
Abstract
Background:
Mental disorders often have their first onset during youth, which justifies targeting treatment services at this age group. Australia has had a substantial increase in youth mental health services since the introduction of the Medicare Better Access scheme and headspace services in 2006–2007. This paper examines trends in the mental health of Australian youth before and after this time using available national and state datasets.
Methods:
The following data were examined for age groups available in the age range of 12–25 years: use of mental health services per 100,000 population provided under Medicare by GPs, psychiatrists, clinical psychologists, other psychologists and allied health professionals; per capita accessing of headspace services; and prevalence of high and very high psychological distress (using the K10) in youth age groups in the National Health Survey, the Victorian Population Health Survey and the New South Wales Population Health Survey between 2001 and 2018.
Results:
There has been a large increase in use of mental health services since the introduction of Better Access and headspace. No significant improvement in youth mental health was evident following the introduction of these schemes. Rather, there appeared to be a worsening of youth mental health from around 2015 onwards.
Conclusion:
Despite a large increase in the provision of mental health services to Australian youth, there has not been a detectable reduction in the prevalence of psychological distress. There may be other factors that have worsened youth mental health in recent years.
Introduction
Jorm (2018) has published data showing that the prevalence of high and very high psychological distress in Australian adults has not improved despite a large increase in the provision of treatment for mental disorders with the introduction of the Better Access scheme in November 2006. Under this scheme, the Australian government greatly expanded the range of mental health treatment services covered under Medicare, which is Australia’s universal health insurance scheme. New benefits were added for mental health services provided by GPs and for the first time, there was coverage of mental health services provided by clinical psychologists, other psychologists and allied health practitioners (social workers and occupational therapists). Services provided by private psychiatrists were covered prior to this reform and continued as before. This reform led to a rapid rise in use of mental health services provided by GPs, clinical psychologists, other psychologists and allied health practitioners, with services provided by psychiatrists showing little change. However, during this period, there was no change in the prevalence of high and very high psychological distress found in the National Health Surveys conducted by the Australian Bureau of Statistics. This finding is consistent with previous reports from other high-income countries that large increases in treatment of adults, mainly use of medication, do not appear to reduce the prevalence of mental disorders (Jorm et al., 2017; Mulder et al., 2017; Nishi et al., 2018; Ormel et al., 2004).
Several explanations have been offered to account for the lack of a detectable impact of increases in treatment services on prevalence in adults (Jorm, 2018; Jorm et al., 2017). It is possible that the benefits of increases in treatment provision have been masked by increases in risk factors for mental disorders, which have occurred at the same time. Another possibility is that the quality of the increased treatment has been wanting, either through failing to meet standards of minimally adequate treatment or not targeting the groups with highest need. A third possibility is that reducing prevalence requires action on prevention as well as increases in treatment services and that this has not occurred.
The purpose of this paper is to extend the examination of the impact of treatment services on prevalence to the Australian youth age group. Mental disorders often have their first onset during youth and there has historically been a low rate of treatment in this age group. This has led to strong advocacy for the importance of early intervention services, with an emphasis on the 12–25 age group (McGorry et al., 2007). It has been argued that ‘early case identification and intensive treatment of first episodes of illness constitute a core preventive strategy with an excellent chance of reducing prevalence, cost and morbidity by preventing progression of illness’ (McGorry et al., 2007). As well as the increase in the availability of mental health services to youth after the introduction of the Better Access scheme, advocacy for the importance of youth mental health led the Australian government to begin funding youth-friendly ‘headspace’ services in 2006, with an initial 10 centres opening in 2007 and increasing to 110 centres in early 2019 (Rickwood et al., 2019). By June 2018, over 446,000 young people had accessed headspace services and 2.5 million occasions of services had been delivered (McGorry et al., 2019). Headspace services are funded from a number of sources, with the two largest being direct government funding to headspace and reimbursement of services under Medicare (Rickwood et al., 2015). An independent evaluation of the impact of these headspace services commissioned by the Australian Government found that, compared to a matched control group receiving no treatment, the effects of headspace on symptoms were ‘relatively weak’ (Hifferty et al., 2015).
There are some existing published population data relevant to the impact of increasing youth services. The first comes from two national surveys of child and adolescent mental health which were carried out in 1998 and 2013–2014. The second national survey found that 45% of adolescents with mental disorders reported using services for emotional or behavioural problems in the previous 12 months (Johnson et al., 2016). While these data cannot be compared directly with results from the first national survey in 1998, which asked about services in the previous 6 months rather than 12 months, the authors of the second survey have concluded that there is likely to have been a substantial increase in service use over this period (Johnson et al., 2016). However, it was possible to directly compare the prevalence of three mental disorders which were assessed in both surveys (Sawyer et al., 2018a). Comparing the data on adolescents aged 12–17 years, this study found an increase in the prevalence of major depressive disorder, but little change in attention-deficit/hyperactivity disorder and conduct disorder.
The second set of relevant data comes from the Household, Income and Labour Dynamics in Australia (HILDA) Survey between 2001 and 2017 (Burns et al., 2020). This survey administered the 5-item Mental Health Index (MHI-5) to adults 18 years and above, with higher scores indicating better mental health. An analysis of time trends found no improvement in mental health which might be attributable to service increases. Rather, there was a small decline in mental health of adults aged 18–24 years from around 2013 onwards.
This paper assembles additional data relevant to the impact of youth mental health services on the mental health of the youth population. It examines time series data on use of mental health services provided through Medicare and headspace to youth. It also uses data on the prevalence of high and very high psychological distress from national, Victorian and New South Wales population health surveys. Meta-analysis is used to combine the prevalence data and get more reliable estimates. In these datasets, age is grouped in various ways, with 12–25 years not being a common grouping. The approach taken here is to report any data that falls within this age range.
Methods
Data on services
Data on Medicare-funded mental health services from 2006 to 2019 were obtained from a publicly accessible online database provided by the Australian Government Department of Human Services (2020). The age grouping available from this database was 15–24 years. The Medicare Benefits Schedule item numbers that were included in the analysis were those listed by the Australian Institute of Health and Welfare (2020) as covering mental health services by psychiatrists, general practitioners, clinical psychologists, other psychologists and other allied health providers over any part of this period, whether or not these were newly introduced with Better Access. Dates for items were determined by the date the service was processed by Medicare Australia, not the date the service was provided. Services per 100,000 population aged 15–24 years were calculated by dividing the number of services by the number of people enrolled in Medicare.
Data on number of Australians aged 12–25 years who were clients of headspace services each year from 2006–2007 to 2018–2019 were obtained from available headspace reports (Headspace 2010, 2012, 2013, 2019; Muir et al., 2009). Number of clients per 100,000 was calculated by dividing the number of clients by the size of the population aged 12–25 years according to the Australian Bureau of Statistics (2019).
Data on prevalence
Prevalence of psychological distress in Australia was based on the K10 questionnaire (Andrews and Slade, 2001) which was administered in the National Health Surveys carried out in 2001, 2004–2005, 2007–2008, 2011–2012, 2014–2015 and 2017–2018 to people aged 18 years or above (Australian Bureau of Statistics, 2002, 2006, 2009, 2012, 2015, 2018). The K10 was scored from a minimum of 10 to a maximum of 50, with scores of ⩾22 being defined by the Australian Bureau of Statistics as ‘high’ or ‘very high’ psychological distress. Data on percent prevalence of scores ⩾22 from people aged 18–24 years were extracted.
Data on the prevalence of high to very high psychological distress (K10 ⩾ 22) were also available for the state Victoria from the Victorian Population Health Survey for people aged 18–24 years between 2002 and 2017 (State Government of Victoria, 2020). These surveys were carried out by telephone, in contrast to the household survey method of the National Health Surveys. From 2002 to 2011, this survey was carried out using random digit dialling of landlines, but in 2015, it began using dual-frame sampling involving both landlines and mobile phones because of the increase in mobile-only households. Youth who are mobile-only users are known to have a higher prevalence of psychological distress (Holborn et al., 2012), so this change in sampling methodology is a factor that must be taken into account when examining changes in prevalence over time.
Data on the prevalence of psychological distress (K10 ⩾ 22) was also available for the state of New South Wales from the New South Wales Population Health Survey for people aged 16–24 years between 2003 and 2019 (New South Wales Government, 2020). As for Victoria, these surveys were carried out by telephone. The surveys involved landline-only sampling until 2012, when dual-frame sampling was introduced.
Statistical methods
The prevalence percentages and their 95% confidence intervals (CIs) for each year were graphed to examine trends before and after the introduction of the additional services. For the National Health Surveys and Victorian Population Health Surveys, 95% CIs were available in the published reports for more recent years but not for earlier years. Where the 95% CIs were not provided, they were estimated from the prevalence proportion and number of participants in the age group using Comprehensive Meta-Analysis Version 3. These CIs are approximations which do not take account of any complex survey weighting.
In order to give greater statistical power to detect any changes in prevalence in psychological distress, data from the three surveys were combined using Comprehensive Meta-Analysis Version 3. Data were extracted from the published reports on the following variables: year of survey, prevalence of psychological distress, age group (18–24 or 16–24 years), population (Australia, New South Wales or Victoria) and survey methodology (household, landline or dual frame). Data for the meta-analysis were independently coded by both authors, who resolved any disagreement by discussion. To give a greater sample size for each time period, data were combined from the 4 years before the introduction of the reforms (2003–2006, referred to as the ‘Pre’ period), the first 4 years after their introduction (2007–2010, referred to as the ‘Early’ period), the next 4 years (2011–2014, referred to as the ‘Mid’ period) and the most recent years (2015 onwards, referred to as the ‘Late’ period). The random effects model was used to combine the data for each time period. Because there were methodological differences between the three surveys and methodological changes over time (the move from landline to dual-frame sampling in New South Wales and Victoria), a dummy variable was created to reflect these differences. This dummy variable involved the following categories: Australia household, New South Wales landline, New South Wales dual frame, Victoria landline and Victoria dual frame, with the first category as the reference group. A meta-regression was carried out examining the effects of survey period adjusting for survey methodology.
Results
Figure 1 shows the number of Medicare mental health services per 100,000 persons aged 15–24 years from beginning of 2006 until end of 2019. The number of services provided by GPs, clinical psychologists, psychologists and allied health practitioners has increased dramatically from the inception of Better Access. The services provided by psychiatrists, who had been covered by Medicare prior to Better Access, showed much less growth over the period. Accumulating all types of services together, by 2019, young people aged 15–24 years averaged 0.66 services per person.
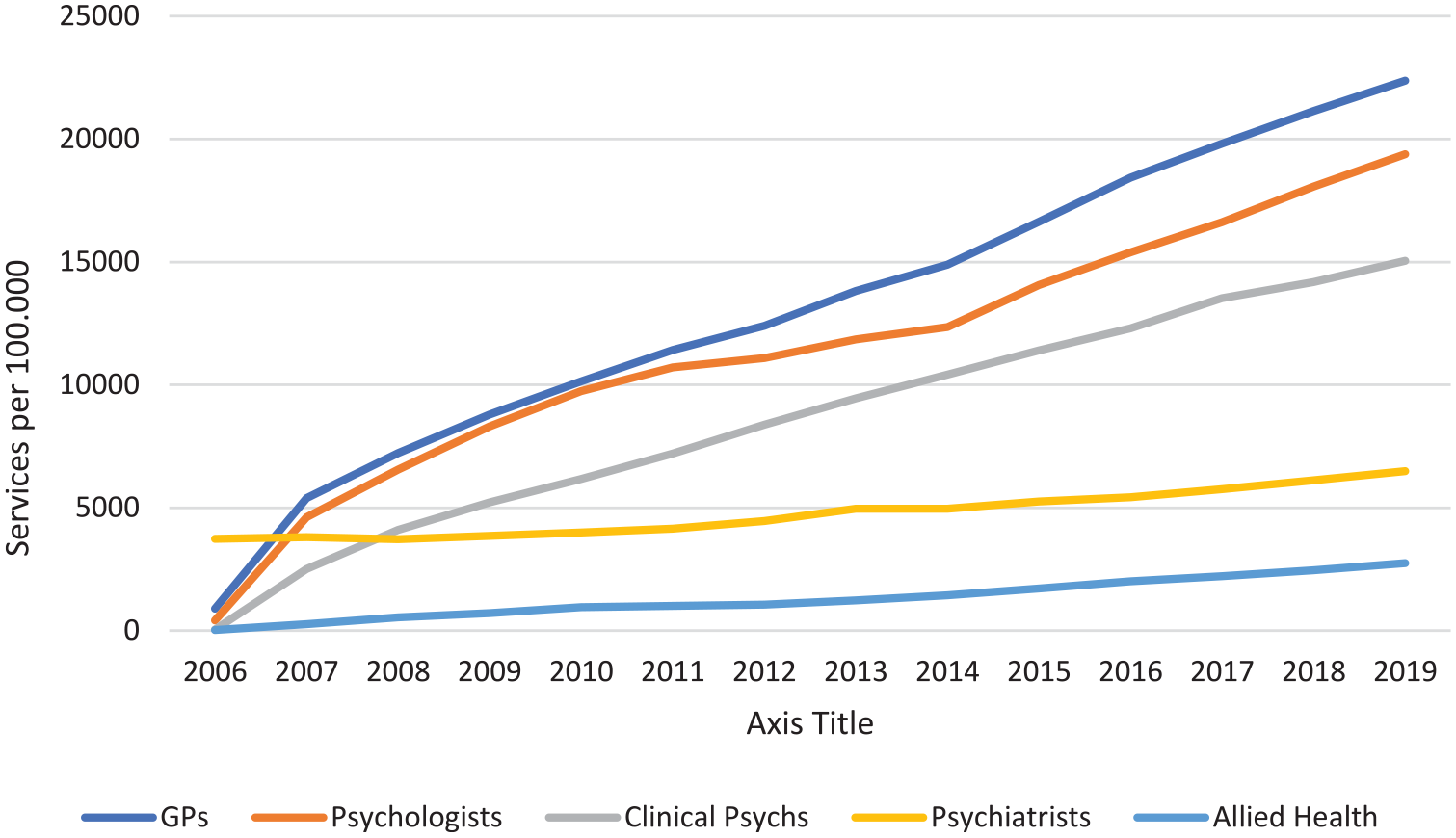
Medical Benefits Schedule mental health services per 100,000 persons aged 15–24 years.
Figure 2 shows the number of headspace clients per 100,000 persons aged 12–25 years. There has been a steady rise since the inception of headspace.
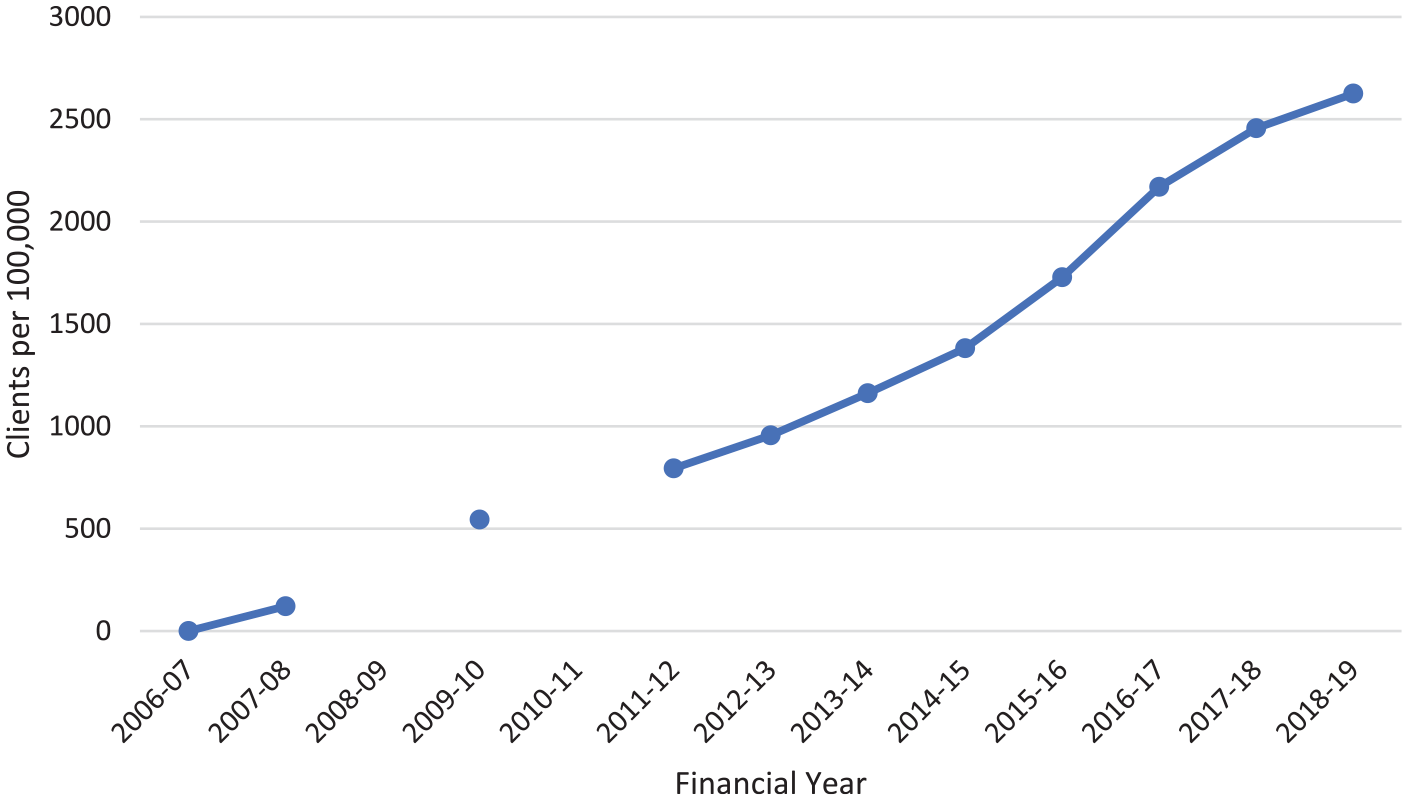
Number of headspace clients per 100,000 persons aged 12–25 years.
Figure 3 shows the prevalence of high and very high psychological distress in adults aged 18–24 years in the National Health Surveys. There was a decrease in prevalence after Better Access and headspace were introduced, but prevalence then increased to be close to previous levels by 2014–2015.
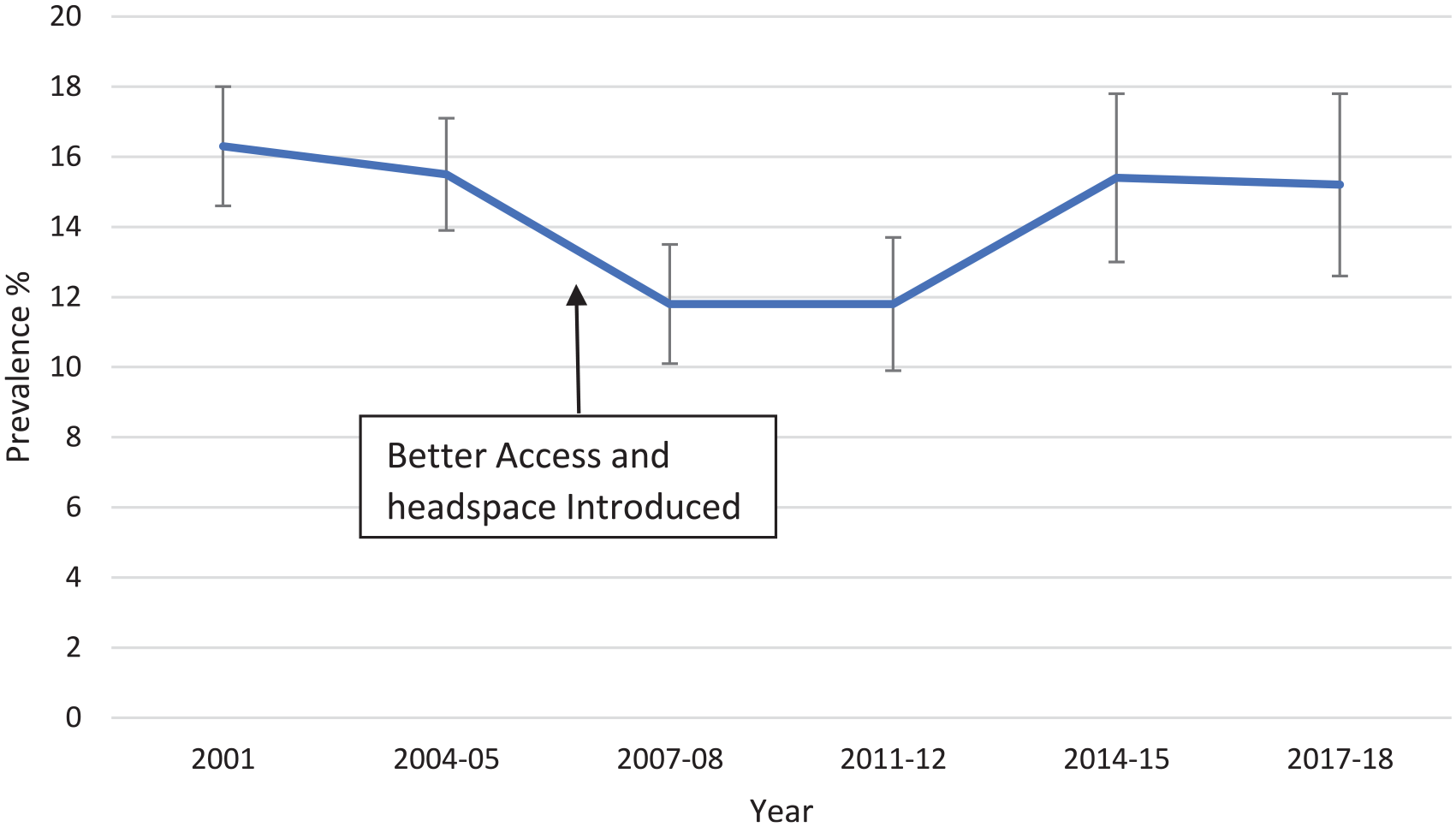
Prevalence of high and very high psychological distress (K10 ⩾ 22) in persons aged 18–24 years, Australia, in the National Health Survey. Error bars are 95% CIs.
Figure 4 shows the prevalence of high and very high psychological distress in adults aged 18–24 years in the Victorian Population Health Surveys from 2002 to 2017. It also shows the point at which the survey sampling changed to dual frame in 2015. Prevalence was similar in the years before and after the introduction of Better Access and headspace. However, from 2012, prevalence began to rise and this does not seem to be accounted for by the change in methodology in 2015.
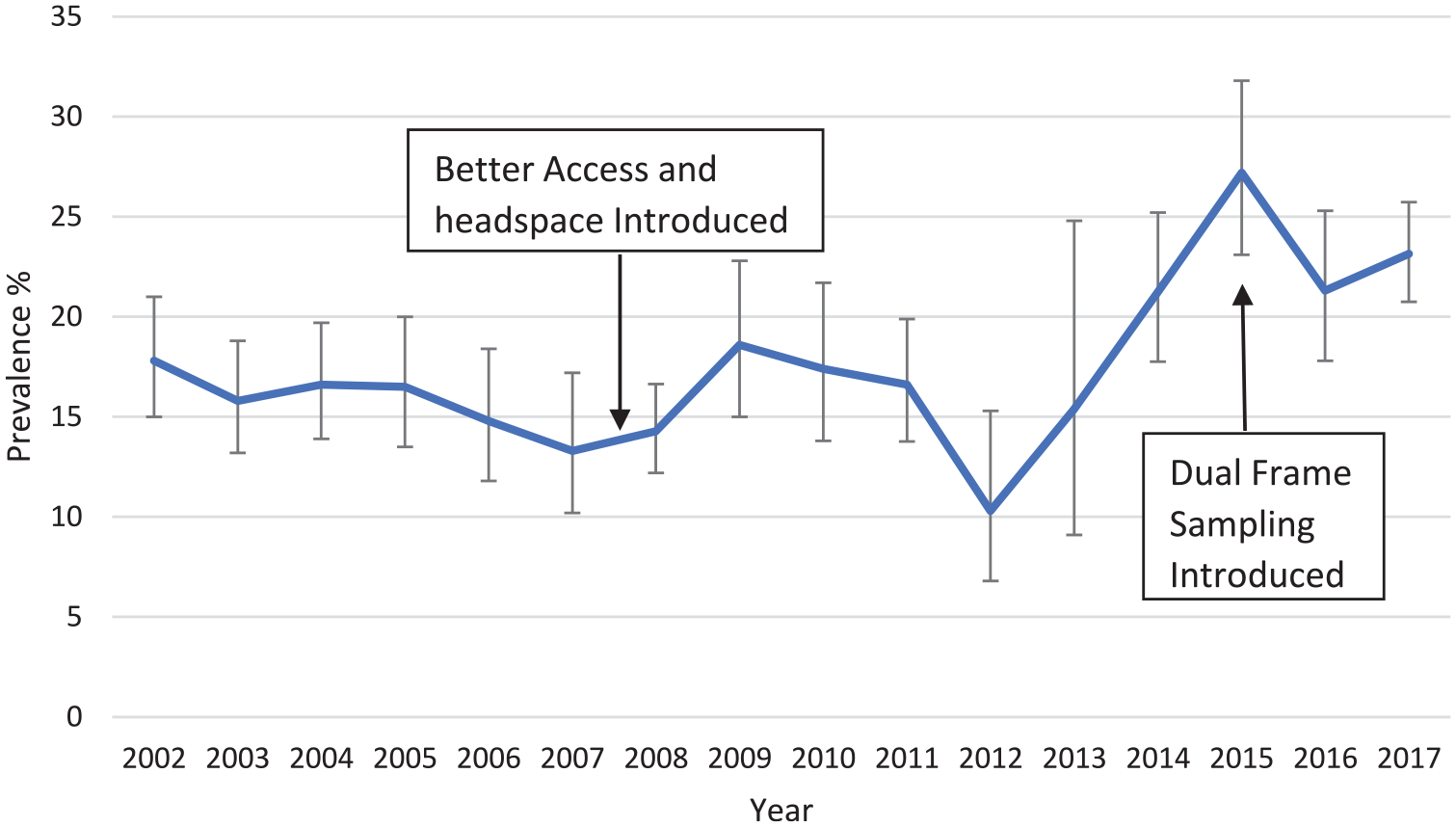
Prevalence of high and very high psychological distress (K10 ⩾ 22) in persons aged 18–24 years in the Victorian Population Health Survey. Error bars are 95% CIs.
Figure 5 shows the prevalence of psychological distress in youth aged 16–24 years from the New South Wales Population Health Surveys from 2003 to 2019. Prevalence did not change in the years following the introduction of Better Access and headspace. However, from 2013, when dual-frame sampling was introduced, the prevalence began to steadily rise.
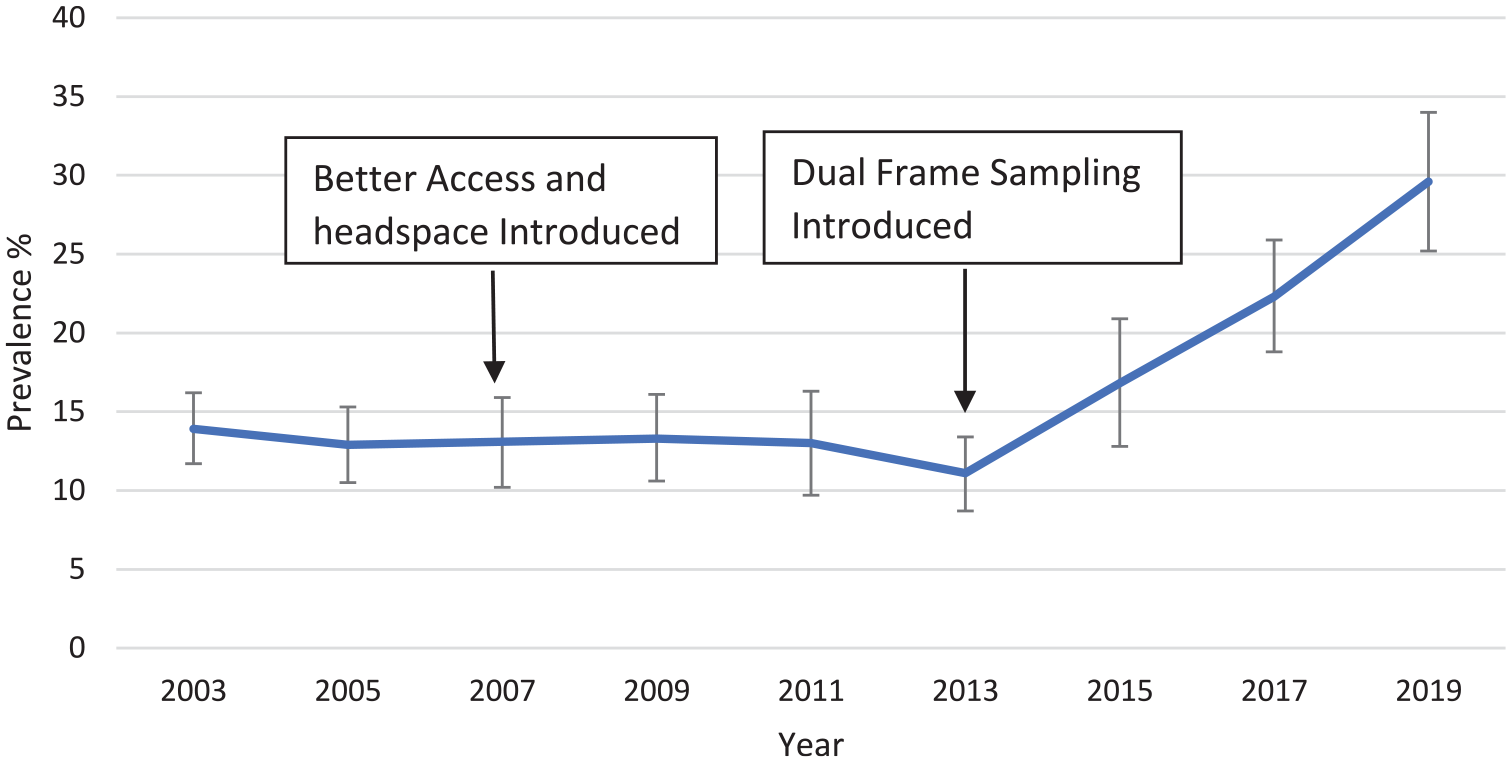
Prevalence of high and very high psychological distress (K10 ⩾ 22) in persons aged 16–24 years in the New South Wales Population Health Survey. Error bars are 95% CIs.
Figure 6 shows the prevalence of psychological distress from the meta-analysis for the Pre, Early, Mid and Late periods. Prevalence did not differ between the Pre, Early and Mid periods, but was higher in the Late period (as judged by non-overlapping CIs). A meta-regression, adjusting for methodological differences between the surveys, found that the Early and Mid periods did not differ significantly from the Pre period (with two-sided p-values of 0.605 and 0.676 respectively), whereas the Late period did differ from the Pre period, with significantly higher prevalence (two-sided p = 0.044).
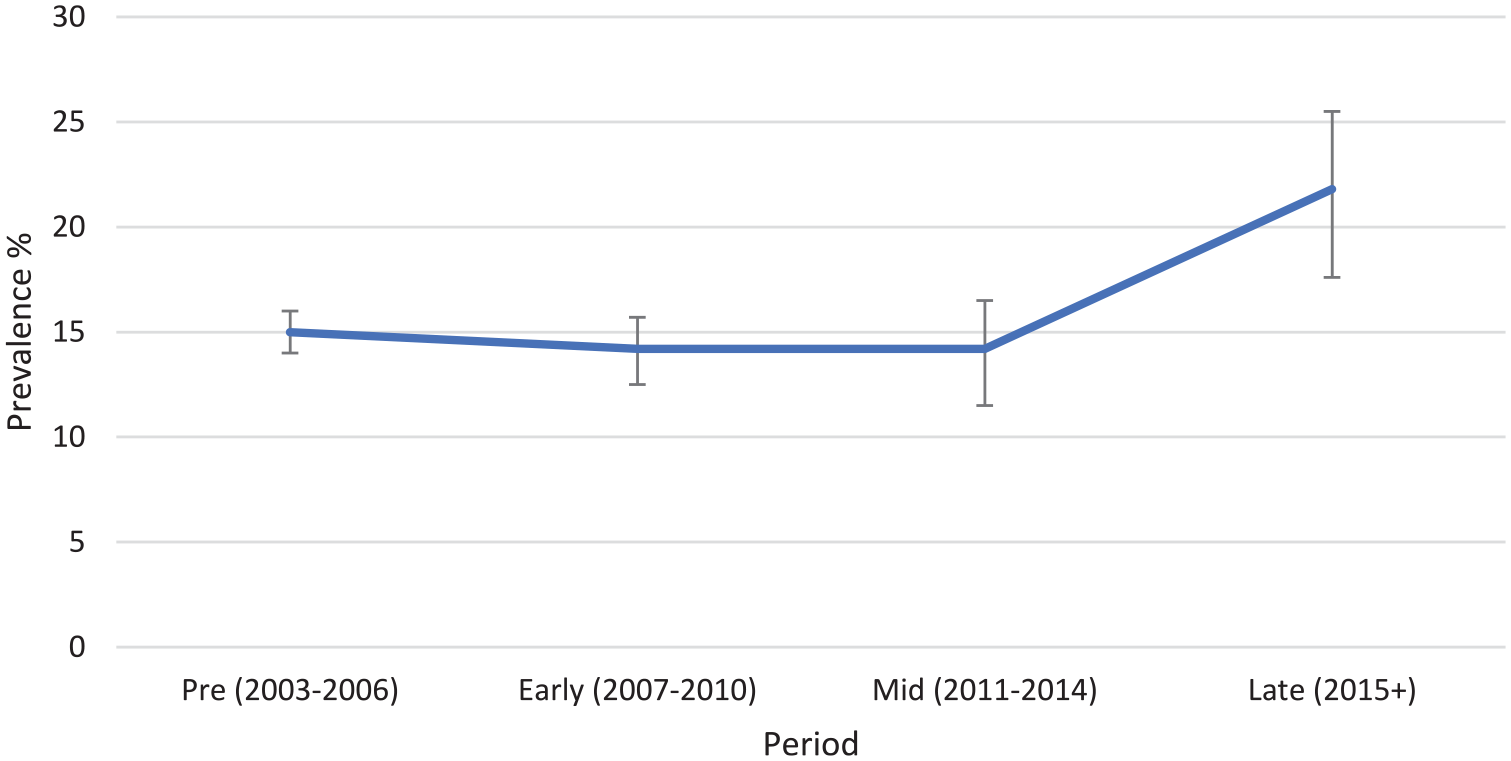
Meta-analytic estimates of prevalence of high and very high psychological distress in periods before and after introduction of additional services (Better Access and headspace). Error bars are 95% CIs.
Discussion
The data show a substantial rise in receipt of treatment services by Australian youth after the introduction of Better Access and headspace. The increases in services from clinical psychologists, other psychologists and allied health would all have been in the area of psychological therapy, as these professions do not have prescribing rights. The increase in GP services might involve either medication use or psychological therapy, but the exact nature of the services is unknown.
Despite these increases in services, examination of national and state data on prevalence of high and very high psychological distress in the years before and after the introduction of these services indicates no reliable change. However, prevalence appears to have risen in more recent years, with a higher prevalence in the period from 2015 onwards even after adjusting for differences in methodology.
These data are consistent with findings from the national surveys of child and adolescent mental health carried out in 1998 and 2013–2014 (Johnson et al., 2016; Sawyer et al., 2018a), which found a likely increase in services and a significant increase in the prevalence of major depressive disorder in adolescents. The data are also consistent with the findings from the HILDA study, which found no improvement that could be attributable to increases in services, but rather a small decline in mental health of adults aged 18–24 years from around 2013 onwards (Burns et al., 2020).
There are a number of possible reasons for the lack of impact of increases in services on prevalence. The first one is that there has been a reduction in prevalence, but it is too small to detect in surveys. Although meta-analysis was used to pool data and give more reliable estimates, it cannot be excluded that there was a small decrease in prevalence in the first 8 years following the introduction of these reforms. However, the higher prevalence from 2015 onwards is not consistent with a positive impact of increasing services.
Another factor behind the lack of change might be that treatments are less effective for the youth age group. A recent systematic review and meta-analysis of psychological therapy for depression in different age groups found that effects were weaker in adolescents compared to adults; however, they were as effective for young adults as for other adult age groups (Cuijpers et al., 2020). Similarly, there are data showing that antidepressant treatment is less effective in adolescents than in adults (Goodyer, 2018). However, given that the data on prevalence of psychological distress reported here are mainly from young adults rather than adolescents, this is unlikely to be a major factor.
A more likely explanation is that the quality of services is lacking – what has been called the ‘quality gap’ (Jorm, 2015a). Data from the 2013–2014 national survey of child and adolescent mental health found that only a small minority of adolescents received treatment that could be regarded as minimally adequate in terms of number of visits (defined as ⩾4 visits for mental disorders involving a psychotropic medication and ⩾8 visits for treatment without medication) (Sawyer et al., 2018b, 2019). It has also been reported that most youth attending headspace services do not receive minimally adequate number of visits (defined for adults as ⩾6 sessions of 30 minutes or longer for psychological therapy), with 45% receiving only 1–2 sessions (Jorm, 2015b). The present data show a mean of 0.66 Medicare services per person aged 15–24 years in 2019. If we assumed that the true prevalence of high and very high psychological distress in 2019 was 20%, this would mean that it would be possible to provide a mean of 3.3 services per case, which would not be sufficient to provide minimally adequate treatment to each individual. However, this estimate does not include non-Medicare services, including state-funded mental health services, some headspace services and mental health services provided by schools and tertiary education institutions. The present data do not allow an estimate of the total service provision for the youth age group.
Another possible explanation is that other factors have occurred in Australian society which are pushing prevalence up and these are masking the positive impact of service increases. One possibility is that Australian youth have become more open about reporting symptoms because of a decrease in stigma. However, an experimental test of this in Australian adolescents found no supporting evidence. In this study, adolescents who received teen Mental Health First Aid training in a randomized controlled trial were found to become more willing to disclose a mental disorder, but this greater willingness did not increase symptom reporting (Jorm et al., 2020).
Another way masking could occur is if risk factors for mental disorders in Australian youth had been increasing over the period examined. In the United States, Twenge (2020) has reported that depression, self-harm and suicide attempts have increased sharply in adolescents since 2011, which she has hypothesized is due to increased technology use, particularly the growth in smartphone use in the early 2010s. Mihalopoulos (2019) has proposed that a similar effect may have occurred in Australia and masked the benefits of the increase in services under the Better Access scheme. However, longitudinal data from both Australia and the United States do not support an association of screen media use and depression in adolescents (Coyne et al., 2020; Houghton et al., 2018).
Finally, it is possible that services alone are insufficient to reduce prevalence and that action is also required on prevention, in particular, a reduction in risk factors such as adverse childhood experiences, which have a major impact across a wide range of mental disorders across the lifespan (Jorm and Mulder, 2018).
This compilation of evidence has a number of limitations. While the focus was on the age range 12–25 years, the datasets used generally did not group age in this way. Most of the data were on young adults, with less on adolescents. The data on increases in services do not tell us what specific treatments were received or how long they were received, so we do not know which particular treatments increased or whether these were minimally adequate in dose. Finally, the data came from various sources and were not linked at the individual level, making it impossible to investigate associations between service use and mental health directly.
Conclusion
The large increase in provision of mental health services that occurred from 2006-2007 was not associated with a detectable reduction in the prevalence of high and very high psychological distress in Australian youth. In fact, it is possible that prevalence has increased since around 2015 and, if this is true, it is likely to be related to factors independent of service provision. As youth is an important phase of life for the onset of mental disorders, with possible lifetime implications for functioning, there is a need for a national discussion of how resources can be best deployed in this area. We also need research on whether there are preventable risk factors that may have worsened youth mental health in recent years.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Anthony F Jorm is supported by an NHMRC Investigator Grant.