
Abstract
This paper summarises a report to the Youth Suicide Committee of the Strategic Research Development Committee of the National Health and Medical Research Council. The objective of the report was to review the epidemiology of suicide and attempted suicide among young people in Australia, highlighting gaps in knowledge.
Definitions of suicide and data collection
Coroners
Considerable heterogeneity exists in the various State and Territory Coroner Acts. Formal suicide verdicts are used only in New South Wales (NSW) and Western Australia (WA). The other states and territories mostly confine findings to medical as opposed to behavioural descriptions of deaths. Some may use the word ‘suicide’ if the circumstances are absolutely clear that this was intended, but others never use the word. All states and territories are inherently conservative in suggesting that deaths were intentionally self-inflicted, requiring high standards of probability.
Australian Bureau of Statistics
The Australian Bureau of Statistics (ABS) provides the official national, state and regional suicide statistics, using the International Classification of Diseases (ICD-9) definition of ‘suicide, or self-inflicted injury’.
Suicides not classified as such are most likely to fall into the ICD categories of ‘undetermined’ or ‘accidental’ deaths. Some coroners are under pressure to emphasise ‘accidental death’ where doubt exists. Australian Bureau of Statistics coders are not permitted to allocate the undetermined death code without coroners' recommendations. Where an ABS coder suspects that a death may have been by suicide but has insufficient evidence to code it as such, it must be coded as an accident or death by natural causes. Cases involving children under 10 years attract a higher threshold for classification as suicide as their intent is more questionable. Delays in resolving cases affect data collection. If a case is not resolved before the ABS cut-off date to produce annual data, it will remain coded as accidental regardless of the likelihood of it being deemed a suicide at a later date.
The National Coronial Information System
A number of states have developed alternative data systems with more detailed and clinicially relevant data than the ABS. Unfortunately, these data systems are not uniform. The National Coronial Information System (NCIS) is a system under development for the provision of uniform, comprehensive, consistent and timely data relating to deaths involving coroners. A steering committee has been convened by the Australian Coroners Society consisting of coroners and major users. This system may lead to uniform guidelines on the reporting of suicides.
Attempted suicide
The official collection of attempted suicide data used to be collated by ABS but is now the responsibility of each state and territory. Data collection procedures and reliability vary across states and territories with one advising that suicide attempts presenting to accident and emergency departments would not be recorded as such unless they were admitted to a mental health facility. Major impediments to reliable data are evident worldwide [1].
Even where a state or territory operates a relatively reliable system, these figures are, in fact, attempted suicides ‘admitted’ to hospitals. Most suicide attempts never come to medical attention. Australian community self-report surveys of young people suggest that self-destructive or suicidal behaviour is likely to be far more common than official data suggest [2–4], with one estimate suggesting 50–80% of attempted suicides did not receive medical attention [5].
Despite these considerable obstacles, some individual states have been able to gather useful data, for example, WA [6], NSW [5] and Victoria [7].
Studies of under-reporting and uncertain suicides
Worldwide, the reliability of suicide reporting is questionable and the validity of suicide as a construct is dubious. Clinicians are aware that suicidal acts are associated with degrees of ambivalence. The World Health Organization (WHO) favours eliminating intent from the definition.
Kosky [8] in an early study of youth suicide documented a 100% rise in suicides in 15 to 19-year-old male Australians 1965–1985. He noted a simultaneous decline in undetermined deaths, suggesting that 20% of the rise in suicides might be associated with coroners becoming less inclined to use the undetermined category. Cantor and Dunne [9] suggested that a rise of up to 8.3% was a more accurate figure.
Cantor and Dunne [10] examined this issue further, demonstrating that the decline in undetermined deaths for 15–19-year-old males involved only a few deaths per year, so was insufficient to significantly influence the suicide rate. Considerable interstate variability was evident. Whereas NSW reported 933 undetermined deaths (all ages) for 1968–1976, only two deaths were recorded in Queensland, a result suggesting massively divergent practices.
With undetermined and accidental deaths, real changes may occur over time. For example, increasing availability and potency of heroin for recreational use has been associated with a rise in opiate deaths 1970–1995, from 10.7 to 77.0 per million of the population aged 15–44 [11]. It is unclear how reliably opiate deaths may be classified.
Epidemiology of suicide and attempted suicide in Australia (all ages)
International comparisons
Bearing in mind the above divergent intranational data practices, international comparisons must be approached conservatively [12,13]. An early study by Goldney and Katsikitis demonstrated rising rates of suicides by Australian males 15–24 years during the 1960s and 1970s [14]. During the 1970s and 1980s, while the suicide rates for males 15–29 years rose further, rates declined for females of this age and for both genders aged 30–54 and more than 55 years [15].
Lester [16] examined changes in suicide rates for 32 countries, 1980–1990. For males, total, youth and elderly suicide rates showed an approximately equal likelihood of decrease or increase, with slightly more countries demonstrating increases in total and elderly suicide rates and decreases in youth suicide rates. Female suicides demonstrated downward trends, with decreases in total and youth suicide rates. Finland, Northern Ireland and Norway experienced increases and Canada, Czechoslovakia, Japan and West Germany experienced decreases for all age and sex combinations.
More recently, in a listing of 51 countries supplying data to the World Health Organization in 1996 [17], Australia's overall male suicide rate was ranked 28th and its female rate ranked 31st.
In almost all countries males have higher suicide rates than females. China is the exception, with female suicide rates exceeding those of males, especially in rural areas. In China, female status is greatly undervalued.
Suicide rates peak in people over 75 years in most countries. With the increasing proportion of older persons in the population, suicide in the elderly is important to consider. In many European and some Latin American countries, sharp increases in suicide in the elderly started to level off in the early 1990s. In some countries, such as the USA, Italy and Japan, rates have fallen during the 1990s [18].
While suicide rates for Australian males 75 years and over are higher than all younger ages [19], their international ranking is typical of developed nations, in contrast to high youth suicide rankings. A study of the elderly found the Australian 1988 65 years and over male rate to be 31.8 per 100 000. This contrasted with Hungary (127.2 per 100 000). In addition, East Germany, Sri Lanka, China, Bulgaria, Austria, Yugoslavia, Denmark, France, Japan, Czechoslovakia, Switzerland, USSR, West Germany and Finland all had rates over 50 per 100 000 [20].
Australia
In Australia, the reported overall suicide rate is similar to that at the turn of the century (males 21 per 100 000; females 5 per 100 000). Data collected over such a period must be interpreted cautiously, as collection procedures have changed over time. There was a peak for males during the Depression in the 1920s and a further peak for both genders in the early 1960s, coinciding with prescribing of barbiturates. A significant subsequent decline followed, associated with the introduction of safer benzodiazepines [21].
Suicide and suicidal behaviour among young Australians
Australian suicide rates by age and gender
An increase in youth (15–24 years) suicide has occurred since the 1960s in Australia. Youth suicide is second only to motor vehicle traffic accidents as a cause of death in young Australians [22]. Gender differences in suicide rates are greater in youth (Male: Female = 6.25:1) than older ages.
Youth age subgroups
0–14 years
Suicide is rare in children under 14 years. This may partly relate to different data collection practices. Youth suicide is predominantly a problem of older adolescents and young adults (Table 1).
Numbers and rates of suicides (per 100 000) in youth age groups by gender, 1990–1995
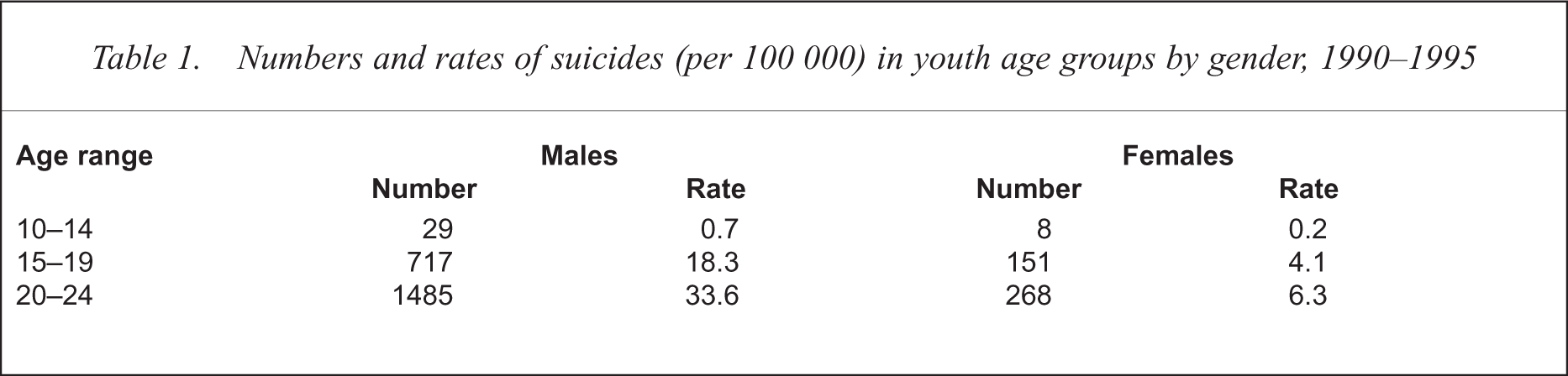
Kosky [23] examined suicide and attempted suicide in children, aged 14 and younger. In Australia, 72 child suicides were recorded during 1969–1978. The male: female ratio was 3:1, with an annual rate of 0.3 per 100 000. The youngest suicide was aged 5. A subsequent study found no noticeable change in suicide rates for either gender aged 10–14, during 1965–1985 [8].
15–24 years
Suicide rates for youth aged 20–24 are much greater than those aged 15–19, especially for males (Table 1), although the rate of increase in recent decades has been greater in 15–19-year-olds. In a study of suicide trends 1960–1989 in ‘New World’ countries (Australia, New Zealand, USA and Canada), the increase for males 15–19 years more than quadrupled and for females increased more than 2.5 times [24]. In the 20–24-year-old group, male suicide rates trebled and female rates doubled.
International rankings
An early study examined suicide rates for 1970 and 1985/1986 for 19 heterogeneous countries spanning the continents [15]. Australian males aged 15–29 ranked seventh in 1970 and second in 1985/1986, with females ranking eighth in 1970 and 13th in 1985/1986.
Pritchard [25] compared suicide rates of Australia and New Zealand with 19 countries from Western Europe, North America and Japan. Australia's male youth (15–24 years) suicide rate for 1987 ranked seventh and New Zealand's ninth. For female youth suicide, Australia ranked seventh and New Zealand fourth. North-west European countries (Finland, Austria, Switzerland, Denmark) had the highest rankings and southern European countries (Greece, Italy, Spain) and the UK had the lowest.
A UNICEF [26] study of 14 industrialised countries, ranked Australia as having the highest rate (16.4 per 100 000) of youth suicide during 1987–1990. This study is often misrepresented as implying Australia has the world's highest youth suicide rate. A more recent UNICEF [27] study ranked the youth suicide rates of 32 countries from Europe, America, Asia and Oceania, for 1991–1993. Australian males ranked ninth and females 11th.
Table 2 reports recent youth suicide rates for 50 countries ranked according to male rates [17]. Australian male youth ranked 13th, mostly behind newly independent states of the former USSR and northern European countries. Australian rates were lower than New Zealand, but comparable with Canada, Norway and USA. Female rankings placed Australia around 30th. Female rates were all under 12 per 100 000 except for selected rural areas of China (33 per 100 000).
International youth suicide rates (per 100 000) ranked by males, 1994a
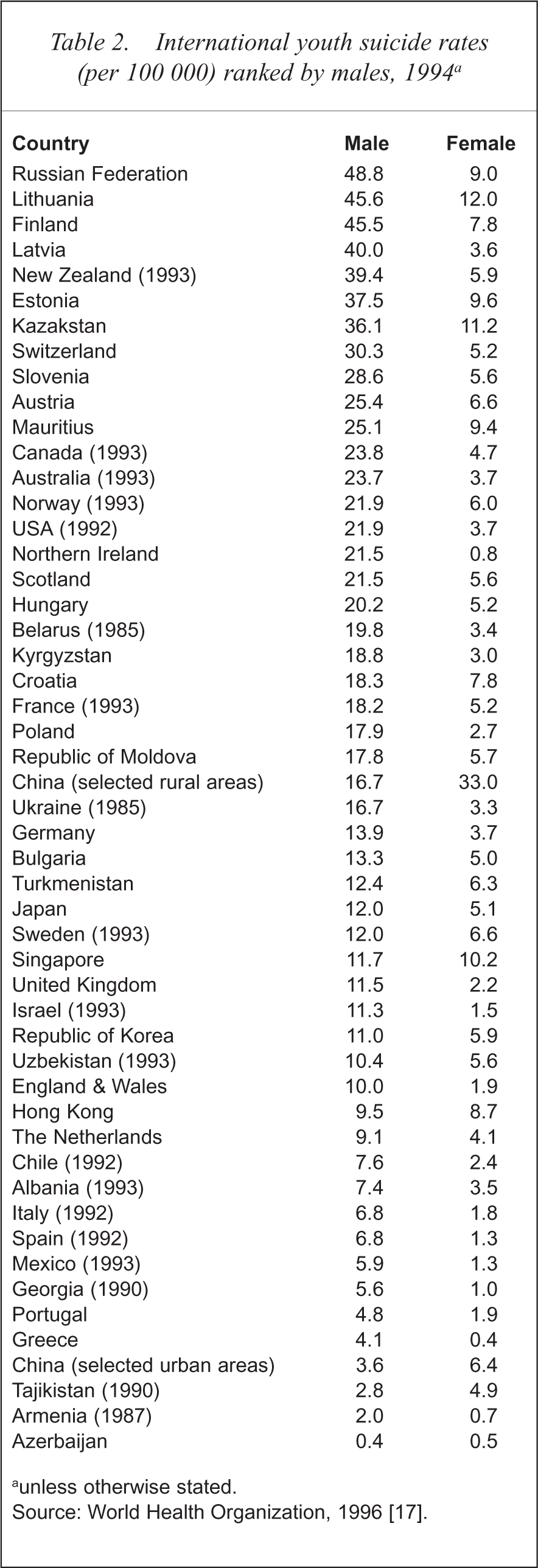
unless otherwise stated.
Source: World Health Organization, 1996 [17].
International trends
For some purposes it may be more productive to compare similar nations. Cantor et al. [24] examined eight English-speaking nations sharing common characteristics, but also subdivided them into four ‘Old World’ and four ‘New World’ countries (Scotland, Northern Ireland, Ireland, England and Wales vs Canada, USA, Australia and New Zealand respectively). The hypotheses were that the eight nations would show relatively similar patterns of suicide overall, but also would group into ‘Old’ and ‘New World’ subgroup patterns. Both hypotheses were supported. Youth suicide trends during 1960–1989, for all eight English-speaking countries, showed significant commonalties. In the ‘New World’ countries, USA and Canada clustered together as did Australia and New Zealand. La Vecchia et al. [28] also found that overall suicide trends of Australia and New Zealand followed those of North America. This suggests study of ongoing North American trends may be relevant to Australian developments.
Male trends
Male youth suicides over the past 40 years have generally increased. Suicide trends in males aged 15–29 from 1970 to 1985/1986 increased in 16 of 19 diverse countries [15]. Similarly, Pritchard [25] found that during 1973–1987, of 21 developed countries, only three experienced decreases in male youth suicide.
Youth suicide trends in the eight English-speaking countries study, also showed great increases in males 15–29 years from 1960 to 1989. However, the ‘New World’ countries had almost double the suicide rates of the ‘Old World’ countries for this age group [24].
In Lester's [16] study of youth suicide trends in 32 countries from 1980 to 1990, 15 countries had increases, including Australia, USA, New Zealand and many European countries from which people immigrate to Australia (e.g. Italy, Greece, England and Wales, Ireland, Northern Ireland and Scotland), while 17 had decreases.
Female trends
Suicide trends in young females are less clear. Trends in females aged 15–29 years from 1970 to 1985/1986 decreased in seven of 19 diverse countries (including Australia and North America) and increased in 12 [15]. Pritchard's study of 21 developed countries reported decreases or no change in female youth suicide in 11 countries, during 1973–1987, indicating variable trends [25].
In the study of eight English-speaking countries, female youth suicide rates were more uniform than males in all the countries, although the ‘New World’ countries did have higher suicide rates than the ‘Old World’ [24]. Increasing trends were evident in the 1960s, with rates reaching a plateau in the 1970s. The 1960s' increase was also evident in all older females. However, both New Zealand and Scotland demonstrated upward trends from the mid-1980s.
In Lester's [16] study, 22 countries experienced decreases (including most English-speaking countries) from 1980 to 1990 in female youth suicide rates while 10 experienced increases.
Studies of Australian trends
A number of studies have examined Australian suicide trends for gender over time. Figure 1 illustrates the youth suicide rate in Australia, 1921–1995. Male youth suicide rates demonstrate a steady increase since the early 1970s, while female youth suicide rates have been fairly stable [29].
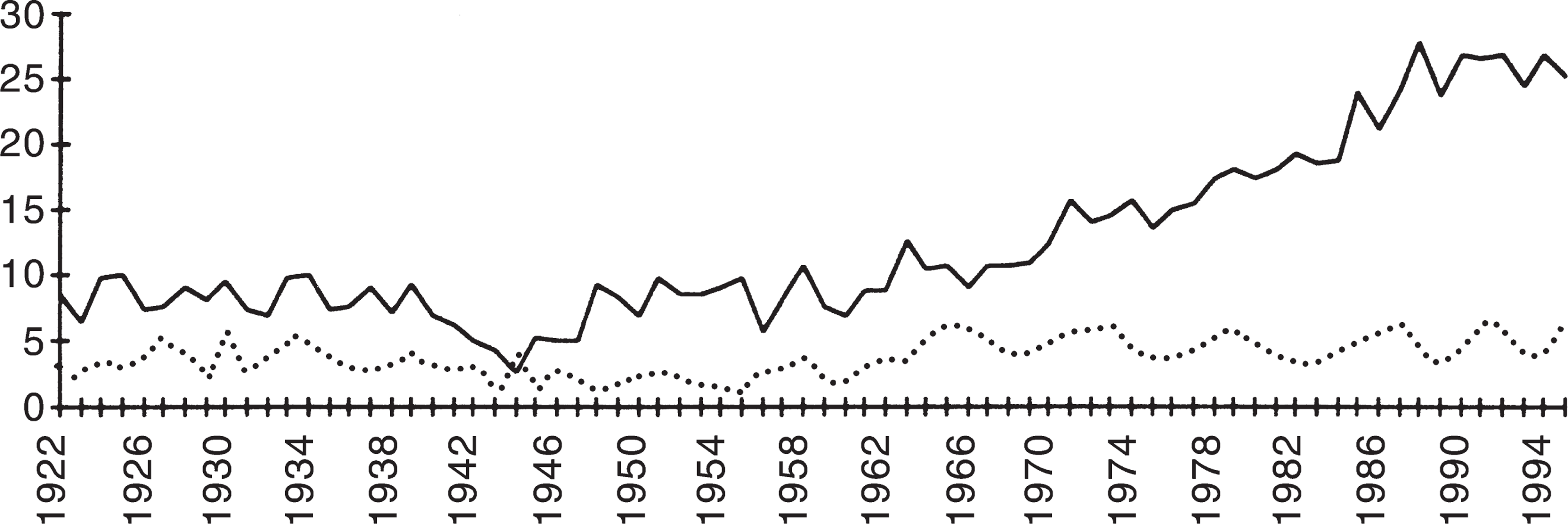
Youth suicide rates (per 100 000) in Australia 1921–1995. —, male; —, female. Source: Baume et al. [29].
Male trends
Burvill [30] studying suicides in Australia during 1910–1977, found that suicide rates for males aged 15–19 were relatively constant until around 1963 when rates started to increase. The 20–29-year-old group followed the overall male suicide pattern until 1968 when the rates started to increase. These increases were in contrast to older age groups, which showed decreases.
Pritchard [25] found that during 1973–1987, rates for young males (aged 15–24) increased by 66% in Australia and 127% in New Zealand. Lester [16] found an increase of 51% in Australia from 1980 to 1990 and an increase of 95% for New Zealand.
Krupinski et al. [31] examined youth suicide trends in Victoria finding that during 1907–1990 an increase in male youth suicides started around 1962. For the 20–24-year-old group, this figure reached a plateau in 1980.
Female trends
During 1910–1977, female rates were found to follow the same general patterns, except the youth groups showed higher rates in the 1920s compared with the other age groups [30].
Between 1973 and 1987, Pritchard [25] reported a decrease of 6% in Australia, and an increase of 70% in New Zealand for young female suicides. In contrast, Lester [16] reported a slight increase of 4% for Australian female youth suicide rates and a decrease of 17% for New Zealand females, during 1980–1990.
In Victoria, during 1907–1990, no trend was found for females [31].
Attempted suicides
Attempted suicides are reported as being greater in females than males. However, as there are many problems with the data it is impossible to determine accurate rates. These problems include attempted suicide data usually based on hospital admission samples; little consistency between hospitals regarding what constitutes an admission; hospital data biased towards self-poisonings and lacerations; and only those people who present to hospitals are recorded, omitting those who see general practitioners or who do not seek any medical assistance, estimated to be between 50 and 80% of all attempted suicides [5].
Studies have tried to overcome the biasing of hospital samples by using community samples. These are also problematic as they rely on self-report questionnaires, which are unreliable due to subjectivity. A study in Australia found that of 40 people who initially reported having suicidal ideation in 1984, 16 denied ever having had suicidal ideation 4 years later [32]. While community self-report studies have low reliability they offset the biases of hospital samples.
Hospital samples
An early study of attempted suicides (all ages) in Perth, used hospital data for 1971–1972 [33]. A doubling of the attempted suicide rate was found since 1961, with rates of 85 per 100 000 for males and 203 per 100 000 for females.
A study of attempted suicide, as measured by admission to a state or children's psychiatric hospital, was conducted for children 14 years and under in WA during 1969–1978 [23]. For children less than 12-years-old, boys attempted suicide 2.5 times more than girls, in contrast to children under 15 years, with girls outnumbering boys 4:1.
Increases of 114% for males aged 15–19 and of 26% for 20–24-year-olds were found when comparing attempted suicide hospital data in Perth from 1971–1972 with 1986–1987 [34]. For females, an increase of 7% in 15–19-year-olds and a decrease of 13% in 20–24-year-olds were found. Examination of attempted suicide rates in Adelaide during 1986–1987, found for both genders that 60–67% more attempted suicides occurred than were reported [34]. The attempted suicide ratio of females to males was reported as 1.9:1 for 15–19-year-olds and 1.3:1 for 20–24-year-olds. These ratios were similar to those in Perth and showed narrowing of the youth attempted-suicide gender ratio. Both the Perth and Adelaide samples showed the peak age group for attempted suicides in males to be 20–24 years, and for females, 15–19 years.
Another study of attempted suicide among Perth youth (aged 10–24) measured attempted suicides by hospital admittance in 1990. It was estimated that the annual rate of attempted suicide in Perth was 364 per 100 000 for 15–24-year-olds [35]. The hospital attempted suicide rate was 21 times greater than that of completed suicides in Perth youth. The female: male attempted youth suicide ratio was 1.6:1, comparable to that found by Davis and Kosky [34].
In Victoria, youth attempted suicide was examined in two groups: hospitalised (at least 24 h) and non-hospitalised. Again, gender differences were small, with the female: male ratio for the hospitalised group at 1.6:1 and 1.7:1 for the non-hospitalised group [7].
A European study of attempted suicides established 15 catchment areas across 13 countries [36]. During 1989–1992, the average female: male attempted youth suicide ratio for all of the centres was 1.7:1, with a range from 0.9:1 in Helsinki (Finland) to 2.8:1 in Emilia-Romagna (Italy). The lowest suicide attempt rates were found in centres in Spain and Italy (which also have the lowest suicide rates), while the highest attempt rates were found in France and England. Finland also had high male attempted suicide rates and was the only country to record higher male attempted suicide rates than female.
Community samples
Schweitzer et al. [3] measured suicidal ideation and behaviours of 1678 Queensland University students, two-thirds female and one-third male. Results showed that 61.5% of the sample reported via a questionnaire to have had some ‘suicidal ideation’ in the preceding 12 months, with 11% reporting having made at least one self-destructive act. The reliance on questionnaires and wording of responses would have contributed to high positive responses. More females than males were categorised as ‘minimal level of suicidal ideation’, while significantly more males than females were in the category ‘high level of suicide ideation’ [3]. University students may not be representative of the normal population, generally experiencing better mental health than other populations of similar ages. This sample had a disproportionate number of females.
A study of 1699 students from 44 Victorian schools examined suicidal behaviour in 15–16-year-olds in 1993 [4]. Suicide attempts were determined by self-report of deliberate self-harm within the last 12 months and, as reported on the Beck Suicide Intent Scale, that they had been ‘seriously trying to end their life at that time’. Only 0.2% (n = 5) of the sample were classified as ‘true suicide attempts’, all of them female and 4% of males and 6.4% females reported deliberate self-harm. Both sexes showed a significant association between self-harming behaviour and psychiatric morbidity and sexual activity [4].
Zubrick et al. [37] surveyed students in WA high schools and found that of adolescents aged 12–16, 15% (15 500) reported suicidal ideation within 6 months of the survey. There was also twice the proportion of 15–16-year-olds as 12–14-year-olds, who reported suicidal ideation. Further, 8% (8300) of adolescents reported having attempted suicide within 6 months of the survey, with no significant differences between younger and older adolescents.
Geographical differentials
Interstate comparisons
Interstate comparisons must be approached cautiously given different recording practices. Overall suicide rates over the past 15 years have consistently been higher in Queensland and Tasmania than for Australia as a whole, with NSW having a lower rate [38].
Firearm suicides have been found to be more frequent in Tasmania and Queensland, while hanging is the most common method of suicide in the other four states [39]. Queensland and Tasmania, which had the highest firearm suicide rates, also had the highest overall suicide rates, while NSW had one of the lowest firearm suicide rates and the lowest overall suicide rates. In contrast, WA, which had the lowest firearm suicide rate, had the second highest overall suicide rate. This discrepancy was associated with a high use of vehicle exhaust as a method of suicide in WA, more than twice that of other states.
Urban–rural differences
Official data on urban–rural differences in Australia have been available since 1986 [38]. Although the number of suicides is far greater in urban areas, rural areas often demonstrate greater suicide rates. Suicide rates 1990–1992 for Australian males 15–24 years were greater in rural and remote areas that were not major population centres (Table 3). Young male suicide rates were higher than overall male rates in all areas, especially in rural and remote ‘other’ areas [40]. Suicide rates for young females suggested the same pattern as for males, but due to small numbers, these conclusions were unreliable.
Suicide rates (per 100 000) in rural and urban areas of Australia, 1990–1992
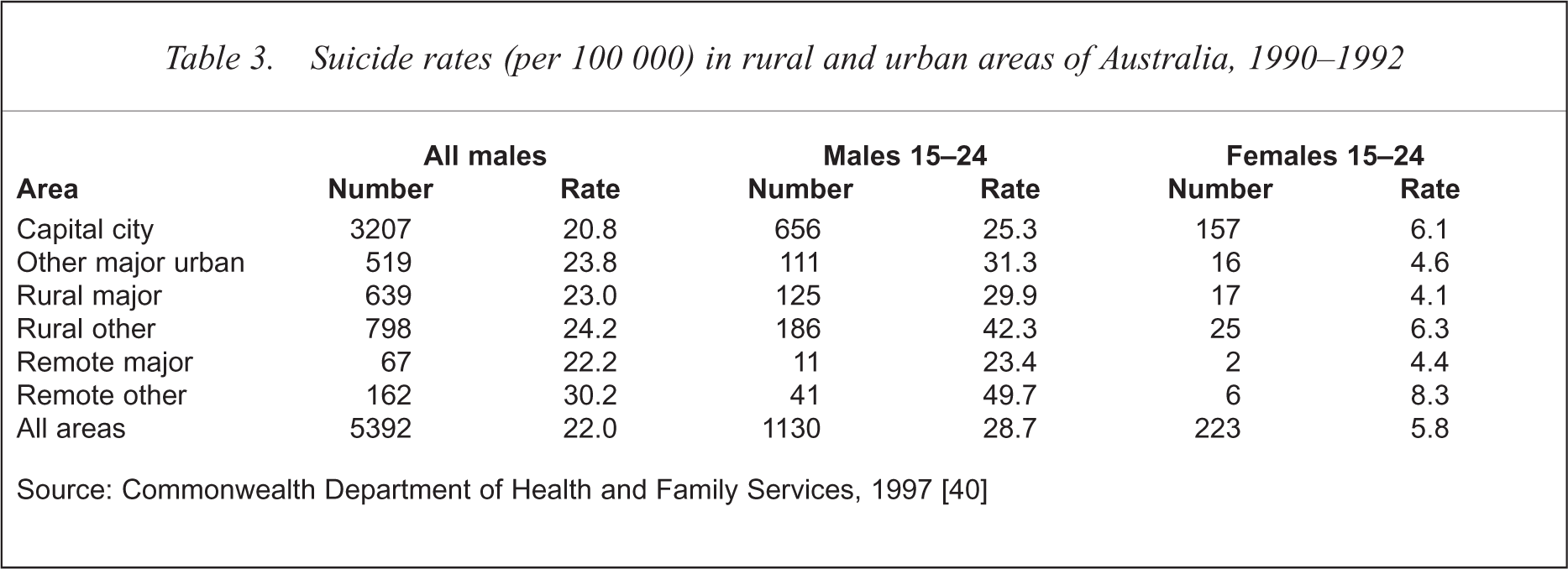
Source: Commonwealth Department of Health and Family Services, 1997 [40]
Several studies have examined urban–rural suicide rates in various states. Higher youth suicide rates were observed in rural shires and municipalities in NSW compared with Sydney and Newcastle and Wollongong, during 1984–1988 for 10–19-year-olds [41]. In Victoria, higher male youth suicide rates 1980–1990 were observed in non-metropolitan areas, compared with metropolitan areas. The youth male to female suicide ratio was 4:1 for Victoria, with a ratio of 3:1 for the metropolitan and 7:1 for the non-metropolitan areas [31]. However, neither study conducted statistical analyses to determine significance of the differences.
Subsequently, a study using Australian data revealed significant differences over time between the areas for male youth [42]. However, it was not clear where these differences lay.
A study during 1986–1990, of suicides aged 15–29 years divided Queensland into metropolitan, provincial city and rural. Rates were higher in rural areas for males and females aged 15–19, but suicide rates in rural areas were lower for 20–29-year-olds. These differences were not statistically significant [43]. Similarly, a later Queensland study of years 1990–1992 found suicide rates for males 15–29 years were highest in rural areas and lowest in the metropolitan areas, but again these differences were not significant. Female suicide rates (15–29 years) were similar in the three areas [44]. Suicide rates of males aged 15–29 in rural areas showed marked heterogeneity, with both lowest and highest rates occurring in specific rural regions. The Darling Downs, a conservative, religious and relatively affluent farming area, had the lowest suicide rates in the state. In contrast, the rural areas of the Cape York, an impoverished area, had the highest rates.
Australian Bureau of Statistics data for urban (populations greater than 20 000) and rural (less than 20 000) areas, by state for 1991–1995, found the aggregated rural suicide rate to be approximately 50% greater than the urban rate for all states and Australia [ABS: unpublished data]. Victoria had the greatest rural: urban youth suicide ratio and WA had the smallest.
Urban–rural trends
An early study of youth urban–rural trends in NSW from 1964 to 1988 found the suicide rate in Sydney, for males aged 15–19 years, had significantly increased over the 25 years, however, there had been no significant increase in the Newcastle and Wollongong areas. For the rural areas, significant increases were evident, with a doubling of the suicide rates in the rural cities and an increase of five times for rural shires and municipalities. There were no significant differences or trends found for females aged 15–19 years [41].
Subsequently, Dudley et al. [42] examined urban– rural Australian trends in ages 10–24, for the period 1964–1993. Areas were divided into metropolitan areas, cities with populations greater than 100 000 and greater than 25 000, and towns with populations greater than 4000 and less than 4000. Trends for males aged 15–24 showed significant increases in all areas, with marked increases in the town areas. Metropolitan rates doubled, while a 12-fold increase was found for towns with populations less than 4000.
Female youth suicide rates were found to show less variation over time for the metropolitan and city areas. However, a significant fourfold increase was found for small towns with less than 4000 people.
Significantly higher firearm suicide rates have been found in rural areas, for both genders. In metropolitan and provincial areas, males were found to use carbon monoxide poisoning and drugs or poisons and females to use drugs or poisons, significantly more than in rural areas [44].
In Australian towns with populations less than 4000, firearm rates for males aged 15–24 years increased 12 times, during 1964–1993, and between two and four times for larger towns and cities. Firearm suicide rates (1989–1993) were seven times higher in small towns than metropolitan areas. A significant increase in firearm suicides by males aged 15–19 living in rural shires and municipalities was found for NSW in the period 1964–1988 [41].
In conclusion, these studies suggest generally greater male youth suicide rates in small rural communities compared with non-rural areas, although this may vary between rural communities. Greater availability of firearms is the only issue convincingly demonstrated to be associated with risk for suicide [42,44]. Rural migration, unemployment, abuse of alcohol, medical service utilisation, socioeconomic status and resource deprivation are legitimate issues needing examination [42,44].
Socioeconomic differentials
Socioeconomic status
Little research in Australia has examined the relationship between socioeconomic status and suicide. Cantor et al. [45] used measures of socioeconomic disadvantage (low income and educational attainment and high unemployment) and economic resources (income and expenditure and assets of families) to determine the socioeconomic status of suicides in Queensland between 1990 and 1992 by ages 15–29, 30–54 and 55 and above years old. For both genders and all age groups a significant positive correlation was found between economic disadvantage and suicide. For the 15–29-year-old age group there was also a significant negative correlation between economic resources and suicide.
A National Health Strategy [46] study examined health and the effects which income and environment have on it, during 1985–1987 in 25–64-year-olds. The results were broadly consistent with those of the Cantor et al. study [45].
International studies produce variable findings. Studies from Sweden [47] and England and Wales [48] found low socioeconomic areas had higher suicide rates. In Canada higher suicide rates were associated with higher income [49,50], while only weak and inconsistent findings of economic stress and suicide rates in Los Angeles were found [51,52]. The impact of socioeconomic factors on suicide may be relatively culture specific.
International studies of attempted suicide have more consistently found higher rates of attempted suicides to be associated with lower socioeconomic status [53–57].
Unemployment, recessions and prosperity
Over the last 100 years in Australia, suicides peaked during the Depression when unemployment was at its highest [19,58]. Hassan [19] noted that during the stockmarket crash of 1987, suicides were significantly greater 3 months before and 6 months after the crash. High suicide rates were also found during the 1960s when the economy was at its most prosperous. These findings support Durkheim's theory that suicide rates increase when economic fluctuations, good or bad, occur.
Morrell et al. [58] examined suicide and unemployment data between 1907 and 1990 in Australia, for ages 15–64. They found that 18% of the variance in male suicides could be explained by unemployment and 11% in females. When focusing on the period when youth suicides started to increase, the unemployment rate explained 68% of the variance between 1966 and 1987, for male suicides aged 15–24. This association was not found for females.
An earlier study by Martina [59] also found a strong positive correlation between suicide and unemployment rates in Australian males aged 20–24, during 1966–1982.
Graham and Burvill [60] compared all youth suicides in WA between 1986 and 1988, with 68 older suicides aged 45–59. They found greater proportions of unemployed people in youth suicides compared with older ages.
No association was found between youth suicide and youth unemployment in Victoria during 1907–1990, noting that a recent substantial increase in youth unemployment was not matched by an increase in youth suicide [31]. However, for the period 1983–1989, a significant correlation for males, but not females was found.
A study which contradicts these findings compared suicide and unemployment rates in Australia and the USA [61]. Between 1946 and 1984, for all ages, unemployment rates were significantly related to suicide rates in the USA, but not Australia. However, they did not examine youth separately, and they used a time period 20 years before those studies yielding different results.
A study of suicidal ideation and unemployment in Australian youth also failed to show a significant association [62]. International studies of attempted suicide have shown significant relationships, with attempted suicide ratios of up to 15:1 for unemployed: employed people [63–66].
Overall, most research seems to indicate a positive relationship between unemployment and youth suicide rates in Australia for males, especially those aged 20–24 years. However, no causal relationship can yet be attributed to unemployment and suicide. The reasons why a person becomes unemployed (e.g. mental illness) could account for why they committed suicide.
Occupational prestige
Hassan [19] examined the relationship between type of occupation and suicide rates in Australia for 1986. For 15–24-year-old males, suicide rates were significantly higher in blue-collar occupations and in professional/technical occupations.
Mathers [67] examined occupational prestige and suicide in males aged 25–54, in 1985–1987. An inverse relationship was found with suicide rates in the least prestigious jobs being two times greater than those in the most prestigious occupations.
Marital status
Marital status has attracted surprisingly little attention in the suicide literature, internationally and in Australia. International studies have reported a positive association between divorced status and suicide rates [68–72].
The Australian Bureau of Statistics [38] reported suicide rates of Australians aged 15 years and over for 1982–1992; over 20 000 suicides recorded and accurate figures for total Australian populations lend confidence to their rates. Married status was associated with the lowest suicide rates. Divorced and widowed males had rates three times the married rate. Divorced female suicide rates were 3.6 times the married rate and widowed female rates were 2.2 times the married rate.
Legal definitions of marital status allocate separated persons (those potentially at greatest risk of suicide) to the married category (those at lowest risk). Cantor and Slater [73] examined 1375 suicides between 1990 and 1992 via the Queensland Suicide Register. Their findings for never-married, married, divorced and widowed males and females were in keeping with ABS [38] Australian findings. However, the standardised mortality ratios of separated males were 6.2 times the married rate (p < 0.05), but separated females only 1.7 times greater (p > 0.05). Within the separated male category, males aged 15–29 had suicide rates of approximately 150 per 100 000 (higher than older ages). Divorced males aged 15–29 had a suicide rate of approximately 40 per 100 000 suggesting that marital dissolution (as opposed to status), may play a causative role generating suicide.
In an exploration of the contribution of parenthood to protectiveness against risk for suicide, a linear decline in suicide rates of females with greater numbers (up to six) of children was found [73], although an alternative explanation is that factors promoting suicide might inhibit having children. This finding concurred with a prospective study of 1 million females in Finland in 1970–1985, who generated 1190 suicides [74]. Large numbers of children were associated with vulnerability to suicide if children were born to particularly young or old parents. Larger families may be associated with high rates of stress and depression [75]. However, larger numbers of offspring may be protective against suicide by promoting identity as a parent, fostering personal responsibility to offspring and providing reasons for living [76]. Certain religions, such as Catholicism and Islam, confound this issue by their taboos on both contraception and suicide.
Methods of suicide
Changing rates of methods of suicide
During 1974–1994, hanging rates rose for Australian males from two to nearly 10 per 100 000 with the sharpest rise around 1986–1987. In the mid-1980s there was also a rise in motor vehicle exhaust gassings with male rates rising from around 2–4 per 100 000 in 1994. These two methods amounted to a rise in young male suicide of 10 per 100 000, which was partially offset by a decline in firearm suicides (by approximately 4 per 100 000) from the mid-1980s. This leaves an overall rise from these three methods of 6 per 100 000. These constitute the leading methods of suicide for young males [39].
Changes for young females show partly similar trends. Rates of hanging and vehicle exhaust gassing have risen significantly. However, since 1974, suicides by solids and liquids declined substantially in females, from around 2.5 to 1 per 100 000 in 1994 [39].
Availability and acceptability
Both availability and sociocultural acceptability determine choice of method of suicide [19,77–80]. Marzuk et al. [81] compared five counties in New York whose populations had similar access to some methods (e.g. hanging), but different access to jumping from heights, drowning and carbon monoxide. Counties had similar suicide rates for equally accessible methods, but different rates for methods that were differentially accessible. Counties with more tall buildings had more suicides by jumps, and those with more private garages had more suicides by exhaust gas. Clarke and Lester [77] have listed the key factors influencing method choice, with 19 of 20 items having more to do with acceptability than availability.
In a review of the evidence on limiting access to means of suicide, considerable evidence supported an association between method availability and method-specific suicide rates [39]. A substantial, but lesser amount, of evidence supported the notion that restrictions on method availability decreased method-specific suicide rates. Modest support was found for restrictions on method availability reducing overall suicide rates.
Drug overdoses
A major rise in fatal self-poisonings in Australia occurred in the early 1960s relating to barbiturates. In the late 1960s better prescribing practices, legislative restrictions on barbiturate prescribing and substitution of safer benzodiazepines resulted in a major decline in suicides by overdose, especially in females for whom drug overdose constituted the leading method of suicide [21].
Certain drugs have been found to be used more frequently for overdoses. Some of these were associated with greater toxicity. In particular, barbiturates, chloral hydrate, tricyclic antidepressants, dextropropoxyphene, calcium channel blockers, colchicine, opioids and illicit drugs were associated with disproportionate mortality. Benzodiazepines were over-represented in those reaching hospital, but not among those who died [82–85].
Potential approaches to limiting suicides by overdoses include [39]: (i) safety packaging and limited tablet quantity per packet (especially over the counter analgesics); (ii) limited prescription size and frequency; (iii) limited tablet strength for high risk drugs such as tricyclics; (iv) education of practitioners regarding safer practices, though there is little evidence supporting its efficacy [84]; (v) disposal of out-of-date and unwanted drugs; (vi) limiting advertising, especially that aimed at the young.
Domestic gas
In Britain, detoxification of domestic gas coincided with a substantial decline not only in suicides by this method, but also in overall suicide rates [77,86]. However, Burvill [30] suggested that although the introduction of non-toxic domestic gas in Australia lead to a decline in suicide by this method there was a compensatory increase in suicide by motor vehicle exhaust gas.
Motor vehicle exhaust gas
As car ownership has risen, there has been a rise in the use of exhaust gas for suicide [87]. Federal emission control standards introduced in the USA in 1968 led to a considerable reduction in carbon monoxide content of exhaust gas [88], which was followed by an increase in failed suicides and a decrease in successful suicides by this method [89]. Statutory introduction of catalytic converters in all new cars in the European Community from 1993 [90] has yet to be evaluated.
In Australia, Routley [91] reported that prior to the introduction of modest emission controls in 1986, exhaust suicides were increasing. In the subsequent years up to 1992 no change was detected. However, Victorian hospital admissions for carbon monoxide suicide attempts increased from 15 in 1989–1990 to 56 in 1993–1994 [92] and to 95 in 1994–1995 [93].
In Australia, catalytic converters to date have functioned inefficiently until the engine has warmed up, making suicide with a cold engine easy [94]. Over time, the condition of catalytic converters may deteriorate and car engines may require tuning. Further, the pollution performance of 4–9-year-old cars has been found to deteriorate faster than that of older cars [95]. Between 1976 and 1991 exhaust gas suicides increased at a faster rate than motor vehicle registrations suggesting that, not only availability, but acceptability issues operated.
Hanging
Despite significant increases in suicides by hanging in Australia [39,41] and the UK [96–98], minimal research attention has addressed causation. Hanging points and available materials have been universally available throughout history. Change in cultural acceptability must be the key issue [39]. Pounder [98] speculated that in the UK, hanging may have risen with the demise of capital punishment in 1965 removing previous stigma. There has been speculation in Australia that rises in hangings may have followed publicity associated with the inquiry into Aboriginal deaths in custody.
Firearms
Dudley et al. [99] have comprehensively reviewed firearm suicide in Australia. A link between firearm availability and firearm suicides in Australia has been demonstrated [41,100,101]. Between 70 and 80% of firearm-related fatalities in Australia are due to suicide [102,103]. Queensland and Tasmania historically have been the states with the least restrictions on firearms and have had higher overall suicide rates and a greater proportion of all suicides committed by firearms [100].
The firearm suicide rate in South Australia decreased after restrictions were introduced in 1980. This decline was minor and was also noted in states where no legislation had been introduced, suggesting the operation of factors other than gun laws, such as attitudinal change [101]. A preliminary analysis of firearm suicide rates in Queensland immediately preceding and following the introduction of the Weapons Act, 1990, found that mean annual firearm suicide rates declined significantly in metropolitan and provincial city areas after legislation especially in males aged 15–29 [104]. A 28-day ‘cooling off’ period may have been a factor. There were no declines in firearm suicides in rural areas where firearm suicide rates and ownership were greatest.
Jumping from heights
The suicide rate by jumping from high places for 15–29-year-olds is modest, around 1 per 100 000 [39]. A small series of suicides by jumping from multistorey car parks in Adelaide suggested an association with psychosis [105,106]. Subsequently, a study of 63 jumps from Brisbane river bridges, found that 46% had previously been diagnosed as suffering schizophrenia [107]. These subjects had extensive histories of previous self-harm. Studies from countries where high-rise living is more widespread have suggested lower proportions of jumps by psychotic persons [108].
Suicide in indigenous populations
Suicide was uncommon in traditional Aboriginal culture [109–114]. Studies of suicide rates in Aboriginal populations are summarised in Table 4 and highlight the lack of adequate studies. Collecting accurate information on Aboriginal suicide has been difficult due to remote communities, unsystematic recording procedures and with Aboriginal people defining aboriginality by identification with aboriginal culture as opposed to the Western orientation to genetics.
Historical perspective on Aboriginal suicide
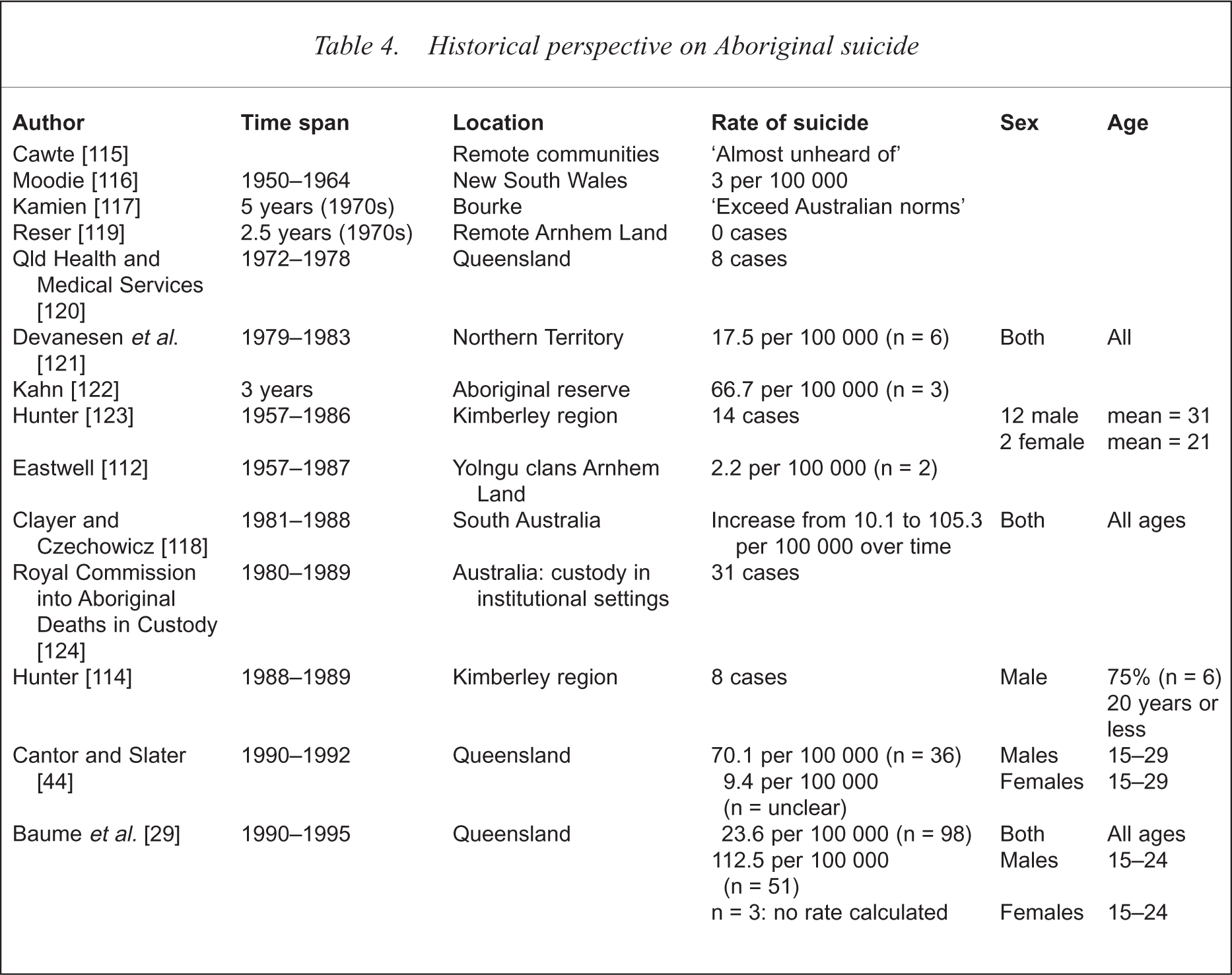
Studies prior to the Royal Commission tended to find little or no suicide [115–117]. This contrasts with recent high rates [44,118].
An examination of SA coronial records, 1981–1988, found increases in non-Aboriginal suicide rates from 11.2 to 17.4 per 100 000, and an increase in Aboriginal suicide rates from 10.1 to 105.3 per 100 000. A total of 71.4% of Aboriginal suicides were under age 29, compared with 34.8% of non-Aboriginal suicides. Rural SA Aboriginal suicide rates were slightly lower than urban rates. Female suicide rates were higher for Aborigines than non-Aborigines [118].
A recent Queensland study yielded the biggest sample size to date [29]. A conservative estimate of the overall indigenous rate was 23.6 suicides per 100 000, compared with 14.5 per 100 000 for Queensland. Eighty-eight of 98 indigenous suicides were male and 75 of the 88 were aged under 35. The indigenous 15–24-year-old suicide rate for males was 112.5 (vs 30.9 for all of Queensland), with female numbers too small to calculate rates. The mean age of indigenous suicides (26.3 years) was significantly younger than for Queensland as a whole (41.4 years). Yarrabah and Palm Island in Queensland were identified as communities with higher than expected numbers of suicides.
International studies
Studies of North American and Canadian indigenous populations [125] have shown similar findings to those of Australia. In New Zealand, male suicide rates for 15–19-year-olds were greater in Maoris (35 per 100 000) than non-Maoris (27 per 100 000). For males aged 20–24 the trend was reversed with non-Maoris (49 per 100 000) having the greater suicide rate than Maoris (38 per 100 000). The small population limits the significance of these variations [126].
Suicide in migrant populations
Research on migrant suicides was more prolific during the 1960s and 1970s, when European immigration was dominant, than in the recent era of Asian migration. Early studies found rates of suicide [127–129] and attempted suicide [130] for migrants were greater in Australia than in their country of birth, as well as greater than Australian-born rates. More recent studies found correlations between migrant suicide rankings and the rankings of their countries of birth, with western and eastern European countries having higher suicide rates and southern European countries lower rates [131,132]. Similarly, suicide rates were higher in migrants from Oceania and western and eastern Europe and lower in southern Europe and Asia than in Australian-born [38].
Methods of suicide used by migrants from English-speaking and western European countries were found to be more similar to Australian-born residents, while non-English speaking migrants used methods more similar to those used in their countries of birth [127–129,133]. Suggestions of greater integration for migrants from English-speaking countries and more distinct ethnic groups for non-English speaking migrants have been made. The hypothesis that migrant suicide rates would become more like those of Australia over time was not supported by evidence [19,128,133].
Most of the migrant studies have not considered youth suicide, and where they have, different migrant groups have not been separated (often due to small samples), obscuring the possibility that some migrant youth may have higher suicide rates than Australian-born and others lower. A recent NSW study conducted on suicide in migrants aged 15–24 from 1970 to 1992 found a similar profile to that above for all ages [131].
Suicide in custody
Of 635 Australian deaths in custody in 1990–1997 (all custodial settings), 245 were suicides, with 74% by hanging and 14% by firearms. Eighty-five (35%) were aged 15–24 years [Dalton V: personal communication].
From 1980 to 1997, suicide was the cause of 67% of prison deaths in persons aged 17–30 years, but only 21% in those over 40 [134]. The mean ages of indigenous and non-indigenous people dying in prison was 31 and 36, respectively. New South Wales data indicate that the suicide rate in prison is about three times the community rate [135].
Aboriginal suicide in police custody
Following public concern regarding Aboriginal suicide rates in late 1986 and 1987, the Royal Commission into Aboriginal Deaths in Custody was instituted in December 1987. The Commission investigated deaths in custody since 1980. Accurate recording of such events was unsystematic prior to the Royal Commission.
The Royal Commission's inquiry into Aboriginal suicides in police custody established that 93% were males, and 57% were under age 30. Of these younger people, 66% were aged 15–19, all were alone and committed suicide by hanging [113].
An increase in suicides in police custody in 1987 was attributed to the hanging of a North Queensland Aboriginal man in police custody at Yarrabah Watchhouse, in December 1986 [136]. Although clustering and media coverage have been suggested as possible explanations for the sudden increase in Queensland suicides in custody in 1986–1987, clustering was not evident in WA during this time [136–138].
In Australia, Aborigines comprise less than 2% of the population, yet account for 30% of those in police custody, and 15% of the prison population [119]. In 1995, 4 years after the Royal Commission's report, almost 25% of the 86 deaths in custody involved Aboriginal people. While Aboriginal people are over-represented in custodial settings, their suicide rates in custody tend to be similar to non-Aboriginal persons.
Suicide attempts in custody
A survey of suicide attempts in Longmore Remand Centre in WA, found Aboriginal adolescents were less likely to attempt suicide than non-Aborigines [139]. Those on remand for longer than 7 days appeared most at risk, contrasting with adult suicides in custody which are most likely to occur within hours of incarceration. Aborigines accounted for 45% of the adolescents in Longmore, a 15 times overrepresentation. Kosky et al. [140] noted ‘extraordinarily high scores on the alcohol- and other drug-use items’ of the Youth Self-Report in young suicide attempters at a remand centre in SA.
Gay and lesbian
High-quality studies of suicidal behaviour in young homosexual people are difficult to conduct because data on sexuality are sensitive and not routinely collected. Consequently, studies have tended to focus on attempted suicides and suicidal ideation, bringing problems with unrepresentative sampling and reliance on self-reports. A report conducted for the Young Lesbian Support Group investigated suicide attempts and ideation in 200 Australian lesbians aged 14–25 years [141]; 47.5% reported having made a suicide attempt at some time in their life, with 31% of attempters indicating it was because of their sexuality. Similarly, prior suicidal ideation was common, but attributed to sexuality in less than 50%.
A USA study compared suicidal ideation, intent and attempts in homosexual and bisexual with those of heterosexual students in grades 7–12 [142]. A total of 336 subjects identifying themselves as homosexual or bisexual were gender-matched to 336 heterosexual subjects. Homosexual or bisexual males were significantly more likely to report suicidal intent and attempts than heterosexual males, but no significant differences were found for females. A study of 4159 students in grades 9–12 from 59 Massachusetts public high schools, found that suicide attempts were reported by 36% of students who identified themselves as homosexual, bisexual or having had same-sex sexual contact, compared with only 8.9% of suicide attempts in the others [143].
Future research priorities
Data systems deficiencies
Suicide research could be greatly facilitated by the setting up of a detailed national suicide data system. Such systems' changes would include uniformity of definitions and procedures across all states and territories and should apply across all ages.
Hospital suicide or suicide attempt definitions and procedures are similarly in need of change. Detailed exploration of the feasibility of setting up a national attempted suicide data system is needed.
Research priorities
Limited and generally poor quality data suggest that young indigenous males may be greatly at risk of suicide, but data are deficient.
Studies of suicidal behaviour in older age groups are essential. There is no dispute that youth are the correct priority group, but the needs of older ages, which include those aged 25 and over, are great and there is a danger of age discrimination if youth priorities overlook other ages.
Subgroups of young people need to be examined including children under 15 years of age.
Much could be learnt about risk and protection issues by simple studies exploring gender issues. Gender issues are multiple, but include violent behaviour, lethal methods, approaches to problem solving and help seeking, caregiver responses, diagnostic issues, support networks and more.
Suicide research examining marital status, interpersonal, parenthood and other attachment issues has received little attention, despite clinicians being aware of the importance of interpersonal issues both in generating protectiveness against suicide and in fuelling suicidal behaviour.
Acknowledgement
This report was funded by a grant from the National Health and Medical Research Council.