
Abstract
In 2000 the Australian Federal government published a national survey of the mental health of 4500 children and adolescents [1]. The results showed that, of those sampled, 14% of children and 19% of adolescents scored above the recommended cut-off (i.e. in the clinical range) on one or more of the mental health problem areas assessed. More recent statistics suggest that an estimated one in five children and adolescents is likely to suffer from a mental health problem before the age of 24 [2]. Based on these figures, and with a current population of >10 000 deaf children and adolescents in Australia [3], it is possible that >2000 deaf children and adolescents are likely to have some form of mental health problem before reaching adulthood. Recent Australian and international studies investigating the prevalence of mental health problems in deaf children and adolescents, however, indicate that upwards of 40% have significant emotional, behavioural and attentional problems [4–9]. This has important implications for deaf children and adolescents in terms of social and academic functioning and overall quality of life.
There is considerable heterogeneity in the deaf child and adolescent population with respect to type and degree of hearing loss, preferred mode of communication, and type of schooling. In Australia the majority of deaf children and adolescents have acquired mild to moderate hearing loss [3], communicate using spoken English [10], and attend inclusive educational settings [11,12]. One of the difficulties, therefore, in establishing a prevalence rate of mental health problems for the deaf child and adolescent population is accounting for this heterogeneity. In fact, similar to the hearing population, it seems that there may be a range of prevalence rates applicable to the deaf child and adolescent population depending on the demographic characteristics of the sample studied. For instance, Cornes et al. investigated mental health problems in deaf adolescents who communicate using Australian Sign Language (Auslan) attending either a bilingual/bicultural school for the deaf or a class for the deaf children in mainstream schools [4]. Using a validated translated version of the Youth Self-Report (YSR) the overall prevalence rate of mental health problems (42.6%) was higher than that of the Australian hearing adolescent population (18.9%). It would be interesting to establish if prevalence rates are different for deaf children and adolescents who are placed in bilingual/bicultural programs compared to those deaf children and adolescents who are supported in mainstream education. Unfortunately no Australian data have been published in this area as yet.
In recent years there have been numerous Australian Federal and State government initiatives surrounding mental health and social emotional well-being of children and adolescents but to date few have focused specifically on the mental health problems of special populations. In 2008 a pilot project, funded by Melbourne Graduate School of Education at University of Melbourne, was undertaken to investigate the mental health of deaf children and adolescents in Western Australia [13]. This project aimed to fit within current government initiatives with a specific focus on the deaf child and adolescent population to better inform health and education professionals working within this population. This paper presents an overview of the key findings from the project, including the demographic characteristics and prevalence and nature of mental health problems in the study sample.
Method
Participants
At the time of recruitment there were 1244 deaf children and adolescents aged 6–18 years enrolled in one of the two educational organizations servicing deaf students in Western Australia. A pool of 120 deaf children (6–11 years) and 120 deaf adolescents (12–18 years) were selected by senior leadership staff of these organizations and invited to participate in the study. The selection of invited participants was based on an even distribution related to age cohort (child and adolescent), gender (male and female) and degree of deafness (mild–moderate, moderate–severe, and severe–profound). The parents of 66 (28%) gave informed consent for inclusion in the study. The participants included 66 parents: 28 of deaf children (10 male, 18 female) and 38 of adolescents (16 male, 22 female), their teachers of the deaf (66) and 38 deaf adolescents. Incomplete or missing data obtained from one parent, one teacher and three deaf adolescents were removed and not included in data analyses. All other participant data obtained (n = 65 parents; n = 65 teachers; n = 35 deaf adolescents) were complete and used in the data analyses.
Instruments
Mental health problems
The Child Behaviour Checklist (CBCL) [14], YSR written version [14] and YSR Auslan signed version [4] were used to assess adaptive functioning and emotional and behavioural problems as reported by parents and adolescents, respectively. The CBCL and YSR are integrated forms that ask parents and adolescents to reflect on the past 6 months and provide ratings for items related to emotional and behavioural functioning (CBCL = 113 items; YSR = 112 items). Items are rated as either 0 = true, 1 = somewhat or sometimes true, or 2 = very true or often true. Three problem scale (Total Problems, Internalizing Problems, Externalizing Problems) and eight syndrome scale (Anxious/Depressed, Withdrawn/Depressed, Somatic Complaints, Social Problems, Thoughts Problems, Attentional Problems, Rule-breaking Behaviour, Aggressive Behaviour) scores can be derived from CBCL and YSR ratings. In the hearing population, the CBCL and YSR are considered to be valid and reliable instruments that assess child and adolescent mental health [14], and although they are both widely used with deaf children and adolescents there is no specific information related to their psychometric properties for use with this population [9,15].
The YSR signed version is an Auslan translated version of the YSR written version presented in a CD-ROM format, which allows adolescents to view and respond to items via a PC or laptop computer. It contains an introduction to the YSR including instructions on how to respond to items, and presents all 112 items of the YSR written version in Auslan presented by an accredited Auslan interpreter. The YSR Auslan signed version has been shown to be a valid and reliable instrument for use with deaf adolescents for whom Auslan is the preferred language [4].
In the present study CBCL and YSR problem and syndrome scale scores within the clinical range (>97th percentile) were considered to reflect a mental health problem.
Demographic characteristics
A parent survey and a teacher survey were used to obtain information from parents and teachers regarding the audiological (age of diagnosis, cause of deafness, degree of deafness, type of listening device), educational (level and type of support, use of additional support services) and health background (physical health, other disabilities, mental health) of the child or adolescent and information regarding family background and related characteristics (type of household, preferred language of household, household income, parent occupation, parent education) [13]. In relation to any pre-existing mental health characteristics, parents were asked two questions specific to the current mental health of their child or adolescent. These were: ‘Has your child had emotional and/or behavioural problems in the past?’ and, if so ‘Did you child receive specialist support services related to these emotional and/or behavioural problems?’ In addition to these two questions teachers were also asked: ‘Did the child receive specialist support or services from a professional with qualifications and/or experience in working with deaf children and adolescents?’ Responses from parents and teachers to these questions were analysed and included in the results.
Procedure
The study was approved by the Human Research Ethics Committee of the University of Melbourne and was also granted approval by the Western Australian Institute for Deaf Education, Department of Education and Training Western Australia, and Telethon Speech and Hearing. Participants were recruited by a third party on behalf of the researchers to ensure privacy and confidentiality. No inclusion or exclusion criteria were applied in the recruitment of participants. Prior to completion of any project documentation, informed consent was first obtained by parents. Parent participants received via the deaf educational service currently supporting their child a project information package containing detailed information about the project, a copy of the CBCL and parent survey, and a consent form. Adolescent participants were also then approached to give informed consent. These participants received a project information package from their teacher of the deaf containing easy-to-understand information about the project, a consent form and a copy of the YSR. Adolescents for whom the preferred language was spoken English received a copy of the YSR written version in their project package, while adolescents for whom the preferred language was Auslan were shown the YSR signed version on a laptop computer with assistance from an Auslan interpreter. Administration of the YSR (written English and Auslan signed versions) was completed in a quiet room located within the adolescent's school supervised by their teacher of the deaf. Teachers of the deaf and interpreters could respond to questions about the YSR that clarified vocabulary and meaning but were instructed not to assist the adolescent with their responses. It is important to mention that there were no reports of any adolescent participants having difficulties in reading, understanding or completing the YSR (both written English and Auslan versions).
Results
Mental health problems
Table 1 lists the prevalence of mental health problems for deaf children and adolescents as reported by parents on the CBCL. Although there were no significant differences between the two groups it is interesting to note that parents of deaf adolescents reported overall more internalizing problems, and in particular anxious/depressed and somatic complaints, than did parents of deaf children.
Prevalence (%) of mental health problems in deaf children and adolescents as reported by parents on CBCL
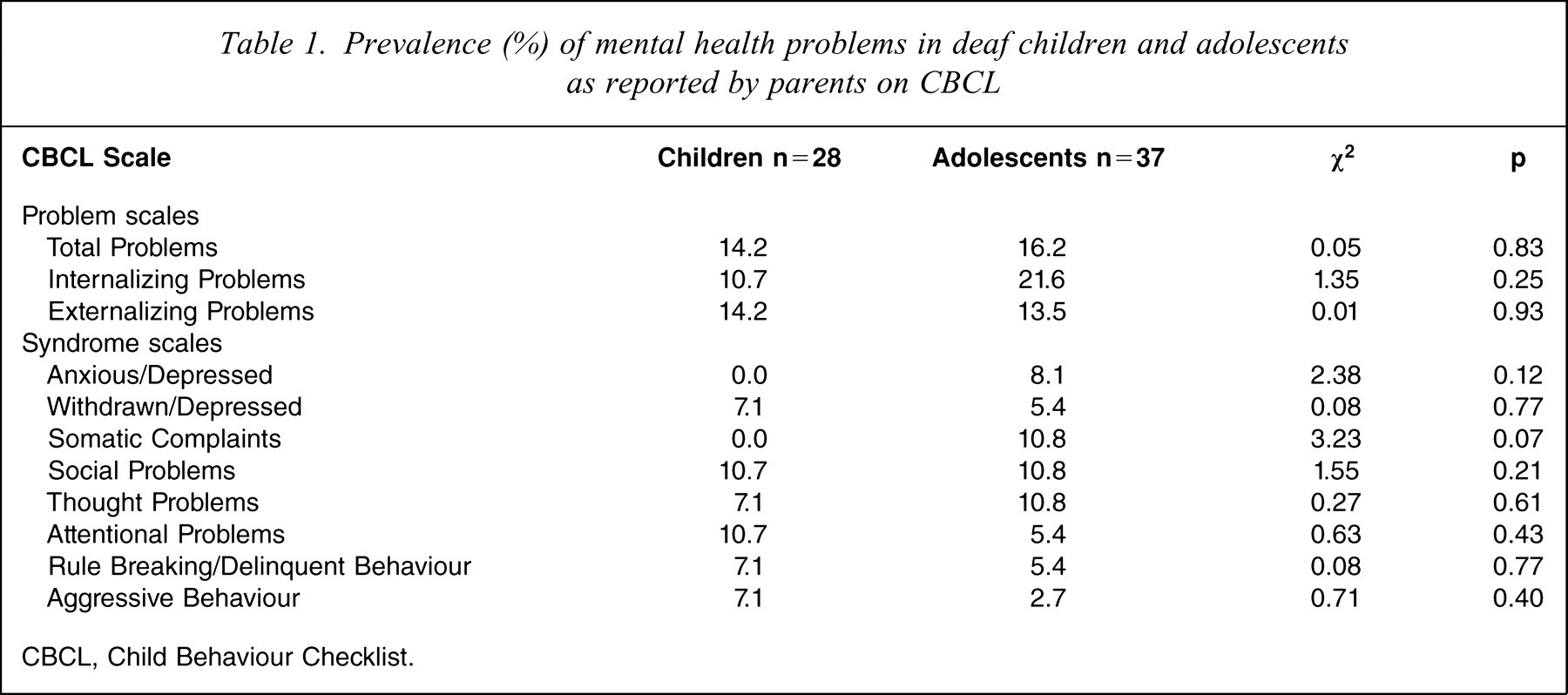
CBCL, Child Behaviour Checklist.
The prevalence of mental health problems as reported by parents on the CBCL as compared to Australian hearing 6–17-year-olds [16] is presented in Table 2. Overall, there is a similar prevalence rate of mental health problems between the deaf children and adolescents in the present study when compared to hearing children and adolescents. There was, however, a significantly higher prevalence of social problems and thought problems among deaf children and adolescents when compared to their hearing peers.
Prevalence (%) of mental health problems in deaf and hearing children and adolescents as reported by parents on CBCL
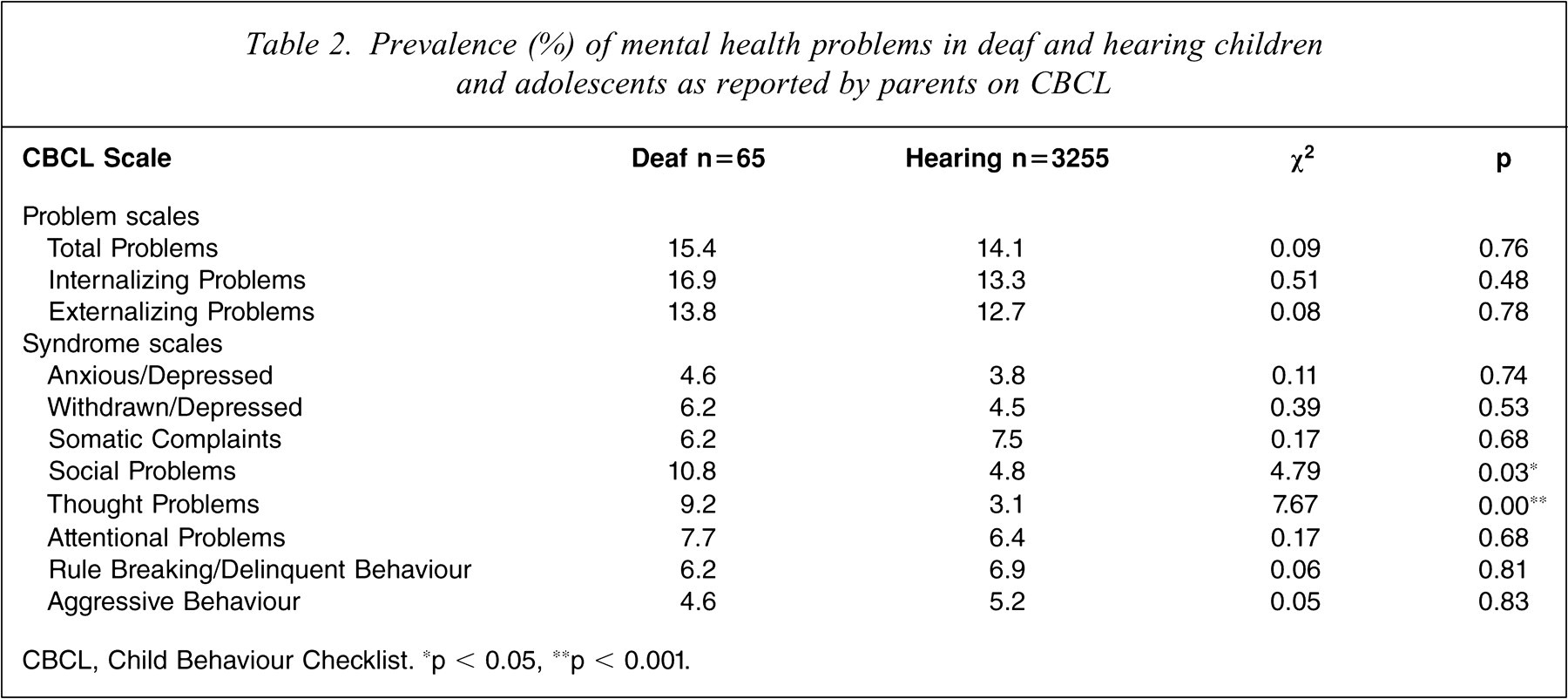
CBCL, Child Behaviour Checklist. ∗p < 0.05, ∗∗p < 0.001.
Table 3 lists the prevalence of mental health problems as reported by adolescents on the YSR in the present study as compared to Australian hearing adolescents [1] and Australian deaf signing adolescents [4]. While there were no statistically significant differences in the prevalence rate of mental health problems between hearing adolescents and the deaf adolescents in the present study there were some noticeable differences with regard to a higher prevalence of externalizing problems (rule breaking/delinquent and aggressive behaviour) reported by hearing adolescents.
Prevalence (%) of mental health problems in deaf and hearing adolescents as reported by adolescents on the YSR
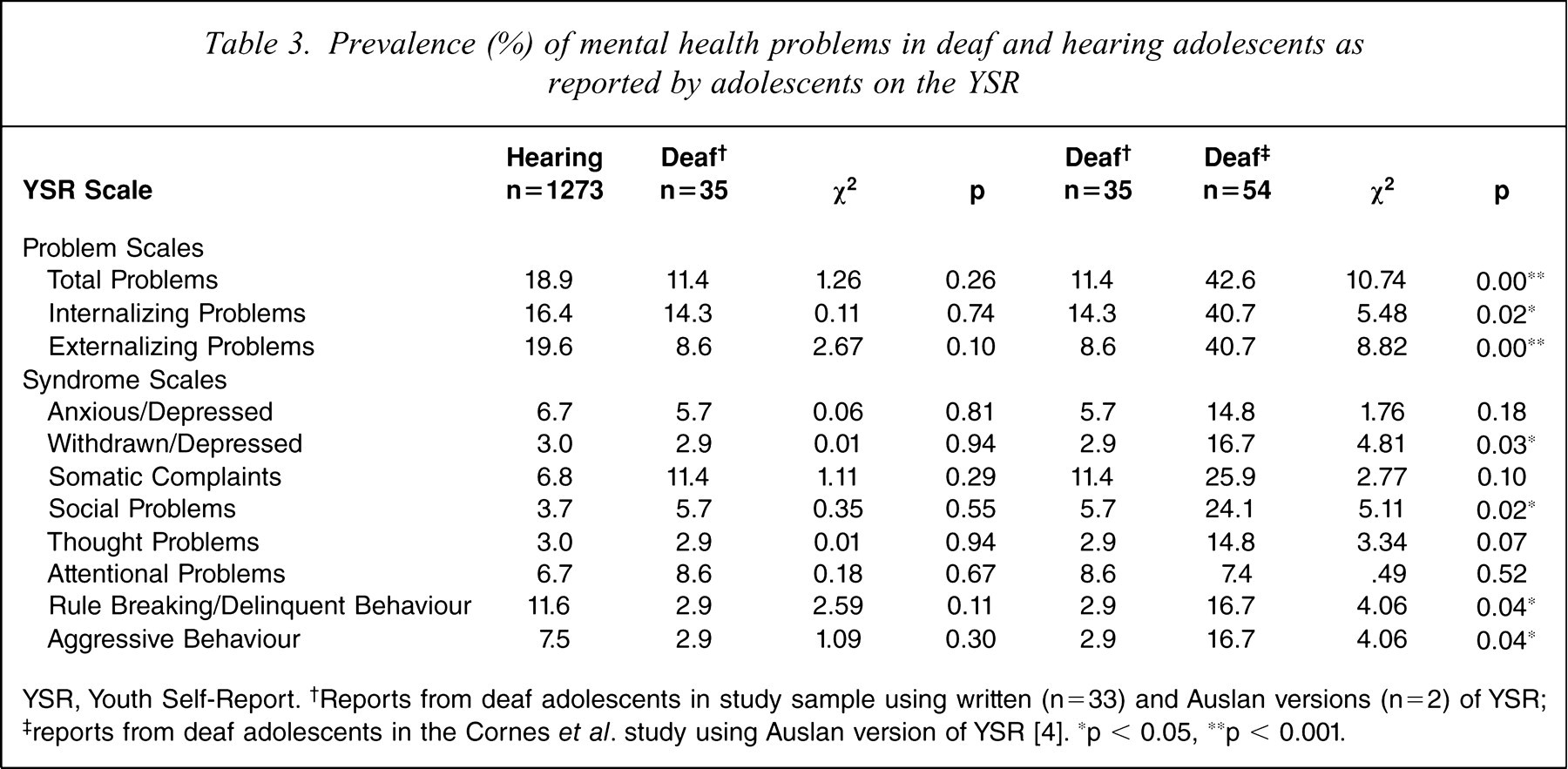
YSR, Youth Self-Report. †Reports from deaf adolescents in study sample using written (n=33) and Auslan versions (n=2) of YSR; ‡ reports from deaf adolescents in the Cornes et al. study using Auslan version of YSR [4]. ∗p < 0.05, ∗∗p < 0.001.
When comparing the prevalence of mental health problems for the deaf adolescents in the present study and those of deaf signing adolescents there some noteworthy findings. Specifically, there was a significantly higher prevalence of total problems, internalizing problems, externalizing problems, withdrawn/depressed, somatic complaints, rule breaking/delinquent and aggressive behaviour for deaf signing adolescents than for the deaf adolescents in the present study. It is important to mention that the two deaf signing adolescents who participated in the present study who completed the YSR signed version did not obtain clinical scores on any problem or syndrome scale scores on either the YSR or CBCL.
Demographic characteristics
The demographic characteristics of child and adolescent participants in the study sample as reported by their parents are given in Table 4. In relation to general physical health and well-being the majority of parents reported their child to be in very good to excellent health. Of the remaining parents, most reported their child to be in good health, with only one reporting their child to be in poor health. Approximately one-third of parents in each of the age cohorts reported the presence of a physical health condition or problem. Of those reported, asthma was the most common, followed by epilepsy. Other problems and conditions reported include arthritis, cleft palate, kidney problems and migraines. In comparison to adolescent participants, significantly more child participants were reported as having had a late diagnosis of deafness (>18 months of age) and, although not statistically significant, a large proportion of these were diagnosed with mild–moderate deafness. Spoken English was the most common mode of communication for both age cohorts. Other communication modes included Auslan (3.0%) and spoken and signed English (4.6%). Most participants attended inclusive educational settings with only a few notable exceptions attending either a deaf unit, education support centre or undertaking an apprenticeship. In relation to the presence of an additional disability significantly more child participants than adolescent participants were reported by parents as having more than one additional disability or disorder. The most commonly reported additional disabilities for both child and adolescent cohorts were speech language impairment, visual impairment, developmental delay and learning disability. More than one-third of child participants and almost half of the adolescent participants received a written referral for follow up following their participation in the project.
Demographic characteristics of deaf children and adolescents
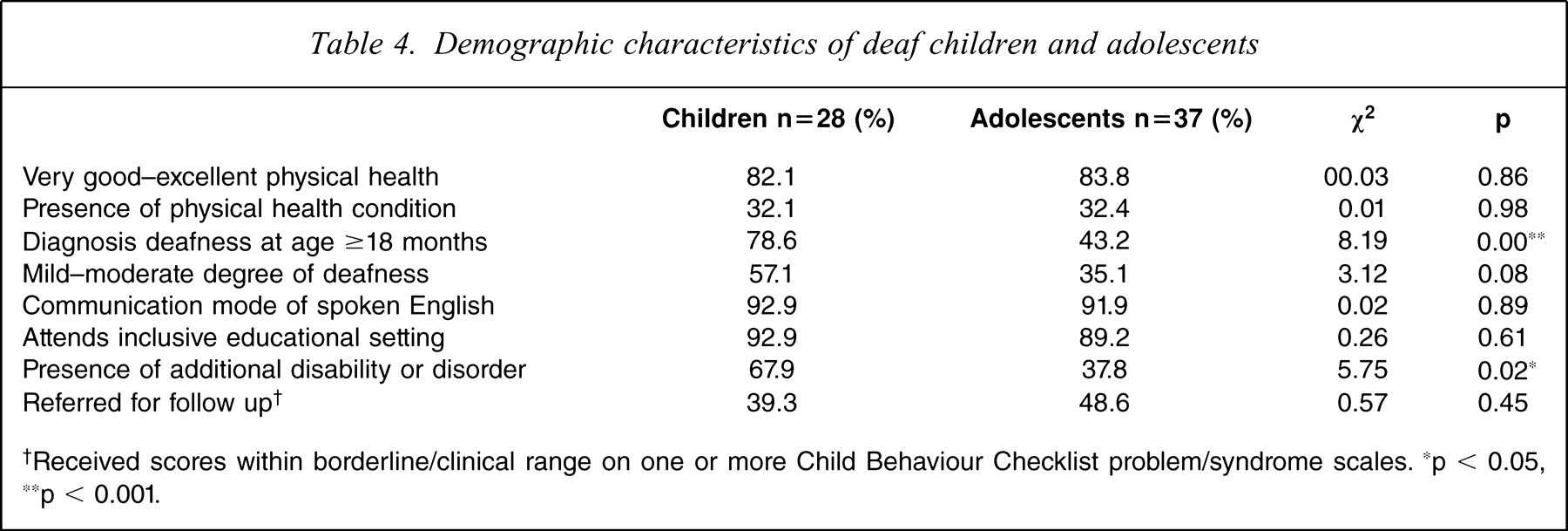
†Received scores within borderline/clinical range on one or more Child Behaviour Checklist problem/syndrome scales. ∗p < 0.05, ∗∗p < 0.001.
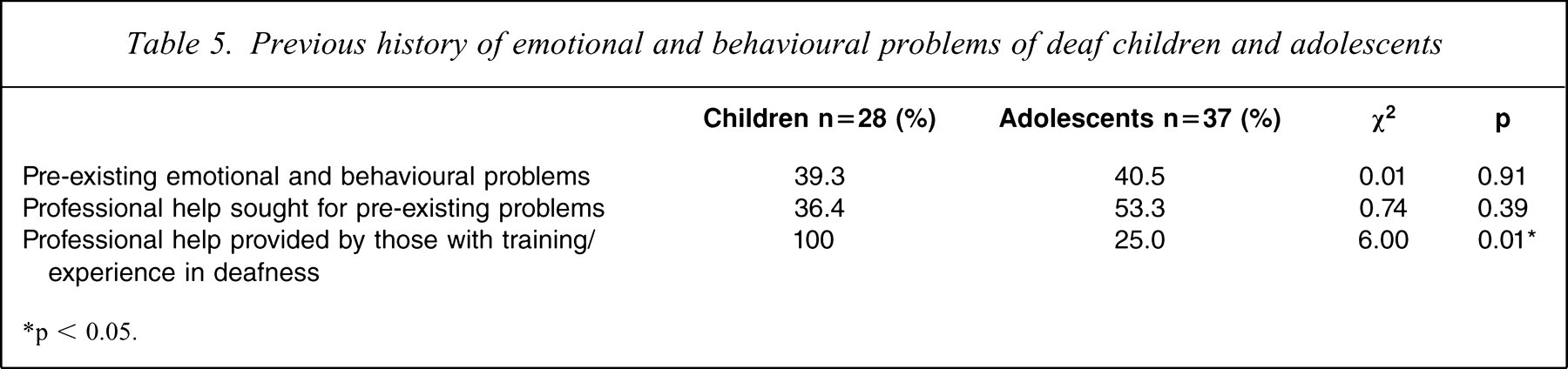
Table 5 lists the previous history of emotional and behavioural problems of child and adolescent participants as reported by their parents and teachers. Although a similar number of child and adolescent participants were reported as having pre-existing emotional and behavioural problems, only one-third of child participants and approximately half of the adolescent participants sought professional help for these problems. Interestingly, the professional help sought for child participants involved solely those with training or experience in the deafness area, whereas the majority of professionals involved with adolescents had no training or experience. Parents and teachers reported that professional help was sought from a range of professionals including general practitioners, psychiatrists, clinical psychologists, school counsellors, and school psychologists. The professionals reported as having specific knowledge, training or experience in working with deaf children and adolescents were psychologists employed by an independent educational organization for deaf children and adolescents.
Previous history of emotional and behavioural problems of deaf children and adolescents
∗p < 0.05.
Discussion
In recent years there have been several Australian Federal and State government initiatives and research programmes launched to investigate the mental health of young Australians. Few, if any, of these initiatives have specifically targeted special populations, such as the deaf population. In 2008, however, Melbourne Graduate School of Education at the University of Melbourne in conjunction with the Western Australian Institute for Deaf Education and Telethon Speech and Hearing conducted a survey of the mental health of young deaf West Australians [13]. The principal objective of that pilot project was to identify the prevalence and nature of mental health problems and what, if any, characteristics typify deaf children and adolescents with mental health problems. Another objective of the project was to obtain information that could provide a context and rationale upon which to launch further research, with a nationwide focus, investigating the mental health of deaf children and adolescents.
The results have shown that, according to parent report using the CBCL, the prevalence and nature of mental health problems in deaf children and adolescents (15%) is, in the main, comparable to the Australian hearing population (14%). There are differences between parents of deaf and hearing children and adolescents with respect to concerns on the social problems and thought problems scales. Specifically, parents of deaf children and adolescents report significantly more concerns on these scales than hearing parents. In explaining these findings it could be argued that they are reflective of the frequently reported social characteristics of deaf children and adolescents, which include feelings of isolation and loneliness, low self-esteem, difficulty in forming a sense of self, difficulty sustaining friendships, and being teased or bullied at school [17–21].
There is a comparable prevalence rate of mental health problems reported by the deaf adolescents in the present study (11.4%) and those adolescents in the Australian hearing population (18.9%). There are, however, significant differences in the reported mental health problems from the deaf adolescents in the present study (11.4%) as compared to those reported by deaf adolescents in the Cornes et al. study (42.6%) [4]. These differences seem, for the most part, to be explained by particular demographic characteristics and subsequent use of different versions of the YSR (written English and Auslan). That is, the deaf adolescents in the Cornes et al. study preferred to communicate using Auslan and were, therefore, given the YSR using the Auslan version. When compared to the deaf adolescents in the present study the Cornes et al. participants reported significantly more concerns on the Internalizing, Externalizing, Withdrawn/Depressed, Social Problems, Rule breaking/Delinquent Behaviour and Aggressive Behaviour scales. In the present study, within-group comparisons between the written English and Auslan versions of the YSR could not be undertaken because only two participants undertook the Auslan version. More in-depth investigation, however, of differences between the two YSR versions would be worthwhile in future studies.
Another important consideration when comparing the results from the present study and that of the Cornes et al. study is that there is a noticeable difference in the participation response rates between the two studies. The response rate for the current study was 28% while that of the Cornes et al. study was 72% [4]. Even though the response rate for the present study is inexplicably low it should be noted that more than one-third of participants, across both age cohorts, were reported as having pre-existing emotional and behavioural problems. It may have been that the parents of these participants were particularly keen to participate so as to get an update on these problems and/or receive a referral for follow up. It may also be the case that many parents who were invited to participate in the study chose not to because they did not have any concerns for their child's mental health and well-being, and as such may have felt that they did not have time to complete the project documentation and/or felt it less important to. It is not known whether any participants in the Cornes et al. study had pre-existing mental health problems.
Overseas studies report a prevalence rate of mental health problems in the deaf child and adolescent population between 28% and 41% [5–9]. Interestingly, there appears to be a correlation between particular demographic characteristics of the sample and the rate of mental health problems reported. For instance, the prevalence rate of mental health problems is higher in those studies that involve participants attending schools for the deaf and preferring to communicate using sign language [5–7]. Caution is warranted, however, with this interpretation, because unfortunately some of these studies identify participants with both borderline and clinical scores as having mental health problems, which results in an artificially inflated prevalence rate.
What is evident from the present results is that it is important for mental health professionals to consider the heterogeneity of the deaf child and adolescent population. Although the majority of Australian deaf children and adolescents prefer to communicate using spoken English and are educated alongside their hearing peers in their local school, each brings with them a unique set of characteristics that must be considered when selecting and using psychiatric instruments. There is no doubt that the development and validation of the Auslan version of the YSR has been a significant contribution to the psychiatric assessment of signing deaf adolescents. There is, however, still a need for use of the written English version of the YSR in psychiatric assessment, particularly for the majority of Australian deaf adolescents for whom the preferred language and communication mode is English.
Considering the potential increasing prevalence of deafness in the Australian child and adolescent population in the future it is incumbent on researchers and practitioners alike to work together in developing a better understanding of the mental health and social emotional well-being of deaf children and adolescents.
Footnotes
Acknowledgements
This project was funded by a competitive research grant provided by Melbourne Graduate School of Education at the University of Melbourne to the first author. The authors would like to acknowledge the Western Australia Institute for Deaf Education, Telethon Speech and Hearing, Department of Education and Training in Western Australia and the Western Australia Foundation for Deaf Children for their contributions and support of this work. A special note of thanks to Dr Andrew Cornes, Principal Family and Systemic Psychotherapist at Royal Liverpool NHS Children's Trust Alder Hey Hospital CAMHS, for his generous provision of the Auslan CD-ROM translation of the Youth Self-Report for use in this project.