
Abstract
Keywords
Human immunodeficiency virus-infected women, particularly those with low CD4+ cell counts, exhibit higher rates of persistent human papillomavirus infection with multiple oncogenic viruses, more abnormal Pap tests, more prevalent cervical intraepithelial neoplasia (CIN) lesions, increased progression rates of low- to high-grade squamous intraepithelial lesions, and aggressive invasive carcinoma of the uterine cervix when compared with their HIV-negative counterparts [1,2]. CIN is considered to be a HIV-related condition, whereas invasive carcinoma of the cervix is an AIDS-defining disease.
It has previously been shown that CIN in women with HIV infection is more likely to recur [3–5], especially in those individuals with severe immunosuppression [6]. In the aforementioned study involving 136 eligible HIV-infected women from the Bronx in NY, USA, Reimers et al. set out to determine predictors of treatment failure and recurrence for CIN in this cohort [7]. In most patients, surgical treatment of CIN either failed, or the patients experienced recurrence. Treatment failure was defined as the presence of CIN (1+) at initial follow-up, whereas recurrence was defined as the presence of CIN (1+) subsequent to initial normal follow-up.
Endocervical extension of CIN, a frequent finding among HIV-infected women [8], probably contributes to this high rate of recurrence. In this study, Reimers et al. reported that the majority (59%) of their patients had positive endocervical and/or ectocervical margins following an excisional procedure for CIN. Several other studies similarly demonstrated that HIV-infected women more often have incompletely excised (positive) endocervical margins, related to frequent glandular involvement [3,8]. Potential limitations of this study highlighted by the authors are the preference of providers in their region to perform a loop electrosurgical excision procedure (LEEP) for CIN; the number of women lost to follow-up; the fact that CD4+ and HIV RNA levels were obtained only at the time of excision (i.e., they may not be representative), and the variation in time they experienced between patient follow-up visits.
Results
In this retrospective cohort study of unselected, sequential HIV-infected women (mean age: 39 years) who had an extirpative procedure for confirmed CIN between 1999 and 2005, treatment failure and recurrence of CIN was common
Summary of treatment failure and recurrence rates of cervical intraepithelial neoplasia in studied HIV-infected women.
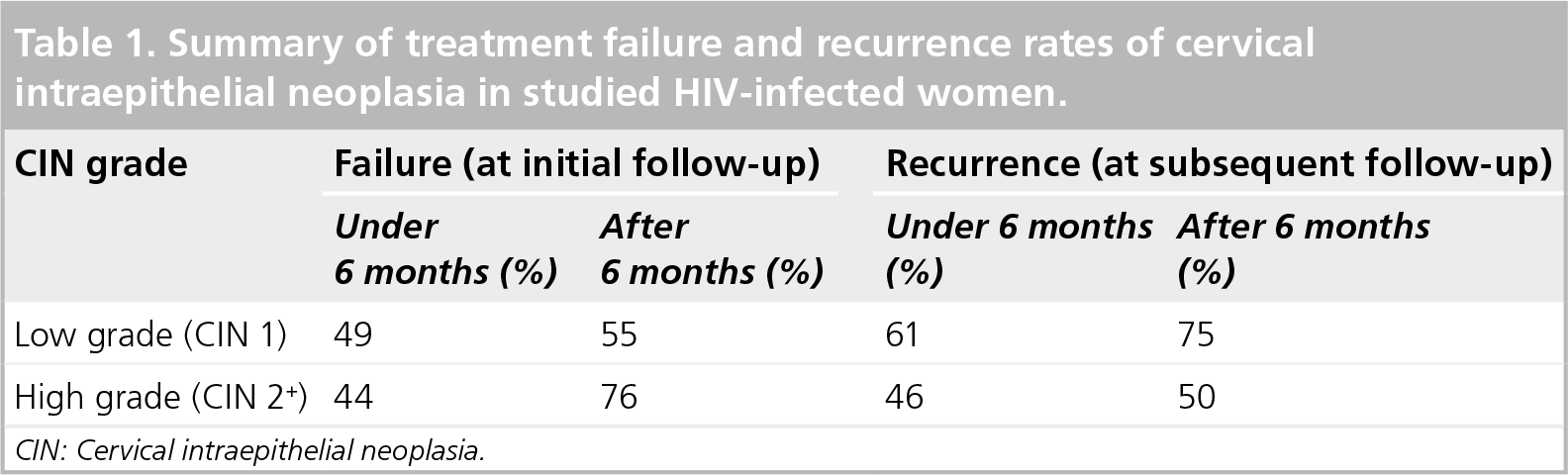
CIN: Cervical intraepithelial neoplasia.
Recurrence in these cases was associated with the use of LEEP, higher HIV RNA levels, and positive margins following excision. The median recurrence time following LEEP and conization was 33 and 81 months, respectively.
Significance
It has been suggested that the management of CIN in HIV-infected women should be the same as that in the general population [9]. There is currently no evidence that women living with HIV benefit from more aggressive treatment. Some authors recommend monitoring low-grade CIN and surgical treatment of high-grade CIN lesions [9]. However, this approach will probably depend upon the availability of resources. In the aforementioned study, 45% of women who had an excision of the uterine cervix had a low-grade CIN lesion; the remainder (55%) had high-grade CIN. Most of the lesions diagnosed in this study population at treatment failure or recurrence were high-grade CIN. The authors suggested that regular, frequent follow-up of these individuals was accordingly important. Follow-up in this population is likely to be problematic since, as reported in the study conducted by Reimers et al., many of their patients (56.2%) frequently missed three or more appointments.
Once high-grade CIN is confirmed on a tissue biopsy, it can be treated by ablative methods (e.g., cryotherapy or laser ablation) and excision (e.g., cold knife/laser conization or LEEP). Ablative therapy is typically considered for women with no suspected glandular or invasive squamous disease and those who are compliant with follow-up. In general, LEEP is favored by clinicians since this is an office procedure that reportedly has fewer short-term side effects. However, since conization in this study was associated with significantly less failure/recurrence than LEEP, the authors recommend that in this population a cervical cone is more desirable. Cold knife conization also permits margins to be better evaluated histologically without cautery artifact.
Future perspective
Based on these and previously published data, it is apparent that the treatment of CIN in HIV-infected women often fails. While other studies also found LEEP to be inferior to a cone biopsy [8], some investigators found no significant differences between cold knife, laser and LEEP [10]. The management of CIN in HIV-infected women needs to be further refined (e.g., LEEP vs conization in these patients). At present, the management of HIV-infected women with CIN should be the same whether they are receiving HAART or not [9]. However, the exact effect of HAART on CIN is unclear. Some studies have shown a benefit, whereas many others have not. Future studies related to the role of HAART as well as the impact of human papillomavirus vaccination on CIN are anticipated.
Executive summary
Cervical intraepithelial neoplasia (CIN) lesions are more prevalent in women infected with HIV.
In a retrospective cohort study of 136 HIV-infected women, treatment failure and recurrence of CIN were common, even after initial successful treatment of CIN.
Failure/recurrence of CIN is particularly high in women with poorly controlled HIV, after loop electrosurgical excision, and those with positive tissue margins following treatment.
Cervical conization appears to be superior to loop electrosurgical excision in the treatment of CIN in HIV-infected women.
Footnotes
The author has no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
No writing assistance was utilized in the production of this manuscript.