
Abstract
The Australian National Hearing Screening Committee in November 2001 concluded that 1–1.5 in every 1000 live births or approximately 250–400 children are born with a significant hearing impairment each year [1]. Schooling of deaf children varies according to state and territory, but the overall trend is towards mainstreaming. For example, in the State of New South Wales, deaf and hearing impaired children are included into mainstream government schools [2, 3]. In contrast, Tasmania has provided bilingual (Auslan and English) education for deaf children since 1991 [4].
What happens when deaf children are referred to a mental health clinician for assessment and treatment of emotional and behavioural problems? Will a competent interpreter be present? Will the clinician have some understanding of deaf culture, the social and cognitive development of deaf children, or other relevant issues that provide the contextual framework in which the young person is assessed? For example, will children's frustration resulting from attempts to communicate with a professional who has no understanding of sign language be interpreted incorrectly as indicating emotional or conduct problem, or will their inability to complete written tests be interpreted as an indication of low IQ? Inadequate assessment of deaf children may result in wrong diagnosis as well as incorrect treatment [5]. Misdiagnosis of deaf individuals is common [6].
Research into the mental health of deaf children has been largely anecdotal and hampered by the lack of instruments that can be understood by them. It has been suggested that the application of standard psychiatric instruments to assess young deaf individuals is unreliable because of linguistic and cultural differences and impoverished language abilities [7–9]. Auditory deficits mean that access to spoken language is severely limited, and as a result, learning and producing spoken or written language is comparable to learning English as a foreign language [10–13]. For example, Australian Sign Language or Auslan is a three dimensional visual language that is vastly different from written or spoken English [14]. Certain concepts in Auslan and English do not share common characteristics and some phrases in vernacular English (e.g. idioms, proverbs and slang) do not make sense to deaf children. As a result, a majority of deaf youth do not have the language skills required to understand and complete standard psychiatric instruments. Thus, the administration of the usual questionnaires in deaf children and adolescents may be invalid or even unethical [15].
The advantages of interactive technologies to assess mental health problems in the deaf population are increasingly being recognized and their use is growing [16], but few studies investigating how questionnaires are translated and applied to deaf children and limited information available about the psychometric properties of such instruments in the literature [17].
This paper presents the results of a study in which the prevalence of emotional and behavioural difficulties in a sample of Australian deaf adolescents was assessed with a very widely used instrument, the Youth Self-Report (YSR) [18], in both its original written form as well as an Auslan version in interactive CD-ROM format to examine the influence of the instrument used on the prevalence of mental disorder in deaf adolescents. The hypothesis was that prevalence of psychopathology, particularly emotional problems, would be higher when using the Auslan version. This entailed the development of an Auslan version of the YSR whose reliability was also examined. The availability of an assessment instrument that could be administered by non-signing as well as signing health professionals would represent a significant advance in this neglected area.
Method
Participants
Criteria for inclusion in the study were: age 11–18 years, severe to profound hearing loss, proficient use of Auslan and not suffering from moderate or severe mental retardation. The study was approved by various Ethics Review Committees including the University of Sydney, Central Sydney Area Health Service, the Strategic Research Directorate of the NSW Department of Education and Training, the Department of Education State Support Service Tasmania, and the Royal Institute for Deaf and Blind Children in Sydney. Both adolescents and parents gave informed consent.
Contact with Deaf Societies of the Australian States of New South Wales and Tasmania, and with educational institutions in both States led to the identification of 81 families of deaf children, 58 of these families (72%) agreed to participate. One of the participating families had two deaf children. Five participants withdrew from the study (one because of absence and four because of a lack of proficiency in Auslan, two of the latter had mental retardation) resulting in a final sample of 54 children (29 male, 25 female). Eleven resided in Tasmania and 43 in New South Wales. Age ranged from 11 years and 6 months to 18 years and 8 months (Mean = 14.9 years).
Instruments
The Youth Self-Report, Child Behaviour Checklist (CBCL) [19] and Teacher Report Form (TRF) [20] are parallel instruments that measure children's and adolescents' adaptive functioning and emotional and behavioural problems in the previous 6 months, as reported by the adolescents themselves (11–18 years old) (YSR), parents or caregivers (CBCL) and teachers (TRF). They consist of 112 items scored on a three-point scale labelled 0 ‘not true’, 1 ‘somewhat or sometimes true’ and 2 ‘very true or often true’. A Total Problem score is computed by summing the individual item scores. Empirical analysis of these items resulted in two broadband syndromes (Internalizing and Externalizing) and eight narrowband syndromes (Anxious/Depressed, Withdrawn, Somatic Complaints, Social Problems, Thought Problems, Attention Problems, Rule-Breaking Behaviour, and Aggressive Behaviour). These scales have been shown to be of acceptable reliability and validity in non-hearing impaired children [21] and are very widely used measures of childhood psychopathology.
The Auslan version of the YSR
A.C., a psychotherapist fluent in Auslan, and J.N., a professionally accredited Auslan interpreter, made the initial translation into Auslan. Each item was filmed on videotape and back-translated into English by two native sign language users (one deaf and one hearing) who had no knowledge of the original written English versions. The translation/ back-translation process was repeated until all signed items were thought to reflect accurately the content of the written English version. Items were also revised to make them easily understood by deaf people from varied educational backgrounds. Semantic rather than literal equivalence to the English version was stressed.
When the team was satisfied with the cultural and linguistic accuracy of the Auslan version, the questionnaire was formatted to CD for use with a PC or laptop computer. When the participant's ID number was entered following a prompt in the screen, a start button appeared and the questionnaire started when this was clicked. A video box then appeared with an Auslan introduction and explanation about how to use the instrument – including response options, which subsequently were presented in English. Each question was represented by a single video clip. On the right of the window containing the video clip were buttons labelled with the three response options. In the introduction, participants were directed to select only one answer, but could change their mind and click on a different response. The last response was recorded. Participants could replay the video clips (introduction and questions) by clicking on the button ‘Rewind video’ underneath the video box. Once a question was answered, a button with the words ‘Next question’ appeared. Although the written YSR invites the respondent to elaborate on certain questions, free text responses were not available in the Auslan version. A prompt appears after every five questions to remind the participant of the three response options.
Procedure
Parents and adolescents were contacted through the schools and sent information explaining the study in detail and inviting them to participate. Those who agreed to participate each completed a booklet of questionnaires that included the standard versions of the CBCL (parents) and YSR (children). The child's teacher also completed a booklet of questionnaires that included the TRF. Approximately 1 week following completion of the written questionnaires, the same children were asked to complete the YSR translated into Auslan, which was administered in interactive CD-ROM format twice 2 days apart (to examine test–retest reliability). All children used computers regularly for their schoolwork. Information on IQ was provided by the school using the Wechsler Intelligence Scale for Children – Third Edition [22], or the Snijders-Oomen Nonverbal Intelligence Test – Revised [23]. Reading ages for all participants were also provided using the Woodcock Reading Mastery Test – Revised [24], or a global reading age determined by the child's main teacher. If IQ was unknown, the Raven Progressive Matrices [25] was administered. This is a widely used test to measure non-verbal intelligence, cited in the literature as a valid IQ test for signing deaf children [8].
Statistical analysis
To evaluate reliability, internal consistency of the YSR scales was computed using Cronbach's α, while test–retest agreement was calculated using Pearson's r. The results thus obtained were compared with data published for the American non-deaf normative sample [21].
The cut-off scores applied to identify adolescents with a clinically significant syndrome that is likely to require mental health treatment in the Australian National Survey [26] were used to estimate the effect of the responses on the English and Auslan versions on the prevalence of psychiatric syndromes. Odds ratios were computed to compare the prevalence obtained with the written and Auslan versions of the YSR and that reported for the National Survey [26]. Data were analysed using SPSS version 11.0 (SPSS Inc., Chicago, IL, US) [27].
Missing data
Following the procedure used in the questionnaire's scoring algorithm [28], up to eight (7%) of the 112 items were allowed to be not answered, and the missing items were conservatively computed as zero. When more than eight of the items were missing, results were considered invalid and not included in analysis. The missing data refer to deaf children not completing or leaving unanswered items in the written version, which reduced by about half of the number of participants available for analyses that included the written version of the YSR. There were no missing data in the signed, computer-administered version.
Results
Sample description
The mean age at diagnosis of hearing deficit was 1.8 years (ranging from birth to 7 years); 8 (14.8%) had severe and 46 (85.2%) profound hearing loss; 31 (57.4%) attended a bilingual, bicultural school, while 23 (42.6%) attended a specialized hearing impaired class. Mean performance IQ was 84.4 (SD = 14.12) and mean reading age was 10.2 (SD = 3.42).
Reliability
Internal consistency data (Cronbach's α) and test–retest reliability(r) for the signed and written YSR scales are presented in Table 1. This table can be summarized as follows:
Internal consistency (α) is acceptable (range 0.74–0.97) for both the written and Auslan (signed) versions, and comparable to that reported for the non-deaf normative sample. Test–retest correlations for the Auslan version (Table 1, column 4) are also acceptable (r ranging from 0.49 to 0.78) but slightly lower to those obtained in the non-deaf normative sample. For example, correlation for the Total Problems scale was 0.73 for the Auslan version in deaf children versus 0.87 for the English version in the normative sample. Correlation between the responses of deaf children to the written and Auslan versions (computed using the first Auslan administration) were low (range 0.29–0.71) and largely non-significant. If both versions (written and Auslan) were valid, it would be expected that the correlation between the written and Auslan versions would be similar to the test–retest correlation. This was not so, suggesting that answers given by deaf children to the written and signed forms of the YSR varied considerably, with the exception of Externalizing Behaviour, Aggressive Behaviour, Attention Problems and Rule-Breaking, in which correlations are not dissimilar from test– retest agreement. It is noteworthy that variation was largely restricted to emotional problems.
Prevalence of clinical syndromes
Prevalence of clinically significant syndromes that are likely to require mental health treatment according to the written and Auslan versions and the mean score for each scale are presented in Table 2, which also lists the parallel rates reported for the wider Australian nondeaf population obtained in the National Survey [26]. These results can be summarized as follows:
Scores for the written version of the YSR in deaf children are consistently lower than those obtained with the Auslan version (i.e. the written version results in lower levels of disturbance). Prevalence of disorder in the deaf sample obtained with the standard written version is comparable to that reported with the same instrument in the National Survey. For example, 21.4% of children in the deaf sample had Total Problems scores within the clinical range compared with 18.9% in the National Survey. This is reflected in a lack of statistically significant differences in prevalence between the deaf sample and the National Survey when using this instrument (with the exception of Social Problems, which were seven times more prevalent among deaf children). Prevalence of disorder in the deaf sample when using the Auslan instrument is about twice as high as when using the written instrument. When assessed with the Auslan version of the YSR, the prevalence of disorder among deaf children is higher than that reported in the National Survey. For example, 42.6% of children in the deaf sample had Total Problems scores within the clinical range compared with 18.9% in the National Survey (OR = 3.2; 95% CI = 1.83, 5.58). A similar result, though smaller, was found when using parent reports. Parents of deaf children were 2.5 times (95% CI = 1.10, 5.78) more likely to report Total Problems in the clinical range in their offspring than parents in the National Survey (Table 2, column 7).
Internal consistency (Cronbach's α) and test–retest reliabilities (r) of the Auslan (signed) and written versions of the Youth Self-Report for deaf sample with comparative data from a hearing normative sample
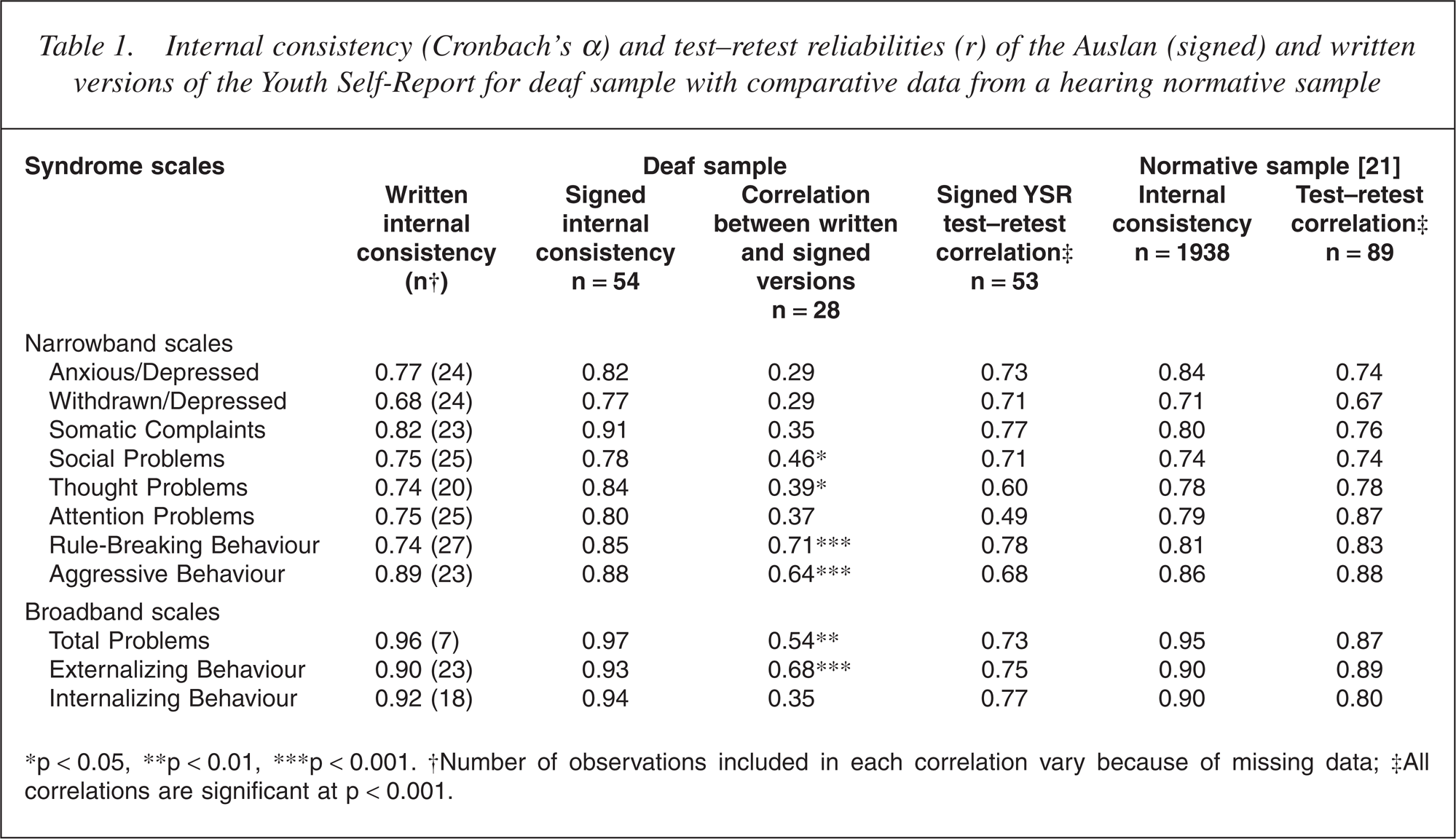
∗p < 0.05, ∗∗p < 0.01, ∗∗∗p < 0.001. †Number of observations included in each correlation vary because of missing data; ‡All correlations are significant at p < 0.001.
Mean scores and prevalence (%) of clinical syndromes according to the signed and written versions of the YSR in deaf adolescents and in the Australian National Survey
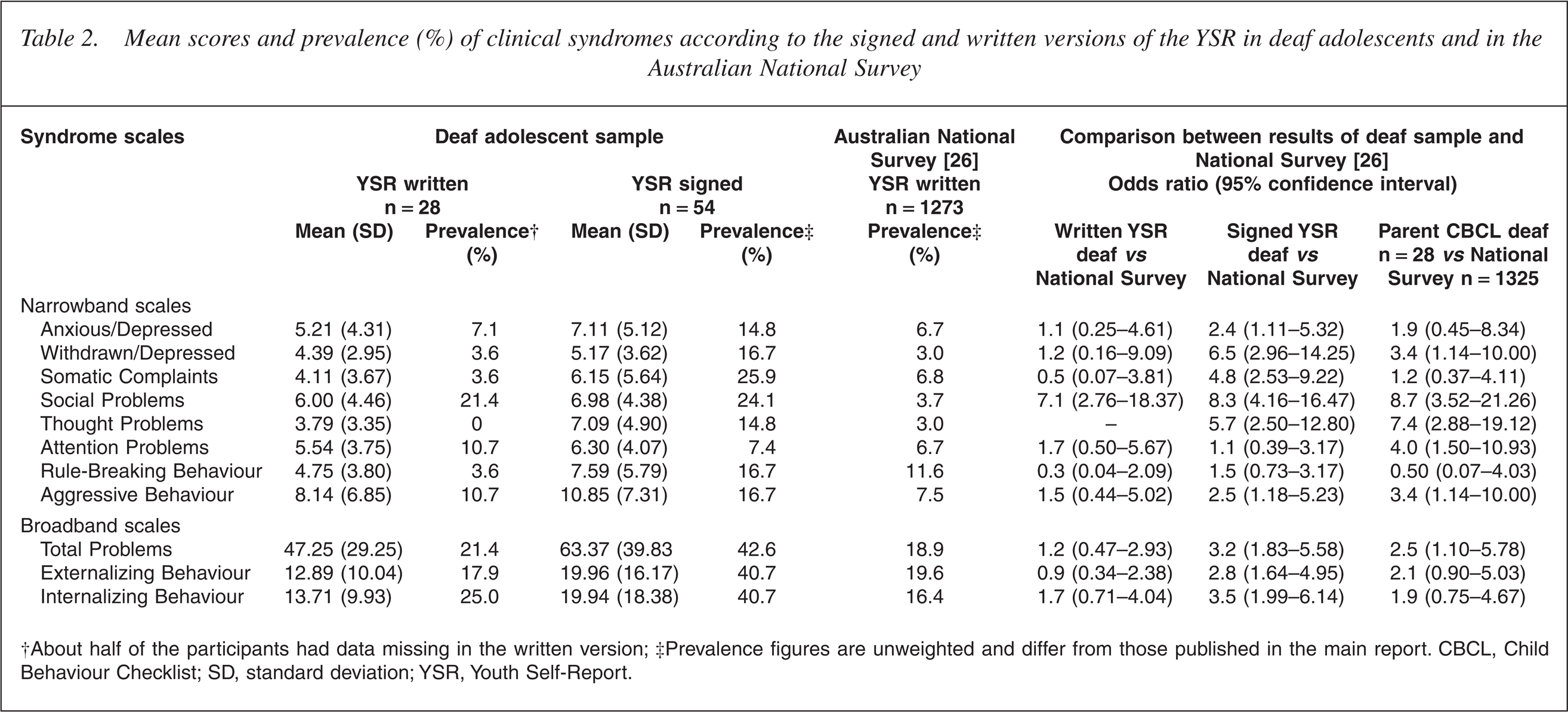
†About half of the participants had data missing in the written version; ‡Prevalence figures are unweighted and differ from those published in the main report. CBCL, Child Behaviour Checklist; SD, standard deviation; YSR, Youth Self-Report.
Prevalence of clinical syndromes according to informant
Figure 1 shows the percentage of deaf children who met criteria for each internalizing syndrome according to the child using the written YSR and the signed YSR, parent (CBCL) and teacher (TRF) while Fig. 2 shows similar data for externalizing syndromes. Overall, data obtained using the signed YSR result in the highest rate of disorder in all syndromes while the TRF produces the lowest. Further, agreement between informants is low. For example, for the Anxious/Depressed syndrome and for the Withdrawn/Depressed syndrome, not one of the children who self-reported a score in the clinical range according to the signed YSR achieved a clinical range score from the written YSR, the CBCL or the TRF.
Percentage of deaf children identified as having scores in the Clinical Range for Internalizing Problems according to the written and signed YSR, parent (CBCL) and teacher (TRF) reports. (▪) written YSR; (▪) signed YSR; (▪) CBCL; (□) TRF. CBCL, Child Behaviour Checklist; TRF, Teacher Report Form; YSR, Youth Self-Report. Percentage of deaf children identified as having scores in the Clinical Range for Externalizing Problems according to the written and signed YSR, parent (CBCL) and teacher (TRF) reports. (▪) written YSR; (▪) signed YSR; (□) CBCL; (▪) TRF. CBCL, Child Behaviour Checklist; TRF, Teacher Report Form; YSR, Youth Self-Report.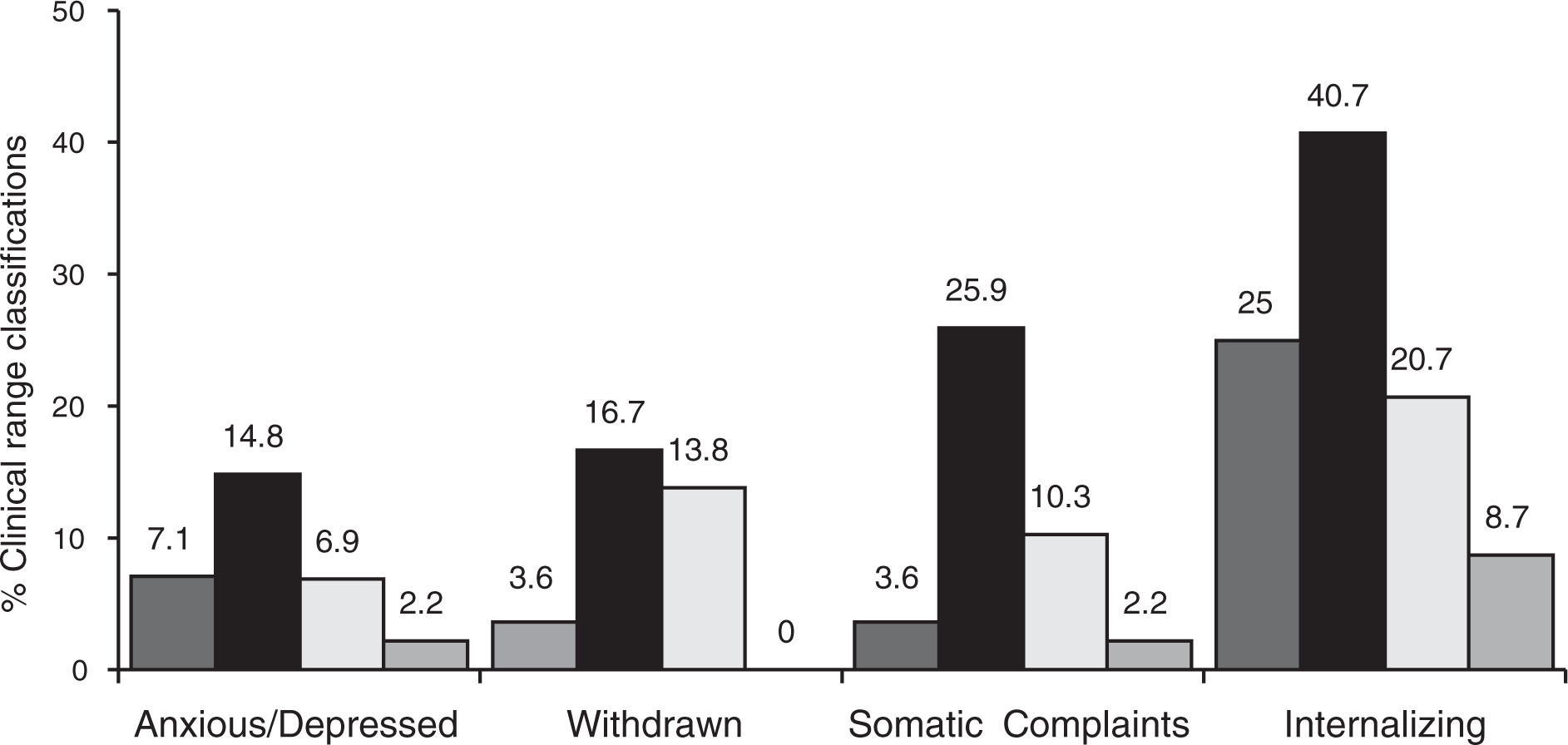
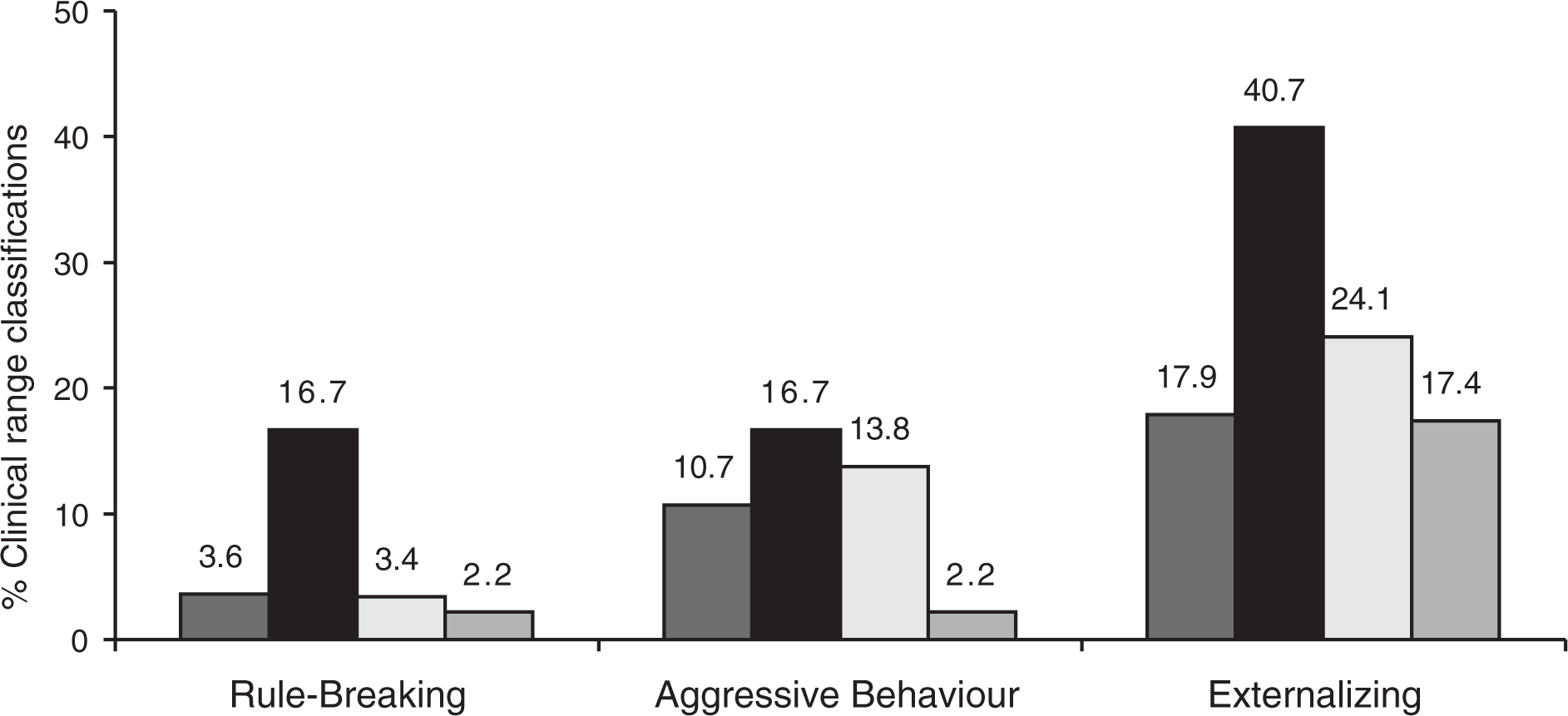
Figure 3 shows parallel data for Social, Thought and Attention Problems syndromes. Unexpectedly, teachers did not report attention problems in the clinical range in any of the deaf adolescents, and parents reported greater attention and thought problems than either adolescents or teachers. The written and signed YSR and the CBCL produced similar rates of clinical range scores in these three scales.
Percentage of deaf children identified as having scores in the Clinical Range for Social, Thought and Attention Problems according to the written and signed YSR, parent (CBCL) and teacher (TRF) reports. (▪) written YSR; (▪) signed YSR; (□) CBCL; (▪) TRF. CBCL, Child Behaviour Checklist; TRF, Teacher Report Form; YSR, Youth Self-Report.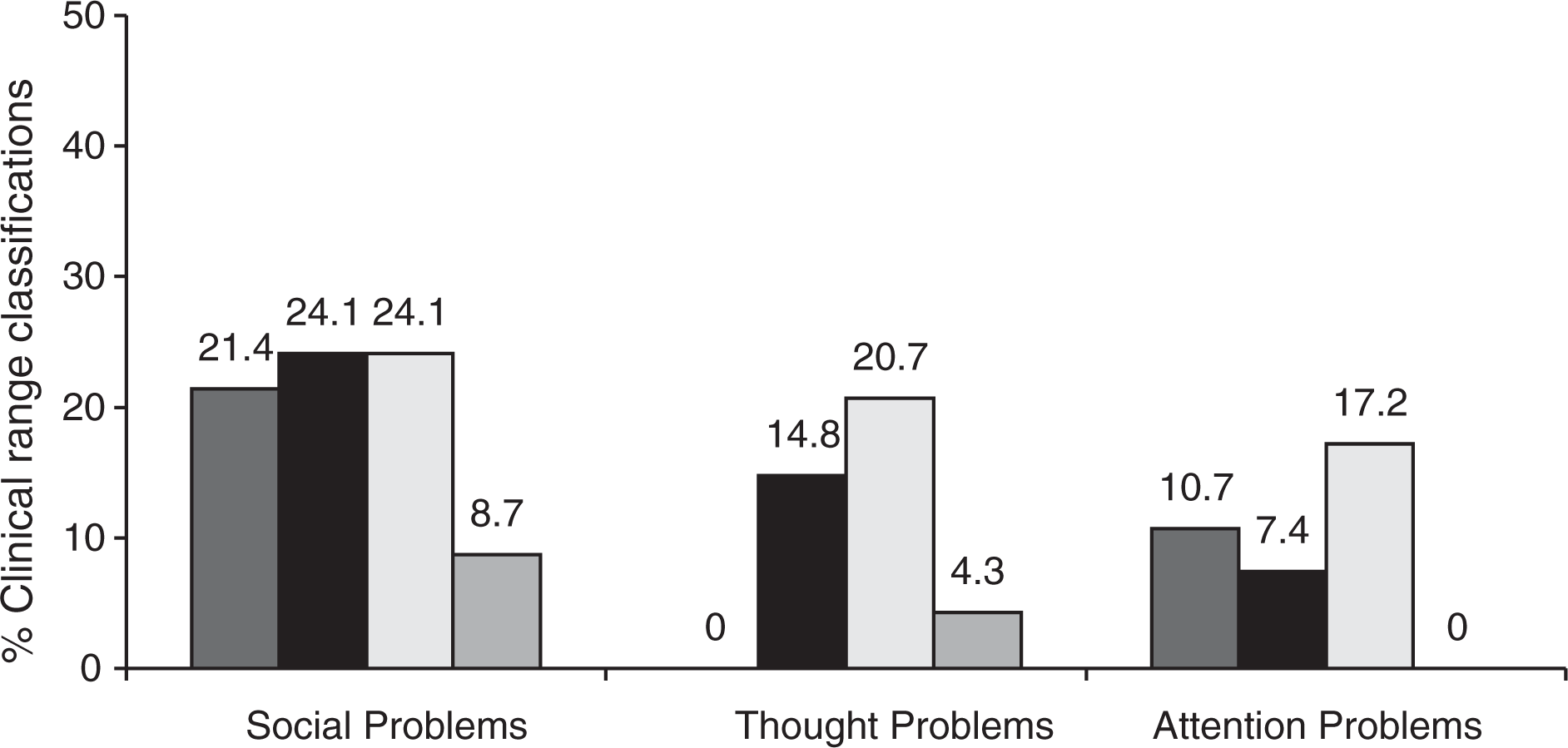
Discussion
Results of this study are consistent with the hypothesis that using standard English questionnaires underestimates the prevalence of psychological problems among deaf adolescents. When using the Auslan version, prevalence of significant problems (Total Problems) was 3.2 times (95% CI = 1.83–5.58) higher than that reported for the wider Australian adolescent population. This is particularly so when emotional problems were concerned. Examination of scores in the clinical range for the Total Problems scale from the signed YSR yielded a prevalence of 42.6%. This is double the rate reported in the general adolescent population but comparable with the results from a recent study using a modified YSR with deaf children who were late users of sign language and/or whose mothers did not sign [29]. The similar, though smaller, result found when using parent reports supports the validity of this finding.
The Auslan version also resulted in a higher rate of clinically significant syndromes than those obtained with the written version or when parents or teachers were the informants, with the exception of Social Problems, Thought Problems and Attention Problems, which were slightly higher according to parent's reports. This is broadly consistent with findings in non-deaf populations in which parents and teachers also underestimate children's emotional problems (e.g. [30–33]). However, differences in prevalence between the written and signed versions of the YSR are difficult to interpret given the high levels of data missing for the written YSR.
Correlation between the Auslan and English versions of the questionnaires was similar to the test–retest reliability in the externalizing scales, but lower for the internalizing ones. For example, test–retest correlation for the Anxious/Depressed scale was 0.73 while it was 0.29 between the English and Auslan versions. There are several explanations for this. It is possible this was due to some children being unable to read English given their reading age. Regrettably, we were unable to exclude this because stratifying the group according to reading age was not possible because of the small numbers, which made statistical tests unreliable. Another explanation is that deaf children are more willing to answer questions about their behaviour than their emotions. This is unlikely because children are typically more willing to answer questions about emotional than behaviour problems [31,34–36]. The most likely explanation in our view is that signing deaf children, though able to read English, may have a limited vocabulary about or understanding of affective states compared with behavioural items, which are more concrete and descriptive. As a result, they may have difficulty comprehending questions about emotions and are less likely to endorse the items. This may also explain the differences in the prevalence of all disorders across the board (i.e. not limited to emotional syndromes): higher with Auslan than when using written English (Tables 1,2).
Teachers tended to report the lowest rate of disturbance. In particular, teachers did not report Attention Problems in the clinical range in any of the deaf adolescents. This may reflect that teachers may make allowances for deaf children or that they may attribute behaviours in deaf children to their impairment rather than to disturbance. Alternatively, deaf children may show behaviours which are different from their hearing counterparts when they have difficulty paying attention. This may be because hearing children largely rely on auditory processes to concentrate in their environment while deaf children rely exclusively on visual cues. This requires further investigation. Results provide support for the reliability, validity and acceptability of the translation of the YSR into Auslan. As discussed, there is a need for such screening instruments so that they are accessible to signing deaf youth who may not have adequate written English skills to complete standard versions of questionnaires. Generally, participants reported that using the interactive CD-ROM was easy, and were able to work on the task of completing the questionnaire without interruption or help from the test administrator. The substantial missing data observed in the written English version of the YSR highlights adolescents' difficulties completing this questionnaire, and hence raises questions about their validity in this population. This was confirmed by the teachers who commented that participants often needed to ask for assistance when completing the written YSR; the extent to which this assistance influenced their answers could be the focus of a future study.
There are shortcomings in the study that need to be considered when interpreting the results, the main one being the already mentioned large amount of missing data in the written version of the questionnaire. This may have obscured further significant differences between the questionnaires, but does not invalidate the conclusions about reliability of, or the prevalence data obtained with the Auslan version. Also, the intellectual functioning of the deaf adolescents (mean performance IQ = 84.4) was substantially lower than that of participants in the National Survey. Although IQ was not measured in the National Survey, given the sample was representative of the population, it can be assumed to have been about 100. It is likely that differences between the National Survey and deaf group in the prevalence of clinically significant disturbance would have been lower should a comparison hearing sample with similar performance IQ had been used.
In conclusion, the results of this study show that an Auslan version of the YSR is reliable, easier to complete by deaf adolescents, and likely to give more reliable estimates of disturbance than standard written questionnaires. The fact that emotional and behavioural difficulties experienced by deaf youth are often overlooked or not treated effectively has already been discussed at length in the literature [5, 13, 37, 38]. Misunderstandings among clinicians about the unique and complex factors that underpin the difficulties experienced by deaf children, and the lack of appropriate assessment instruments, make their evaluation and treatment very difficult. Given that few professionals can communicate in sign language, this is an incentive for the use of contemporary technology and the translation into Auslan of other important psychological measures which will result in better services for this, often ignored, minority.
Footnotes
Acknowledgements
Thanks to the Australian Rotary Health Research Fund and the Deaf Society of NSW who provided financial support for this project.