
Abstract
Background:
Children and adolescents with intellectual disability are at risk of developing psychiatric symptoms and disorders; yet, the estimates reported in the literature have been inconsistent, presenting a potential barrier for service planning and delivery. Sources of variability could arise from differences in measurement instruments as well as subgroup membership by severity of intellectual disability, gender and age. This systematic review aimed to address these gaps.
Method:
MEDLINE and PsycINFO databases were searched from inception to 2018 and selected studies were reviewed. Studies were included if they reported point prevalence estimates of mental health symptomology or diagnoses in a general population of 6- to 21-year-old individuals with intellectual disability. The Joanna Briggs Institute Prevalence Critical Appraisal Checklist was applied to eligible papers to appraise their scientific strength. Pooled prevalence for mental health symptomology was determined using a random-effects meta-analysis.
Results:
A total of 19 studies were included, including 6151 children and adolescents. The pooled prevalence estimate captured by the Developmental Behaviour Checklist was 38% (95% confidence interval = [31, 46]), contrasting with 49% (95% confidence interval = [46, 51]) captured by the Child Behaviour Checklist; both rates were higher than a non-intellectual disability population. Severity of intellectual disability did not significantly influence the Developmental Behaviour Checklist risks. Insufficient data were available to conduct statistical analyses on the effects of age, gender and socioeconomic status. Of diagnosed psychiatric disorders, attention deficit/hyperactivity disorder (30%), conduct disorder (3–21%) and anxiety disorders (7–34%) were the most prevalent conditions.
Conclusion:
This review consists of the largest sample hitherto evaluated. In the intellectual disability population, mental health comorbidities could be better detected by a symptom phenotype than a psychiatric diagnostic phenotype. Crucially, future research needs to address the effect of measurement validity in the intellectual disability population. Estimated prevalence rates were high compared to the general population, indicating the importance of systematic screening, case detection and appropriate management.
Introduction
A recent population-based epidemiological study estimated the prevalence of intellectual disability (ID) in Australia at 1.7% (Bourke et al., 2016), with higher prevalence estimates reported for low-income countries (Maulik et al., 2011). Individuals with ID experience substantial difficulties with everyday living, are at higher risks of physical ill health and have a 5- to 12-fold increased risk of mortality compared to those without ID (Bourke et al., 2017). Cognitive deficits impair communication and impact negatively social functioning, self-esteem and forming and maintaining friendships, which can lead to loneliness, mood, anxiety and emotional problems. Mental health comorbidities are overrepresented in individuals with ID, in both children (Einfeld and Tonge, 1996) and adults (Cooper et al., 2007), when compared to the general population (Merikangas et al., 2009).
Notably, individuals with ID are at risk of underdiagnosis and underservicing for their mental health problems. This could arise from inadequate screening and detection (Kauffman et al., 2007) and/or greater barriers in accessing mental health services (Whittle et al., 2018). Strikingly, even when a psychiatric disorder is diagnosed, there is a considerable variation across regions in the availability of and access to appropriate clinical care (Krahn et al., 2006; McCarthy and Boyd, 2002; Whittle et al., 2018). The phenomenon of ‘diagnostic overshadowing’ may further complicate this process: that is, a clinician may misclassify and misattribute a set of symptoms as an expression of the existing ID rather than as a distinct co-existing psychiatric condition (Mason and Scior, 2004; Rush et al., 2004). For example, a clinician may regard inattention and hyperactivity in a child with ID as an expression of ID rather than as indexing the presence of comorbid attention deficit/hyperactivity disorder (ADHD).
For children and adolescents with ID, a systematic review identified nine studies published up to 2007 (comprising 3396 individuals) and detected psychiatric symptoms in 30–50% of individuals (Einfeld et al., 2011). However, prevalence estimates varied across studies. Furthermore, meta-analytic methods could not be applied, in part, because (1) different instruments were used across studies to measure psychiatric symptoms and disorders and (2) descriptions of potential confounding factors such as age groups and other demographic characteristics of the study samples were incomplete (Einfeld et al., 2011). For these reasons, the field can benefit from an up-to-date review to identify if these limitations can now be addressed.
Since 2011, further studies of the prevalence of psychiatric symptoms and disorders have been published in populations with ID and it is therefore timely to re-evaluate the literature and apply additional analyses. This systematic review aimed to provide the most up-to-date estimates of the prevalence for both psychiatric disorders and symptomology in children and adolescents with ID, and to explore potential influences of measurement instruments, ID severity and demographic characteristics on prevalence rates.
Methods
Definition of mental health terms
Good mental health is considered not merely the absence of mental illness but the ability to engage fully and meaningfully in one’s own communities and pursuits, and to overcome barriers and obstacles without undue distress (Saxena and Setoya, 2014). Conversely, mental ill health disrupts the normative functioning in the domains of family, interpersonal, occupational and wider community social relationships due to abnormal moods, emotions, thoughts and cognitions, manifesting as aberrant behaviours and functional impairments (World Health Organization, 2004).
Since psychiatric symptoms may present without a formal diagnosis (Ji, 2012), this review utilised two types of information to capture mental ill health: (1) dimensional symptomology scores from validated rating scales (typically completed by laypersons, such as parents and teachers) and (2) formal diagnostic categories from psychiatric interviews (typically administered by clinicians or trained researchers). The presence of mental health symptomology was defined as scoring above the clinical cut-off threshold on a standardised behavioural screening questionnaire completed by laypersons, including parents or teachers, such as the Strengths and Difficulties Questionnaire (SDQ; Goodman and Goodman, 2009), the Child Behaviour Checklist (CBCL; Achenbach, 1991) or the Developmental Behaviour Checklist (DBC; Dekker et al., 2002b; Einfeld and Tonge, 1995). The dimensional scores were dichotomised according to published thresholds to yield the respective binary variables and thus prevalence rates. In contrast, categorical diagnoses were clinically defined psychiatric conditions identified by clinician-administered psychiatric interviews according to a standardised classification method such as the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV, DSM-5) or the International Statistical Classification of Diseases and Related Health Problems (ICD-9, ICD-10). Autism spectrum disorder (ASD) was excluded from this review because population-based studies have already estimated that ASD occurs in 5.1 to 15.5 per 1000 births and ASD with ID is present in 3.8 to 8.6 per 1000 births (Bourke et al., 2016; Van Naarden Braun et al., 2015).
Search processes
The review was conducted and reported using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) method (Moher et al., 2009). The study was registered on the PROSPERO International Prospective Register (CRD42017064870). The search was completed using the MEDLINE and PsycINFO databases, from inception until end 2018. Only publications in English were reviewed. For the initial search, the terms within the five subject concepts (mental health, disability, age, prevalence and assessment tools) were combined (Table 1). Over time, different terms have been used to represent ID: these include (1) learning disability, (2) intellectual and developmental disability, (3) mental handicap, (4) mental retardation (DSM-IIIR, DSM-IV, DSM-IV-TR, ICD-9, ICD-10) and (5) ID (DSM-5, ICD-10) (Schalock, 2011). For our comprehensive search, we applied 13 search terms extending beyond those used in DSM and ICD systems, and these include additional variants on terms such as learning disability and mental handicap (Table 1). Terms within each of the first four subject categories were combined using ‘OR’ and each of the four categories were combined using ‘AND’. The fifth subject category (assessment tools) was combined with the disability terms as an additional search.
Search terms used in the MEDLINE and PsycINFO databases to identify relevant papers.
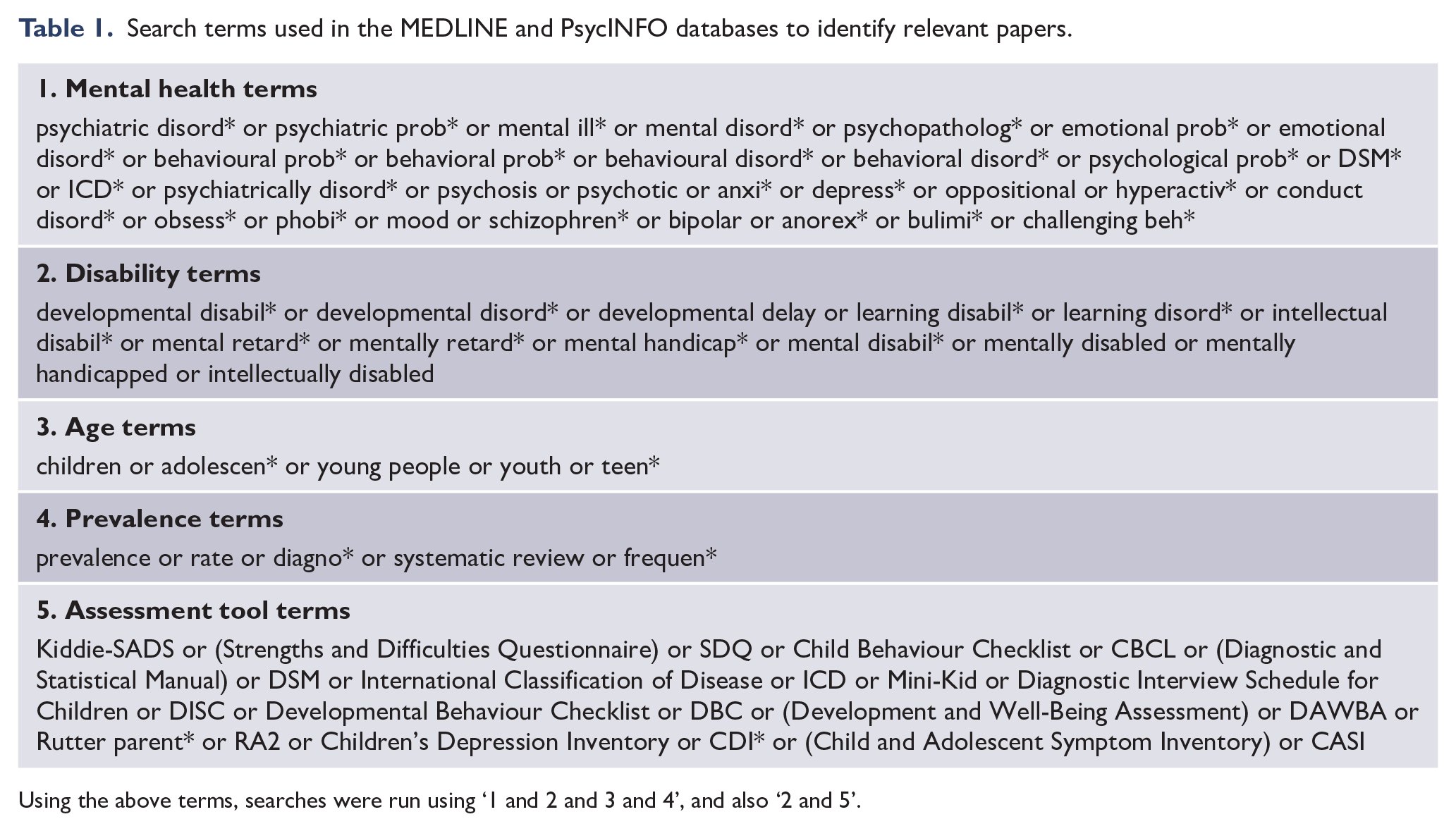
Using the above terms, searches were run using ‘1 and 2 and 3 and 4’, and also ‘2 and 5’.
Inclusion and exclusion criteria
To be included, studies were required to contain data on the prevalence of mental health symptomology or diagnosis in individuals with ID who were 6–21 years of age (studies remained eligible if the mean ± 1 standard deviation [SD] was within the 6- to 21-year age range). Other inclusion criteria included the following: (1) participant diagnosis of ID (excluding those with borderline ID), confirmed by a standardised IQ test such as the Wechsler Intelligence Scale for Children (WISC; Weiss et al., 2016) or a measure of adaptive behaviour such as the Vineland Adaptive Behaviour Scale (VABS; Balboni et al., 2017) or the individuals were enrolled in a support school for children with ID and (2) publication in a peer-reviewed journal.
Studies were excluded for the following reasons: (1) high likelihood of selection bias (i.e. the sample was likely to have an artificially increased prevalence of mental health disorders, such as when individuals were recruited from psychiatric clinic referral lists); (2) high spread of age distribution (i.e. the spread around the mean sample age [i.e. 1 SD] was outside the 6- to 21-year age range); (3) adult samples with participants above 21 years; (4) the mental health disorder diagnosis was derived from case notes or informal parent report, or the diagnostic source was not provided; (5) the study was an intervention-based trial (such as psychotherapy or medication); or (6) the study was a narrative review, systematic review, book chapter, case study, pilot study or informational article. The complete full text of one study was unavailable, and therefore excluded (Singh et al., 2011).
Data extraction process
The MEDLINE and PsycINFO databases were searched by the second author (E.J.G.) using the agreed keywords (Table 1); this yielded 17,446 articles for review. Duplicate records (n = 6955) were removed, and three authors (E.J.G., A.E., H.L.) independently assessed and rated the remaining articles (n = 10,491) based on the content of titles and abstracts according to the agreed criteria. The findings were discussed until consensus was reached. This resulted in exclusion of 10,180 articles. The remaining 311 articles were reviewed by two investigators (E.J.G, N.B.) in full text format to establish eligibility and the findings discussed until consensus was reached. Of these, 293 articles did not meet the inclusion criteria and were excluded. A final set of 18 articles remained for data extraction. The initial search captured systematic reviews; from these, a further set of potentially eligible 42 articles were identified; within the reference lists of this set, only one additional study met the inclusion criteria. Finally, a total of 19 studies were identified as suitable for inclusion in this review (Figure 1).
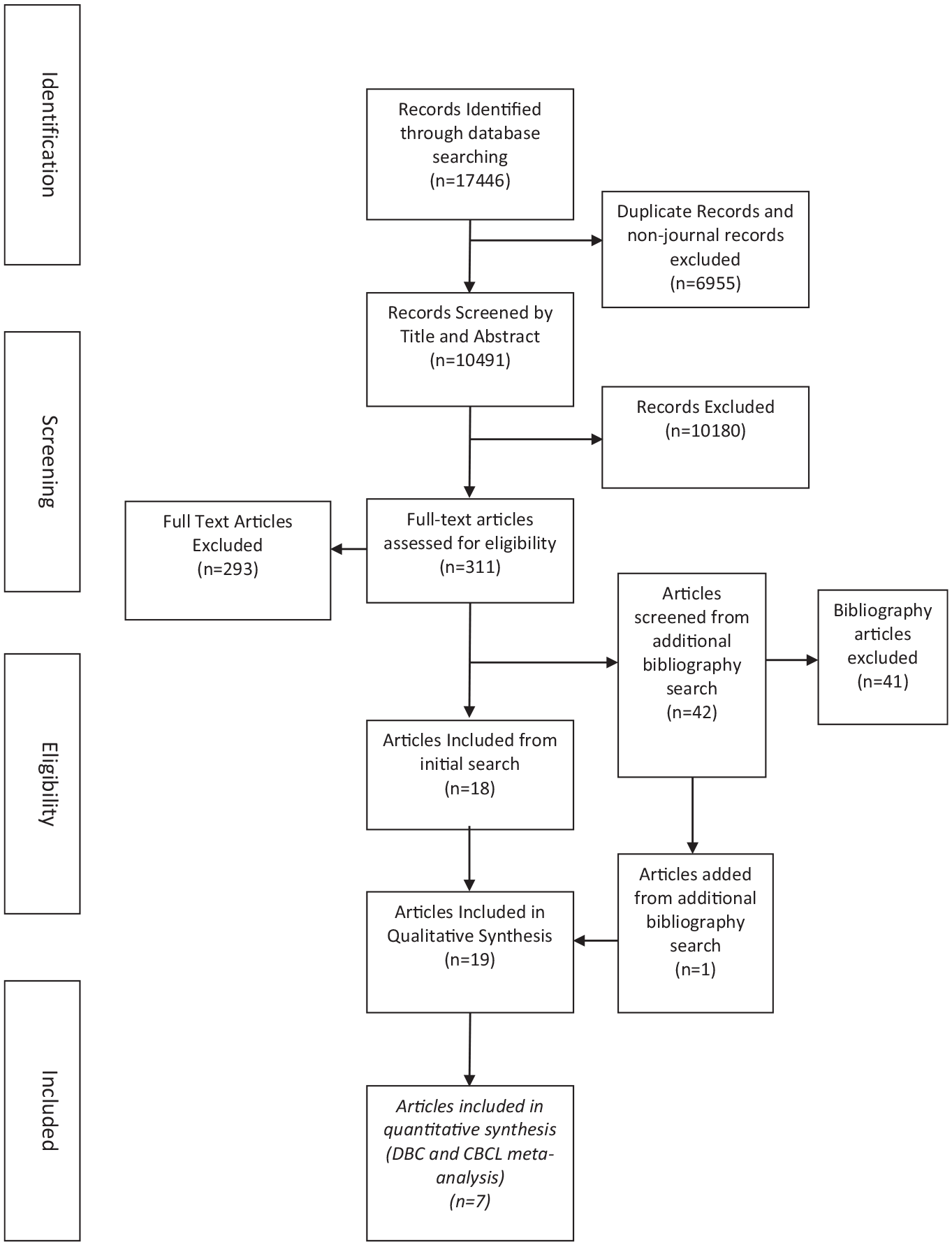
PRISMA flow diagram (Moher et al., 2009) of the literature review and paper inclusion pathways.
Data were extracted independently by three investigators (E.J.G., N.B., R.S.). A standardised spreadsheet was used to extract the following from each article: study design, sample size, ID level (mild, moderate, severe/profound), gender distribution, age range (including mean and SD, where reported), socioeconomic status (SES) distribution, geographic region, diagnosis source/recruitment source, outcome measure(s) used, and prevalence data for mental health symptomology and/or diagnoses.
Critical appraisal
The Joanna Briggs Institute Prevalence Critical Appraisal Checklist (Joanna Briggs Institute, 2014) was used to evaluate the methodological quality of the included articles, and all checklist items were used to evaluate article integrity. For each checklist item, articles were rated as fully meeting requirements (Y), lacking clarity as to whether criteria were fully met (U) or not meeting requirements (N). The three raters (N.B., A.M.B., J.D.) conferred over any differences in findings until consensus was reached.
Data synthesis
The 19 included studies were examined for their suitability for meta-analysis to derive pooled prevalence rates for (1) overall and (2) by severity of ID, age (child/adolescent) and gender. Wherever possible, a random-effects meta-analysis was used to provide a pooled prevalence estimate with confidence intervals, with a forest plot. Heterogeneity between studies was evaluated using the I2 statistic where sufficient studies were available, with I2 > 75% indicating high heterogeneity. STATA version 14 was used for analysis (StataCorp, College Station, TX, USA). A narrative synthesis was conducted when pooling was not possible. Where available, proportions of pooled prevalence of mental health symptoms included in the meta-analysis were compared with general population data with p-values calculated using a normal approximation for the logged prevalence.
Results
The resulting pool of 19 papers included 6151 children and adolescents, and all relevant data were extracted (Tables 2 and 3).
Summary of the included 19 studies describing prevalence of mental health disorders and symptomology in children and adolescents with ID.
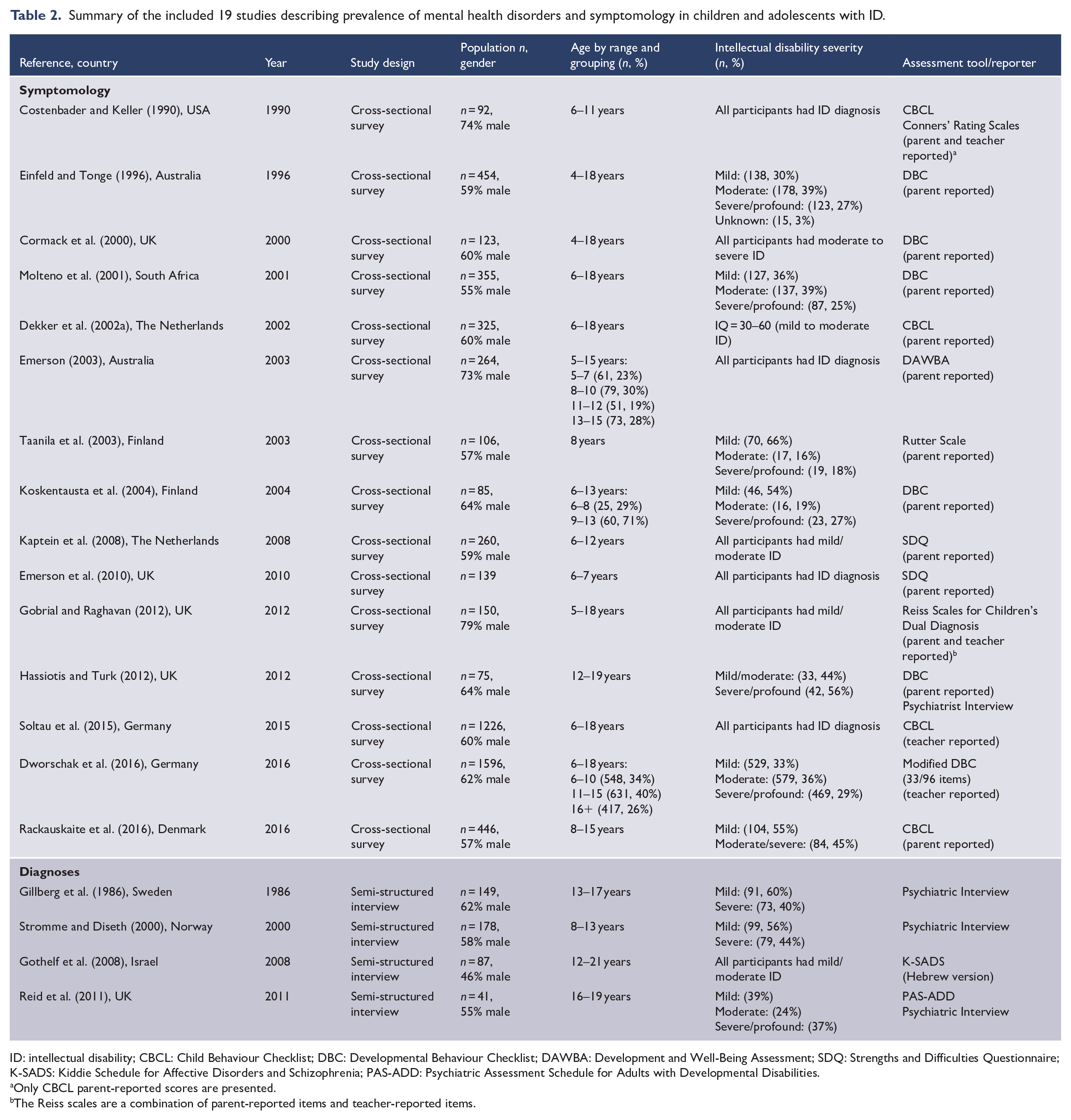
ID: intellectual disability; CBCL: Child Behaviour Checklist; DBC: Developmental Behaviour Checklist; DAWBA: Development and Well-Being Assessment; SDQ: Strengths and Difficulties Questionnaire; K-SADS: Kiddie Schedule for Affective Disorders and Schizophrenia; PAS-ADD: Psychiatric Assessment Schedule for Adults with Developmental Disabilities.
Only CBCL parent-reported scores are presented.
The Reiss scales are a combination of parent-reported items and teacher-reported items.
Summary of mental health disorders and symptomology reported for children and adolescents with ID.
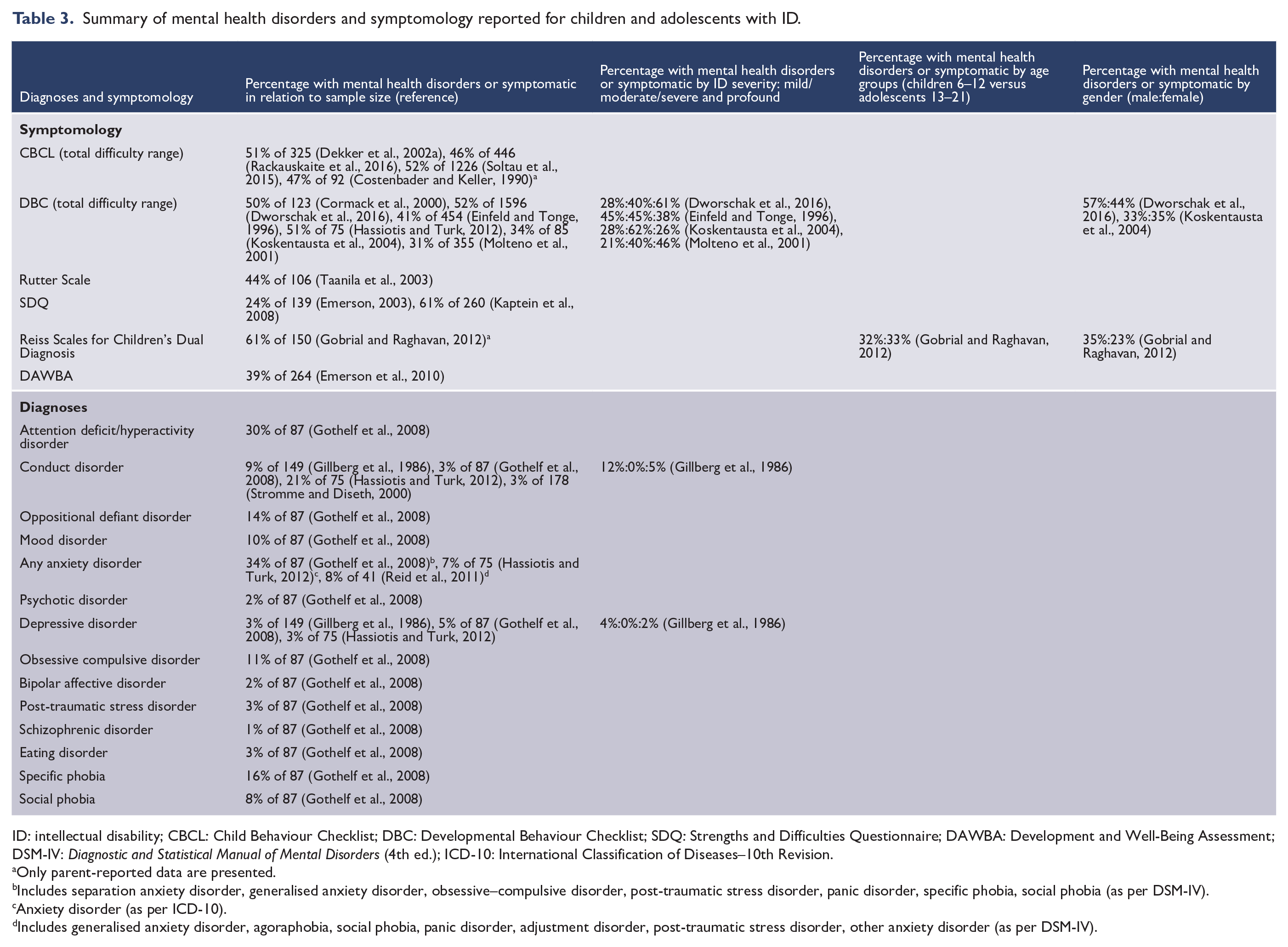
ID: intellectual disability; CBCL: Child Behaviour Checklist; DBC: Developmental Behaviour Checklist; SDQ: Strengths and Difficulties Questionnaire; DAWBA: Development and Well-Being Assessment; DSM-IV: Diagnostic and Statistical Manual of Mental Disorders (4th ed.); ICD-10: International Classification of Diseases–10th Revision.
Only parent-reported data are presented.
Includes separation anxiety disorder, generalised anxiety disorder, obsessive–compulsive disorder, post-traumatic stress disorder, panic disorder, specific phobia, social phobia (as per DSM-IV).
Anxiety disorder (as per ICD-10).
Includes generalised anxiety disorder, agoraphobia, social phobia, panic disorder, adjustment disorder, post-traumatic stress disorder, other anxiety disorder (as per DSM-IV).
Study characteristics
Of the 19 articles, 18 were cross-sectional studies. One was a longitudinal study, in which only data in the follow-up group were included as it was only at this time point that the ages of all participants fell within our age range for inclusion (Emerson et al., 2010). Sample sizes ranged from n = 41 (Reid et al., 2011) to n = 1596 (Dworschak et al., 2016). Five studies were from UK settings (Cormack et al., 2000; Emerson, 2003; Gobrial and Raghavan, 2012; Hassiotis and Turk, 2012; Reid et al., 2011), nine from European settings (Dekker et al., 2002a; Dworschak et al., 2016; Gillberg et al., 1986; Kaptein et al., 2008; Koskentausta et al., 2004; Rackauskaite et al., 2016; Soltau et al., 2015; Stromme and Diseth, 2000; Taanila et al., 2003) and five from other countries (Costenbader and Keller, 1990; Einfeld and Tonge, 1996; Emerson et al., 2010; Gothelf et al., 2008; Molteno et al., 2001).
Eleven studies were based on parent-reported data (Cormack et al., 2000; Dekker et al., 2002a; Einfeld and Tonge, 1996; Emerson, 2003; Emerson et al., 2010; Hassiotis and Turk, 2012; Kaptein et al., 2008; Koskentausta et al., 2004; Molteno et al., 2001; Rackauskaite et al., 2016; Taanila et al., 2003), two on teacher-reported data (Dworschak et al., 2016; Soltau et al., 2015) and two studies provided both parent- and teacher-reported data (Costenbader and Keller, 1990; Gobrial and Raghavan, 2012). The DBC and CBCL were the two most commonly used symptom rating scales: six studies used the DBC (Cormack et al., 2000; Dworschak et al., 2016; Einfeld and Tonge, 1996; Hassiotis and Turk, 2012; Koskentausta et al., 2004; Molteno et al., 2001) and four used the CBCL (Costenbader and Keller, 1990; Dekker et al., 2002a; Rackauskaite et al., 2016; Soltau et al., 2015). Four studies were based on psychiatric interviews (Gillberg et al., 1986; Gothelf et al., 2008; Reid et al., 2011; Stromme and Diseth, 2000).
Breakdown of ID severity (mild, moderate, severe/profound) was presented in 10 of the 19 studies (Dworschak et al., 2016; Einfeld and Tonge, 1996; Gillberg et al., 1986; Hassiotis and Turk, 2012; Koskentausta et al., 2004; Molteno et al., 2001; Rackauskaite et al., 2016; Reid et al., 2011; Stromme and Diseth, 2000; Taanila et al., 2003). The gender distributions in 18 of the 19 studies showed a (marginal to marked) male preponderance (55–79%) and one had marginally more females (54%) (Gothelf et al., 2008). Eleven studies assessed both children and adolescents (Cormack et al., 2000; Dekker et al., 2002a; Dworschak et al., 2016; Einfeld and Tonge, 1996; Emerson, 2003; Gobrial and Raghavan, 2012; Koskentausta et al., 2004; Molteno et al., 2001; Rackauskaite et al., 2016; Soltau et al., 2015; Stromme and Diseth, 2000), four assessed only children (Costenbader and Keller, 1990; Emerson et al., 2010; Kaptein et al., 2008; Taanila et al., 2003) and four assessed adolescents and young adults (Gillberg et al., 1986; Gothelf et al., 2008; Hassiotis and Turk, 2012; Reid et al., 2011).
Critical appraisal
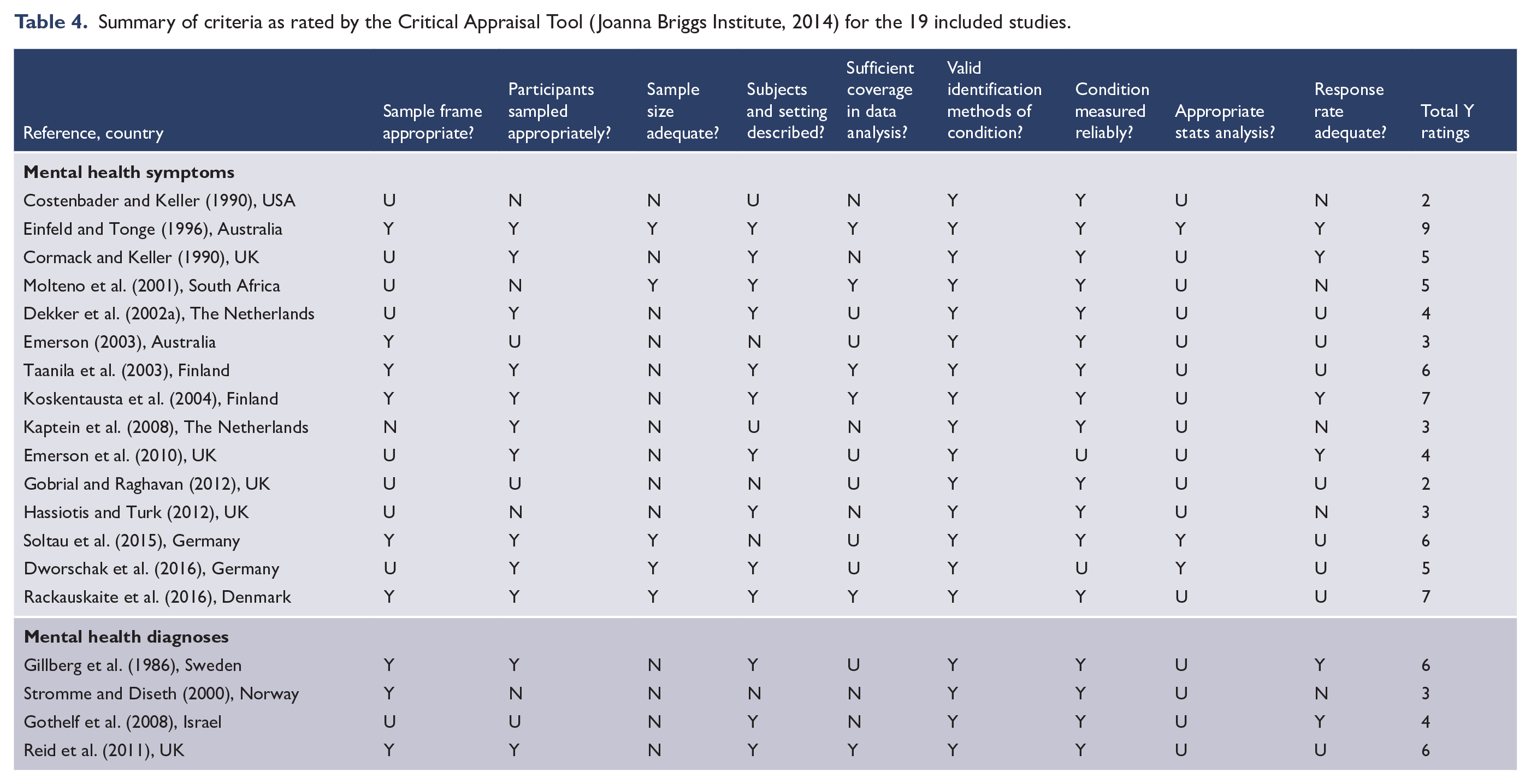
The Joanna Briggs Prevalence Critical Assessment Tool indicated variation in quality within the included studies, with scores ranging from 2 to 9 of the nine items (Table 4). The strongest items indicated the use of validated measures to identify psychiatric symptomology/disorders (19 of 19 studies) and reliable measurement processes (two were unclear: Dworschak et al., 2016; Emerson et al., 2010). Six studies recruited samples that were clearly representative of the broader population of ID (Einfeld and Tonge, 1996; Koskentausta et al., 2004; Molteno et al., 2001; Rackauskaite et al., 2016; Reid et al., 2011; Taanila et al., 2003). The sample size was adequate in five studies (Dworschak et al., 2016; Einfeld and Tonge, 1996; Molteno et al., 2001; Rackauskaite et al., 2016; Soltau et al., 2015).
Summary of criteria as rated by the Critical Appraisal Tool (Joanna Briggs Institute, 2014) for the 19 included studies.
Prevalence of psychiatric disorders
The prevalence estimates of psychiatric disorders using diagnostic interviews varied across studies (Table 3). The commonly reported conditions were as follows: depressive disorders (3–5%) (Gillberg et al., 1986; Gothelf et al., 2008; Hassiotis and Turk, 2012), conduct disorders (3–21%) (Gillberg et al., 1986; Gothelf et al., 2008; Hassiotis and Turk, 2012; Stromme and Diseth, 2000) and any anxiety disorder (7–34%) (Gothelf et al., 2008; Hassiotis and Turk, 2012; Reid et al., 2011). One study reported ADHD in 30% of 87 individuals (Gothelf et al., 2008).
Prevalence of elevated psychiatric symptoms
The prevalence estimates varied between 24% and 61% across studies. Six studies used the DBC, with estimates ranging from 31% to 53%. In our meta-analysis of the four studies that used the DBC (excluding one study that used a modified DBC, Dworschak et al., 2016; and another study with only severely affected individuals, Cormack et al., 2000), the pooled prevalence of psychiatric symptoms was 38% (95% CI = [31, 46]) (Figure 2). Four studies used the CBCL, with estimates ranging from 46% to 52%. In our meta-analysis of three of the four studies (one study using teacher report was excluded, Soltau et al., 2015), the pooled prevalence of symptoms was 49% (95% CI = [46, 51]) (Figure 2). The prevalence of elevated CBCL scores in children and adolescents in the general population has been reported as 14% (95% CI = [13, 15]) (Sawyer et al., 2001), and by comparison, our pooled prevalence for children and adolescents with ID was significantly higher (p < 0.001).
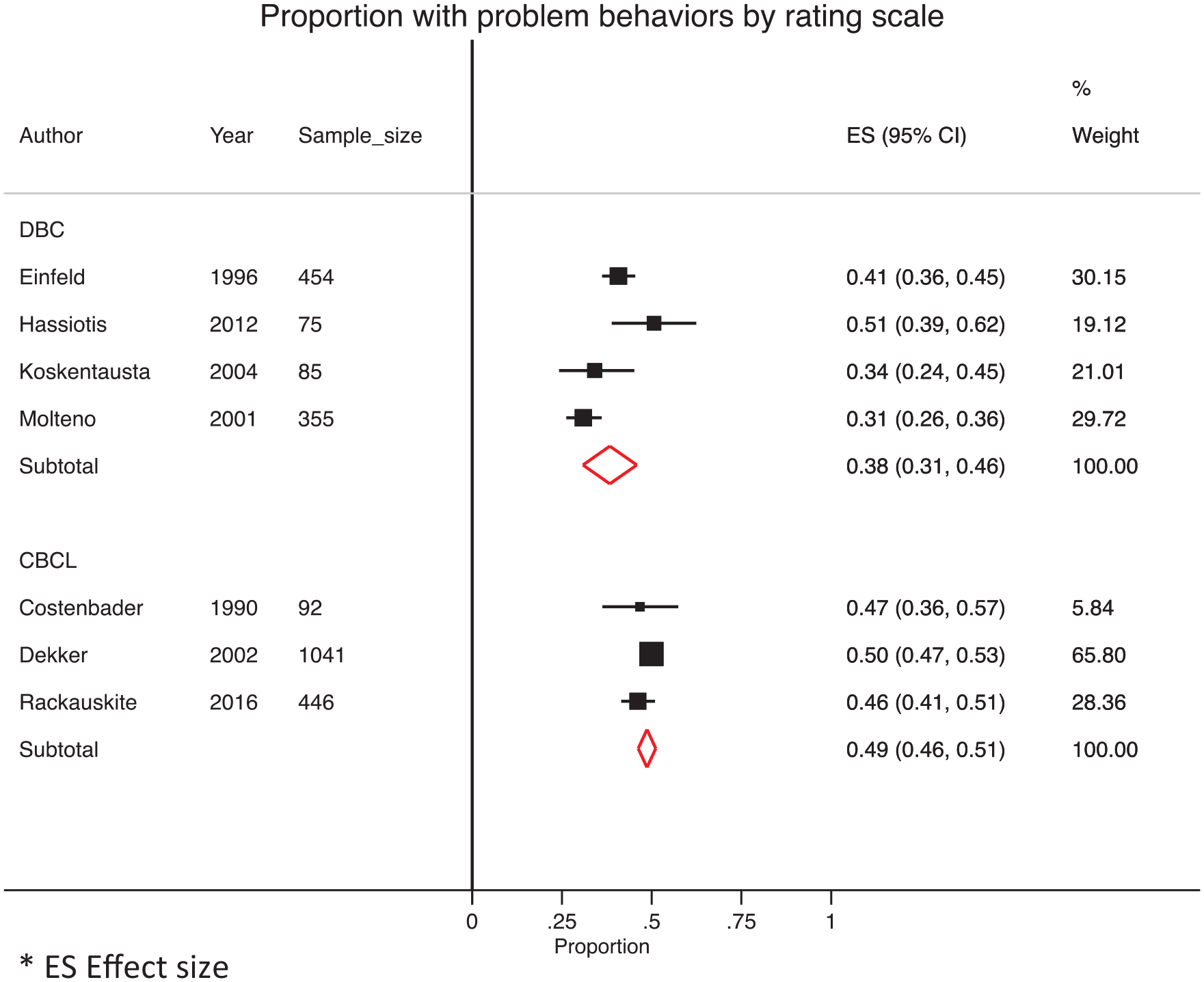
Pooled prevalence rates for mental ill-health symptoms in children and adolescents with intellectual disability according to the Developmental Behaviour Checklist (DBC) and Child Behaviour Checklist (CBCL) rating scales.
Meta-analysis of DBC estimates by ID severity
Random-effects meta-analysis estimated the pooled prevalence rates for three ID subgroups derived from three studies as follows: 32% (95% CI = [16, 47]) for individuals with mild ID, 44% (95% CI = [37, 52]) for individuals with moderate ID and 39% (95% CI = [30, 48]) for individuals with severe ID (Figure 3).
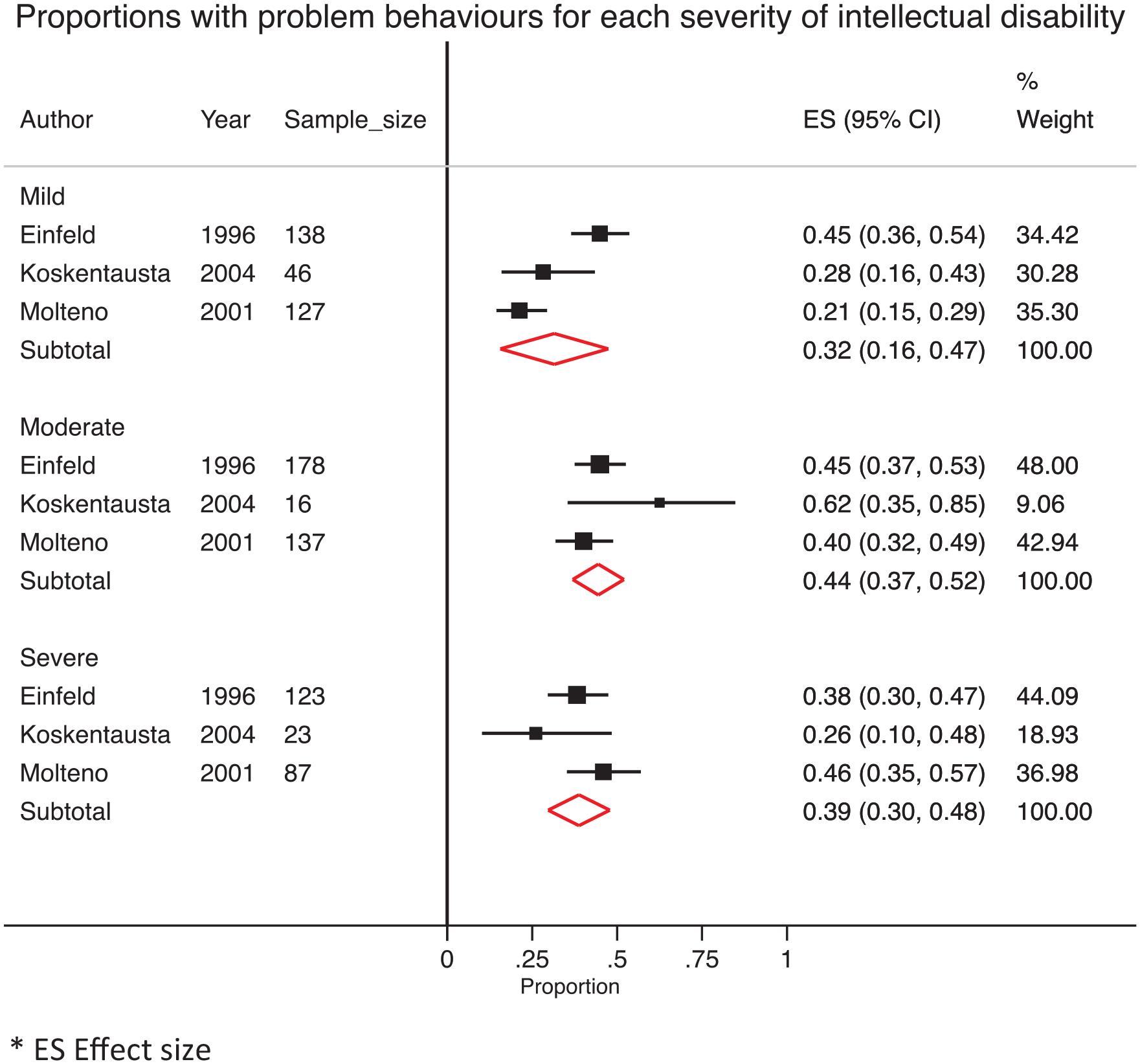
Pooled prevalence rates for mental ill-health symptoms captured by the Developmental Behaviour Checklist for children and adolescents with mild, moderate and severe intellectual disability.
Analyses stratified by age group, gender and SES
The majority of studies did not report separate prevalence estimates by age group or gender. Three studies provided estimates stratified by gender: two studies reported higher prevalence in males (Dworschak et al., 2016; Gobrial and Raghavan, 2012) and one reported similar estimates (Koskentausta et al., 2004) (Table 3). Only one study reported separate prevalence estimates for children and adolescents, and both estimates were similar (Gobrial and Raghavan, 2012) (Table 3). No study reported estimates for early adulthood. No studies reported prevalence estimates for SES status.
Discussion
Our meta-analyses yielded pooled prevalence values of 38% and 49% for psychiatric symptoms in children and adolescents with ID using the DBC and CBCL measures, respectively. Overall, these estimates are much higher than the prevalence (14%) in typically developing children and adolescents identified in a large-scale epidemiological survey using the CBCL (Sawyer et al., 2001). Our review also examined the prevalence of formal psychiatric diagnoses in children and adolescents with ID. The commonly reported psychiatric disorders included the following: ADHD (39%), anxiety disorders (7–34%), conduct and externalising disorders (3–21%) and depressive disorder (3–5%). These data are mostly similar to the worldwide prevalence estimates reported in a recent meta-analysis of child and adolescent community samples which reviewed 41 studies across 27 countries: 5.7% for any disruptive disorder, 9.6% for any anxiety disorder and 2.6% for any depressive disorder (Polanczyk et al., 2015). Overall, these data suggest that formal psychiatric diagnostic categories (except ADHD) may not capture the full extent of mental ill-health problems experienced by individuals with ID, contrasting with ill-health symptoms captured by rating scales. Individuals with ID may express their mental health problems differently, and their problems could be better detected by a symptom phenotype than a psychiatric diagnostic phenotype.
On the effect of ID severity, our meta-analysis of three studies did not detect differences in the pooled estimates across three levels (i.e. mild, moderate and severe ID). The confidence intervals overlapped suggesting similar prevalence of psychiatric symptoms, irrespective of the child’s adaptive functioning levels and capacity for communication. Importantly, most studies reviewed did not provide separate prevalence estimates stratified by gender or age group. The expression of psychiatric symptoms and disorders can vary by gender and across different developmental windows. For instance, anxiety disorders track a U-shaped age prevalence curve, with some gender differences (Copeland et al., 2014). To evaluate the effects of the developmental transitions, we found only one study that reported rates stratified by the age bands (Gobrial and Raghavan, 2012). The risks (captured by the Reiss Scales) appear largely invariant across the developmental windows of childhood and adolescence. We would have liked to evaluate mental ill health in early adulthood from 18 to 21 years to capture the immediate transition period when adolescents graduate to adult services, but no study provided these data, highlighting an important gap in the literature. Only three studies provided data stratified by gender (see Table 3), with two suggestive of a male preponderance. SES data were reported in nine studies but each used a different measure of SES and prevalences for different SES categories were not reported. The degree to which variation in gender, age group and SES across evaluated studies may confound our findings could not be disentangled, given the insufficiency of available data.
Another source of variability across studies may arise from a measurement effect. Our findings raise important questions as to how to measure psychiatric symptoms in ID. Crucially, future research needs to address the effect of measurement validity in the ID population, whether variation exists (1) between symptom dimensions and psychiatric disorder categories or (2) between symptom dimensions captured by different rating scales. The confidence intervals of estimates derived from DBC and CBCL data in our meta-analyses barely overlapped suggesting that some differences in prevalence estimates could arise from the choice of the measurement tool. Both the DBC and the CBCL are checklists of symptoms, but those in the DBC were developed from the examination of extensive case notes on individuals with ID (Einfeld and Tonge, 1995) and good psychometric properties for ID have been reported (Dekker et al., 2002b; Einfeld and Tonge, 1995). The CBCL was developed for the general population (Achenbach, 1991). It is possible that the DBC is more sensitive to psychiatric symptoms in ID, and that the CBCL is also sensitive to unusual behaviours in the ID population that may not be psychiatric symptoms. Therefore, it remains unclear whether the CBCL captures false positive symptoms, as the DBC was designed and developed specifically for children with ID. Alternatively, the DBC could underdetect psychiatric symptoms. We could not identify a study using both measures simultaneously and it is difficult to compare findings using different measures. Our findings would suggest the need for a future study using both instruments which can be validated against a research standard diagnostic interview as well as against external measures of impairment/parental distress.
Additional limitations of our study need to be considered. First, the number of studies reporting certain specific diagnostic disorders was small: for ADHD and some anxiety disorders, it was confined to one study (Gothelf et al., 2008). Second, cross-comparison of the included studies was complicated by the diversity of recruitment methods and assessment tools. Third, many of the included studies had relatively small sample sizes (for 11 of 19 studies, n ⩽ 150) and some may not have been truly representative of the overall population. While all reviewed studies used standardised assessment tools, different tools were used rendering head-to-head comparison of the studies problematic. For the studies of symptoms, parents and/or teachers were assessors, which may yield different results, depending on assessment item (Bordin et al., 2013). While we instituted a number of measures to control bias and misinformation (e.g. rigorous inclusion/exclusion criteria and search terms), it must be acknowledged that this is a body of heterogeneous data from a variety of sources.
Our findings have implications for clinical practice and research. It is apparent that poor mental health presents a significant challenge to well-being for a high proportion of children and adolescents with ID and their families, but providing accurate clinical diagnosis and clinical care encounters barriers such as lack of training and services and poor care coordination (Whittle et al., 2018). Children with ID encounter greater communication barriers when interacting with their parents, carers and teachers, and in turn, with doctors and other health professionals, which can render detection and diagnosis of a specific condition more difficult (Ziviani et al., 2004). Clinicians may attribute symptoms as an expression of the existing ID rather than a mental health condition (Mason and Scior, 2004; Rush et al., 2004) – the phenomenon of diagnostic overshadowing. Specific aspects of healthcare systems (such as a lack of coordination between disability and mental health service sectors both in service accessibility and funding) can also limit access to services for individuals with ID and their carers (Mizen et al., 2012; Trollor, 2014). Individuals with ID disproportionately belong to lower SES groups, experiencing more inequalities of health (Graham, 2005), higher rates of psychopathology (Hudson, 2005; Reiss, 2013) and greater barriers in accessing services (Kauffman et al., 2007; Mizen et al., 2012).
There are several implications for future research. Prevalence data are still underreported for subgroups, thereby impeding more specific analyses. Prevalence by age, for example, is important as many serious psychiatric disorders emerge in the late teens to early 20s (Kessler et al., 2007) and accurate estimates of prevalence in adolescents and young adults are also necessary to support the effective transition from child health services. These latter data are not currently separated in adult studies. Standardisation of measures would also facilitate comparisons across studies. We also do not know the proportion of children with ID who are accessing mental health services and on the differential patterns of low or high service utilisation. A pattern of high service utilisation by a small section of a given population would conform to the well-established Pareto principle (i.e. 20% of a population exert an 80% effect on either burden or productivity) which has recently been demonstrated in hospitalisation cost-burden, with 20% of the Dunedin birth cohort utilising 77% of hospitalisation resources (Caspi et al., 2016). These analyses would be important for service planning and represent a new avenue for future research. Finally, our analysis identified suitable studies that originated from a limited range of countries. For example, one epidemiological paper was conducted in the United States but none from Canada; two were from Australia but none from New Zealand; and notably, there were no studies from Asian countries which publish scientific studies on many psychiatric conditions. We hope that our findings will encourage other research and clinical groups elsewhere in the world to conduct research in this area.
In conclusion, this study provides further support to the evidence regarding the presence of psychiatric symptoms in children and adolescents with ID. This analysis represents the most up-to-date review using stringent inclusion criteria on the largest to date combined sample of children and adolescents with ID, highlighting the mental health needs of this vulnerable population and providing important prevalence estimates for clinicians and policy makers in service planning.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The Telethon Kids Institute and the Department of Health Western Australia Merit Award were acknowledged for awarding seed grants to conduct this review. The funding bodies for this study had no role in the study design, data collection, data analysis, manuscript preparation and/or publication decisions.