
Abstract
Rates of suicide among young males aged 15–24 years in New Zealand (40.9 per 100 000, in 1997) [1], and Australia (31 per 100 000 in 1997) [2] are consistently among the highest for a series of selected developed countries [3]. These international comparisons have led to growing concerns about the issue of youth suicide in Australia and New Zealand, and to consideration of how these recent increases might be arrested [4,5].
One approach to reducing suicide lies in restricting access to specific methods of suicide. The view that suicide risks may be reduced through restricting population access to methods of suicide has a long history that dates from Durkheim's 1897 observation of extensive local and national differences in the methods of suicide [6]. The idea that suicides may be prevented by restricting access to specific means is intuitively appealing and links suicide prevention to other public health initiatives in the area of injury prevention (see, for example [7]). Nonetheless, the prevention of suicide raises more complex issues than does the prevention of unintentional injury since suicide is a purposive act.
The purposive nature of suicide means that restricting population access to one method of suicide may lead to the substitution of other methods. The issue of method substitution has been contentious in the suicide prevention literature, with some studies suggesting the presence of substitution effects whereas others have not [8–13]. Perhaps the best conclusion that may be drawn is that the elimination of a specific method of suicide from a given population does not invariably or reliably lead to a corresponding reduction in overall suicide rates, although it may lead to a reduction in the rate of suicide by that method.
Despite these difficulties, international approaches to suicide prevention place strong emphasis on restricting access to means of suicide. For example, restricting access to means of suicide is a strategy which is included in all national suicide prevention programs [14], and four of the six basic steps for the prevention of suicide recommended by the World Health Organization (WHO) are based upon restricting access to means of suicide (guns possession control, detoxification of domestic gas, detoxification of car emissions, control of toxic substances availability) [15].
Against this background, this paper examines the trends in methods of youth suicide in New Zealand over a 20-year period from 1977 to 1996. The specific aims of this analysis include: (i) to review trends in youth suicide in New Zealand from 1977 to 1996; (ii) to document contemporary methods of suicide in 1996; (iii) to examine changes in the use of specific methods of suicide during the 20-year period from 1977 to 1996; and (iv) to consider the potential role of method restriction in youth suicide prevention in New Zealand given contemporary trends in methods of youth suicide.
Method
Data sources
Data on numbers of deaths and methods of suicide for the population of young people aged 15–24 years were provided by the New Zealand Health Information Service (NZHIS) from mortality data collected and published annually by the Ministry of Health for the years 1977–96.
Data classification
The deaths selected for this review were those deaths which occurred in New Zealand during the period 1977–96 which met the following criteria: (i) they received coroners' verdicts of suicide according to the Coroner's Act 1988; and (ii) they were coded according to the International Classification of Disease (ICD) Codes E950-E959, suicide and self-inflicted injury [16].
Results
Trends in youth suicide, 1977–96
To provide a background to the analysis of trends in youth suicide methods, Fig. 1 gives suicide rates for males and females, aged 15–24 years, for the 1977–96 period. During this time, there were markedly different suicide patterns for males and females. Male suicide rates increased steadily from 20.3 per 100 000 in 1977 to 39.5 per 100 000 in 1996.
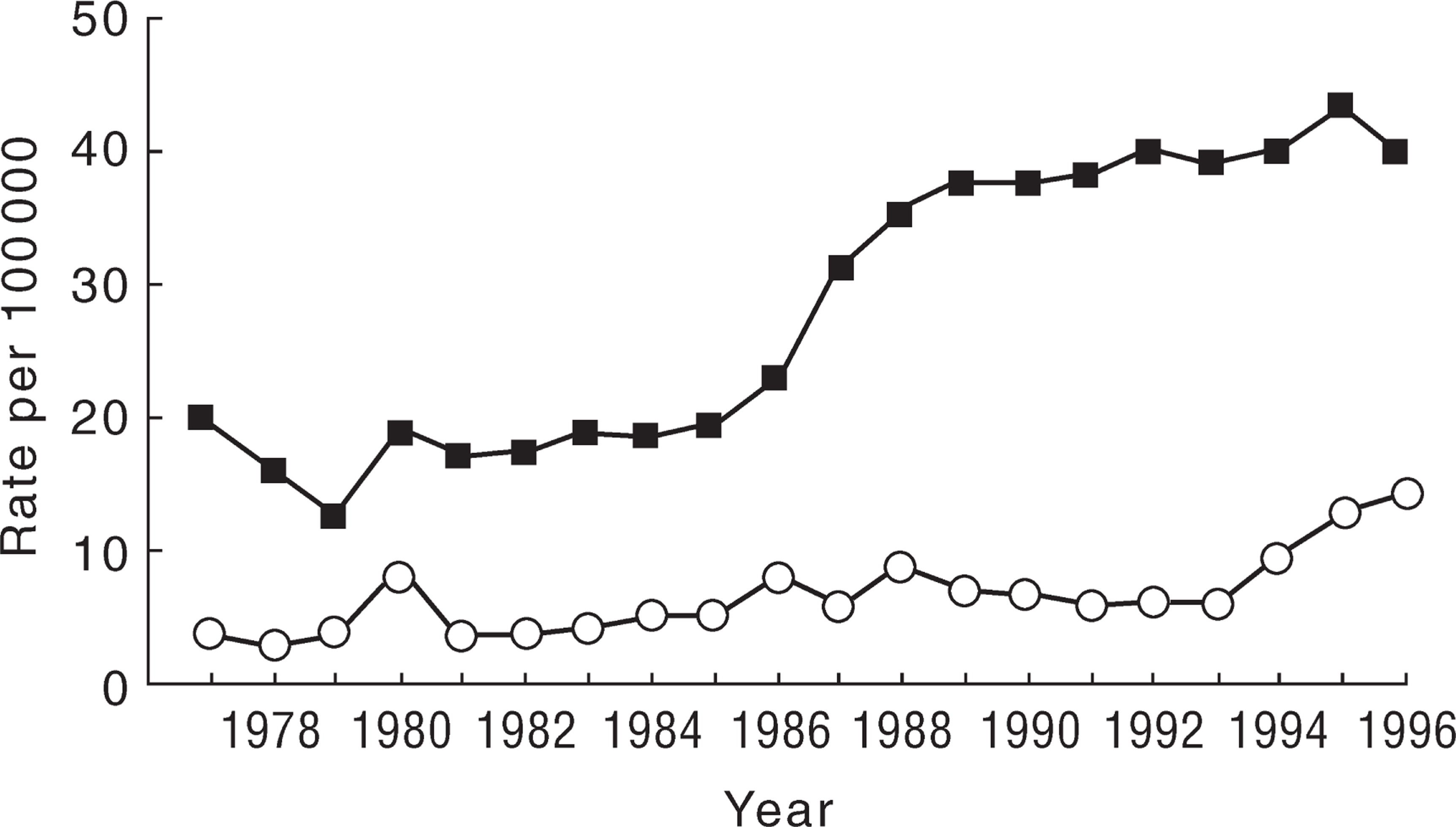
Annual suicide rates (ICD E950-E959), by gender, for young people aged 15–24 years in New Zealand 1977–96. ▪, male; □, female.
By contrast, female suicide rates remained consistently lower and more stable than male rates. Nevertheless, female suicide rates also rose substantially during this time, from 4 per 100 000 in 1977 to 14.3 per 100 000 in 1996, with much of this increase occurring recently, from 1994 to 1996.
Methods of youth suicide, 1996
To provide contemporary data, Table 1 shows methods of suicide in 1996 (the year for which these data are most recently available), for males and females aged 15–24 years and for the total population of young people.
Suicide deaths by method by gender for young people 15–24 years in New Zealand 1996
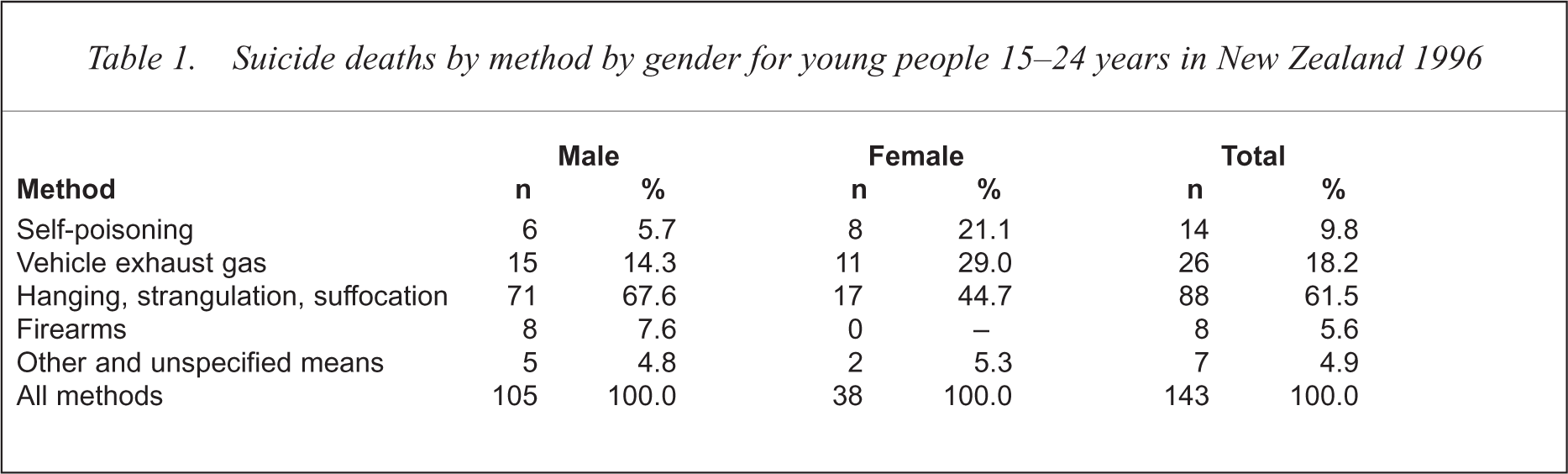
Overwhelmingly, the major method of youth suicide in 1996 was hanging (accounting for 67.6% of male deaths, 44.7% of female deaths and 61.5% of all youth deaths). The second most common method was vehicle exhaust gas. This method accounted for 14.3% of youth male deaths, 29% of youth female deaths and 18.2% of all youth suicides. Hanging and vehicle exhaust gas accounted for almost 80% of all youth suicides, with other methods making relatively minor contributions. Self-poisoning constituted a larger proportion of suicides among females (21.1%) compared with males (5.7%) and accounted for a larger fraction of all suicides (9.8%) than firearms (5.6%). While firearm deaths accounted for 7.6% of male youth suicides, no females used this method.
Trends in methods of youth suicide, 1977–96
Table 2 examines changes in methods of youth suicide, for males and females in New Zealand from 1977 to 1996. As the population in New Zealand is small, the number of suicides in each method category can be very small (particularly for female suicides). For this reason, the table compares the 5-year average suicide rates for each major method of suicide, for the two quinquennial periods, 1977–81, and 1992–96. These data groupings permit a more reliable examination of trends in the use of specific methods of suicide. The table also shows, for males and females, the contribution of specific methods of suicide to the increased rate of overall suicide observed during this time, with this contribution expressed as a percentage of the change in the overall suicide rate (from all methods).
Trends in methods of suicide among young people aged 15–24 years, by gender in New Zealand 1977–96
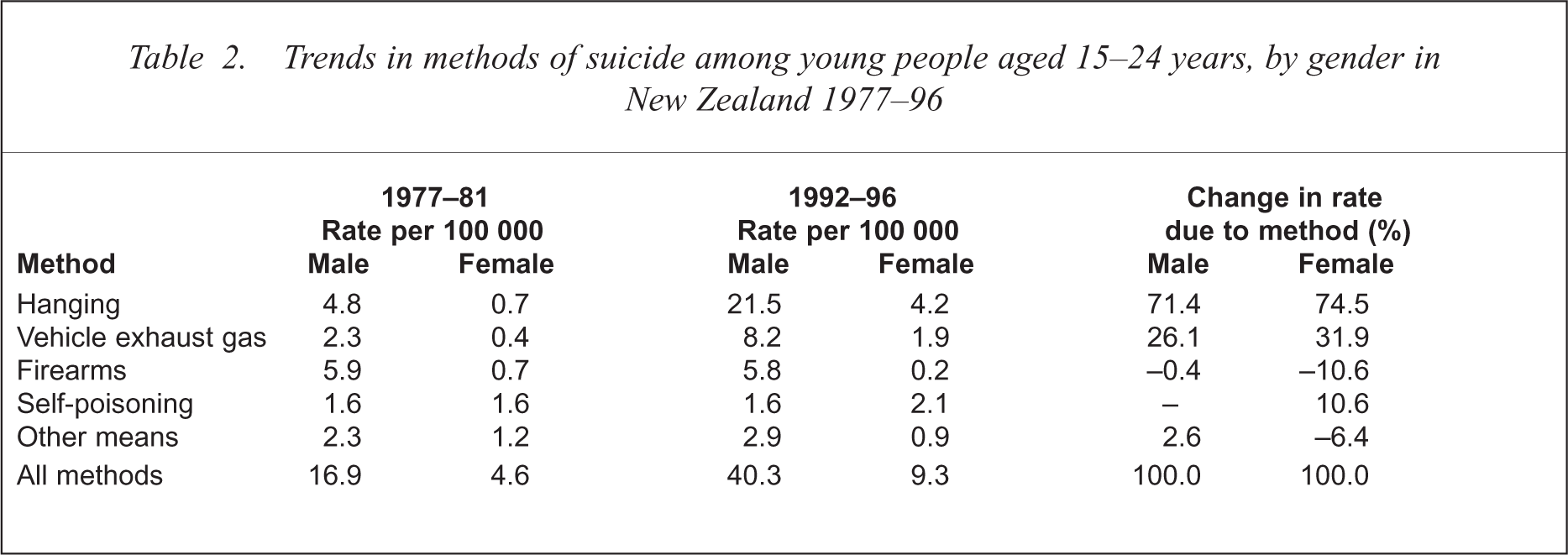
The overall rate of suicide among males aged 15–24 years increased from 16.9 per 100 000 for the 5-year period 1977–81 to 40.3 per 100 000 for the 5-year interval 1992–96. The increased rate of male youth suicide during this time was accounted for, substantially, by the increased rate of hanging (71.4% of total increase) and, to a lesser extent, by the increased rate of suicide by vehicle exhaust gas (26.1% of total increase). Other methods of suicide made negligible contributions to the increased suicide rate. Specifically, there was an insignificant decrease in the use of firearms (–0.4%) and an insignificant change in the use of other, infrequently used methods, including drowning and jumping from a high place (2.6%).
During the same period, the corresponding rate of suicide among females increased from 4.6 per 100 000 to 9.3 per 100 000. While the rise in the rate of female suicide was less marked than the rise in the male rate of suicide, it was accounted for by similar increases in the rates of hanging (74.5%) and vehicle exhaust gas deaths (31.9%). A small decrease in the rate of firearm suicides (10.6%) was offset by an increase in the rate of self-poisoning (10.6%).
Discussion
This analysis has examined trends in youth suicide and methods of youth suicide over a 20-year period from 1977 to 1996. The principal foci of the analysis were upon: (i) documenting methods used in contemporary youth suicide in New Zealand; (ii) documenting changes in youth suicide rates over the 20-year period from 1977 to 1996; and (iii) identifying the contributions of various methods to changing rates of youth suicide. The findings of the study and their implications for suicide prevention by method restriction are reviewed below.
Over the 20-year period studied, New Zealand has experienced substantial increases in rates of both male and female youth suicide with these trends being more marked for male suicides. These increases were shown to be almost wholly attributable to the increased use of two methods of suicide. First, the increase in deaths by hanging accounted for over 70% of the overall increase in suicide rates between 1977 and 1996 for both males and females. Second, the increase in suicide by vehicle exhaust gas accounted for over 25% of the increased suicide rate among males and almost one-third of the increased suicide rate among females.
The net results of these trends was that, in recent years, almost 80% of youth suicides in New Zealand have arisen from just two methods: hanging and vehicle exhaust gas.
These observations provide a context within which to consider the potential for reducing New Zealand youth suicide rates by restrictions of access to various methods of suicide. The following conclusions may be drawn.
First and foremost, it is clear that the high rate of suicide by hanging places considerable limitations on the extent to which youth suicide rates may be reduced through method restrictions. As a number of authors have pointed out, there is no realistic or feasible public health policy by which population access to means of hanging might be restricted [17–22]. The only possible exception to this may be in institutional settings, including prisons, police custody cells and psychiatric hospitals. In particular, there have been persistent suggestions that by structural modifications to ‘suicide proof’ cells, secure and seclusion areas, it may be possible to reduce the number of deaths by suicide among those who are admitted to such institutions [19,23–29]. However, since suicides which occur in institutional settings constitute a very small proportion of all youth suicides, even if it were possible to eliminate all institutional hangings, the impact on total suicide rates would be almost infinitesimally small.
After hanging, carbon monoxide poisoning by vehicle exhaust gas is the second most common method of suicide among New Zealand youth. Given the significant contribution of vehicle exhaust gas to overall suicide rates, proposals to reduce rates of suicide by limiting access to vehicle exhaust gas are appealing.
The role of vehicle exhaust gas in suicide has lead to speculation about the possibility of reducing suicide rates through the detoxification of vehicle exhaust emissions. This may be achieved though the fitting of catalytic converters that purify exhaust emissions and remove noxious emissions including carbon monoxide. Related suggestions have included: (i) the simpler approach of modifying exhaust pipes in ways which make the capture of exhaust gases for the purpose of suicide difficult, particularly by preventing the attachment of hoses (commonly used in suicide attempts); (ii) the development of carbon monoxide sensors in vehicles which would sound an alarm when potentially toxic levels of carbon monoxide were detected; and (iii) the use of an automatic idling device which would stop the engine after a maximum idling time [30–32].
While all four approaches, in theory, would reduce access to vehicle emissions as a means of suicide, research into the likely efficacy of these moves is, as yet, relatively limited and there are equivocal findings from studies which have examined the impact of imposing controls on carbon monoxide emissions from vehicles by the use of catalytic converters, with some countries reporting reductions in overall suicide rates and others failing to find this effect [8,33,34].
In addition, there are some features of the New Zealand context which might limit the implementation of this approach. In particular, the New Zealand transport fleet is composed entirely of imported vehicle technology, with Japan providing the predominant source of importation. The lack of a local car industry and the importation of the vehicle fleet would appear to pose barriers to the widespread or swift implementation of the use of catalytic converters.
In New Zealand, the Ministry of Transport is currently developing a Vehicle Fleet Emissions Control Strategy to improve air quality. A draft report of the strategy suggests that the final policy recommendations to government will not include the imposition of (mandatory) emissions standards [35]. Rather, it seems that, in this area, the Strategy will rely on the fact that importation of vehicles from overseas countries which have imposed such emission controls will gradually change the profile of the New Zealand vehicle fleet, so that, over time, an increasing proportion of vehicles will have catalytic converters. However, the current age of the New Zealand vehicle fleet (9 years) suggests that the lag time before a high proportion of cars owned by both the general population and the population of young males (who tend to own older cars) are fitted with such devices may be of the order of many years.
It seems likely, therefore, that if emission controls are to be introduced to New Zealand, this will follow from moves in other countries to install catalytic converters in vehicles for principally environmental reasons, rather than for the primary purpose of reducing suicide rates.
An issue which has had a high profile in debates about suicide prevention in New Zealand has been firearms restrictions, with a number of authors arguing that restricting access to firearms in New Zealand may lead to reductions to the overall suicide rate [36,37]. These conclusions are clearly not supported by the present analysis which suggests that suicide by firearms has been declining in the last 5 years and this method now accounts for only 7.6% of male youth suicides and 5.6% of all youth suicides. These figures suggest that, even if all young people were prevented from having any access to firearms the consequence to overall suicide rates would be relatively small. This conclusion has also been confirmed by case–control research of the effects of access to firearms on suicidal behaviour, which has suggested that access to a firearm was not associated with significant increases in risk of death by suicide [38].
These figures stand in marked contrast to results from other countries where research has suggested that firearms are the most commonly used method of youth suicide, and that restriction of access to firearms could, in theory, make very substantial contributions to reducing rates of youth suicide [7,39]. This comparison underlines the well-documented fact that method choices in suicide behaviour tend to be highly culturally specific and that method-restrictive strategies which may be effective in one social context may be ineffective in another.
While self-poisoning makes a relatively small contribution to overall rates of youth suicide, this method still accounts for one in five young female suicides and, more importantly, accounts for the overwhelming majority of hospitalisations for (non-fatal) suicide attempts among youth [40]. For these reasons there may be considerable scope to reduce rates of hospitalisation, and, to a far smaller extent, rates of youth suicide, by restricting access to a range of drugs, including, in particular, paracetamol, which are toxic or lethal in overdose. A range of recommendations in this area include, for example: limiting the size of prescriptions; elimination of automatic refills of prescriptions; blister packaging, in preference to loose packaging; given equivalence of effect, encouraging prescription of drugs which are less toxic in overdose; reducing prescription charges (to encourage smaller scripts); regular amnesty, or other means of encouraging return of out-of-date or unused medications [19,41–46].
In summary, the dominant role of hanging and vehicle exhaust gas in youth suicide in New Zealand imposes severe limitations on the potential for method restriction to reduce rates of youth suicide. However, while the potential for reducing youth suicide by method restriction appears to be limited, this argument does not imply that best practice methods should not be developed to restrict access to means of suicide wherever this is possible. For example, although Beautrais et al. found that access to firearms made only a relatively small contribution to death by suicide, they nonetheless noted that prudent restriction of access to firearms may prevent a minority of impulsive suicide attempts, made in situations of extreme anger or distress, in which the availability of a firearm may have had tragic consequences [36].
This conclusion notwithstanding, the results of this analysis clearly suggest that the potential for making major inroads on New Zealand's increased youth suicide rates through method restriction is extremely limited and, accordingly, that major policy efforts need to be directed toward addressing the underlying risk factors, life processes and associated causes that lead individuals to take, or attempt to take, their lives, rather than focusing upon denying these young people access to methods of suicide.
Acknowledgement
This report was commissioned, in part, by the Ministry of Health, New Zealand, as part of the New Zealand Youth Suicide Prevention Strategy.