
Abstract
Objective:
We investigated recent trends in youth suicide and their associations with societal and psychological factors in Taiwan.
Methods:
Suicide data (1971–2019) for 10–24 year olds were extracted from Taiwan’s national cause-of-death data files. We investigated changes in trends in youth suicide rates, societal factors (gross domestic product per capita, Gini index, overall and youth unemployment rates, divorce rates in people aged 40–59 years [i.e. the age of most 15–24 year olds’ parents] and Internet use rates) and psychological distress indicators (youth self-harm rates and the prevalence of worry-related insomnia, and suicide ideation, plan and attempt) using joinpoint regression and graphic examinations. The associations of these factors with youth suicide rates were examined using Prais–Winsten regression.
Results:
Suicide rates in Taiwan’s 10–24 year olds changed from a downward trend (2005–2014) to an upward trend in 2014 and increased 11.5% (95% confidence interval = [5.2%, 18.1%]) annually between 2014 and 2019. There was also an upturn in divorce rates among females aged 40–59 years in 2014 and self-harm rates among 15- to 24-year-old youth in 2013. The prevalence of self-reported insomnia and suicide ideation, plan and attempt in youth started to increase from 2013 to 2016. In the regression analysis, Internet use, female divorce rates and youth self-harm rates were positively associated with youth suicide rates.
Conclusion:
Suicide rates and the prevalence of suicidal behaviors began to increase in Taiwanese youth in the 2010s. These increases may be associated with concurrent rises in parental divorce rates, Internet use and poor sleep. Further research is needed to examine the mechanisms underlying recent increases in youth suicide risk.
Introduction
Suicide is a potentially preventable public health priority. The urgency to act to reduce suicide rates is well recognized. The UN Sustainable Development Goals (SDGs) include an indicator (3.4.2) to reduce suicide by a third by 2030 (United Nations Statistics Division, 2021). Suicide remains the second leading cause of death among young people worldwide (World Health Organization, 2019b). It is estimated that over 150,000 10–24 year olds die by suicide each year globally, accounting for 19% of overall suicide deaths (World Health Organization, 2018).
A worrisome recent rise in youth suicide has occurred in several high-income countries including Australia, Canada, the United States, the United Kingdom and Taiwan (Chang et al., 2020; Padmanathan et al., 2020). For example, in Australia, suicide rates for the 15–19 and 20–24 age groups increased 43% and 39% in 2019 when compared to 2010, respectively (Australian Bureau of Statistics, 2021). In the United States, suicide rates among those aged 10–24 increased nearly 60% between 2007 and 2018 (Curtin, 2020). In Taiwan, suicide rates among youth under 25 years of age increased 84% in 2019 when compared to 2013 (Ministry of Health and Welfare, 2020).
Youth suicidal behavior is a complex issue associated with a multitude of risk factors (Hawton et al., 2012). However, it is not yet clear how changes in these factors may have influenced recent trends in youth suicide rates. A recent study of the 11 most populous high-income countries showed that the recent rises in youth suicide rates were seen in countries with higher gross domestic product (GDP) per capita and income inequality in 2008 (Padmanathan et al., 2020). In some countries such as Australia and the United Kingdom, the recent rises in youth suicide occurred in parallel with unfavorable trends in other population mental health indicators among youth such as the prevalence of psychological distress, common mental disorder and non-suicidal self-harm (Fink et al., 2015; Jorm and Kitchener, 2021; McManus and Gunnell, 2020; Pitchforth et al., 2019). Increased levels of distress reported by adolescents have been found to be associated with a range of factors, such as the 2008 global financial crisis and increased levels of social media use, cyberbullying, academic pressures, family breakdown and concerns about financial security (Gunnell et al., 2018). In Taiwan, a recent study investigating time trends in age-specific suicide rates across all age groups showed an increase in youth suicide rates in the 2010s; the authors hypothesized that such an increase may be associated with unfavorable trends in potential risk factors (e.g. Internet use and adult divorce rates) and several psychological distress indicators (e.g. the prevalence of youth suicide ideation, plan and attempt) and called for more research on this topic (Chang et al., 2020). To the best of our knowledge, there have been no previous studies investigating the associations between recent trends in youth suicide and a comprehensive set of potential risk factors.
This study aimed to investigate recent trends in youth suicide rates and their associations with the trends in a range of potential societal factors and psychological distress indicators in Taiwan. We hypothesized that (1) there were unfavorable recent trends in some societal factors and psychological distress indicators, and such changes occurred closely in time with the upturn in youth suicide rates; and (2) the year-on-year changes in the level of societal factors and psychological distress indicators were associated with the changes in youth suicide rates.
Methods
Suicide data
Suicide data for 10–24 year olds between 1971 and 2019 were extracted from the computerized national cause-of-death mortality data files. International Classification of Disease (ICD) codes, Eighth (ICD-8), Ninth (ICD-9) and Tenth (ICD-10) Revisions, were used to identify suicide (ICD-8 and ICD-9 E950-E959; ICD-10 X60-X84). Past research from Taiwan indicated that many suicides were likely to be misclassified as undetermined deaths (ICD-8 and ICD-9 E980-E989; ICD-10 Y10-Y34), accidental pesticide poisonings (ICD-8 E865; ICD-9 E863; ICD-10 X48) or accidental suffocations (ICD-8 and ICD-9 E913; ICD-10 W75-W76, W83-W84) (Chang et al., 2010); therefore, deaths in these cause-of-death categories were included in the analysis. Annual population data during the study period were obtained from the Statistical Yearbooks provided by the Department of Household Registration, Ministry of Interior (2021).
Potential societal risk factors
Data for GDP per capita between 2000 and 2019 were obtained from the website of National Statistics (https://nstatdb.dgbas.gov.tw/dgbasAll/webMain.aspx?sys=100&funid=dgmaind&mp=4). Gini index data between 2000 and 2019 were obtained from the annual reports of the Survey of Family Income and Expenditure published by the Executive Yuan (www.stat.gov.tw/ct.asp?xItem=19882&CtNode=512&mp=4). Data of unemployment rates in people aged 15+ years and youth aged 15–24 years between 2000 and 2019 were extracted from the Manpower Survey Statistics (www.stat.gov.tw/ct.asp?xItem=41085&ctNode=518&mp=4) to reflect the labor market situation in the population and more specifically in young people, respectively. Divorce rates per 1000 married individuals were obtained from the website of the Ministry of the Interior, Taiwan (Ministry of Interior, 2021); sex-specific divorce rates in 40–59 year olds, the age of most 15–24 year olds’ parents, were used in the analysis. Internet use rates (the percentage of individuals who used Internet in the past 6 months) were obtained from the Taiwan Network Information Centre (TWNIC) (Taiwan Network Information Center, 2019). TWNIC conducted national surveys on Internet use among people aged 12 years and above using telephone interviews annually from 2006. Participants were asked if they ever used Internet and if they ever used Internet through mobile devices in the past 6 months.
Psychological distress indicators
Self-harm episodes in youth were extracted from the annual reports published by the Department of Mental and Oral Health, Taiwan Ministry of Health and Welfare (https://dep.mohw.gov.tw/domhaoh/cp-4904-8883-107.html). The data for self-harm episodes were from Taiwan’s National Suicide Surveillance System (NSSS). Details of the surveillance system were described elsewhere (Pan et al., 2013). In brief, all self-harm episodes (regardless of suicide intent) presenting to emergency departments, the police, firefighters, school and other governmental agencies were reported to the NSSS since its establishment in 2006. Individuals’ basic demographic information (e.g. sex and age), contact address, and the date and method of the self-harm events were uploaded onto the system. Overall and sex-specific rates of self-harm episodes per 100,000 youth aged 0–14 and 15–24 years were calculated.
Data for the prevalence of self-reported worry-related insomnia and suicide ideation, plan and attempt in young people were extracted from the 2012–2018 Taiwan Youth Health Survey (TYHS) reports (www.hpa.gov.tw/Pages/TopicList.aspx?nodeid=257). The TYHS was conducted by the Health Promotion Administration, Taiwan Ministry of Health and Welfare from 2006. The Administration started to collaborate with the US Centers for Disease Control and Prevention (CDC) and included the TYHS as part of the Global School-based Student Health Survey (GSHS) from 2012; meanwhile, the questionnaires were revised and the core modules (e.g. mental health) from the GSHS were added. Details of the GSHS were described elsewhere (www.cdc.gov/gshs/index.htm). In brief, the GSHS is a school-based survey conducted primarily among students aged 13–17 years. In the Taiwanese surveys, a two-stage cluster sampling design was used to recruit a representative sample of middle and high school students (Health Promotion Administration, Ministry of Health and Welfare, 2015). The surveys were conducted biennially in middle schools in 2012, 2014, 2016 and 2018 (four waves) and in high schools in 2013, 2015 and 2017 (three waves).
The prevalence of self-reported worry-related insomnia referred to the weighted percentage of students who answered ‘often’ or ‘always’ to the question ‘during the past 12 months, how often have you been so worried about something that you could not sleep at night?’ Suicide ideation was assessed using the question ‘during the past 12 months, did you ever seriously consider attempting suicide?’ Suicide plan was assessed using the question ‘during the past 12 months, did you make a plan about how you would attempt suicide?’ Suicide attempt was assessed using the question ‘during the past 12 months, how many times did you actually attempt suicide?’ Those who reported one or more suicide attempts were classified as having attempted suicide.
Statistical analysis
Annual overall and sex-specific suicide rates per 100,000 were calculated among individuals aged 10–24 years in 1971–2019; for the period 2000–2019, sex-specific suicide rates were also calculated among those aged 10–14, 15–19 and 20–24 years, corresponding to the early, middle and late adolescence periods (Sawyer et al., 2012), respectively, to investigate age difference.
Trends in suicide rates, potential societal risk factors and youth self-harm rates were investigated using joinpoint regression analysis. The analysis compares a series of joined line segments to identify the combination that fits the trend data best as well as the ‘joinpoints’ where the trends change using a Monte Carlo permutation method. This is useful in examining whether any changes in trends in youth suicide rates have occurred around the time when trends in societal factors also change, which would indicate a possible impact of the risk factors investigated on youth suicide. We used log-transformed annual suicide and self-harm rates in the joinpoint regression analysis and estimated the annual percent changes (APCs), the joinpoints of suicide and self-harm trends, and their 95% confidence intervals (CIs). To investigate trends in the potential societal risk factors for suicide rates, joinpoint regression with linear models was used to estimate the slope coefficients (β, i.e. annual changes), the joinpoints of linear trends and their 95% CIs. A maximum number of five joinpoints were used for all joinpoint regression analyses, and analyses were conducted using the Joinpoint Regression Program 4.6.0 software (National Cancer Institute, 2020). We plotted and examined the observed and estimated trends in suicide rates, societal factors and self-harm rates.
To study the associations between year-on-year changes in youth suicide rates and societal factors and youth self-harm rates, we used Prais–Winsten regression to account for serial autocorrelation in the time-series data. Each model included one factor as well as a calendar year variable to control for linear time trends. Whether the associations differed by sex was investigated by including interaction terms between sex and factors (e.g. sex × GDP per capita) in the models. Sex-specific suicide and self-harm rates and whole-population data for societal factors were used in regression analyses stratified by sex and when examining sex interaction. Prais–Winsten regression analyses were conducted using Stata 15.0 (StataCorp, College Station, TX).
Data for self-reported worry-related insomnia and suicide ideation, plan and attempt were available for only four and three survey waves in middle and high school students, respectively, and did not allow detailed regression analyses. Their prevalence was therefore only examined graphically.
Results
Trends in youth suicide
Suicide rates in males and females combined, males and females aged 10–24 years, showed generally similar trends in 1971–2019 (Figure 1(a)). Overall youth suicide rates decreased between 1971 and the early 1990s, followed by an upward trend in 1993–2005 and a downward trend between 2005 and 2014 (Table 1). Youth suicide rates subsequently changed from a downward trend to an upward trend in 2014—suicide rates of males and females combined increased 11.5% (95% CI = [5.2%, 18.1%]) annually in 2014–2019, and the increase appeared to be more marked in females (APC = 18.0%, 95% CI = [4.2%, 33.6%] in 2015–2019) than in males (APC = 8.3%, 95% CI = [3.2%, 13.7%] in 2013–2019). The youth suicide rates in the late 2010s surpassed the recent peak in the early 2000s and were comparable to those seen in the 1980s.
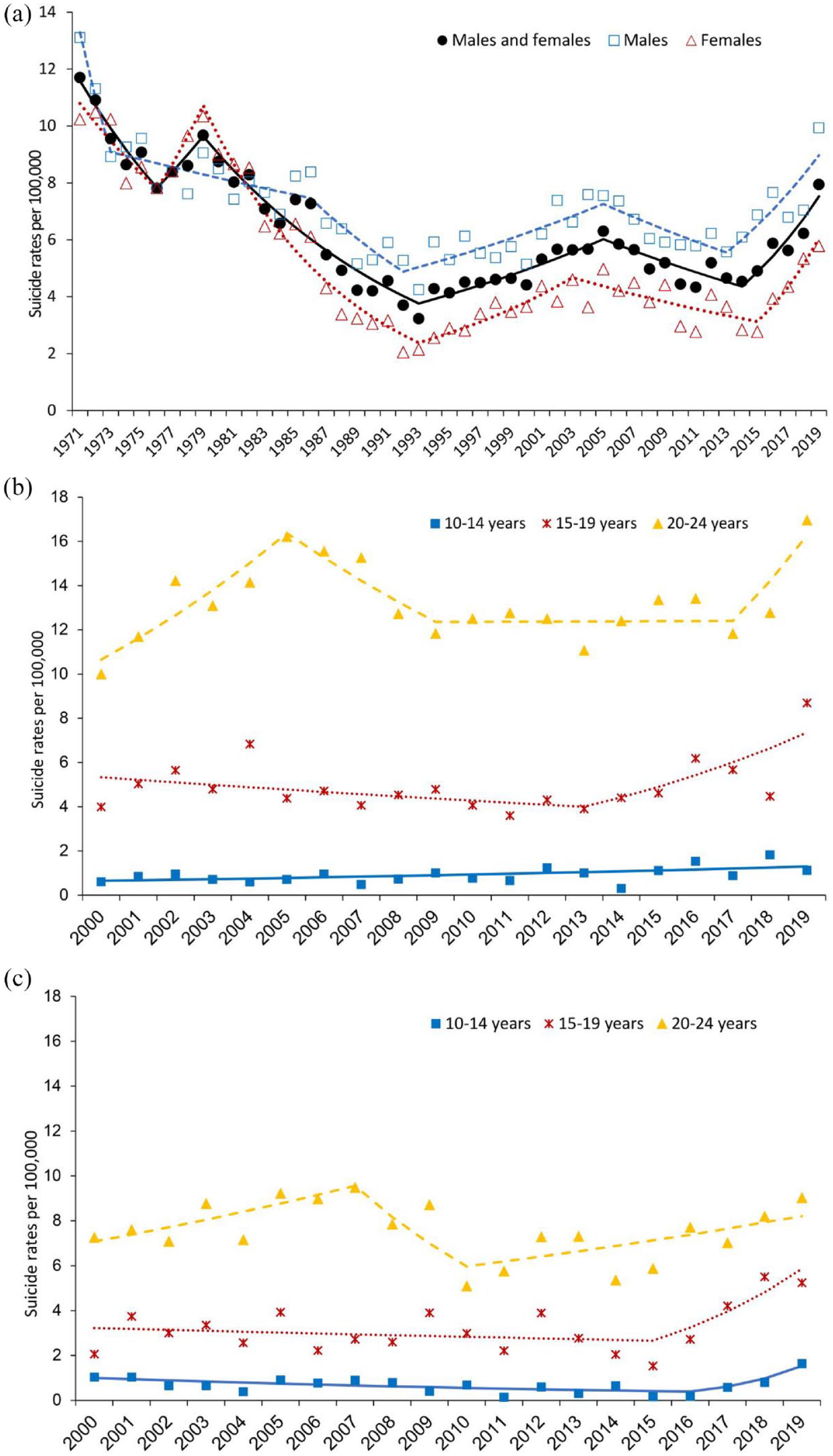
Suicide rates per 100,000 in (a) individuals aged 10–24 years in 1971–2019; (b) males aged 10–14, 15–19 and 20–24 years in 2000–2019; and (c) females aged 10–14, 15–19 and 20–24 years in 2000–2019 with joinpoint regression trend lines.
Results of joinpoint regression analysis of suicide rates in individuals aged 10–24 (1971–2019) and individuals aged 10–14, 15–19 and 20–24 years (2000–2019) in Taiwan.
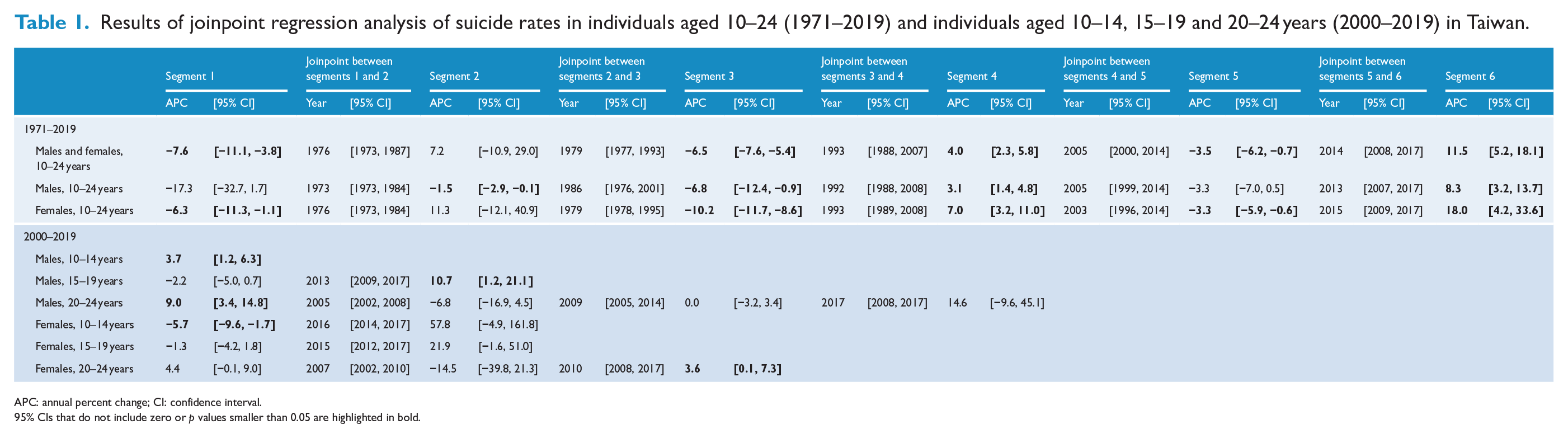
APC: annual percent change; CI: confidence interval.
95% CIs that do not include zero or p values smaller than 0.05 are highlighted in bold.
In males, the recent change in suicide trends was mainly seen in those aged 15–19 years (in 2013) and 20–24 years (in 2017), while males aged 10–14 years showed a continuous upward trend over the study period (Figure 1(b) and Table 1). By contrast, female suicide rates of 10–14, 15–19 and 20–24 year olds all showed a recent change in trends; they changed to an upward trend from 2016, 2015 and 2010, respectively (Figure 1(c) and Table 1).
Trends in societal risk factors and psychological distress indicators
Societal factors (Figure 2 and Table 2) and psychological distress indicators (Figure 3 and Table 2) showed various trends over the study period; a change in their trends around the year (2014), coinciding with the upturn in youth suicide rates, was found for divorce rates in females aged 40–59 years (2014) and self-harm rates in individuals aged 15–24 years (2013). The divorce rates among males aged 40–59 showed a stable trend from 2003, while those among females aged 40–59 had increased from 2014 (Table 2). Self-harm rates in youth aged 15–24 years (males and females combined) upturned from a stable trend in 2013 with further marked increases from 2017, most prominently in females. Self-harm rates among youth aged 0–14 were much lower than those in 15–24 year olds and increased between 2008 and 2019, with a marked further upturn upon the pre-existing increasing trend in 2017.
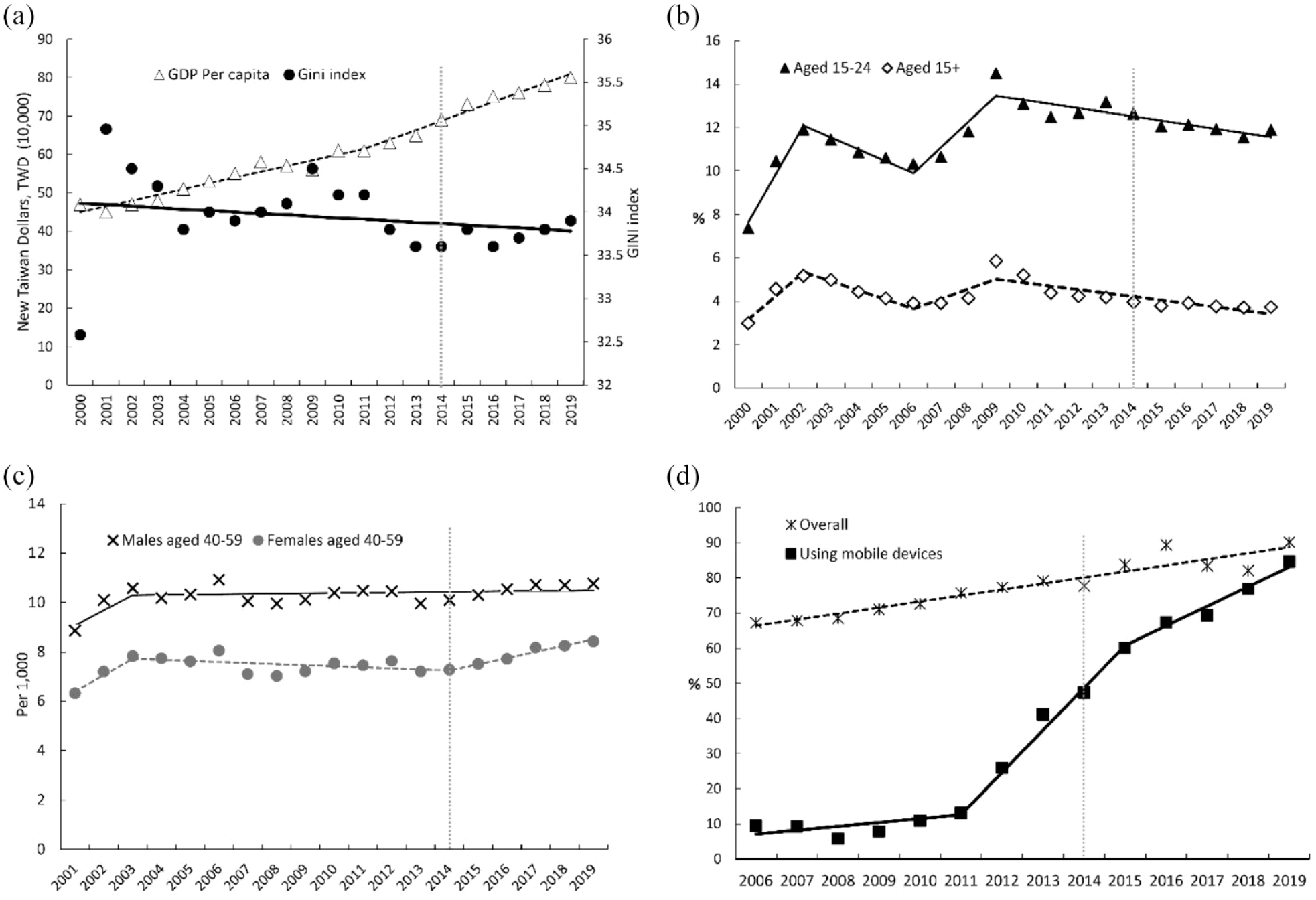
Trends in societal risk factors for youth suicide with joinpoint regression trend lines: (a) gross domestic product (GDP) per capita (10,000 New Taiwan Dollar) and Gini index; (b) unemployment rate (%), aged 15+ and 15–24 years; (c) divorce rates per 1000 married males and females aged 40–59 years; and (d) Internet use in the past 6 months (%), overall and using mobile devices.
Results of joinpoint regression analysis of societal risk factors for youth suicide, and self-harm rates, in Taiwan.
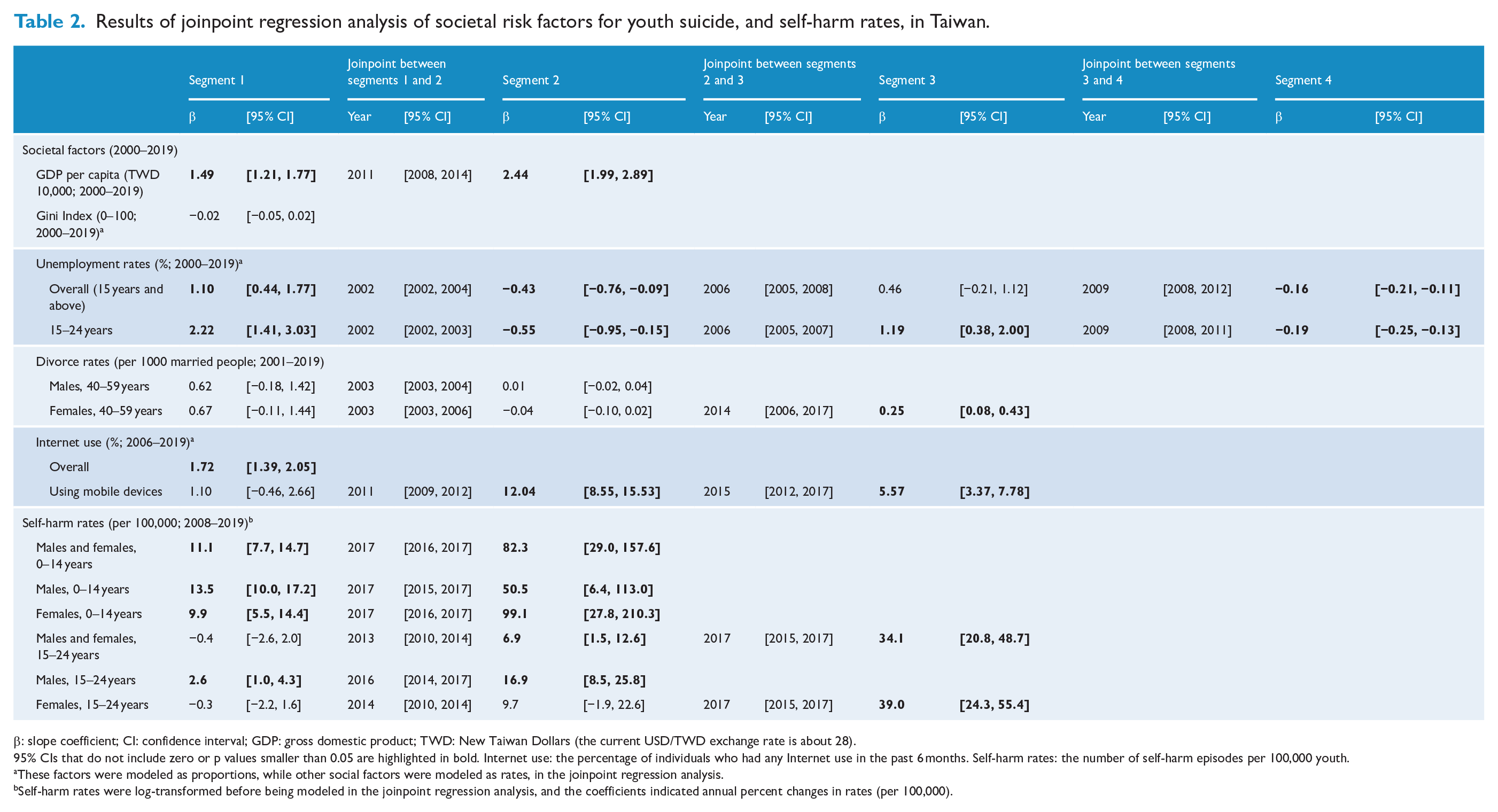
β: slope coefficient; CI: confidence interval; GDP: gross domestic product; TWD: New Taiwan Dollars (the current USD/TWD exchange rate is about 28).
95% CIs that do not include zero or p values smaller than 0.05 are highlighted in bold. Internet use: the percentage of individuals who had any Internet use in the past 6 months. Self-harm rates: the number of self-harm episodes per 100,000 youth.
These factors were modeled as proportions, while other social factors were modeled as rates, in the joinpoint regression analysis.
Self-harm rates were log-transformed before being modeled in the joinpoint regression analysis, and the coefficients indicated annual percent changes in rates (per 100,000).
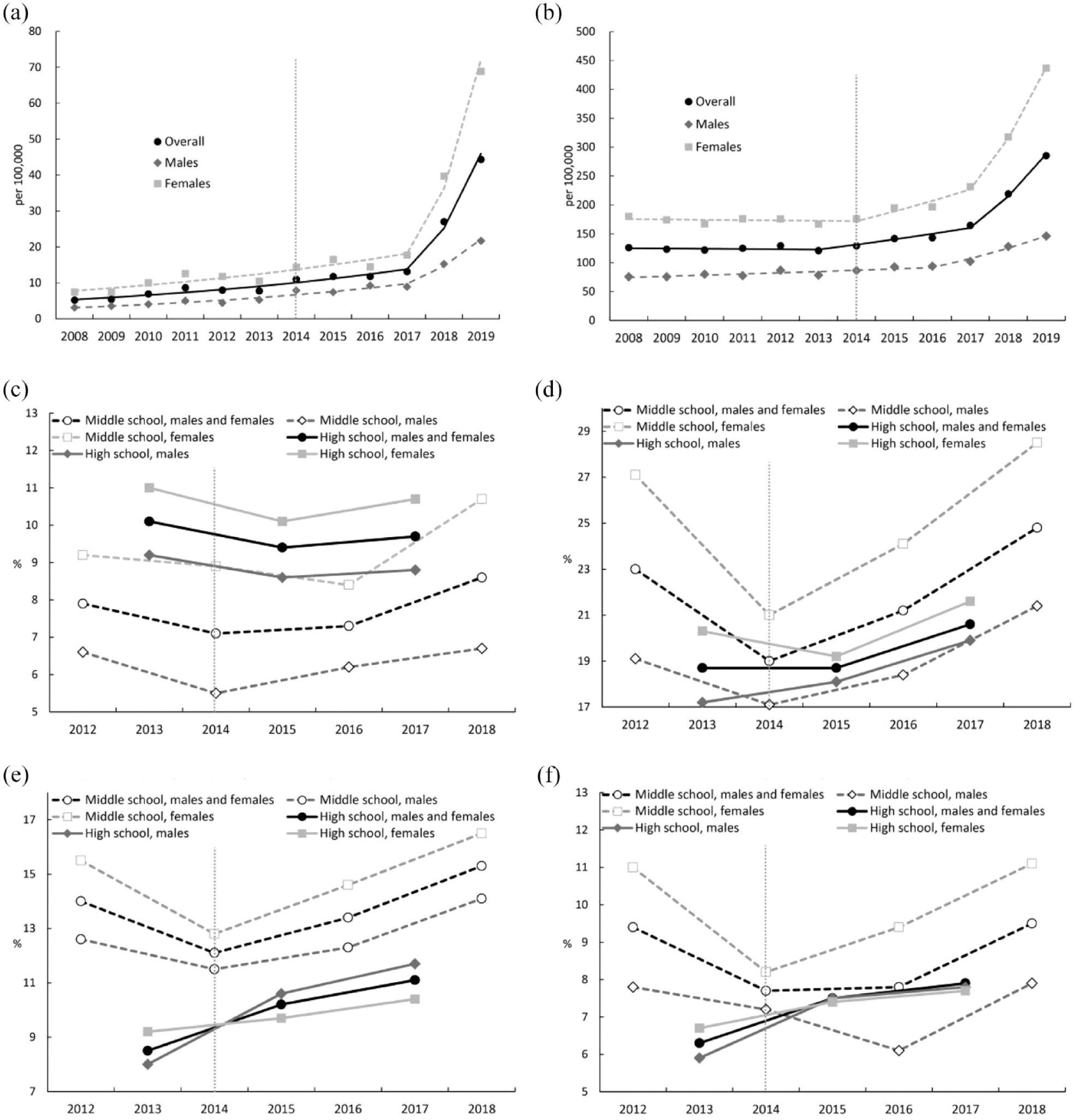
Trends in self-harm rates (number of self-harm episodes per 100,000) in (a) youth aged 0–14 years and (b) youth aged 15–24 years; trends in 12-month prevalence among middle/high school students of self-reported (c) worry-related insomnia; (d) suicide ideation; (e) suicide plan; and (f) suicide attempt.
Trends for other societal factors showed no changes that coincided with the change in youth suicide rates in 2014. GDP per capita showed an overall increase, while the Gini index showed a stable trend over the period. Both overall and youth unemployment rates fluctuated but showed a downward trend from 2009 after the 2008–2009 global financial crisis. Overall, Internet use showed an upward trend in 2006–2019, and Internet use through mobile devices showed a marked increase from 2011, with some level-off of the increase from 2015.
The prevalence of youth self-reported worry-related insomnia and suicide ideation, plan and attempt generally started to increase from 2014/2016 (in middle school students) or 2013/2015 (in high school students) (Figure 3). Overall, the prevalence of all suicidal behaviors (ideation, plan and attempt) in the most recent waves (2018 for middle school students; 2017 for high school students) was higher than that in the first waves (2012 for middle school students; 2013 for high school students), indicating a rise in suicide risk in Taiwanese young populations in recent years.
Associations between trends in youth suicide and potential societal risk factors and psychological distress indicators: Prais–Winstein time-series analysis
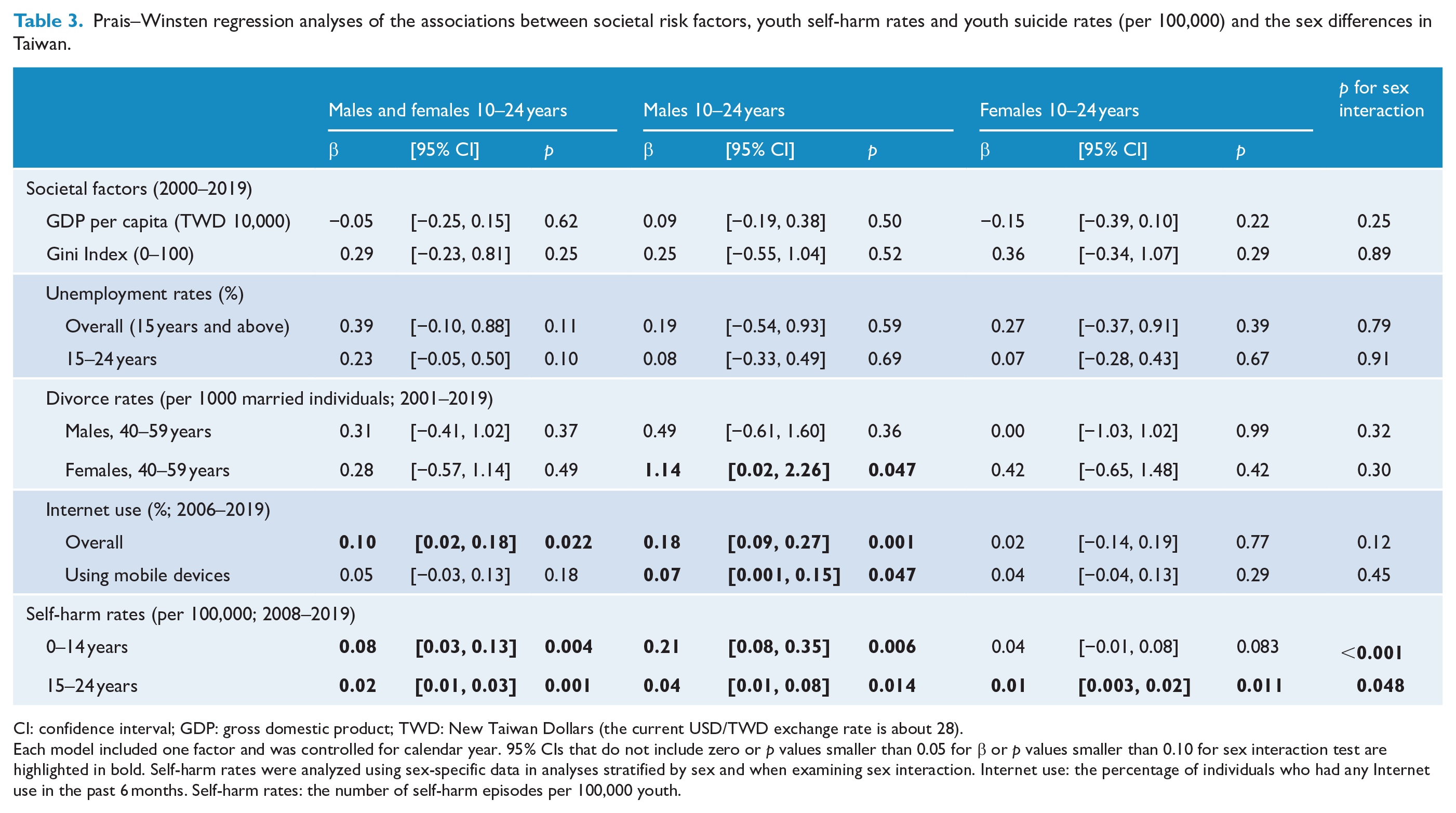
We found no association of GDP per capita, Gini index and unemployment rates with youth suicide rates in males and females combined, males only or females only (Table 3). By contrast, the divorce rates of 40- to 59-year-old females were positively associated with male youth suicide rates (β [i.e. change in suicide rate per 100,000 for each 1% increase in divorce rate] = 1.14, 95% CI = [0.02, 2.26]; p = 0.047). Overall, Internet use was positively associated with youth suicide rates of males and females combined (β = 0.10, 95% CI = [0.02, 0.18]; p = 0.022) and males only (β = 0.18, 95% CI = [0.09, 0.27]; p = 0.001), while Internet use through mobile devices was positively associated with youth suicide rates in males only (β = 0.07, 95% CI = [0.001, 0.15], p = 0.047). However, no statistical evidence for sex interaction was found for the associations of youth suicide rates with divorce rates or Internet use (p for interaction > 0.10). Self-harm rates in youth aged 0–14 and 15–24 years were positively associated with youth suicide rates; the coefficients were 0.08 (95% CI = [0.03, 0.13]; p = 0.004) and 0.02 (95% CI = [0.01, 0.03]; p = 0.001), respectively. The associations between youth self-harm rates and suicide rates were stronger in males than females (p for interaction < 0.05).
Prais–Winsten regression analyses of the associations between societal risk factors, youth self-harm rates and youth suicide rates (per 100,000) and the sex differences in Taiwan.
CI: confidence interval; GDP: gross domestic product; TWD: New Taiwan Dollars (the current USD/TWD exchange rate is about 28).
Each model included one factor and was controlled for calendar year. 95% CIs that do not include zero or p values smaller than 0.05 for β or p values smaller than 0.10 for sex interaction test are highlighted in bold. Self-harm rates were analyzed using sex-specific data in analyses stratified by sex and when examining sex interaction. Internet use: the percentage of individuals who had any Internet use in the past 6 months. Self-harm rates: the number of self-harm episodes per 100,000 youth.
Discussion
Suicide rates and the prevalence of suicidal behaviors began to increase in Taiwanese youth in the 2010s. The recent increases in suicide were found among youth across the early, middle and late adolescence periods. In keeping with our hypotheses, the recent rise in youth suicide was associated with unfavorable trends in some societal factors and psychological distress indicators. The change in youth suicide trends in 2014 occurred closely in time with the upturn in divorce rates among females aged 40–59 years (i.e. the age group most likely of youth’s mothers) in 2014 and the rise in youth self-harm rates (aged 15–24 years) in 2013. Furthermore, annual youth suicide rates were associated with female divorce rates aged 40–59 years (male youth suicide only), Internet use rates and youth self-harm rates. Moreover, the increases in the prevalence of self-reported worry-related insomnia and suicidal behaviors among young students in the mid-2010s were in parallel with the increase in youth suicide rates. The findings suggested that these factors may have contributed to the recent increase in youth suicide in Taiwan.
Strengths and limitations
This is among the first studies investigating the association between recent trends in youth suicide and a range of societal factors and psychological distress indicators that may increase youth suicide rates in the 21st century. Data for these factors/indicators were extracted from nationally representative databases or surveys over more than a decade when the youth suicide rates showed an upturn from a previous downward trend, providing an opportunity to identify potential causes of the recent rise in youth suicide. Nonetheless, there are several limitations of the study. This is an ecological study and the association between youth suicide rates and potential risk factors could not be directly inferred as causal. However, analysis of factors contributing to secular trends in population health outcomes such as suicide rates can only be or is best done at the ecological level. Data for some key potential risk factors such as Internet use were not age-specific. Some measures such as Internet use, worry-related insomnia, and suicide ideation, plan and attempt were based on single-item questions in surveys. The prevalence of Internet use is a relatively crude indicator. Previous research suggested that social media content—what young people post and view online—is particularly important for mental health problems (George, 2019). Annual data for potential societal risk factors/self-harm rates were available for only 13–20 years, and this would limit the statistical power of identifying associations of a smaller strength and prevent multivariable analyses controlling for multiple risk factors. Self-reported data for insomnia and suicidal behaviors extracted from the biennial youth health surveys were only available for three or four waves, and therefore, regression analyses could not be applied. The finding may be specific to the setting of Taiwan, while many other countries also experienced similar trends in potential societal risk factors for youth suicidal behavior such as a marked increase in Internet use (Padmanathan et al., 2020).
Comparison with previous findings
Recent rises in youth suicide rates were found in several English-speaking countries including Australia, Canada, the United Kingdom and the United States (Padmanathan et al., 2020). A study of suicide rates among 15–24 year olds in 11 high-income countries in 2000–2017 showed an upturn from a previous downward trend in Australia and Canada in 2009 and 2007, respectively; in the United Kingdom and the United States, where the rise in youth suicide began from 2003 and 2007, respectively, youth suicide rates experienced a further increase from 2014 (Padmanathan et al., 2020). Recent rises in suicide rates were also found among 20–29 year olds in Brazil in 1997–2019 (Arruda et al., 2021), and among 15–19 year olds in Denmark and Turkey from 2014 and 2015, respectively (Eurostat, 2021). By contrast, recent youth suicide rates fluctuated or showed a downward trend in France, Italy, Poland, Spain, Germany, Japan and South Korea (Padmanathan et al., 2020). In Japan and South Korea, which are in the same geographic region as Taiwan, youth suicide rates changed from an upward trend to a downward trend in 2009 (Padmanathan et al., 2020). However, there are few studies on recent youth suicide trends in other Asian countries. Recent trends in youth suicide appear to vary in different countries and require context-specific investigations into factors associated with changes in trends, although some phenomena, e.g. growth in social media use, are global.
The recent increase in youth suicide in Taiwan was found across the early, middle and late adolescence periods, suggesting possible shared factors underlying the increase in suicide across young people of different ages. By contrast, suicide rates of older groups showed no increase over the recent decade (the 2010s) in Taiwan—suicide rates were stable in middle-aged groups aged 25–64 years and decreased in older people aged 65+ years (Chang et al., 2020). Similarly, all-age suicide rates in Canada showed a relatively stable trend in 2006–2015 (Alicandro et al., 2019) when youth suicide rates increased over the same period (Padmanathan et al., 2020). By contrast, recent increases in youth suicide paralleled the upward trends in overall suicide rates in Australia, the United Kingdom and the United States (Alicandro et al., 2019; Padmanathan et al., 2020). This suggests that recent rises in youth suicide may be influenced by certain age-specific factors in some countries, such as Canada and Taiwan, while the rises in youth suicide rates may reflect trends in overall suicide in other countries such as Australia, the United Kingdom and the United States.
Recent increases in youth suicide were found in both sexes in Taiwan, and males consistently showed higher suicide rates than females. By contrast, trends in youth suicide appeared to differ by sex in some countries. In Australia, suicide rates among young females increased between 2004 and 2014 and became stable in 2014–2018, while suicide rates among young males were stable in 2004–2014 and subsequently increased (Australian Bureau of Statistics, 2021; Stefanac et al., 2019). It is important to examine sex-specific youth suicide rates and related factors in countries that showed divergent youth suicide trends in males and females.
When youth suicide rates showed an upturn from a downward trend in the 2010s, Taiwan experienced continuous economic growth, a decrease in unemployment rates and no obvious change in income inequality over the period. Our regression analyses showed no association between these economic factors and youth suicide rates in Taiwan. By contrast, the recent rises in youth suicide were found to be associated with the level of Gini index, but not its changes, across 11 high-income countries (Padmanathan et al., 2020). The association between youth suicide rates and income inequality, which has increased in many countries in recent years, requires further research.
Our data showed that trends in both the divorce rates of 40- to 59-year-old females and youth suicide rates turned upward in 2014. Moreover, regression analysis showed a positive association between year-on-year changes in the divorce rates among 40- to 59-year-old females and the suicide rates among young males aged 15–24. Offspring of divorced parents were found to have increased risk of mental disorders (Sands et al., 2017), suicide ideation (Fuller-Thomson and Dalton, 2011), suicide attempt (Donald et al., 2006; Siu, 2019) and suicide (Grande et al., 2021). In Taiwan, the divorce rates in the 40- to 59-year-old married population were relatively stable in the early 2010s but increased 21% and 16% in males and females, respectively, between 2014 and 2019 (Ministry of Interior, 2021). Taiwan’s existing policies and resources that support young people from divorced families may be insufficient to meet the increased needs and contribute to poor mental health and suicide risk in the young population.
We found an association between Internet use rates and youth suicide rates. By contrast, a recent study found no difference in the increase in time spent on social media in the population between high-income countries with and without a recent increase in youth suicide (Padmanathan et al., 2020). Person-based research showed mixed findings about the relationship between young people’s Internet and social media use and mental health problems (Keles et al., 2020; Sedgwick et al., 2019). Several factors may contribute to increased risk of suicidality among young Internet users: (1) the dissemination of suicide-related information on the Internet that may trigger imitation or the use of lethal methods for suicide (Biddle et al., 2016); (2) imitative suicidal behaviors triggered by media reporting of celebrity suicides or popular web series or movies available on the Internet that include dramatic depictions of suicidal behaviors (Niederkrotenthaler et al., 2019, 2020); and (3) the emergence of cyberbullying (John et al., 2018). Harmful Internet content such as irresponsible media reporting (World Health Organization and International Association for Suicide Prevention, 2017) or inappropriate drama representations of suicidal behavior (World Health Organization, 2019a) should be regulated.
Our findings of the parallel trends in deteriorating youth mental health, increases in self-harm rates and the prevalence of suicidal behaviors, and rises in suicide rates were also reported in several countries. In the United States, where overall youth suicide rates increased from 2009 (Padmanathan et al., 2020), the prevalence of suicide ideation among adolescents also increased annually by 3.4% between 2009 and 2019 (Xiao et al., 2021). In the United Kingdom, the prevalence of mental illness and self-harm in young people increased between 2003 and 2018 (Cybulski et al., 2021); meanwhile, youth suicide rates started to rise from 2003 and increased further from 2014 (Padmanathan et al., 2020). Worsening mental health appeared to be a potentially important contributor to the increase in youth suicide rates in these countries. In Taiwan, a recent cohort study indicated that adolescents with higher levels of sleep problems were more likely to have suicide ideation (Chang et al., 2021). Youth suicide prevention could include strategies aimed at addressing the causes of poor mental health, early identification and treatment of sleep problems and suicide ideation, plan and attempt, and encouraging help-seeking.
Conclusion
Taiwan’s youth suicide rates started to increase in the mid-2010s. The rises in parental divorce rates, Internet use and young people’s poor sleep and self-harm may be associated with the increase in youth suicide rates. Further research is needed to examine the mechanisms underlying the associations of these factors with the rise in youth suicide. Potential youth suicide prevention strategies may usefully target on providing support to minimize the negative impact of parental divorce, regulating potentially harmful content on the Internet, and the early detection and management of youth’s psychological symptoms and suicidal behaviors.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The study was funded by a grant awarded to C.-Y.H. by the Taiwan Ministry of Science and Technology (grant number MOST 109-2314-B-038-019-MY2). C.-Y.H. is supported by Wan Fang Hospital (grant numbers 110-swf-07 and 111-wf-swf-04). Y.-H.C. is supported by the Taiwan Ministry of Science and Technology (grant number MOST 109-2811-B-002-589, MOST 110-2811-B-002-588). D.G. is supported by the NIHR Biomedical Research Centre at University Hospitals Bristol and Weston NHS Foundation Trust and the University of Bristol, England. The funding sources have no role in the data collection, analysis, interpretation or writing of the manuscript or the decision to submit the paper for publication. The views expressed in this publication are those of the authors and not necessarily those of the NHS, the National Institute for Health and Care Research or the Department of Health and Social Care.
Ethical Approval
The study was entirely based on aggregated vital or survey statistics or anonymous data and thus ethical approval is not required.