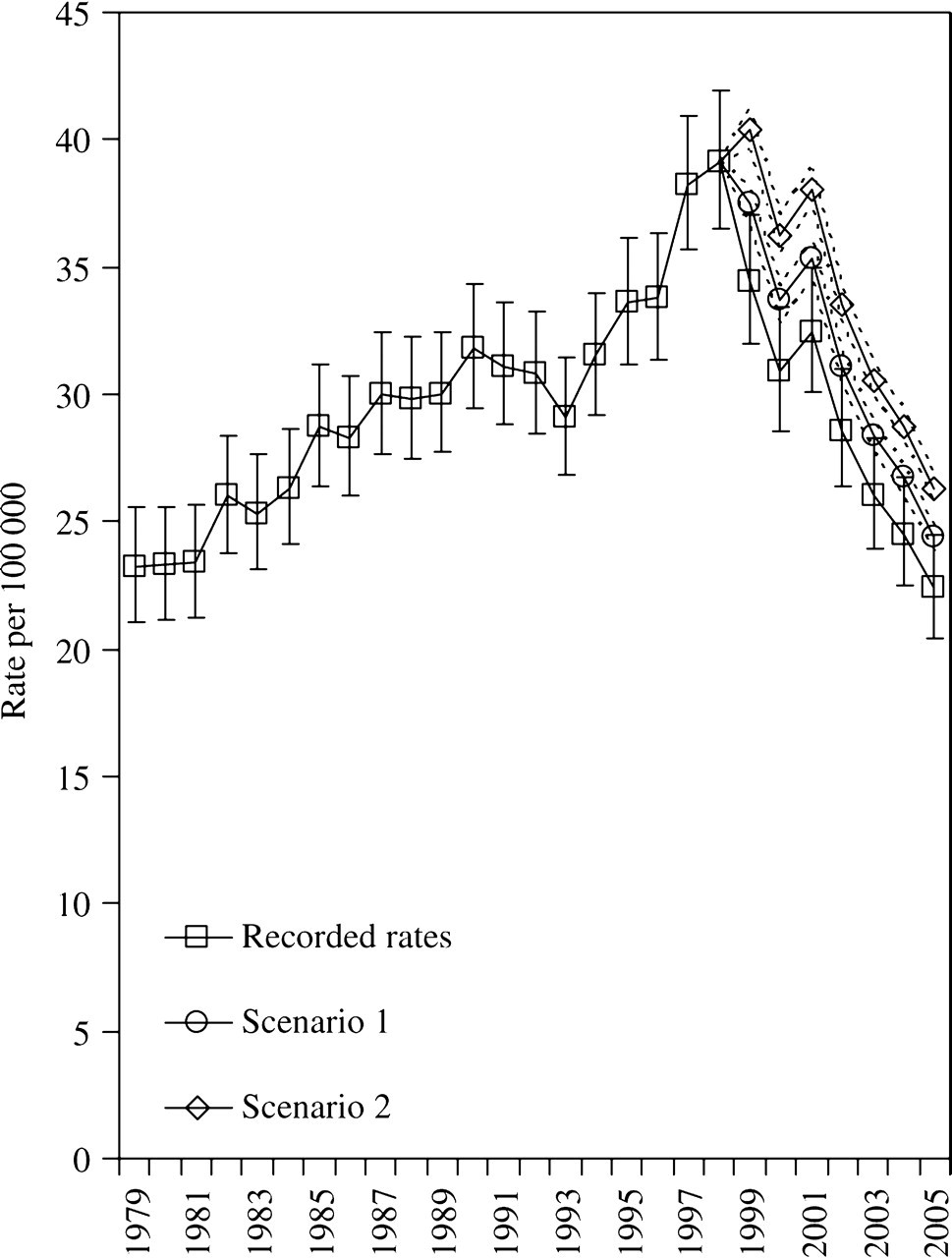
Australian suicide rates in young men (20–34years), variously adjusted for misclassification of likely suicide cases to other external causes (1979–2005). Poisson 95% confidence intervals presented. Recorded rates: suicide rates based on cases reported by Australian Bureau of Statistics (ABS). Scenario 1: suicide rates assuming 9% under-enumeration [8] and non-differential misclassification of likely cases of suicide to other external causes for each year after 1998. Suicide rates based on the reported range of under-enumeration (6–11%) [8]. Scenario 2: suicide rates assuming 17% (range 15–20%) under-enumeration and non-differential misclassification of likely cases of suicide to other external and unknown causes for each year after 1998.
Australian suicide rates in young men (20–34 years), 1997–2005
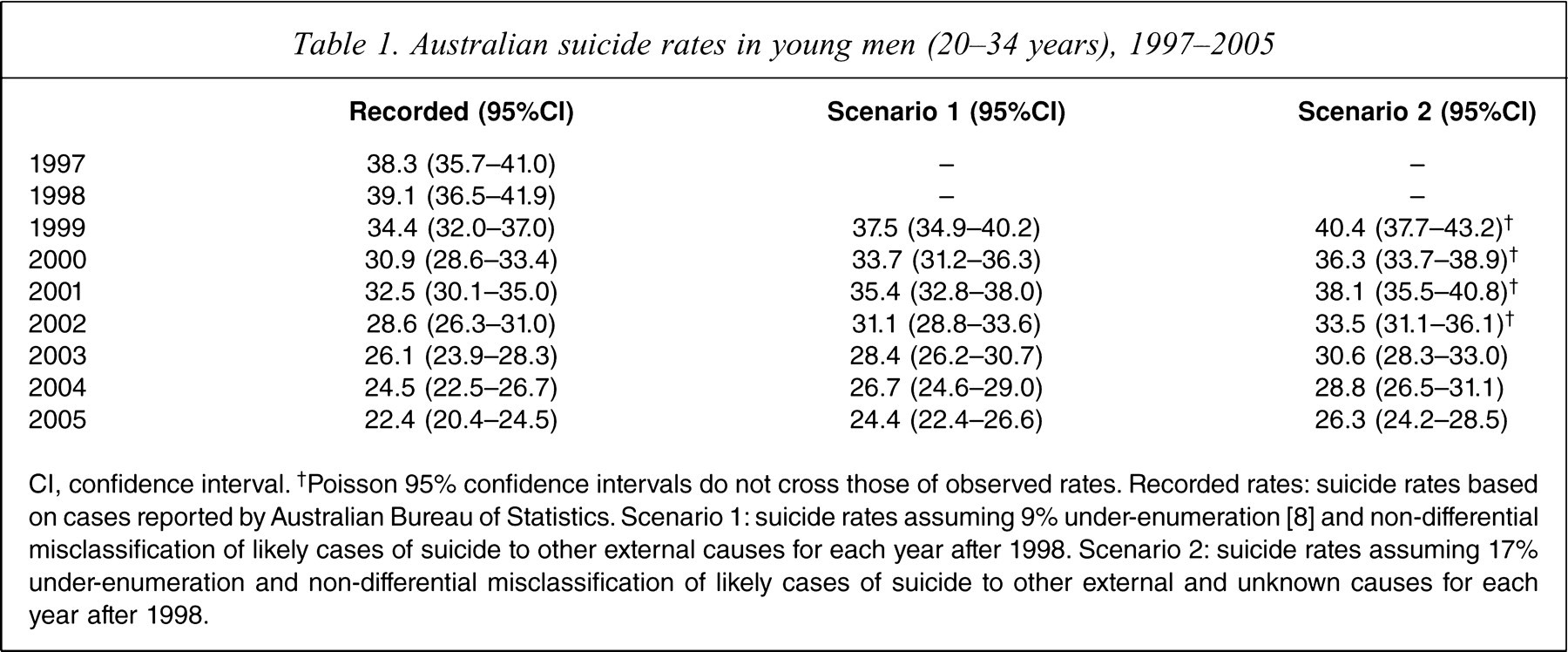
CI, confidence interval. †Poisson 95% confidence intervals do not cross those of observed rates. Recorded rates: suicide rates based on cases reported by Australian Bureau of Statistics. Scenario 1: suicide rates assuming 9% under-enumeration [8] and non-differential misclassification of likely cases of suicide to other external causes for each year after 1998. Scenario 2: suicide rates assuming 17% under-enumeration and non-differential misclassification of likely cases of suicide to other external and unknown causes for each year after 1998.
Proportional mortality of intentional causes show declines in suicide by poisoning and suicide by shooting, which were not reflected in commensurate changes in corresponding unintentional categories (Figure 2). Increases in proportional mortality in ‘accidental hanging and strangulation’ and ‘accident other and unspecified’ increased from approximately 1% in the period 1979–2003 to 5% in the period 2004–2005. It is unclear why there was a sharp increase in unintentional poisoning (1998–2001) with the advent of ICD-10, but this sharp increase is not reflected in a corresponding decline in suicide by poisoning (even though it is likely that part of this decline is attributable to misallocation to unintentional poisoning). The sharp increase in unintentional poisoning was attributable to ‘accidental poisoning by and exposure to narcotics and psychodysleptics’ (X42), and ‘accidental poisoning by and exposure to other and unspecified drugs, medicaments, and biological substances’ (X44). Total mortality for young adult men also declined over the period 1999–2008 largely due to declines in suicide, external causes (other than suicide and motor vehicle accidents), and non-external causes (Figure 3).
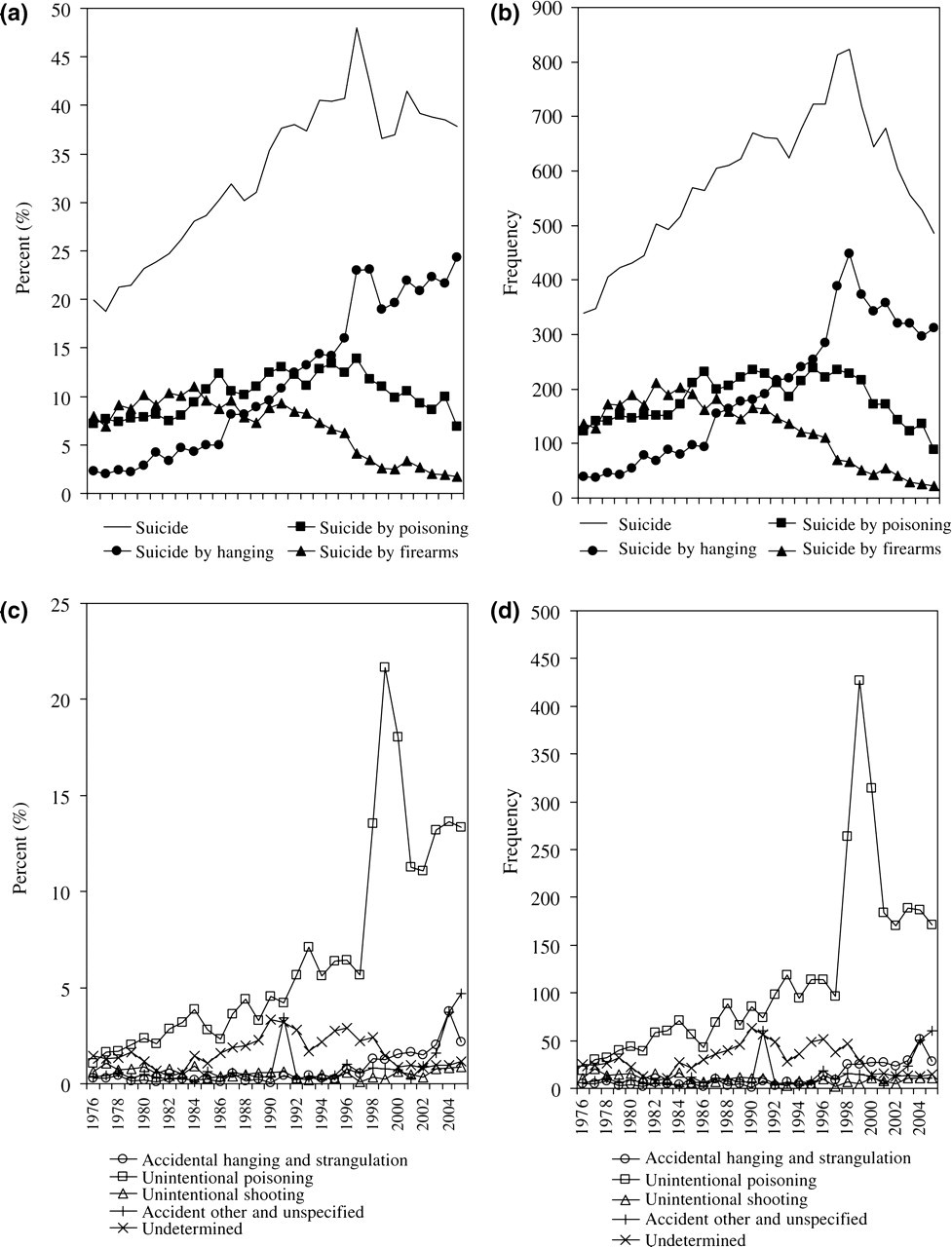
(a) Intentional and (c) unintentional causes of death as a proportion of all external causes; (b) counts of intentional causes of death; and (d) counts of unintentional causes of death for selected external causes, males aged 20–34 years, 1976–2005. Suicide: ICD codes E950–E959, X60–X84. Accidental hanging and strangulation: ICD codes E913.1, E913.8, E913.9, W76. Unintentional poisoning: ICD codes E850–E858, E860–E869, X40–X49. Unintentional shooting: ICD codes E922, W32, W33, W34. Accident other and unspecified: ICD codes E928.8, E928.9, X59. Suicide by poisoning: ICD codes E950–E9520, X60–X69. Suicide by hanging: ICD codes E953, X70. Suicide by firearms: ICD codes E955, X72–X74. Undetermined: ICD codes E980–E989, E970–E978, Y10–Y36, Y87, Y88. External causes: ICD codes E800–E999, V01–Y98.
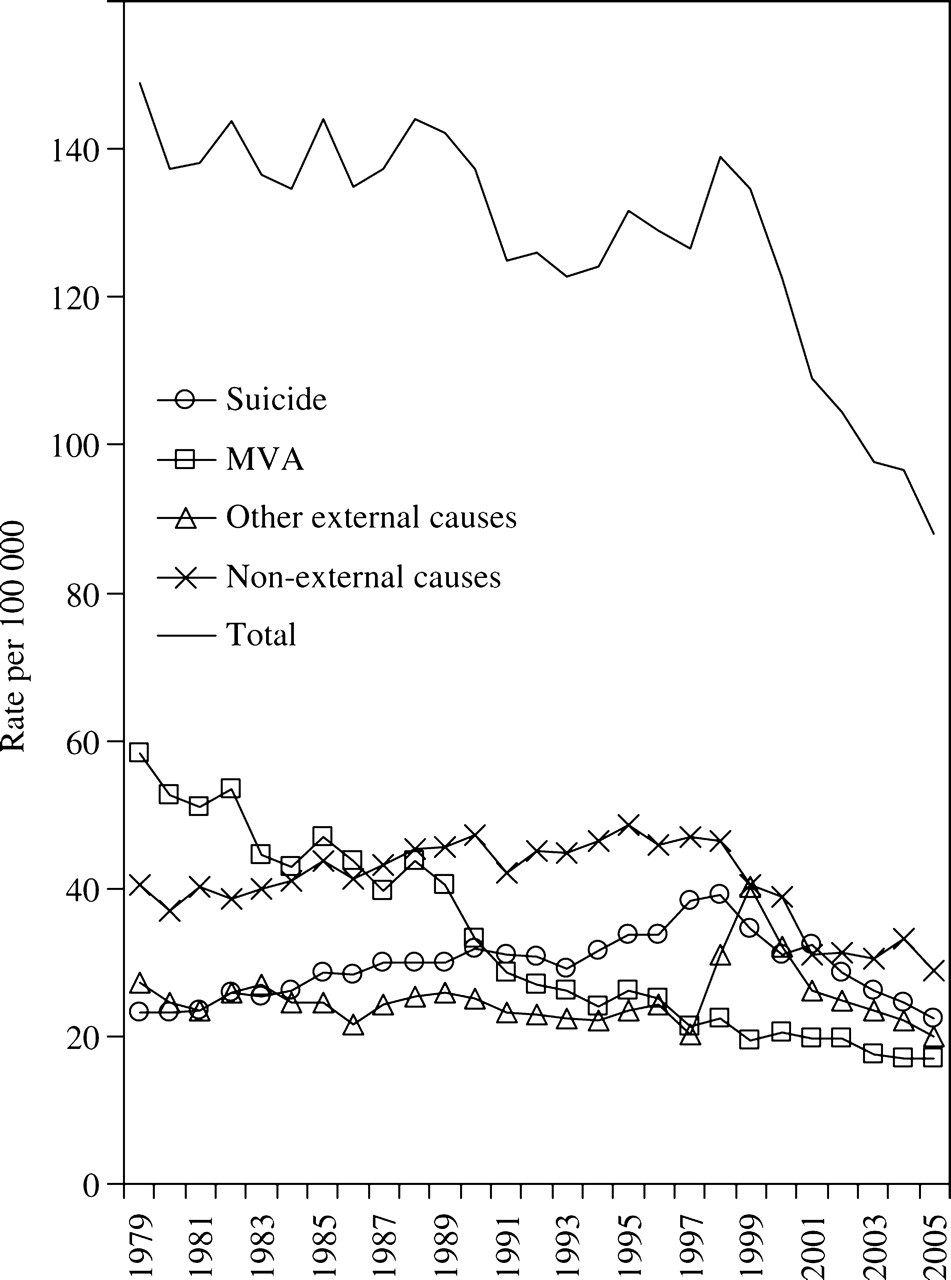
Australian all-cause and selected cause-specific mortality rates in young men (20–34years) (1979–2005). Suicide: ICD codes E950–E959, X60–X84. Motor vehicle accidents (MVA): ICD codes E810–825, E829, V20–V69, V80–V89. External causes: ICD codes E800–E999, V01–Y98.
Discussion
This study confirms that a small part of the apparent marked decline in young male suicide since 1998 can be attributable to under-enumeration of suicide, resulting from the misclassification of likely suicide cases to other external causes of death. The likely effects of this under-enumeration, however, do not substantially change the rate or level of suicide decline previously reported based on routinely available ABS data [1], and is also reflected in declines in total mortality rates, which are not subject to misallocation of cause.
Numerous previous studies, both in Australia and internationally, have indicated that misclassification of cause does occur in the vital registration of suicide [6,9–12,14–18], and that there are likely to be numerous underlying reasons for cases of suicide to be misclassified (such religious or cultural reasons) [12,18]. For example, cross-national comparisons of suicide and undetermined deaths have shown that in some instances, although not all, high rates of undetermined deaths and low rates of suicide occur in predominantly Islamic countries (such as Egypt) where suicide is prohibited [12]. Also, in the USA suicide rates are lower in black people compared to white people, and this differential is significantly reduced after adjusting for suicide misclassification by considering undetermined causes of death [16,18], indicating systematic differences in the classification of suicide by race, but also over-representation of black people in undetermined categories of death in which cases of suicide may be hidden within homicide (e.g. ‘suicide-by-cop’) [18].
In Australia, previous studies of the undetermined death category have shown that suicides are likely to be under-enumerated for males by 5–10% (with lower rates of ‘undetermined’ cases in European migrants) [11], and that the use of the undetermined category did not change substantially during the period of the emerging youth suicide epidemic [9,10]. More recent investigations focusing on the period (2000–2005) after the implementation of the ICD-10 have found that suicide is likely to be under-enumerated by 9%, and that this period is characterized by misclassifications of likely cases of suicide to unintentional causes of injury, namely accidental hanging and strangulation, unintentional poisoning and unintentional shooting [8]. As shown in the present study, however, it is unlikely that this under-enumeration is of a magnitude to wholly account for the recent marked decline in suicide [6,7].
For artefactual changes in suicide enumeration to account for the substantial decline in male suicide since 1998, a number of alternative explanations would need to be discounted. It is of note that much of the decline in young male suicide occurred prior to the period when reports of a significant increase in the number of open verdicts occurred (2004–2006) [7]. Prior to this period open verdicts were <5% [7]. An additional consideration is that most of the decline in the period after 1998 occurred due to declines in hanging [1], a method less likely to result in an open verdict from a Coroner than other more equivocal methods, such as poisoning and drowning [10,18], and a method that has not declined as a proportion of all external causes (Figure 2). Finally, it could be argued that misclassification of likely suicide cases to other external causes would be non-differential across jurisdictions, by sex and age, and other sociodemographic strata. The decline in suicide, however, has occurred differentially in different socioeconomic groups [3] and in different geographic areas [2] – associations that generally accord with previously validated and sociologically plausible distal antecedents to suicide.
Valid and reliable vital registration of suicide is integral to monitoring the effects of suicide prevention activity, mental health policy, and broader social and cultural phenomena on secular suicide trends, and researchers and governments alike must work jointly to improve emerging problems of data quality as they relate to suicide [6]. To overemphasize the artefactual dimension of the recent decline in male suicide is a distraction to developing an understanding of other more pertinent reasons for what has been real and significant suicide decline, and to disentangling the effects of recent prevention activity and other sociocultural factors on distal, intermediate and proximate factors associated with Australian suicide.
Footnotes
Acknowledgements